
Abstract
Introduction
Kitchen-related tasks are widely used in occupational therapy for adults with acquired brain injury. This study aimed to investigate the effectiveness of kitchen-related, task-based occupational therapy interventions for improving clinical and functional outcomes in the rehabilitation of adults with acquired brain injury.
Method
A systematic review of the literature was conducted with narrative synthesis (PROSPERO registration CRD42019141898), by searching relevant electronic databases (BNI, CINAHL Plus, MEDLINE, DORIS, OT Seeker etc.), registries of ongoing studies (ISRCTN, PROSPERO, etc.), and grey literature (OpenGrey, etc.). English-language studies that evaluated kitchen-related tasks in the rehabilitation of adults with acquired brain injury were included and independently appraised for their methodological quality by two reviewers.
Results
Seventeen primary studies met the eligibility criteria. Studies were heterogeneous in methods, methodological quality, setting, sample size, purpose, and design of kitchen-related tasks. Fifteen studies evaluated kitchen-related, task-based treatments for improving function, and two studies examined kitchen-related task assessments for safety and task performance. This provides very limited evidence for the effectiveness of kitchen-related, task-based interventions compared to interventions not based on kitchen-related tasks.
Conclusion
While kitchen-related, task-based occupational therapy interventions in acquired brain injury rehabilitation are common practice, there is currently limited research evidence to support this. Further studies are warranted to strengthen the evidence base.
Introduction
Occupational therapy emphasises the relationship between cognition and occupation through occupation-based, client-centred intervention (Gillen, 2015; Katz, 2005). The intervention focuses on assisting people to engage in daily life activities that they find meaningful (COT, 2013). Hence, task-based approaches using a variety of common activities of daily living (ADL) are frequently used in clinical practice to facilitate functional rehabilitation after brain injury and stroke. Such task-based interventions and ADL retraining not only provide a holistic approach to treatment; there is also strong evidence that these improve functional independence and prevent skill deterioration after stroke (Legg et al., 2006). Task-specific training is also highly recommended in stroke and brain injury rehabilitation to access enduring motor learning-associated cortical re-organisation (Harvey, 2009).
Kitchen-related tasks (KRTs) in various forms, such as preparation of snacks, meals, breakfast, and hot drinks, are routinely used as instrumental ADL in occupational therapy for patients who have acquired brain injury (ABI). KRTs have been in common practice in occupational therapy due to their high therapeutic properties, for example, their continuous demand on the person’s ability to schedule, predict, and plan a series of abstract consequences of actions, with a high motor and sensory requirement to complete the task (Cerasa et al., 2017). However, although the perceived value of using such a task-based approach is well established, the evidence on the specific use of these KRTs is unclear.
A substantial number of people experience cognitive and motor impairment after ABI, which influences their participation in various occupational tasks (Gillen, 2015). This is commonly manifested as having difficulty in performing basic and domestic ADL. Various studies have established a strong correlation between decreased processing speed and executive functioning difficulty during meal planning and preparation in closed head-injured patients and patients with resected frontal lobe tumours (Godbout et al., 2005). Literature suggests performance and skills in functional cooking are related to intact cognitive abilities in delayed verbal memory, simple auditory attention, and visuospatial skills, as well as overall cognitive performance, although cooking also involves significant motor ability (Yantz et al., 2010). Cognitive difficulties, especially those involving executive functions and visuospatial perceptions, are associated with an individual’s ability to plan and prepare a meal after a traumatic brain injury (Neistadt, 1994a, 1992a). Similar relationships have also been established in patients who have had a stroke (Yantz et al., 2010). Strong correlations have been described between functional cooking and neuropsychological performance of attention, working memory, and verbal fluency cognitive performance such as orientation, perception, visuomotor organisation, and ‘thinking operations’ in inpatients with stroke (Baum et al., 2008; Katz et al., 2000). Moreover, functional cooking activities have been identified as important for the individual’s sense of life satisfaction (Hartman-Maeir et al., 2007) and are highly valued by patients as a meaningful occupation during rehabilitation after stroke and head injury (Bigelius et al., 2010).
Hence, KRTs are used both as brief, non-standardised, performance-based instrumental ADL measures for functional assessment of impaired skills (Baum et al., 2008; Hartman-Maeir et al., 2009; Neistadt, 1992a), and as part of the assessment in preparation for discharge. These typically involve self-report or non-standardised clinical assessments. Meal preparation tasks have also been frequently used in neuropsychological research exploring cognitive functioning of the brain in relation to self-awareness, occupational identity, and community integration after brain injury (Chevignard et al., 2008; Hartman-Maeir et al., 2007; Schmidt et al., 2015). In addition, KRTs are frequently used as treatment activities for improving specific functional performance. The use of KRTs for functional retraining has been described as an excellent opportunity for procedural skill development in people after brain injury, using learning through the implicit memory system and neuro-functional approaches through task-specific training (Trevena-Peters et al., 2018). However, there are few standardised approaches for the implementation and evaluation of KRT-based interventions (Zhang et al., 2003).
Little is known about current practices and the value of using KRT interventions in the rehabilitation of adults with ABI, particularly in the acute setting. Despite the frequent use of KRTs in clinical practice for both assessment and treatment purposes in acute inpatient rehabilitation units in the United Kingdom (UK), there is a scarcity of evidence to support their clinical effectiveness and cost-effectiveness in these settings. Also, there have been reports of inconsistency in the application of KRT activities, especially for clinical decision-making prior to discharge (Crenan and MacRae, 2010). There is, therefore, a need to identify the evidence for KRTs as an intervention in acute rehabilitation settings to inform and guide current clinical practice. A systematic review was conducted, with the aim of investigating the effectiveness of KRT-based occupational therapy interventions for improving clinical and functional outcomes in the rehabilitation of adults with ABI. The objective was to identify and summarise the evidence for the use of KRTs in occupational therapy, both as assessments and treatments for adults with ABI in rehabilitation settings.
Methods
A systematic review is the appropriate method to systematically search for, appraise, and synthesise research evidence in order to answer a defined, focused question (Grant and Booth, 2009; Unsworth, 2017). Details of the protocol for this systematic review were registered on PROSPERO and can be accessed at www.crd.york.ac.uk/PROSPERO. Reporting of this systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009). The PRISMA checklist is given in Online Appendix 1.
The search strategy was developed based on concepts and keywords used in the Population, Intervention, Comparison, Outcomes and Study design (PICOS) framework:
Types of participants: Adults (age 18+ years) with ABI. ABI defines a brain injury that is not hereditary, congenital, degenerative, or induced by birth trauma, but a type of brain injury that has occurred after birth, including stroke, cerebrovascular accident (CVA), traumatic brain injury (TBI), and head injury (HI). Types of interventions: KRTs either directly facilitated or supervised by an occupational therapist, in the context of rehabilitation provision. For the purpose of this review, the term ‘intervention’ was used to encompass both ‘assessments’ (patient evaluations using KRTs with implications for clinical decision-making such as discharge planning) and ‘treatments’ (KRT-based activities which are commonly delivered over a course of sessions and which aim at achieving functional gain). Types of comparators: Any alternative intervention(s) or usual care. Types of outcomes: Performance in specific task components or functional outcomes, quality of life, length of hospital stay, discharge goals or destinations, level of support required for independent living post discharge, patient satisfaction, outcomes related to safety or other risks that might guide rehabilitation practice. Types of study designs: Controlled trials (including randomised and quasi-randomised controlled trials), cohort studies, case-control studies, case series, and single case studies/case reports were included for review of the evidence and quality analysis.
The search strategy included search terms such as ‘meal preparation’, ‘kitchen’, ‘hot drink’, ‘stroke’, and ‘brain injuries’. The full search strategy is given in Online Appendix 2. The authors searched relevant electronic databases and registries (from inception or from 1979, whichever was later) for peer-reviewed scientific publications (BNI, CINAHL Plus, CDSR, DORIS, Google Scholar, MEDLINE, OT Seeker, OTDBase, PEDro, PsychBITE, PsychINFO, REHABDATA, Scopus, TRIP Pro, Web of Science Core Collection), records of ongoing studies (CENTRAL, Clinical Trials, ISRCTN registry, PROSPERO), and grey literature (Ethos, HILO, OpenGrey). Reference lists of review articles and other relevant papers were hand-searched, and researchers were contacted directly when necessary. Searches were completed from 08 to 16 July 2019. Time-restricted searches were re-run prior to the final analysis to include further relevant studies (last date searched 20 November 2019). Published English-language reports of completed studies were included in the first instance; unpublished studies were also considered if the relevant information was made available.
The two authors independently screened search results against eligibility criteria according to the PICOS. Results were de-duplicated after screening the title and abstract, and the two authors independently reviewed the remaining results in full text. Disagreements were resolved by discussion and consensus. As part of this process, a decision was made to revisit and refine the eligibility criteria to ensure that relevant literature was included. The study setting had initially been restricted to inpatient settings where occupational therapy was provided as a part of rehabilitation on a regular basis, such as in acute hospitals or inpatient rehabilitation facilities. Due to the small number of eligible studies, this eligibility criterion was widened to include studies conducted in community settings. In addition, the comparator criterion was widened to also include usual care. It was decided to explicitly exclude studies conducted within the context of (neuro-)psychology, where the focus was on validating standardised psychological assessments against an individual’s performance of KRT, as opposed to occupational therapy rehabilitation. Lastly, the authors decided to include studies that did not report patient outcomes but that were directly relevant to KRTs in the context of occupational therapy in rehabilitation of ABI.
A standardised data extraction form was used to independently extract specific data items for each study, including the first author and year of publication, aim(s), design and methods, study setting, intervention, comparison, description of the KRT(s), participant characteristics, outcome measures, and study findings extracted against each outcome measure. The authors used the checklist for assessing the quality of quantitative studies developed by the Alberta Heritage Foundation for Medical Research (2004) to accommodate a variety of study designs in assessing the risk of bias of individual studies. In addition, for all controlled studies, the PEDro quality assessment tool was completed with the calculated PEDro summary score (De Morton, 2009). The hierarchy of evidence developed by the Oxford Centre for Evidence-Based Medicine (OCEBM, 2011) was used to give a description of the level of evidence for individual studies.
After considering the feasibility and appropriateness of combining quantitative data in view of statistical, clinical, and methodological heterogeneity, a decision was made to conduct a narrative synthesis of findings. Quantitative data were analysed descriptively (summary measures for each relevant outcome).
Results
The titles and abstracts of 2227 records were screened. Of these, 2031 records did not match the PICOS and were excluded. After de-duplication, 78 full-text articles were assessed for eligibility and 56 were excluded. Reasons for exclusion at this stage are given in the PRISMA flow diagram (Figure 1). The remaining 22 articles reported 17 primary studies and were included for data extraction, assessment of bias, and narrative synthesis.
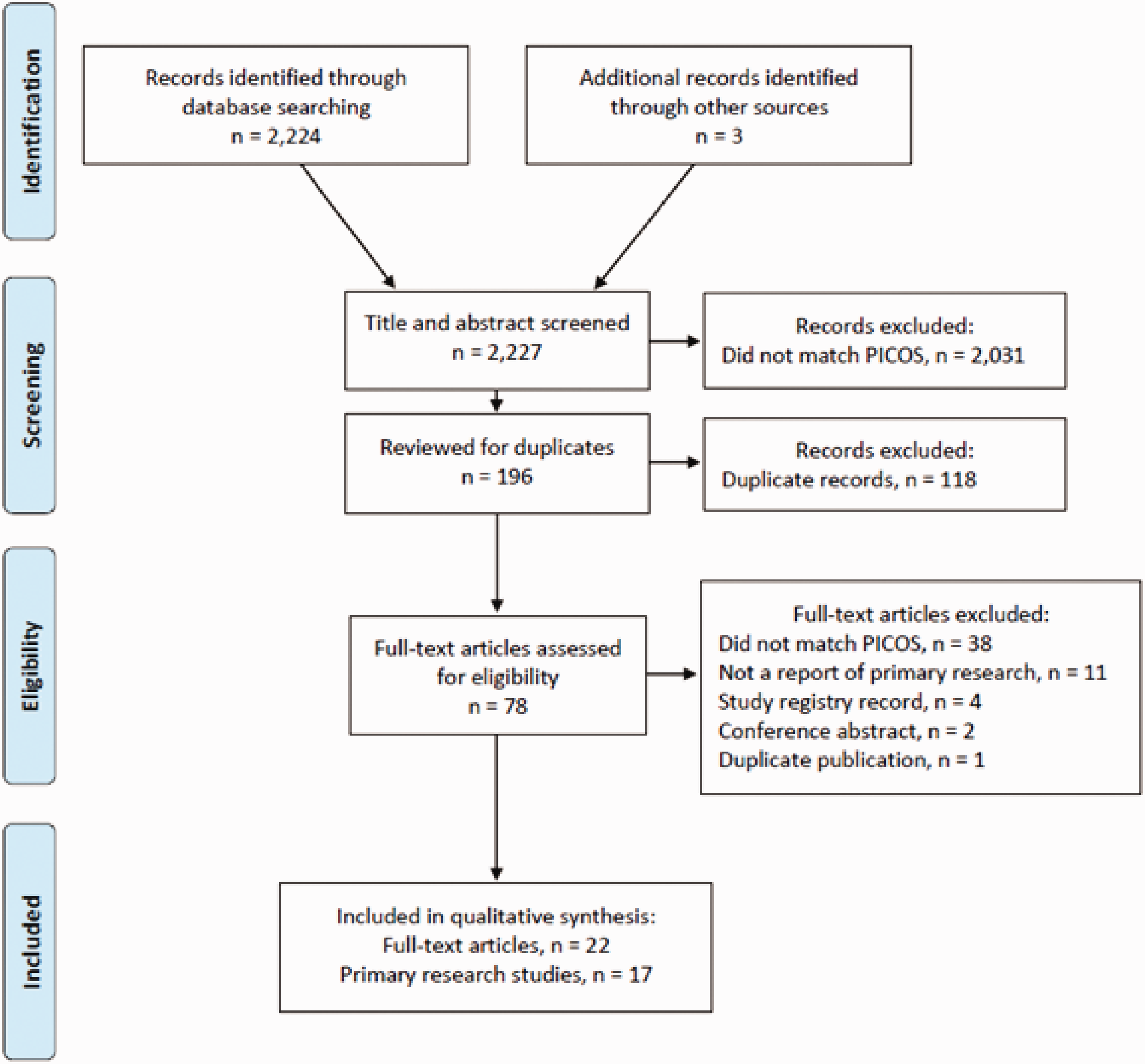
PRISMA flow diagram.
The included studies were heterogeneous with respect to PICOS criteria, sample size, and follow-up period. Eleven studies were conducted in inpatient settings (Cerasa et al., 2019; Eakman and Nelson, 2001; Edmans et al., 2009; Foxhall and Gurr, 2014; Liu et al., 2004; Logan et al., 2003; Patterson et al., 2017; Paul 1997; Schmidt et al., 2013; Tanguay et al., 2014; Trevena-Peters et al., 2018) and six in community settings (Gasser-Wieland and Rice, 2002; McGraw-Hunter et al., 2006; Neistadt, 1992a; Ownsworth et al., 2017; Poncet et al., 2018; Robnett et al., 2016). Participant characteristics included individuals with TBI in five studies (McGraw-Hunter et al., 2006; Ownsworth et al., 2017; Patterson et al., 2017; Schmidt et al., 2013; Trevena-Peters et al., 2018), CVA in six studies (Cerasa et al., 2019; Edmans et al., 2009; Gasser-Wieland and Rice, 2002; Liu et al., 2004; Logan et al., 2003; Paul 1997), and ABI from various causes in the remaining six studies. Six studies were randomised controlled trials (RCTs) (Eakman and Nelson, 2001; Liu et al., 2004; Neistadt, 1992a; Ownsworth et al., 2017; Schmidt et al., 2013; Trevena-Peters et al., 2018). Other study designs included a retrospective analysis of trial data (Logan et al., 2003), cross-sectional observational studies (Patterson et al., 2017; Robnett et al., 2016; Tanguay et al., 2014), and single case reports or case series with a repeated measures design (Cerasa et al., 2019; Edmans et al., 2009; Gasser-Wieland and Rice, 2002; McGraw-Hunter et al., 2006; Patterson et al., 2017; Paul 1997; Poncet et al., 2018). In one study (Foxhall and Gurr, 2014), therapeutic meal preparation group sessions were observed to describe and assess the content of sessions. Sample sizes ranged from a few participants in single case reports and case series to n = 309 in the retrospective analysis of trial data by Logan et al. (2003). Detailed study characteristics are presented in Table 1.
Study characteristics.

ABI: Acquired Brain Injury; ADL: Activities of Daily Living; CG: control group; CVA: cardiovascular accident; EBL: Error-Based Learning; ELL: Error-Less Learning; IG: intervention group; KRT: kitchen-related task; PT: physiotherapist; TBI: traumatic brain injury.
With respect to the intended purpose of KRT interventions, the studies were thematically grouped to give an overview of the investigators’ rationales and approaches for studies of KRTs (Table 2). Fifteen studies pursued the overall aim of improving cognitive function, physical function, or task performance through KRT treatments. Of these, five studies compared KRT against non-KRT treatments or usual care; that is, the KRT treatment constituted the aspect under investigation (Cerasa et al., 2019; Edmans et al., 2009; Logan et al., 2003; Neistadt, 1992a; Poncet et al., 2018). Eight studies examined treatments in which the aspect under investigation was delivered through a KRT, but was not inherently related to KRTs; for example, a comparison of error-less and error-based learning in cooking (Eakman and Nelson, 2001; Gasser-Wieland and Rice, 2002; Liu et al., 2002; McGraw-Hunter et al., 2006; Ownsworth et al., 2017; Paul 1997; Schmidt et al., 2013; Trevena-Peters et al., 2018). Two studies aimed to provide detailed descriptions of KRT treatments without investigation of the outcome (Foxhall and Gurr, 2014; Patterson et al., 2017). In contrast to these 15 studies, the studies by Robnett et al. (2016) and Tanguay et al. (2014) examined the use of KRTs for the purpose of assessing safety and/or capability of task performance. In addition, several of the included studies addressed two distinct points of interest: firstly, the comparison of KRTs as occupationally embedded and meaningful activities as opposed to abstract or isolated tasks and activities (Eakman and Nelson, 2001; Gasser-Wieland and Rice, 2002; Neistadt, 1992a); and secondly, the use of virtual KRTs to substitute actual kitchen environments (Edmans et al., 2009; Tanguay et al., 2014) (Table 2).
Thematic grouping of studies according to the intended purpose of kitchen-related tasks.
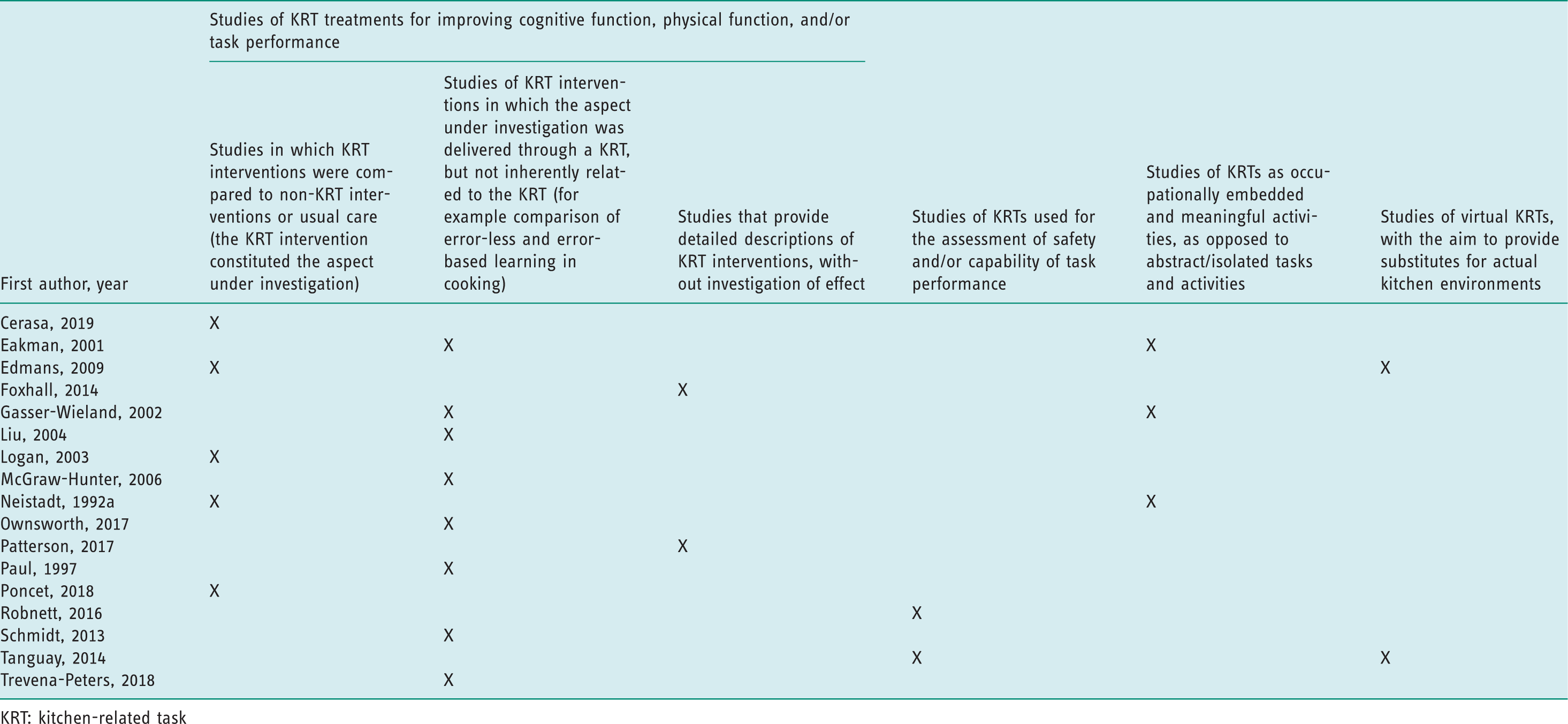
KRT: kitchen-related task
Individual quality assessments of included studies are presented in Online Appendix 3. Summary quality scores ranged from 37% to 100%, with a median of 67% (percentage of the possible maximum score, higher percentages reflect better study quality). For the six RCTs, the PEDro score ranged from 6/11 to 9/11 with a median of 9/11 (higher scores reflect better study quality). The RCTs also yielded the highest level of evidence (OCEBM level 2), except for the study by Eakman and Nelson (2001), which was graded down to OCEBM level 3 due to lower quality. The remaining studies were graded at evidence levels 3, 4, and 5, based on study design and quality. The study by Foxhall and Gurr (2014) was not graded due to its purely descriptive design.
Study outcomes reflect the heterogeneity in study aims and designs. Outcome measures included standardised measures of cognitive/physical impairment and activity (including standardised assessments of KRTs), as well as measures that were customised specifically to the KRT and intervention or the respective study (for example computerised scoring of a virtual KRT training programme). Details of outcome measures and results are presented in Table 3.
Outcome measures and results.

ABI: acquired brain injury; ABS: Agitated Behaviour Scale; ADL: activities of daily living; ANCOVA: analysis of covariance; ANOVA: analysis of variance; AQ: Awareness Questionnaire; CANS: Care and Needs Scale; CD: Freehand Copying of Drawings; CDL: Copying Drawings with Landmarks; CG: control group; CIQ: Community Integration Questionnaire; COPM: Canadian Occupational Performance Measure; COWAT: Controlled Oral Word Association Test; CVA: cardiovascular accident; DASS-21: Depression Anxiety and Stress Scale; EADL: Extended Activities of Daily Living Scale; EBL: error-based learning; ELL: error-less learning; FIM: Functional Independence Measure; HAMA: Hamilton Anxiety Rating Scale; HAMD: Hamilton Depression Rating Test; IADL Profile: Instrumental Activities of Daily Living Profile; IG: intervention group; IQR: interquartile range; KELS: Kohlman Evaluation of Living Skills; MANCOVA: Multivariate analysis of covariance; NLQ: Nottingham Leisure Questionnaire; NOE: non-occupationally embedded; OE: occupationally embedded; PCRS: Patient Competency Rating Scale; PT: physiotherapist; PTA: post-traumatic amnesia; RADLS: Rehabilitation Activities of Daily Living Survey; RKE-R: Rabideau Kitchen Evaluation-Revised; SAH: Safe at Home Screening; SDMT: Symbol Digit Modalities Test; SPIRQ: Self-Perception in Rehabilitation Questionnaire; SPRS: Sydney Psychosocial Reintegration Scale; TBI: traumatic brain injury; TMT: Trial Making Test; TOL: Tower of London; VS: visual research; WAIS-R: Wechsler Adult Intelligence Scale – Revised; WCST: Wisconsin Card Sorting Test.
KRTs as treatment
In the group of studies that compared KRT treatments to non-KRT treatments or usual care, the RCT by Neistadt (1992a) provided high-level, moderate-quality evidence that an occupationally embedded KRT in patients with ABI in a community setting did not result in better improvement in the Rabideau Kitchen Evaluation-Revised (RKE-R) than an abstract construction task, although there was a trend in favour of the KRT group. The secondary analysis of RCT data by Logan et al. (2003) provided moderate-level, moderate-quality evidence that the provision of cooking therapy in inpatient rehabilitation of patients with CVA did not increase the likelihood of independence in cooking tasks. The single case reports/series by Cerasa et al. (2019), Edmans et al. (2009), and Poncet et al. (2018) yielded low-level, moderate-quality evidence for their respective KRT treatments and patient groups, with mixed findings of some improvement in co-ordination and cognitive function in Cerasa et al. (2019); no improvement in hot drink-making scores in Edmans et al. (2009); and statistically significant improvement in the Cooking Task in Poncet et al. (2018).
Other treatments delivered through KRTs
In the group of studies in which the aspect under investigation was delivered through a KRT but not inherently related to the KRT, the RCT by Eakman and Nelson (2001) provided moderate-level, moderate-quality evidence that hands-on meal preparation training in inpatients with CVA led to better recall of the recipe than verbal training; the RCT by Liu et al. (2004) provided high-level, high-quality evidence that task training (including KRTs) based on mental imagery in inpatients with CVA led to greater independence in task performance compared to ‘demonstration-then-practice’ training; the RCT by Ownsworth et al. (2017) yielded high-level, high-quality evidence that error-based learning in task training (including KRTs) in community-dwelling patients with TBI led to improvements in the Cooking Task compared to an error-less learning approach; the RCT by Schmidt et al. (2013) provided high-level, high-quality evidence that KRT training with video and verbal feedback in inpatients with TBI achieved KRT performance with fewer errors than training with verbal or experiential feedback alone; and the RCT by Trevena-Peters et al. (2018) yielded high-level, high-quality evidence that ADL training (based on error-less learning and including KRTs) in inpatients with TBI and post-traumatic amnesia led to Functional Independence Measure improvements in a greater proportion of patients compared to usual care. The single case series by Gasser-Wieland and Rice (2002), McGraw-Hunter et al. (2006), and Paul (1997) yielded low-level and low- to moderate-quality evidence for their respective treatments and patient groups, with findings of improved upper limb kinematics (Gasser-Wieland and Rice, 2002), improved performance of a KRT (McGraw-Hunter et al., 2006), and improved scanning time and accuracy (Paul, 1997).
KRTs as assessments
In the group of studies that investigated the use of KRTs for the assessment of safety and/or capability of task performance, the study by Robnett et al. (2016) provided moderate-level, moderate-quality evidence of moderate and statistically significant correlations between the Safe at Home Screening score, the Kohlman Evaluation of Living Skills score, and the treating occupational therapist’s judgement on participants’ functional independence and home safety in ABI patients in a community setting. The study by Tanguay et al. (2014) yielded low-level, moderate-quality evidence that performance in a computerised breakfast task correlated poorly with performance in real-world meal preparation in inpatients with ABI.
Discussion
Seventeen primary research studies that evaluated the use of KRTs as an intervention within occupational therapy for adults with ABI were identified and their results summarised. The value of KRTs in various forms for brain injury rehabilitation has been considered within the literature, with a wide range of outcome measures used to report their impacts. This systematic review provides an overview of the available literature with a description of investigators’ approaches and study designs, and an appraisal of methodological quality and levels of evidence.
The review covered a heterogeneous group of studies that used KRTs as a key component of occupational therapy interventions towards a range of outcomes in people with brain injury, both in their task performance and specific motor or cognitive impairments. Results of the studies included in this review suggest diverse levels of certainty regarding the effectiveness of KRT interventions. Due to the heterogeneity in study design, purpose, design of KRT interventions, and selection of outcomes, each study included in this review should be interpreted on its own merit.
When setting out to conduct this review, the intention was to identify the evidence for using KRTs in the rehabilitation of ABI, as compared to other non-KRT-based interventions. However, a number of studies were also included in the review that did not use KRTs as the actual ‘active ingredient’ under investigation, but which used KRTs as the activity or ‘setup’, with a different focus, such as the comparison between error-less and error-based learning approaches in the study by Ownsworth et al. (2017). These types of studies made up almost half (8/17) of the included studies. Although these studies did not investigate the effectiveness of KRTs in rehabilitation per se, they were considered as relevant for this review and provided a more comprehensive overview of the currently available literature. These studies also provided evidence of the widespread use of KRTs in occupational therapist-led rehabilitation of adults with ABI.
KRTs as treatments
Most studies (15/17) focused on improving cognitive and physical functions, or task performance through KRT-based treatments. Of these, five studies compared KRT treatments to non-KRT treatments or usual care; however, these studies varied greatly in terms of the intended outcomes, such as restoration of cognitive deficits (Cerasa et al., 2019) and effect on constructional abilities (Neistadt, 1992a), and the use of measures in line with the intended outcomes. Most of these studies scored low in methodological quality (one RCT). Two further studies only provided detailed descriptions of KRT activities but did not include an investigation of effectiveness (Foxhall and Gurr, 2014; Patterson et al., 2017). This provided very limited opportunity to synthesise the evidence to describe the actual effect on functional abilities, thereby contributing to limited confidence in the evidence towards the effectiveness of KRT-based treatments for improving function or task performance in patients with ABI.
In eight studies, the aspect under investigation was delivered through a form of KRT as part of the treatment, but not inherently related to the KRT. In other words, these interventions could also have been delivered through other functional tasks. Three studies explicitly proposed the use of KRTs as meaningful, occupationally embedded activities for their therapeutic value compared to other ADL (Eakman and Nelson 2001; Gasser-Wieland and Rice, 2002; Neistadt, 1992a). Consistent with the literature, this supports the perception that KRTs form a major part of activity-based treatments for improving performance in instrumental or extended ADL. As occupational therapy emphasises interventions designed to achieve the functional outcomes necessary for dwelling in a given socio-cultural environment (Legg et al., 2007), KRTs are used as a key activity in treatments aiming to improve skills for independence in preparing meals for oneself.
Occupational therapy is a complex intervention and forms an established and essential element in the rehabilitation of patients with ABI to promote health, prevent disability, and restore the highest possible level of independence (COT, 2013). Despite this, there have been few studies of the nature and effectiveness of activity-based interventions provided by occupational therapy practitioners and their specific impacts on patient outcomes (Powell et al., 2016). Level of dependence in meal preparation is an important measure of the success of rehabilitation and a commonly used functional outcome in brain injury rehabilitation; however, the specific impacts of KRT-based treatments remain to be established.
KRTs as standardised outcome measures
It is acknowledged that cognitive disorders and executive functioning following brain injury are best tested in ecologically valid, naturalistic settings close to real life, using a real task (Poncet et al., 2014). It has been suggested that the clinical usefulness of standardised neuropsychological tests is limited due to their lack of sensitivity to reflect the true impact of cognitive disorders on everyday life tasks (Chevignard et al., 2000; Poncet et al., 2014). In this regard, this review has demonstrated the extensive use of KRTs towards assessment of a range of cognitive, motor, and functional deficits following ABI. Several studies in this review used standardised and validated assessment tools such as the RKE-R (Neistadt, 1992a), the Cooking Task (Chevignard et al., 2000), and the Kettle Test (Hartman-Maeir et al., 2009). These assessments use a KRT as the main task to systematically assess individuals’ levels of task performance and to identify deficits. However, these measures are not very widely used and are constructed to test various aspects of KRT, such as cognitive deficits (Kettle Test), executive function (Cooking Task), and skills for meal preparation (RKE-R). Moreover, there are only a few studies on the reliability, validity, and clinically important difference of these measures. Hence, the current evidence suggests that there is a lack of well-validated standardised outcome measures for KRT intervention studies that can reliably report a clinically meaningful change in the participants’ ability to complete a meal preparation task.
Standardised home safety assessments
Although KRTs commonly form part of standardised assessments for home safety, the review has not identified any evidence that a standalone KRT-based assessment could predict the safety of the person at home post discharge. A variety of cognitive deficits resulting from ABI can directly affect safety for living in the community and occupational performance in a variety of tasks (Eriksson et al., 2006). Therefore, it is common practice in occupational therapy to assess for potential safety issues in function through both informal and formal assessments (Robnett et al., 2016). Only two studies were identified where KRTs were used for this purpose in individuals with ABI. One study demonstrated the limitations in substituting a computerised KRT for actual meal preparation (Tanguay et al., 2014); another established the potential value and validity of the Safe at Home Screening, a quick assessment tool for safe living skills in patients with ABI (Robnett et al., 2016). In the Safe at Home Screening, a mock hazardous situation is set up in a kitchen setting. This could provide a standardised tool for occupational therapists to assess home safety in patients with ABI and guide discharge planning; however, no study was found that investigated its effectiveness for clinical outcomes such as reduction of adverse events post discharge. The literature also describes other in-depth standardised assessment tools for assessing safety, such as the SAFER, the Westmead Home Safety Assessment (WeHSA), the Home Falls and Accidents Screening Tool (HOME FAST), the CASPAR, the Housing Enabler, and the Kohlman Evaluation of Living Skills (KELS) (Robnett et al., 2016). A general disadvantage of these tools is their lengthy assessment process.
Limitations
The main limitation of the review relates to the high level of heterogeneity of the studies, restricting the reviewers’ ability to compare and pool the evidence. Many studies had small sample sizes with weaker methodologies (for example case reports/series) and short intervention periods with no long-term follow-up. Variations in the appraised studies must be considered when interpreting the results. Another limitation relates to heterogeneity in the original study authors’ descriptions of KRT-based interventions. While some authors have given relatively detailed descriptions of their KRT interventions within articles or in referenced intervention protocols and manuals, the level of detail provided by others is rather sparse. It may be recommended that future studies make use of the Template for Intervention Description and Replication (TIDieR) reporting guideline for complex interventions (Hoffmann et al., 2014), to provide comprehensive intervention descriptions that will allow replication by other investigators. Lastly, non-English publications were excluded, and it is possible that relevant study reports published in other languages were missed.
One of the strengths of the review was the use of a comprehensive search strategy, which included searching in occupational therapy-specific databases and grey literature. This resulted in a large number of studies considered for review. In addition, a rigorous and explicit approach was applied to identifying, appraising, and synthesising this heterogeneous and complex body of literature in a concise manner.
Implications for occupational therapy
Although there have been several studies of instrumental ADL training for people who have had a stroke and are living in the community (Walker et al., 2004), there has not been a previous review of the effectiveness of KRTs specifically for the rehabilitation of people with ABI. The review adds to the literature by reporting on the use and effects of occupational therapy-focused KRTs in patients with ABI. These results have several implications for practice, education, and research.
Although there is evidence for some applications of KRTs in clinical practice, the effectiveness of KRTs is not fully established for rehabilitation of specific performance components after ABI. Hence, practitioners should be cautious in applying KRTs in occupational therapy treatments and assessments with this cohort, especially for the purpose of determining discharge recommendations. On the basis of the evidence, educators and practitioners are encouraged to seek relevant evidence in broader studies about KRTs in mixed or other similar patient groups. Practitioners may consider the results column in Table 3 of this review along with the quality assessment provided in Online Appendix 3 for detailed practice information.
Further work is required to define the actual benefits of using KRTs as an intervention. Economic studies are also required to examine the cost-effectiveness of using kitchen-related activities for occupational therapy interventions, especially within acute rehabilitation settings. The role of KRTs in determining safety for discharge requires further investigation. Although it has been established that occupational therapy as a package of interventions is effective (Legg et al., 2007), further research is needed to better understand specific components within this, for example the effectiveness of KRT-based interventions for improving long-term functional outcomes for people with ABI. Larger sample sizes with randomised allocation to intervention will permit further analysis of the impact of the intervention.
Conclusion
This review has identified literature to demonstrate that KRTs are used in various forms as part of occupational therapist-led rehabilitation for people with ABI, both for therapeutic assessment and as treatments for improving specific impairment or occupational performance. However, heterogeneity between included studies and partly low methodological quality complicate the interpretation of findings. Judging from this body of evidence, the effectiveness of KRT-based interventions for improving clinical and functional outcomes remains to be established. Hence, practitioners should be cautious while using KRTs as occupational therapy interventions for ABI and seek further clarification of purpose. In addition, detailed description, such as a protocol for using KRT interventions, should be encouraged. Further research is warranted to address limitations of previous studies and generate more definitive results.
Key findings
Literature reflected the use of KRTs in common practice in occupational therapy for ABI rehabilitation, both for assessment and treatment. There is limited evidence of occupational therapist-led KRTs as an effective intervention for ABI rehabilitation due to heterogeneity of intervention design and methodical quality of available studies.
What the study has added
The study provides evidence on the continuing use of KRTs in occupational therapy interventions for brain injury rehabilitation along with other functional activities. However, the effectiveness of KRT-based interventions in restoring specific deficits remains to be established.
Supplemental Material
sj-pdf-1-bjo-10.1177_0308022620950975 - Supplemental material for Kitchen-related tasks used in occupational therapy during rehabilitation of adults with acquired brain injury: A systematic review
Supplemental material, sj-pdf-1-bjo-10.1177_0308022620950975 for Kitchen-related tasks used in occupational therapy during rehabilitation of adults with acquired brain injury: A systematic review by Sushmita Mohapatra and Stefan Tino Kulnik in British Journal of Occupational Therapy
Footnotes
Research ethics
Ethics approval was not required for this study. This study was registered with the International Prospective Register of Systematic Reviews (PROSPERO): registration number CRD42019141898.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Contributorship
Both the authors have equally contributed to the study and consent to the authorship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.