
Abstract
Introduction
The clinical benefits of 24-hour postural management are widely recognised by occupational therapists, but little is known about its impact on service users and carers or whether clinical practice is consistent across regions. The aim of this research was to investigate the use of 24-hour postural management by occupational therapists and to explore its impact on service users with neurodisability and their carers.
Methods
Quantitative and qualitative methods were employed in two phases: (a) online survey with 96 occupational therapists across one UK region, with data analysed by descriptive statistics and correlations; (b) focus groups with service users and/or carers (n = 9), with data analysed by thematic analysis.
Results
Findings showed moderate positive correlation between frequency of use and (a) all key intervention skills and (b) knowledge of night-time positioning (p < 0.001). Moderate positive correlations were found between level of training and (a) assessment skills and (b) knowledge of night-time positioning (p < 0.001). The overarching theme from focus groups was ‘reliance on individualised equipment’, with overwhelming frustration from lack of support, loss of identity, equipment cost, insufficient focus on preventative strategies and accessibility issues.
Conclusion
A clinical practice guideline, including training, is crucial to direct practice. Providers must engage with service users and carers to address their frustrations.
Introduction and review of literature
Expert consensus has defined neurodisability as ‘a group of congenital or acquired long-term conditions that are attributed to impairment of the brain and/or neuromuscular system and create functional limitations’ (Morris et al., 2013). Muscle imbalance and spasticity are common features, leading to asymmetry, pain, contractures and poor postures, and reduced participation in everyday life (Crawford and Stinson, 2015). Neurodisability is a global problem affecting individuals across the lifespan, and includes conditions such as cerebral palsy, spina bifida, spinal cord injury and multiple sclerosis. Such conditions are not only associated with chronic disability but with rising worldwide mortality rates that are set to steeply increase with growing and ageing populations (GBD, 2019). The documented global burden of neurological disorders demands that health providers offer more effective treatment and preventative strategies to reduce mortality and minimise the impact of significant disability (GBD, 2019).
Twenty-four-hour postural management is both a treatment and preventative strategy used by occupational therapists to address body positions over a 24-hour period to optimise function and minimise disability (Hutton and Coxon, 2011; McDonald and Surtees, 2007; Maher et al., 2011; Wynn and Wickham, 2009). It usually involves provision of adaptive seating and/or moulded wheelchairs, orthoses, night-time positioning equipment (also known as ‘sleep systems’), showering equipment and occasionally standing frames. Moving and handling techniques and training care staff, professionals and family are also essential components (Humphreys and Pountney, 2006; Hutton and Coxon, 2011; Maher et al., 2011). As such, the intervention considers the environmental context (Gough, 2009), providing individualised, comprehensive 24-hour postural management programmes (Maher et al., 2011; Wynn and Wickham, 2009). Over the last 2 decades there has been increasing awareness and emphasis on the clinical importance of 24-hour postural management (Clarke et al., 2014; Goldsmith, 2000; Humphreys and Pountney, 2006; Pountney et al., 2002) to facilitate musculoskeletal alignment, function and participation in everyday life (Farley et al., 2003; Stephens et al., 2018).
However, despite the recognised clinical benefits there is a lack of robust, high quality evidence to fully support this often costly intervention (Humphreys et al., 2019; Gmelig Meyling et al., 2018; Robertson et al., 2016). Due to the individualised nature of 24-hour postural management, the use of a randomised controlled trial design may not be the most appropriate or achievable method to evaluate its effectiveness (Humphreys et al., 2019; Gmelig Meyling et al., 2018).
Although the evidence base for 24-hour postural management continues to grow (Hotham et al., 2017; Meyling et al., 2018; Picciolini et al., 2016; Stephens et al., 2018), not enough is known about current practices in its use and its actual impact on the everyday life of individuals and carers (Nicolson et al., 2012; Robertson et al., 2016). Indeed, there has been acknowledgement of this important gap in evidence and a subsequent shift towards use of qualitative and/or mixed methodologies (Goodwin et al., 2018a, 2018b, 2019; Hotham et al., 2017). The current study was therefore designed to address this gap.
Aims
Study aims were as follows: To examine current use of 24-hour postural management within occupational therapy clinical practice across one region of the UK. To explore the impact of 24-hour postural management on service users with neurodisability and their carers.
Methods
This two-phase study comprised qualitative and quantitative methods, as deemed appropriate for examining complex health-related interventions (Palinkas et al., 2015). Phase 1 comprised an online survey investigating the current use of 24-hour postural management among occupational therapists, the healthcare professional group predominantly involved with postural management within this UK region. Phase 2 used focus groups to explore the impact of 24-hour postural management on service users with neurodisability and their carers. Appropriate ethical and research governance approvals were obtained through the Health Research Authority Research Ethics Committee in 2017 (Ref: 17/WA/0199).
Phase 1
Following a literature review and consensus discussion among the research team, an online survey was employed to explore the clinical implementation of 24-hour postural management by occupational therapists across a selected UK region. The survey was initially tested using 10 occupational therapists to ensure face and content validity. The survey questionnaire, devised using Survey Monkey®, explored the following: respondent demographics; understanding and experience of 24-hour postural management; training; perceived knowledge and skills; and facilitators or barriers to its clinical use. A combination of open and closed questions was included, taking approximately 10 minutes to complete.
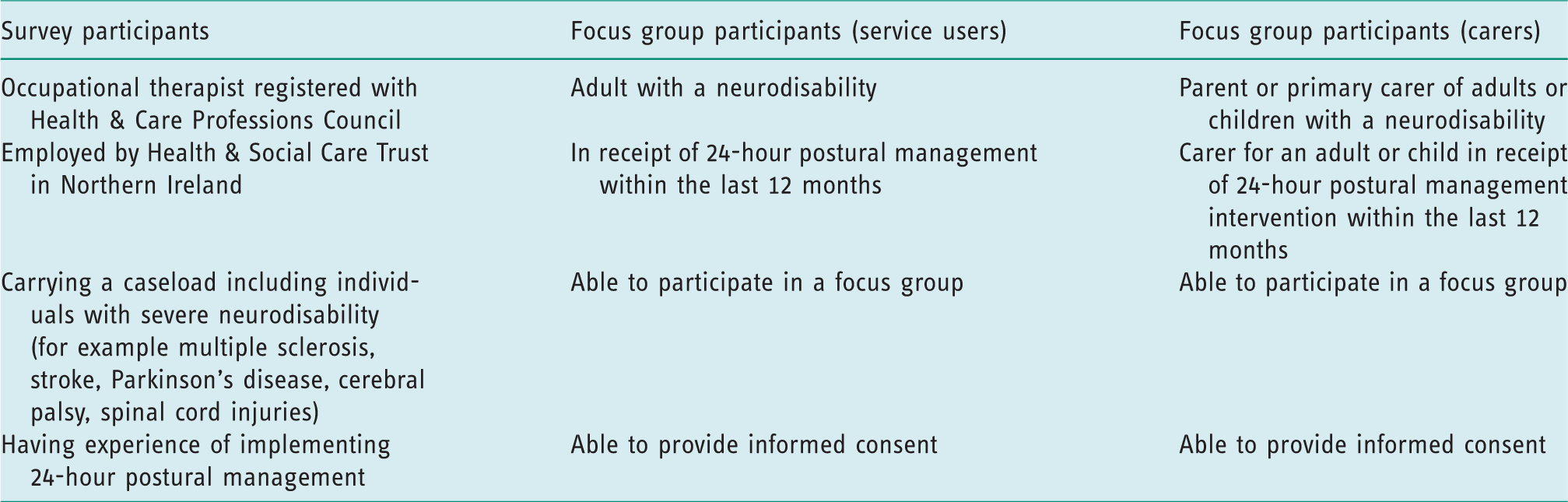
Purposive sampling was used to recruit occupational therapists with relevant experience in 24-hour postural management. Within this UK region there are approximately 980 full-time equivalent employed occupational therapists (Department of Health, 2019), a significant proportion of whom work in settings where patients have minimal physical needs; therefore, the exact number of eligible participants was unknown. The inclusion criteria for occupational therapists are presented in Table 1. Those not meeting the inclusion criteria were excluded. Potential participants were identified via professional leads within relevant programmes of care, including acute, community, paediatrics, rehabilitation and specialist services. Each potential participant was invited by email, with a participant information sheet included. Those meeting inclusion criteria and interested in participating were asked to complete the secure, anonymous online survey. Consent was implied by completion.
Inclusion criteria for survey and focus group participants.
Phase 2
Service users with neurodisability and/or their carers were also recruited by purposive sampling to ensure the study findings were based on the views of ‘information rich’ informants (Palinkas et al., 2015). All were identified from caseloads of occupational therapists providing wheelchair services within a single healthcare trust. The wheelchair service assesses individuals with severe neurodisability who rely heavily on the implementation of 24-hour postural management. Inclusion criteria for service users and carers are presented in Table 1. Those not meeting inclusion criteria were excluded. Written invitations were mailed to potential participants and informed consent was obtained by a research team member (MS). To facilitate open discussion, no service user and their carer were invited to the same focus group.
Two focus groups (n = 4 and n = 5) were held in accessible locations. Both were chaired by an experienced focus group moderator, who was not an occupational therapist in order to limit bias. Two research team members (MS and EM) were present to audio record the discussions and take field notes (for example body language). A pre-determined question schedule explored the following aspects of 24-hour postural management: participants’ understanding and experiences; use of equipment; education and support; benefits and drawbacks. Probing was used where appropriate. A written summary of findings from each focus group was sent to participants for member checking. Audio recordings were transcribed verbatim and independently checked for accuracy by MS and SC. Field notes were added to transcripts.
Semi-structured interviews had been considered and may have enhanced recruitment; however, the researchers believed that group interaction and the richness of discussion would more fully explore this under-researched area.
Data analysis
Phase 1
Data were entered into the Statistical Package for Social Science Version 25 (IBM Corp., 2017) and cleaned before analysis. Ten percent of questionnaires were independently checked for accuracy by a research team member (MS), based on a study by Blackburn et al. (2018). Analysis of closed questions included descriptive statistics, calculating percentages and frequencies. In addition, Spearman’s Rho was used to investigate correlations between knowledge, skills and the following: years of clinical experience as an occupational therapist, years of experience implementing 24-hour postural management, frequency of use, and level of training in 24-hour postural management. Free text responses from open questions were coded into categories by one research team member (SC) and independently verified by another (MS).
Phase 2
Focus group data were analysed using the staged thematic analysis method (Braun and Clarke, 2006). This flexible method is appropriate for under-researched areas, where participants’ views may not be well known (Braun and Clarke, 2006; Devery et al., 2018).
Stages 1 and 2: data familiarisation and initial coding
Transcripts were read multiple times and coded manually and independently by two researchers (SC and MS). An inductive, semantic approach was used to generate ‘data driven’ themes.
Stages 3, 4 and 5: searching for themes, reviewing themes, refining and naming themes
A consensus meeting considered each researcher’s analysis. Emerging codes were discussed and agreed. Quotations were grouped together under each code. In a further consensus meeting, similar codes were grouped together to develop agreed themes and subthemes. Although the above linear stages were used as a framework, in reality the process was iterative and reflexive, coding and re-coding before moving to further analysis. This ensured developing themes were grounded in the original data.
Reflexivity and trustworthiness
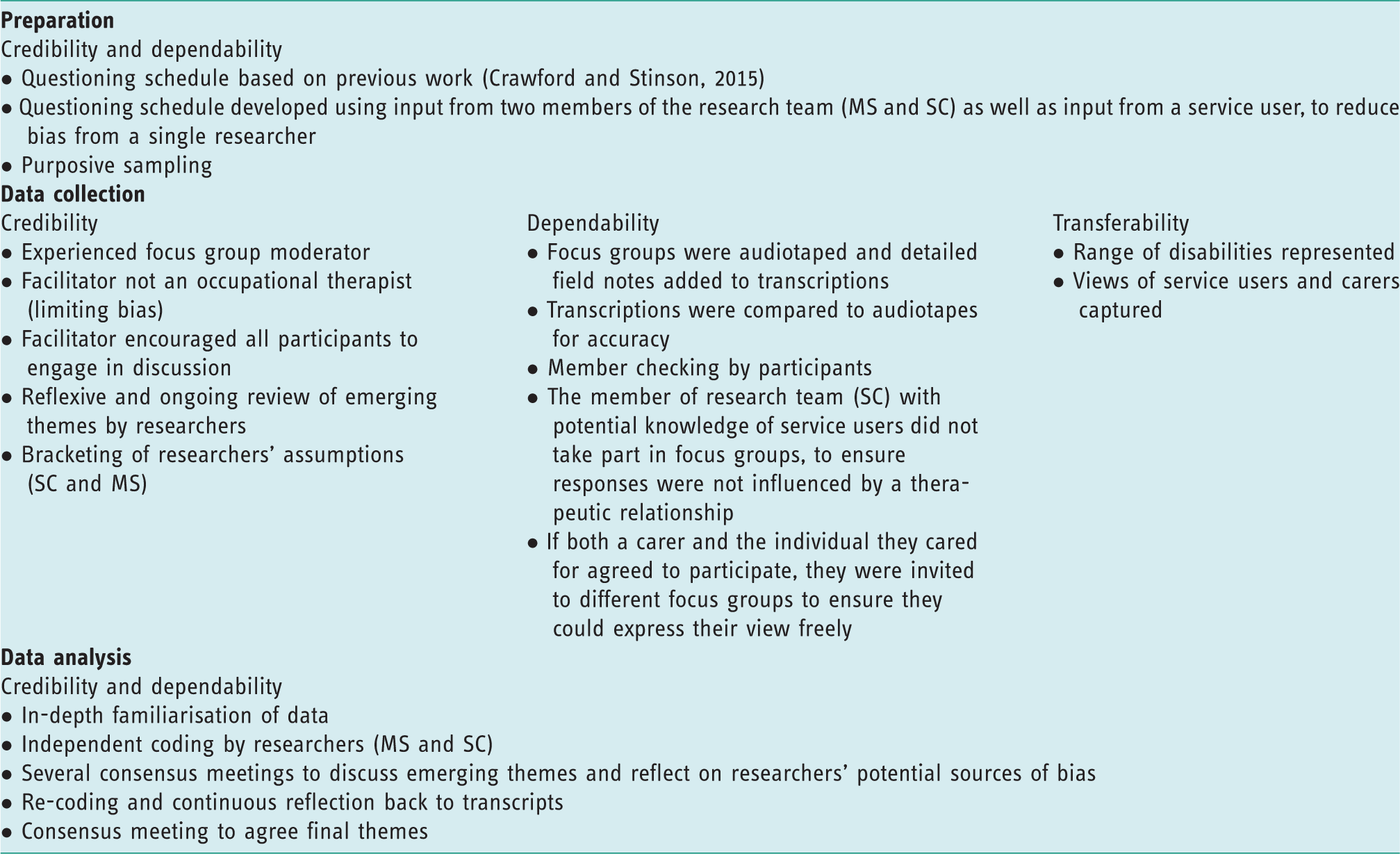
The researchers continuously reflected on their potential bias throughout the study, as both were occupational therapists familiar with current evidence and practice in this field. Their knowledge and experience were also recognised as strengths that allowed in-depth engagement with the data, including the emergence of unexpected themes. Transcripts were continuously referred to, ensuring that interpretations were linked directly to the data. Table 2 shows strategies used to promote trustworthiness.
Methods used to promote trustworthiness for focus groups (adapted from Hanratty et al., 2016, with permission).
Findings
Phase 1: survey
Respondents
Within the 10-week data collection period, 102 occupational therapists returned the online survey. Data from six therapists were excluded as they had greater than 50% of responses missing (Stockley et al., 2019), resulting in analysis of data from 96 respondents. The nature of the questions made it inappropriate to force responses; therefore, responses to individual questions are collated based on the number who provided responses.
Practice and experience
The majority of occupational therapists (90%; 84/93) had worked clinically for more than 5 years, with 77% (72/93) having at least 10 years’ experience. Respondents worked in a variety of clinical areas, including physical disability (25%; 24/96), older adults (19%; 18/96), learning disability (10%; 10/96), paediatrics (10%; 10/96) and stroke (10%; 10/96). Most were community based (75%; 69/92), with 22% (20/92) based in hospitals. A significant proportion (81%; 62/77) reported having at least 3 years’ experience in implementing 24-hour postural management, and 65% (50/77) had 5 or more years’ experience. Sixty-eight percent of occupational therapists (65/96) completed a 24-hour postural management assessment once a month or less, 10% completed them once a fortnight and 22% completed them at least once a week.
Understanding of ‘24-hour postural management’
Analysis of an open-ended question on the occupational therapists’ understanding of the term ‘24-hour postural management’ showed the majority (n = 90/96) had a good understanding, identifying key components including managing positioning both day and night and use of specialised equipment. The remaining therapists were unable to fully define it, either in relation to its application to lying, sitting and standing postures or to the inclusion of appropriate equipment and advice. The most prevalent category to emerge was ‘sitting and lying’. The majority of respondents understood that both these postures required management over the 24-hour period. Ten therapists addressed standing posture. The second emerging category was ‘purpose’ as many occupational therapists showed awareness of what postural management aimed to achieve.
Training
A substantial number of respondents (n = 56/96) had not received postgraduate training in 24-hour postural management within the previous 5 years. Of those who did, training included Master’s level modules in complex seating and/or pressure ulcer prevention (n = 22), healthcare trust training courses (n = 8), in-service/company representative sessions (n = 7) and other relevant training (n = 3).
Knowledge and skills
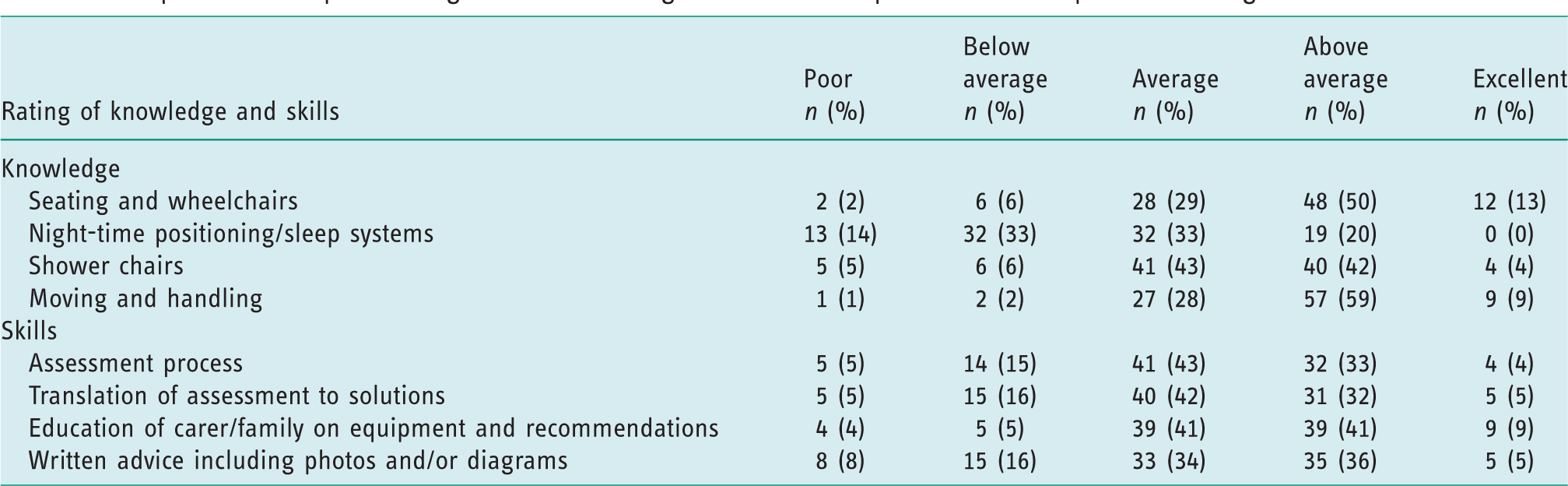
The occupational therapists’ rating of their knowledge and skills across key aspects of 24-hour postural management are detailed in Table 3.
Occupational therapists’ rating of their knowledge and skills of aspects of 24-hour postural management.
Correlations between therapists’ experience and training and their knowledge and skills are presented in Table 4. The frequency of use of 24-hour postural management showed positive correlations with knowledge of both complex seating/wheelchairs (r = 0.207, n = 96, p < 0.05) and night-time positioning (r = 0.400, n = 96, p < 0.01), and moderate positive correlations with all skills explored: assessment (r = 0.511, n = 96, p < 0.01), translating assessment into solutions (r = 0.502, n = 96, p < 0.01), educating carers (r = 0.411, n = 96, p < 0.01) and providing written advice to carers (r = 0.435, n = 96, p < 0.01). The level of training in 24-hour postural management showed moderate positive correlations with knowledge of night-time positioning (r = 0.396, n = 96, p < 0.01) and skills in assessment (r = 0.343, n = 96, p < 0.01), and weak positive correlation with providing written advice (r = 0.217, n = 96, p < 0.05). Years of experience working as an occupational therapist showed no correlation with knowledge or skills in 24-hour postural management, and years of experience using 24-hour postural management showed minimal correlation (see Table 4).
Spearman’s Rho correlations between knowledge and skills and other factors.
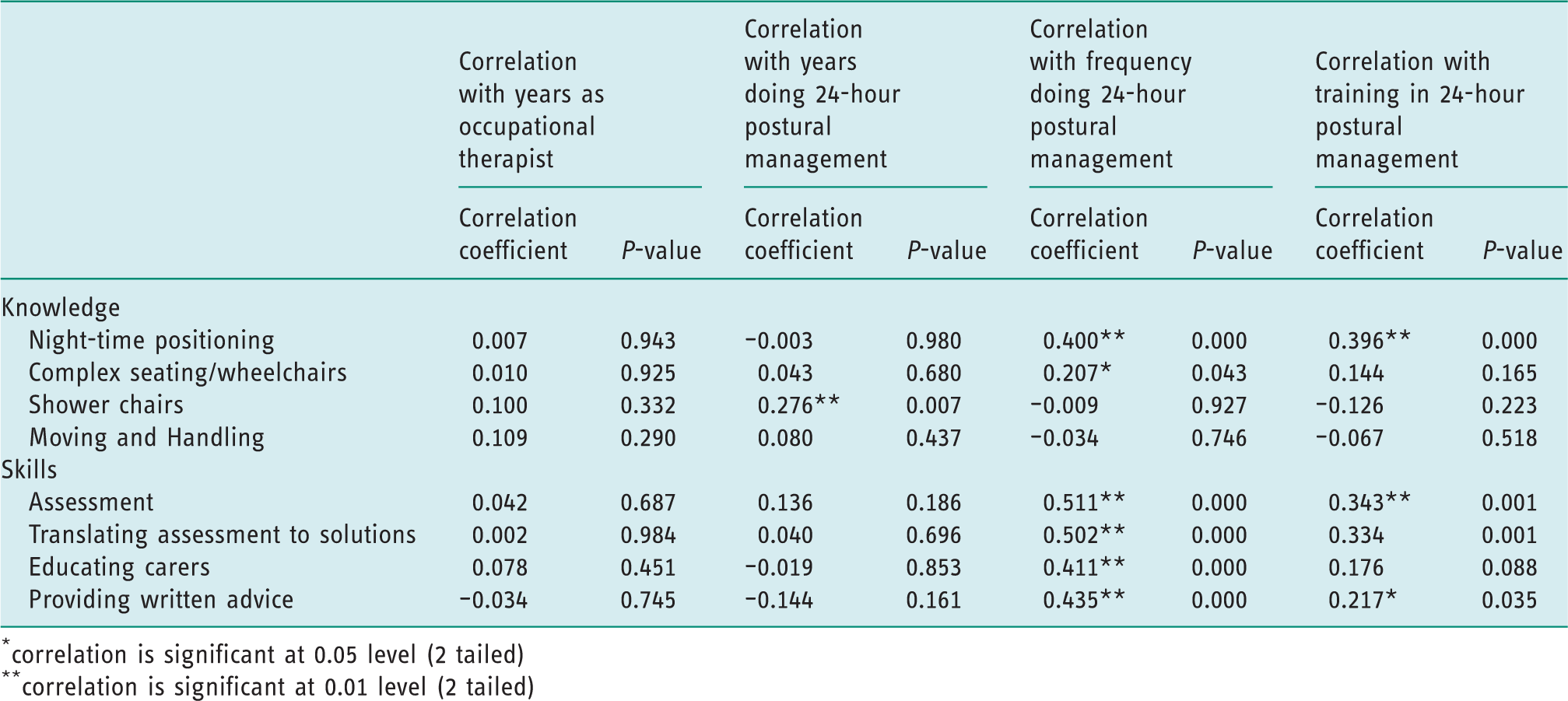
correlation is significant at 0.05 level (2 tailed)
correlation is significant at 0.01 level (2 tailed)
Facilitators and barriers to implementing 24-hour postural management
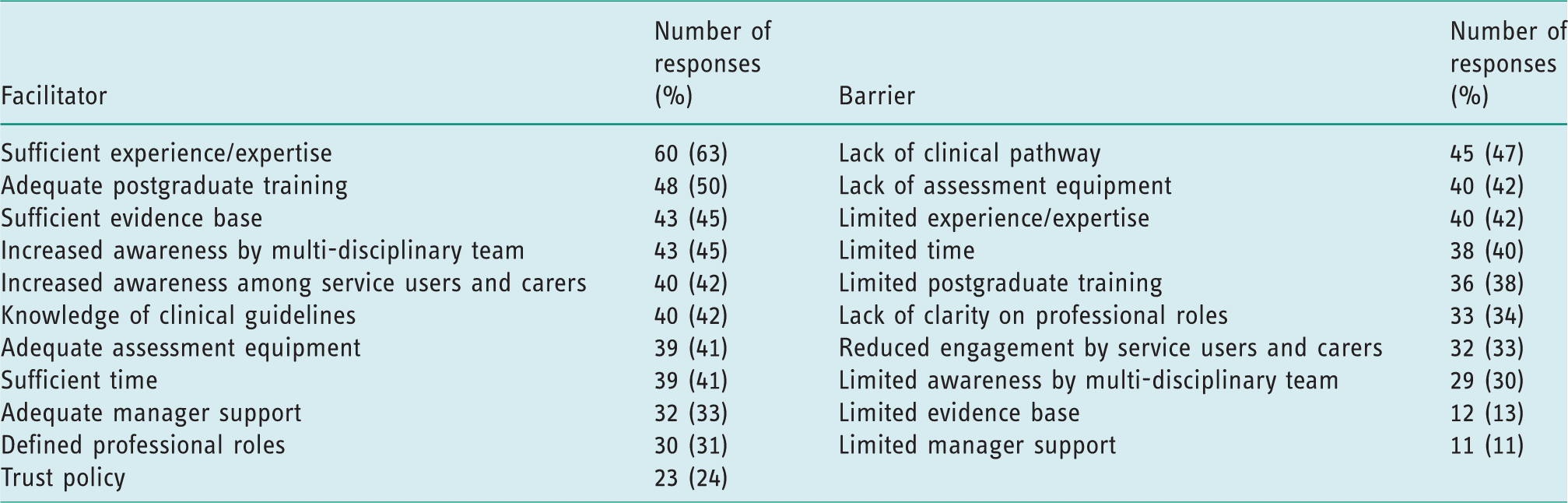
Respondents selected facilitators and barriers to implementing 24-hour postural management in relation to process, equipment, roles, support, time, expertise and training (see Table 5). The most frequently reported enabling factors were having sufficient experience/expertise and adequate postgraduate training. The most common barriers were lack of a clinical pathway for 24-hour postural management, lack of assessment equipment and limited experience/expertise.
Facilitators and barriers to 24-hour postural management.
Phase 2: focus groups
Eighty-five people were invited to take part in focus groups, 11 of whom consented to participate. Two subsequently withdrew for personal reasons. The first focus group included three service users and one carer (three female, one male) and the second focus group included two service users and three carers (two female, three males). All carers bar one were caring for a child. Each focus group lasted between 60 and 90 minutes.
Overarching theme: reliance on individualised equipment
Service user is abbreviated to SU and carer to CR.
Participants deemed the equipment as an absolute necessity, as without it, ‘we’d be left not able to move from bed’ (SU1). One participant stated, ‘well, I need a mould. I wouldn’t be able to sit without it’ (SU2). Not having access to the equipment, particularly their wheelchairs, left many feeling totally dependent and helpless: ‘If this thing [wheelchair] is away from me, or (like) if someone left it out of my reach, I’d feel naked. (Like) it’s me legs now’ (SU3).
Theme 1: enabling function and empowerment
Within this overarching theme, the equipment issued ‘enabled’ those with neurodisability to have a better quality of life: ‘I know it takes a long time to get the equipment and all, but his quality of life now is improved’ (CR2).
The equipment ‘creates independence at the end of the day, ye know’ (SU4) and facilitates participation in meaningful activities as ‘it means I can walk my dog’ (SU3). For one service user, the reliance on this individualised equipment was to facilitate efficient breathing: ‘The position’s right [in a moulded seat], so your lungs are in the right position, you know’ (SU2).
Having the opportunity to make decisions about their equipment was viewed as ‘enabling’ and empowering, and could lead to better outcomes for their wheelchair provision. I feel much more part of my care now (and all), what you would be calling the 24-7 so I felt I was a lot more involved in the decision making. I would feel I now have a chair that is probably the best fit (SU4).
Theme 2: frustrating impact of reliance on 24-hour postural management equipment
Despite the positive acknowledgements about the necessity of the equipment and its enabling benefits, the need to rely on individualised equipment as part of 24-hour postural management emerged as predominantly frustrating for many of the service users and their carers. One participant highlighted her frustration at the lack of personalised information provided in relation to her child’s care: ‘When they are giving you an answer it’s like they are taking it out of a text book rather than relating it to the person in front of them’ (CR1).
Subthemes within this overwhelming sense of ‘frustration’ included lack of support and training, waiting times for equipment and repairs, costs of equipment, lack of accessibility for wheelchair users, lack of a focus on prevention and a sense of loss of identity due to reliance on individualised equipment.
Subtheme 2a: lack of support from professionals
From the outset, it became apparent that occupational therapists were the professional group most involved in postural management and therefore the profession with whom participants had most engagement. The support received from occupational therapists was generally regarded as positive; however, at times frustration emerged at not being able to contact the occupational therapist. [Occupational therapists held in] high regard (SU3). [Occupational therapists are] really good (CR2). They are hard to get (SU1). They are, aye, very hard (CR1). I’ve been asking about a sleep system as well but nothing (SU2). Aye, it seems to be as long as it’s nine to five, with them; and I’m not being critical but within the [occupational therapist’s] nine to five day, that seems to be what they are concerned about with regards to the person as well (CR1).
Subtheme 2b: lack of support/training for carers
The lack of support from formal care companies was highlighted a number of times, mainly in relation to appropriate positioning of individuals. It was felt that they were ‘not being trained enough’ (SU3) and this clearly impacted on parents and service users. But the problem I find, [be]cause I have domiciliary care for my wee girl as well … they do a fantastic job but they haven’t been properly trained as to, you know, they have been trained through their organisation but there hasn’t been any real input from [occupational therapists] or anything to say, ‘alright, do you know what’s the best position for her to be in?’ I’m shown, but I’m not qualified. I’m her mother (CR1).
It became clear that if formal carers do not position the individuals correctly, it can have an immense impact on their ability to participate in even the most basic everyday tasks, creating a sense of dependency and helplessness: ‘I would need to be straight up in the chair, you know, because if I’m not sitting right, there’s nothing I can do’ (SU1).
Subtheme 2c: loss of identity
There was general agreement that dependency on carers and individualised equipment often led to a loss of identity. Service users commented that attention was too often focused on the carer, rather than addressing the individual and considering their views and wishes: ‘When someone’s like that, I’m like, “I’m here too. You can talk to me”’ (SU3).
There was also a sense of disappointment that individuals and/or their parents felt like they were on a conveyor belt when engaging with some services; one participant stated it was ‘just like rushing you out the door again, ye know’ (CR2) before the next client was brought in.
Subtheme 2d: lack of a preventative approach from health providers
Twenty-four-hour postural management focuses on preventing postures from getting worse. However, the impact of only addressing the sitting position at the detriment of lying was noted. One focus group participant highlighted that a similar amount of time is habitually spent sitting as lying and ‘if it’s not maintained… they are going to deteriorate’ (CR1). Another participant felt that once the spine had curved, there was no desire from health professionals to intervene to manage this: ‘Once you have a scoliosis they leave that too, they don’t want to manage your posture too much’ (SU2).
Subtheme 2e: long waiting times
Waiting times for equipment caused considerable frustration for participants, mainly in relation to lower limb splints and wheelchair repairs. Their sense of frustration was heightened when the equipment caused pain or inconvenience. So after the 7 months, we went, we got them [splints] on him and they hurt him, they had to be changed, they had to be moulded on him again and things like that. We waited another 3 months to get them back and I thought this is just horrendous. This is like a year before, he didn’t even want them back on his feet again (CR3). That’s another thing too, like [name of son]’s wheel buckled on his chair and he had to wait up to 10 days for a call out to come and see… I told him, I said, ‘He doesn’t have a spare chair’ [voice raised] (CR4).
Subtheme 2f: the burden of equipment cost
Frustrations regarding the cost of the individualised equipment varied from ‘feeling guilty for needing a mould’ (SU2) to feeling sorry for the health service due to ‘companies… taking the hand out of the national health’ (SU3) and holding them to ‘ransom’ as the ‘buying power should be in health’ (SU4). There were also feelings of frustration resulting from the fact that service users were often being informed of the costs associated with this essential equipment. I have to say this past year or so that’s all I hear, when I’m asking for anything… is ‘money money money’; and as real as that is, it shouldn’t be put on us or the people we care for to worry whether there is going to be funding for a piece of equipment. That should… be for the [occupational therapist’s] managers to decide without saying it to us, I feel (CR1).
Subtheme 2g: lack of accessibility for wheelchair users
There was general agreement that reliance on individualised equipment led to issues with accessibility. This caused considerable frustration and was frequently mentioned across a wide range of environments. The issues ranged from ‘it’s almost impossible to find an employer that would have a hoist and all’ (SU2) to ‘not many hotels have hoists’ (SU2), thus impacting on holidays. Accessing the local city was also described as a stressful task, resulting in parents and carers not wanting to take the service user out. …sure go up the town and you’re planning, and you’re getting him into the car, what to take, where am I going to have to park? [Name of city] is not designed for wheelchairs. How will I get him here and here? (CR2).
Theme 3: fear regarding equipment failure and future health needs
The concept of fear was frequently mentioned, permeating a range of areas including equipment failure, for example: ‘the threat of a battery running out., because I’d be stuck’ (SU3), fear of not ‘properly securing’ the equipment (CR1), to pressure ulcer risk as ‘it can be really dangerous’ (SU3). There were fears around trying something new like a moulded seat in case it was ‘too restrictive’ (SU1). Several others had fears that if posture was not managed effectively surgery may be required, and this was a real concern ‘as it [surgery] would set him right back’ (CR3). One carer also had fears relating to her own health: ‘My biggest fear is her night-time positioning. Because I also have a heart condition myself, so I’m moving her on my own’ (CR1).
Theme 4: the need to develop strong advocacy roles
Service users and carers were not only aware of the importance of good positioning but showed awareness of broader issues relating to physical disability. This awareness, along with the above-mentioned frustrations, often led to participants emerging as strong advocates. They had become accustomed to struggling with disabilities and wider social issues, such as having to ‘fight and fight and fight to get him swimming’ (CR2); having ‘to change care companies’ to get the right care (SU2) and pleading for the right equipment, asking ‘can we try something else?’ (CR2). This sense of advocacy often left carers and service users feeling like they were ‘begging for stuff’ (CR4). Parents in particular felt the need to ‘argue’ and ‘fight’ for change, to ensure that input best met their child’s needs. My parents fought that battle for me which meant they had to put ramps into the school [be]cause there actually was no access before I went to it. So they actually had to put ramps into the school. Otherwise there was zero access. That’s how bad it was back then (SU4).
Discussion
The first aim of this study was to examine current occupational therapy practice in the use of 24-hour postural management intervention across a UK region. Survey respondents were experienced occupational therapists, mostly community based. They considered themselves to be most knowledgeable in the areas of complex seating/wheelchair provision, and moving and handling techniques (see Table 3). In contrast, therapists felt least knowledgeable about night-time positioning, an unsurprising finding given that more than half of the therapists (58%) had not received any postgraduate training in postural management within the last 5 years. This was substantiated by a positive correlation being found between therapists’ knowledge of night-time positioning and the level of training they had received (r = 0.396, n = 96, p < 0.01).
Following on from this, it was noteworthy that adequate postgraduate training along with clinical experience were the two most frequently recorded facilitators for implementing 24-hour postural management (see Table 5). Interestingly, no correlation was found between either years of experience working as an occupational therapist or years using 24-hour postural management and knowledge or skills (apart from the knowledge of shower chairs) (see Table 4). These findings emphasise the importance of postgraduate training, rather than years of experience, in the perceived competency of therapists in delivering 24-hour postural management.
The lack of an agreed clinical pathway was the most commonly perceived barrier to the implementation of 24-hour postural management. The findings from this study aim to provide valuable evidence to influence the development of such a pathway as care pathways have been identified as an effective tool for improving service delivery (Humphreys and Pountney, 2006). It was somewhat surprising that lack of experience was rated as one of the most common barriers, yet 81% of occupational therapists had at least 3 years’ experience in implementing 24-hour postural management, with some even having 10 or more years’ experience. One likely explanation for perceived lack of experience is the frequency of implementation, as 68% of respondents reported undertaking 24-hour postural management once a month or less; therefore, they may not have been employing the intervention frequently enough to feel competent in its delivery. In support of this, the largest and most notable correlations were found between the frequency of using 24-hour postural management and therapist skills. Positive correlations were identified with all the key skills explored: assessment, translating assessment into solutions, educating carers, and providing written advice to carers (see Table 4). This data suggests that therapists must ‘use it or lose it’ in terms of 24-hour postural management, and thus targeting therapists who are engaging in 24-hour postural management infrequently warrants careful consideration in the organisation of services.
The second aim of this study was to explore the impact of 24-hour postural management on service users with neurodisability and their carers. This is the first study to examine both carers’ and service users’ experiences of 24-hour postural management as a whole using focus group methodology. Previous studies have addressed certain elements, such as standing frames, and have focused solely on conditions such as cerebral palsy (Goodwin et al., 2018a, 2018b, 2019), while others have addressed the views of parents, teachers and therapists (Hotham et al., 2017; Hutton and Coxon, 2011; McDonald et al., 2007; Maher et al., 2011; Nicolson et al., 2012).
Individuals who require 24-hour postural management will have severe neurodisability, thus it is not surprising that the overarching theme emerging from the focus groups was ‘reliance on individualised equipment’. Service users and their carers relied heavily on equipment to complete even the most basic aspects of daily life, such as getting out of bed and sitting up. It was interesting that the impact of this essential equipment on participants was found to be both enabling and frustrating, similar to findings from other studies (Goodwin et al., 2018a, 2018b, 2019; Hutton and Coxon, 2011). Notably, participants made little reference to the widely perceived physiological benefits of postural management reported in previous studies (Robertson et al., 2016; Vekerdy, 2007), with only one participant acknowledging a positive impact on breathing. Participants prioritised the enabling impact of equipment more in terms of daily participation rather than focusing on alignment of body segments, impairments and physiological impact. This finding is consistent with both the International Classification of Functioning, Disability and Health framework (WHO, 2001) and with the recent research trend of moving away from focusing on body structures and impairment (Gmelig Meyling et al., 2018; Robertson et al., 2016) to prioritising personal preference, broader environmental issues and social considerations.
The overwhelming sense of frustration from reliance on individualised equipment was palpable across the focus groups. Previous studies identified frustrations such as the bulky and restrictive nature of equipment (Hutton and Coxon, 2011; McDonald et al., 2007). The current participants identified additional frustrating factors including loss of identity, the burden of equipment costs, inadequate focus on prevention and wider accessibility difficulties, reflecting the many challenges faced when living with such complex neurodisability (Geuze and Goossensen, 2018; Nicholl and Begley, 2012).
Providing support and training is an integral and fundamental element of 24-hour postural management (Castles et al., 2014; Hotham et al., 2017; Humphreys and Pountney, 2006; Maher et al., 2011), and the current survey found that this was the area wherein occupational therapists felt most skilled. In contrast, the service users and carers found that the training and support they received was inadequate, especially lack of support for night-time positioning. The respondents’ perceived lack of knowledge about night-time positioning and the fact that the majority of therapists had received no recent training in this area may help to explain this incongruence.
Inadequate training in postural management has been highlighted by previous researchers as an issue with parents and teachers in school settings (Goodwin et al., 2018a; Hutton and Coxon, 2011; Maher et al., 2011). Focus group participants in this study also reported inadequate training in correct positioning within care companies, which clearly impacted upon the functional ability and comfort of service users. In addition, the current study highlighted the need to address training and support for families and care companies in order to successfully implement individualised programmes that incorporate day and night-time positioning. Utilising a multi-disciplinary approach to training would be preferable and would reduce dependence on community occupational therapy services.
There is minimal evidence on the impact of postural management on family life (Gmelig Meyling et al., 2018), with researchers calling for more qualitative methods to examine the emotional implications of providing highly specialist equipment (Nicolson et al., 2012). The current study identified important new findings regarding carers’ feelings of fear and parents needing to become strong advocates, which may reflect the broader daily challenges in caring for someone with complex neurodisability (Geuze and Goossensen, 2018; Nicholl and Begley, 2012). Indeed, previous research has echoed parental stress for carers of children with physical disabilities, with Egilson (2011) reporting positive support from therapy services but also frustrations including a lack of consideration regarding the family’s needs and a desire for more information from therapists. Many healthcare organisations have designated care co-ordinators who support primary carers to continue delivering this vital role. It is imperative that health professionals address this sense of fear and empathise with carers’ struggles, so that they can signpost carers to support sources within local communities as well as those available through healthcare organisations.
Study limitations
Due to financial and time constraints, focus groups were only conducted within one healthcare trust. Although no new themes emerged in the second focus group, it cannot be guaranteed that data saturation was achieved and that no new themes would have arisen had further focus groups been conducted; therefore, the findings may not be transferable to service users and their carers across the UK or beyond.
The low focus group response rate (13%) reflects the huge challenges of living with complex neurodisability as the service users, for example, had to arrange for personal paid carers and wheelchair transportation to attend the focus groups. It is imperative to note that these participants are amongst the most physically disabled service users within the healthcare system, and thus it is crucial to have their voices heard. Indeed, the current study is the first to use focus group methodology to explore the views of service users with severe neurodisability directly in relation to their postural care. Focus group numbers were small and this is not uncommon in healthcare research, particularly with groups that are difficult to recruit (Castles et al., 2014). In addition to the challenges faced by service users, the carers found it difficult to find time to engage with the research. Furthermore, carers for children with complex disabilities are reluctant to entrust them to the care of others (Nicholl and Begley, 2012).
Recommendations for clinical practice and future research
The training gap identified needs to be urgently addressed by service providers. Formal carers in particular should be offered training on good positioning. Future research, using qualitative methods, should capture the experiences of service users and families across larger geographical areas, and explore the barriers and facilitators experienced by therapists.
Conclusion
The development of a clinical practice guideline for 24-hour postural management is needed to shape practice. Organisations must engage with service users and carers to help minimise factors associated with frustrations, especially relating to equipment. Training is needed for families and formal care companies around good positioning.
Key findings
Occupational therapists’ skills in 24-hour postural management improve with frequency of use. Reliance on postural management equipment leads to service user and caregiver frustrations that need to be addressed.
What the study has added
This is the first study to explore the experiences of carers and service users with 24-hour postural management as a whole. A clinical practice guideline is needed to shape and further inform practice.
Footnotes
Acknowledgements
We would like to thank Prof Suzanne Martin for her support in the initial stages of this study. We gratefully acknowledge the invaluable insight and advice provided from a service user perspective by the late Mr Michael Heverin. This research would not have been possible without the occupational therapists who took time to complete the online survey, and the service users and carers who undertook considerable planning and effort to attend the focus groups and share their experiences.
Research ethics
Full ethics approval was gained from the Health Research Authority Research Ethics Committee in 2017 (Ref:17/WA/0199).
Consent
Informed consent was obtained from all participants.
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Contributorship
Shelley Crawford and May Stinson contributed to the study design, ethical approval application, data collection (survey), data analysis and drafting of the manuscript. May Stinson and Emma Madden undertook data collection for the focus groups, and Emma Madden contributed to analysis of the survey data.
Funding
This research was funded by a Western Health and Social Care Trust Research and Development Discretionary Fund.