
Abstract
Introduction
Home assessments are integral to the occupational therapy role, providing opportunities to personalise and integrate care. However, they are resource intensive and declining in number.
A 3-month service development within one United Kingdom National Health Service acute hospital setting explored the concept of using digital technology to undertake remote home assessments.
Methods
Four work streams explored the concept’s feasibility and acceptability: real-world testing; user consultations; narrative case study collection; traditional visit resource use exploration.
Project participants were occupational therapists and patient and public representatives recruited via snowball sampling or critical case sampling.
Qualitative data were thematically analysed identifying key themes. Analysis of quantitative data provided descriptive statistics.
Findings
The remote home visit concept was feasible within four specific contexts. Qualitative themes suggest acceptability depends on visitor safety, visitor training, visitor induction and standardisation of practice. Consultees perceived the approach to have potential for resource savings, personalisation and integration of care. Barriers to acceptance included data security, data governance, technology failure and threat to occupational therapists’ role and skills.
Conclusion
Applying digital technology to occupational therapy home assessment appears feasible and acceptable within a specific context. Further research is recommended to develop the technology, and test and investigate perceived benefits within wider contexts and stakeholder groups.
Introduction
Home assessments (or home visits) are integral to an occupational therapist’s role (Atwal et al., 2014; Drummond et al., 2012; Godfrey et al., 2019; Wilson et al., 2012). They provide occupational therapists with an opportunity to gather the information required to deliver personalised and integrated care (Lockwood et al., 2017) by physically travelling to the patient’s home to consider the patient’s abilities and needs in their own real-world environment (Atwal et al., 2014). However, several studies have identified resourcing pressures as a limiting factor in the decline of home assessments (Drummond et al., 2012; Ninnis et al., 2019).
A ‘Collaboration Aiming to Build Occupational Therapy Research’ (CABOT) (Di Bona et al., 2018; Jones, 2015) facilitated occupational therapists to work with university academics in exploring solutions to real-world problems. Clinicians felt delivering occupational therapy home assessments in some circumstances was problematic. Computer scientists collaborated with occupational therapists to find a potential digital solution only previously applied within emergency services (Mazumdar et al., 2017).
The Office of Life Sciences 2016 guide to the healthcare innovation pathway suggests that once an idea has been generated, the concept requires testing with key stakeholders to explore its ability to address unmet needs and outcomes. Only when this has been achieved can the idea move into the ‘development’ phase (Office for Life Sciences, 2016).
This project aimed to explore the concept of undertaking occupational therapy home assessments using secure digital videoconferencing within one United Kingdom (UK) Teaching Hospital National Health Service (NHS) trust.
Literature review
Occupational therapy pre-discharge home assessments are an important aspect of occupational therapy practice nationally and internationally (Atwal et al., 2014; Drummond et al., 2012; Godfrey et al., 2019), with the benefits, economic impact and clinical reasoning underlying such assessments explored by Ninnis et al. (2019). Atwal et al. (2008) conducted a qualitative study to explore if pre-discharge home assessments enhanced the health and wellbeing of older adults. Their findings suggested older adults are not fully prepared to undertake home assessments and find them daunting. Carers, however, appeared to find visits reassuring (Atwal et al., 2008). A narrative synthesis undertaken by Atwal et al. in 2012 found the wider body of international knowledge exploring patients’ perceptions and experiences of the pre-discharge home assessment to be limited (Atwal et al., 2012). In addition, Drummond et al. (2012) found little is known about day-to-day procedures of conducting occupational therapy pre-discharge home assessments, despite them being commonplace.
Clemson et al. (2016) found that therapists who conducted home assessments implemented twice as many occupational therapy recommendations as those undertaking in-hospital only consultations. They recommend that home visits should not routinely be carried out as part of acute hospital discharge planning, but guidelines should be developed for quality in-hospital consultations (Clemson et al., 2016).
More recently, Godfrey et al. (2019) published a qualitative exploration of occupational therapists’ experiences of pre-discharge home assessments, which found that a clinician’s own experiences and contextual influences create variation in home assessment practice. An example of a contextual influence is the ‘discharge to assess model’ (NHS England, 2016) aimed at reducing length of hospital stays. This model changes the traditional discharge planning process by focusing acute hospital assessment on immediate inpatient needs only, passing responsibility for home assessment to community-based integrated health and social care teams.
Due to the ever increasing demands being made on health and social care services, digitalisation is considered essential to future services (NHS England, 2019). The King’s Fund promotes the potential to deliver improved quality of care and cost savings across health and social care services (The King’s Fund, 2018). Allied health professionals are urged to lead innovations in digital health and make the most of new technologies for the benefit of patients (NHS Improvement, 2018). The NHS 2019 long term plan (NHS England, 2019) pledges to make digitally enabled care mainstream within the next decade, develop integrated care models and prevent delayed discharges and avoidable admissions.
Ninnis et al.’s (2019) synthesis of studies exploring information and communication technology use within home assessment interventions found barriers to traditional visits included time constraints and geographical distance, and identified technology use as a possible solution. This work suggested that although occupational therapists have explored the use of existing video conferencing equipment, digital photographs and digital report writing for home assessments, this technology is still viewed as novel (Ninnis et al., 2019).
Work to explore remote video consultation has been undertaken in non-occupational therapy fields, for example patients with obesity (Sturesson and Groth, 2018); specialised palliative care needs (Funderskov et al., 2019) and diabetes (Greenhalgh et al., 2018). In addition, remote video consultation has been used to include relatives and carers in the ward-round process (Østervang et al., 2019).
Sturesson and Groth (2018) wanted to understand when and in what circumstances remote technology would be feasible to use with certain patients with obesity. By introducing technological solutions for outpatient care, the researchers evaluated the concept of ‘video visits’ and explained why some patients were more suited to this approach than others (Sturesson and Groth, 2018). They suggest decisions to use video technology were influenced by practicalities, the patient’s ability and the content of the outpatient meeting (Sturesson and Groth, 2018).
Greenhalgh et al. (2018) defined good practice guidance regarding the use of virtual consultations, finding that when deemed clinically relevant and technical conditions were agreeable, they were considered popular and safe by patients and staff. When compared to face-to-face consultations, results suggested that although video consultations were shorter in duration, this approach resulted in patients talking more (Greenhalgh et al., 2018). In addition, they identify the content of video consultations needed to be made explicit, whereas within traditional meetings this is implied (Greenhalgh et al., 2018). Successful video discussions and improved patient self-management were also linked with familiar and trusting patient/clinician relationships (Greenhalgh et al., 2018). Challenges in scaling up the intervention included technical considerations and organisational reluctance to wholescale change, especially at times of austerity (Greenhalgh et al., 2018).
Østervang et al.’s (2019) qualitative study focused on video consultation use within ward rounds to include relatives and carers. Findings suggest the technology enables health care professionals to remotely engage patients’ relatives, but time pressures, culture and change of work routines in complex health care systems were barriers to implementation (Østervang et al., 2019).
A broader body of knowledge suggests remote visit consultations are an emerging service delivery model within the NHS with potential for improved efficiency and patient experiences (Greenhalgh et al., 2018; Østervang et al., 2019; Sturesson and Groth, 2018). This project explores the potential of using such technologies in occupational therapy practice.
Method
Project overview, aims and objectives
A 3-month collaboration was undertaken between March and May 2016 by a clinical academic occupational therapist, health service researcher, two computer scientists from a UK university, a clinical occupational therapist and an occupational therapy service manager from an NHS teaching hospital NHS foundation trust.
The aim was to test the concept of using a specific video conferencing technology to explore the feasibility, acceptability and potential benefits in home assessments, within one UK NHS teaching hospital setting. The project was split into four work streams, which ran simultaneously, addressing the specific objectives using a range of data collection methods and populations. This is summarised in Table 1.
Overview of project work stream objectives, data collection method and populations.
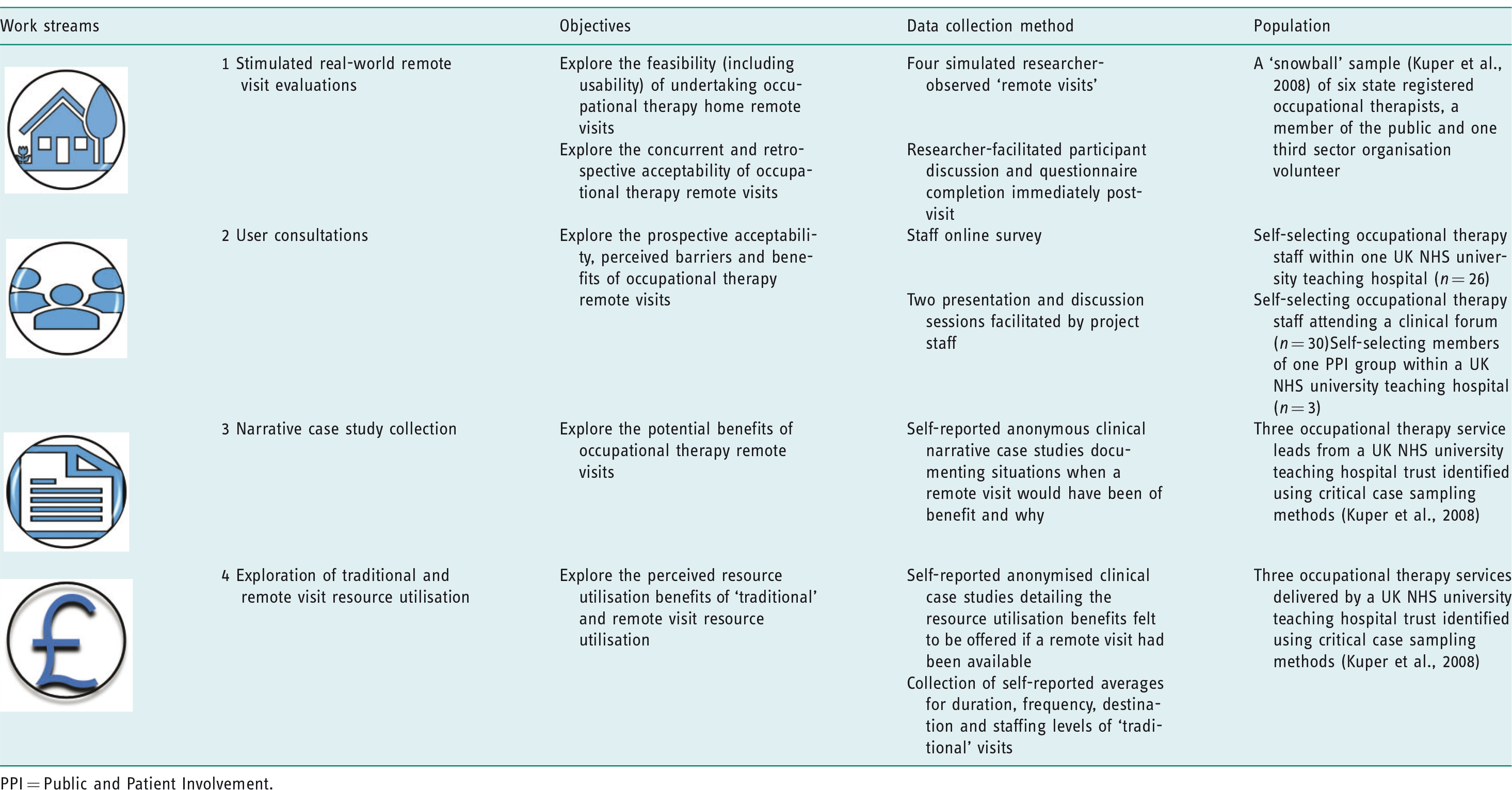
PPI = Public and Patient Involvement.
The technology
Created by adapting an existing technology developed for use with Italian emergency services called ‘eyes on the ground’ (Mazumdar et al., 2017), the ViVA (Virtual Visit Approach) technology used within this project offered occupational therapists the ability to undertake remote audio/video home assessments or ‘virtual visits’.
ViVA works by allowing a hospital-based occupational therapist to communicate and capture images via a hyperlink that is texted or emailed to a smartphone controlled by a trusted visitor (such as a relative or member of a third sector organisation). Once opened by the trusted visitor, the link allows the visitor to communicate with the occupational therapist via a video call and show them the residence remotely. This process is outlined in Figure 1.
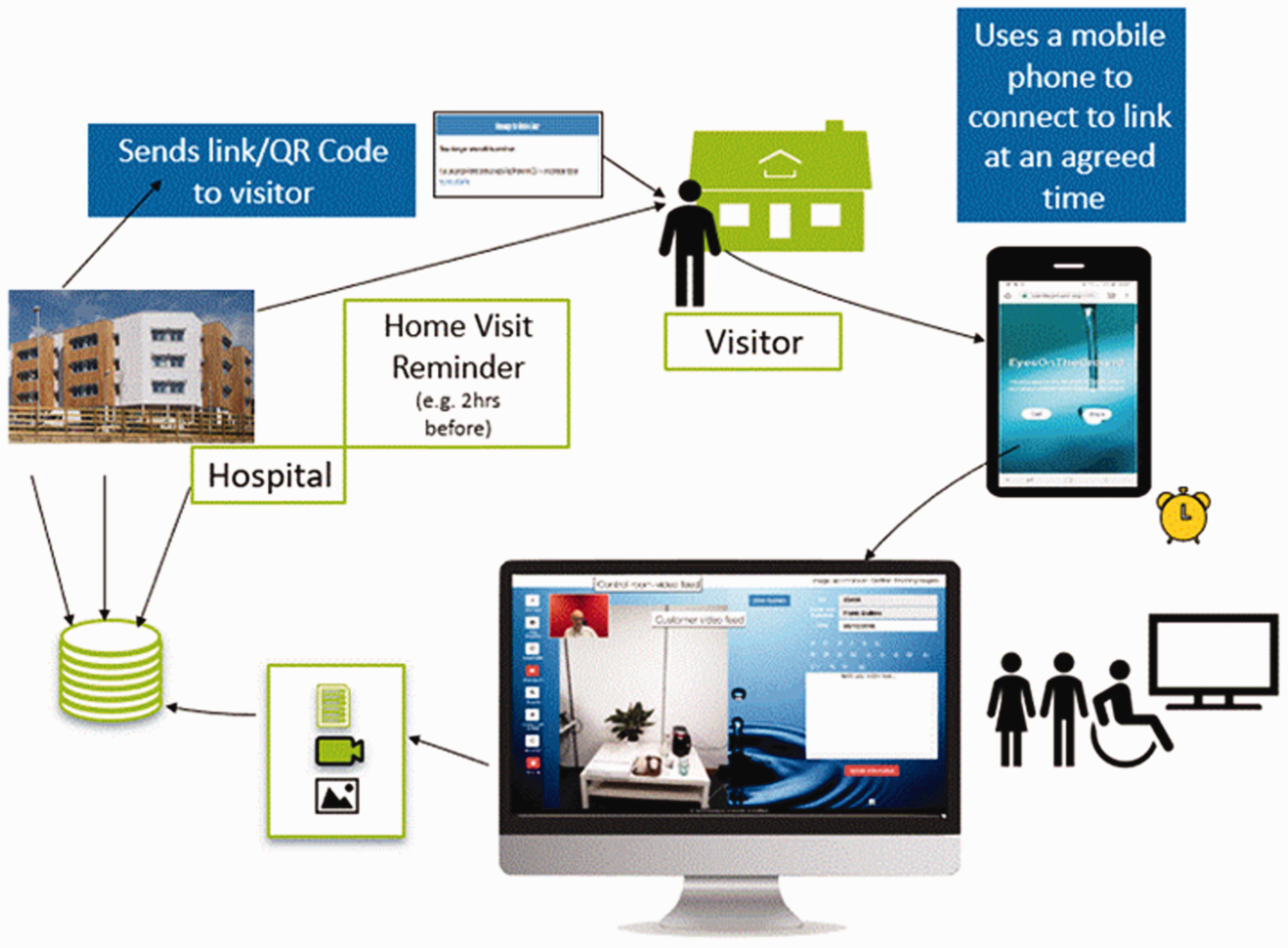
Outline of the remote ‘virtual visit’ process.
ViVA also provides additional functions, as shown in Figure 1. For example, the hospital-based occupational therapist can control the visitor’s camera and flash, take photographs and capture videos (as shown by the control panel screen shot of the hospital base computer in Figure 2), and take real-time digital notes.
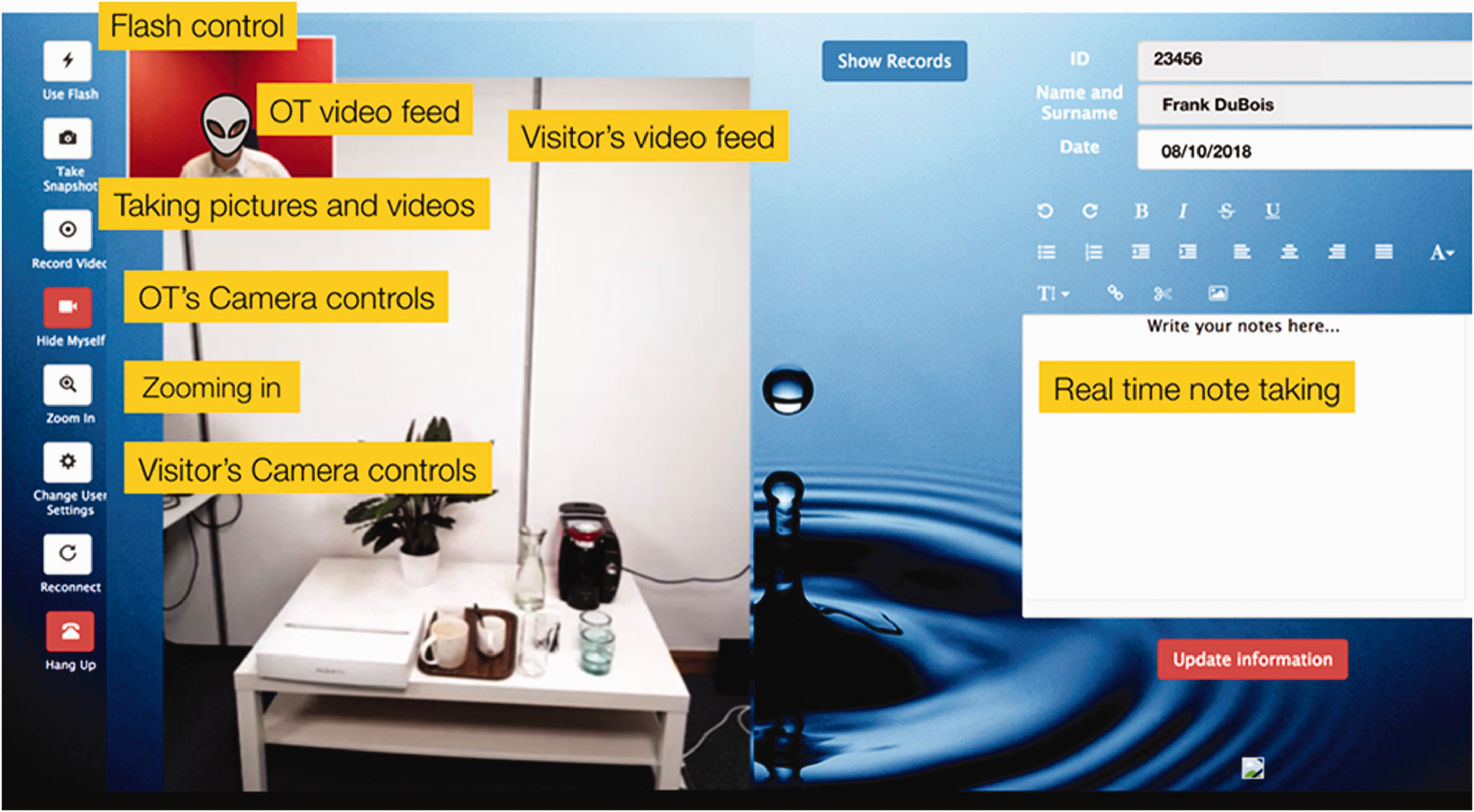
Screen shot of the occupational therapist’s remote ‘virtual visit’ control panel, showing the control buttons on the left, which allow the therapist to control the visitor’s smartphone and right-hand panel for them to capture real-time notes.
Ethical approval
This project was categorised as a service evaluation by the Medical Research Council, NIHR Health Research Authority decision tool (2019) because participants were not randomised, and changes to routine care and generalisable findings were not intended (Health Research Authority, 2013). Formal ethical approval was therefore not required.
The project was registered with a UK NHS Foundation Trust Clinical Effectiveness Unit, who provided scrutiny and oversight, as a service evaluation. It adhered to the National Institute of Health Research Good Clinical Practice (NIHR GCP) standards (National Institute of Health Research, 2019), which included providing a full explanation of the project to participants, ensuring they understood they could withdraw from the project at any time and ensuring that their anonymity was maintained when capturing and reporting findings. NHS project staff were Health and Care Professions Council (HCPC) registered and university project staff held NIHR GCP certification.
Project work stream design
Work stream 1: simulated real-world remote ‘virtual visits’
Four remote virtual home visits were undertaken to explore their feasibility and concurrent and retrospective acceptability (Sekhon et al., 2017) using observation, discussion and questionnaire data collection methods that are detailed in Table A1 in the online appendix.
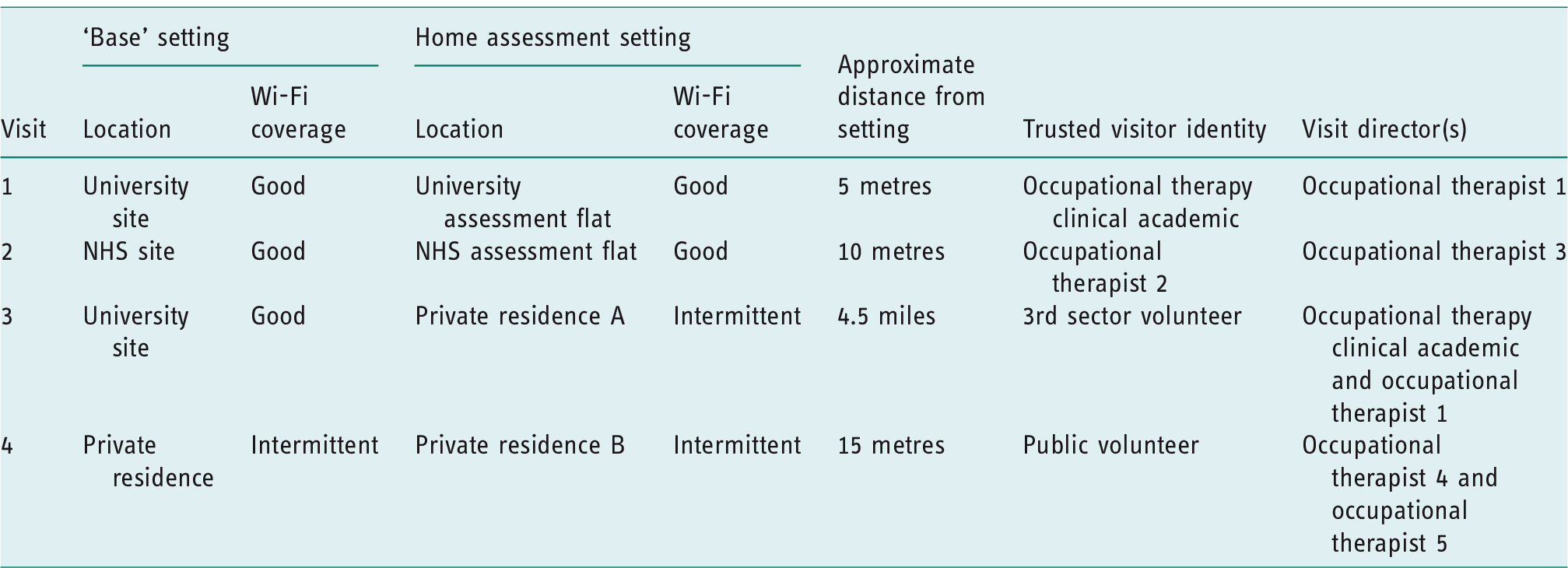
Although not used in real clinical situations, the evaluation conditions were constructed to simulate a range of ‘real-world’ contexts, as shown in Table 2. This included varied ‘base’ and home assessment settings, varied Wi-Fi coverage and varied trusted visitor and occupational therapist identity.
Details of the four real-world remote ‘virtual visits’.
Snowballing sampling methods (Kuper et al., 2008) were used to recruit the trusted visitors and directors required for each visit. Potential participants were sent a project information sheet and asked to contact the researchers if interested.
Visit directors were all qualified occupational therapists and recruited from the project team or via occupational therapy clinical networks. ‘Trusted visitor’ participants included an interested volunteer member of the public employed by the university in a non-related department and a third sector organisation volunteer. Visit locations were two assessment flats (a university digital technology home laboratory and an NHS patient rehabilitation flat) and two private residences (the homes of two of members of the research team).
Prior to every visit, the participant information sheet was reviewed, participants were briefed on the project and visit process, and there was a demonstration of the technology provided.
The clinical research occupational therapists collated all acceptability data within NVivo software (QRS International, 2019), identifying key descriptive themes using thematic analysis (Braun and Clarke, 2006). Objective assessment (SUS) questionnaire responses were statistically analysed and detailed within Mazumdar et al. (2017).
Work stream 2: user consultations
Self-selecting staff and Public and Patient Involvement (PPI) group, PPI stakeholders were consulted to explore the prospective acceptability (Sekhon et al., 2017) of digital technology use to undertake remote occupational therapy home assessments. Online survey and face-to-face presentation methods were employed and detailed in Table A2.
Qualitative anonymised open text survey responses and anonymised presentation discussion minutes were collated within NVivo software (QRS International, 2019) by the clinical academic occupational therapist. Key descriptive themes were identified using thematic analysis (Braun and Clarke, 2006). Quantitative survey responses were collated and summarised using descriptive statistics (Campbell et al., 2010).
Work stream 3: collecting narrative case studies
The potential benefits of the virtual visit concept were explored by approaching three critically case sampled (Kuper et al., 2008) occupational therapy service leads within the participating NHS trust. These services had reported the highest frequency of home assessments in addition to significant interest in the project (Table A3). Services were were asked to provide anonymised case studies of clinical cases where, in their subjective opinion, the digital home assessment approach or remote ‘virtual visit’ would have been beneficial and why.
Five narrative case studies were provided to the clinical academic occupation therapist, who collated them within NVivo software (QRS International, 2019) and identified key descriptive themes using thematic analysis (Braun and Clarke, 2006).
Work stream 4: understanding current resource utilisation
Current resource utilisation was explored by approaching the three critically case sampled (Kuper et al., 2008) occupational therapy services engaging in work stream 3. They were asked to provide details of access visit resource use in their department from the previous year. Details of this work stream can be found in Table A4.
The information regarding visit duration and staffing levels was then compared to that recorded for the three remote virtual visits conducted in work stream one.
Findings
Feasibility of ViVA
Four real-world remote ‘virtual visits’ were successfully completed within work stream 1, suggesting the concept of remote home visits is feasible in those specific contexts. Communication between the trusted visitor and occupational therapists was maintained with accurate information about the environment obtained and recorded in photographic, video and note form. The ‘virtual visit’ achieved success even when key visit stressors (barriers to adoption) identified by occupational therapists prior to the project’s inception by the technology developers (Mazumdar et al., 2017) were imposed and varied as shown in Table 2. Stressors were Wi-Fi coverage, geographic distance from the base, and trusted visitor and occupational therapists identities.
Work stream 1’s post-visit user study questionnaire indicates that most of our users felt the system was simple to use, that they wanted to use the system more frequently, and that it was quick and easy to learn. Most users felt confident using the system and felt that the system performed consistently. However, most users highlighted the potential need for the presence of technical support. While we only highlight some of the findings of our user studies here (for brevity and avoiding repetition), we discuss our findings and the user evaluations in more detail in Mazumdar et al. (2017).
Acceptability of ViVA
Concurrent and retrospective acceptability data from work stream 1 suggests the success of the virtual visit concept is dependent on four key elements: ensuring visitor safety, visitor training, visitor induction and standardisation of practice. This data was used within the project to iteratively develop documents and processes to address issues and also refine the technology.
Visitor safety
A pre-assessment of the visitor’s abilities and needs was found to be essential. Without it the visitor could be placed at risk and the data collected may not be accurate. Data from the real-world simulations suggested this was best achieved via a trusted visitor risk assessment. The cognitive and physical abilities of trusted visitors needed to be established in order to maximise their safety and visit success. Feedback from the ‘trusted visitor’ suggests that if the visitor did not have the dexterity or cognitive ability to use the phone, or physical ability to bend down and take measurements, the visit could be potentially unsafe and measurements inaccurate. Prospective acceptability data from the online staff survey within work stream 2 supports this finding. A member of the occupational therapy staff suggested that ‘People [visitors] may not have the capabilities to assist at home’ (occupational therapy staff member, online survey response).
Visitor training/induction
Prospective, concurrent and retrospective acceptability data suggests that a pre-visit discussion was essential to put the visitor at ease, ensure they know what to do if the signal fails, and address any confidentiality and privacy concerns about filming a person’s home environment, for example, identifying with patients and visitors if there are any areas of the home they did not want recording and reassuring patients and visitors about data security. This quote from a patient representative from the PPI panel consultation in work stream 2 summarises this need: I am a techno-phobe so would have real sympathy with people who may feel somewhat panicked by using technology in this way. Plenty of training is required so they are confident about what they need to do. Be aware that what may appear very simple to confident phone/computer users is not simple to many people. (Patient representative, PPI panel verbal feedback)
Visit standardisation
Concurrent and retrospective acceptability data from work stream 1 suggests that clear instructions and virtual visit protocol were fundamental for visit success. For example, professional terminology and instructions were found to be confusing to ‘trusted visitors’. As Mazumdar et al. (2017) explain, an instruction such as ‘measure the door width’ resulted in the door width being measured rather than the space between the right and left door frames.
Barriers for ViVA
Findings from work stream 1 and 2 prospective, concurrent and retrospective acceptability data indicate barriers to acceptability and adoption are perceived. They suggest that data security and data governance, including the consent of those in the home but not involved in the assessment, were of concern to staff and the PPI groups. Concerns existed regarding Wi-Fi coverage, IT equipment failure, and resource implications for the NHS and ‘trusted visitors’, which include paying for data and a smartphone. Findings also imply that some occupational therapists may perceive the virtual visit approach as a threat to their role and skills. Some of these perceived drawbacks are illustrated by the following staff and patient representative feedback: I hope that it wouldn’t get into the mentality of ‘anyone can do it’ and we lose our OT [occupational therapist] identity/skills. (Occupational therapy staff member, online survey response) I would be happy to do this as I can see an increasing need for patients to help with the financial burden on the NHS. I don’t think it will be very difficult to persuade many people to that idea though! I do not have to worry about paying my phone bill, some people will. (Patient representative, PPI panel verbal feedback)
Potential benefits of ViVA
Resource utilisation
There was agreement within work streams 1, 2 and 3 prospective and concurrent acceptability data that participants perceived the concept to have resource utilisation benefit potential. These included assisting in minimising the number of unsuccessful discharges, reducing the length of hospital stays, preventing avoidable admissions and minimising duplication of services/support. The following extracts from occupational therapy staff and the PPI group illustrate this: I think this is a good idea as it makes better use of valuable and limited OT time. It’s obviously much quicker for an OT to undertake an assessment and give advice remotely rather than having to visit the patient’s home. (Patient representative, PPI panel verbal feedback) The approach could result in no travelling time to patients’ homes. Reduces waiting lists for patients needing environmental checks for powered equipment. Patients may receive equipment more quickly. (Occupational Therapy staff member, online survey response) The ‘virtual visit’ would help to cut out driving time to patients’ properties, thereby saving much time and petrol expenses. Saving this travel time, we could probably do more ‘visits’ per day. We would be able to write the virtual visit up at the same time, again saving time. If the ‘virtual visit’ works for the team it could drastically reduce our waiting times for provision of powered wheelchairs. Patients would get a much better service and the number of complaints about waiting times would reduce too. Our patients live out of area. We can sometimes do a 50-mile round trip to see a patient. (Wheelchair and specialist seating service case study excerpt)
Personalising care
Prospective and retrospective acceptability data from work streams 1 and 2 suggests that the ability to engage the patient and trusted visitor in a ‘virtual visit’ prior to discharge could result in facilitating a person-centred approach. Where previously they may not have been engaged, the ‘virtual visit’ offers an opportunity to involve them and thus potentially personalise the experience for the individual. Occupational therapists thought that this technology had the potential to provide a conduit via which patients can make empowered decisions, and engage in positive risk taking and co-ordination of their own care. This is illustrated by the following patient representative and staff member response to the question ‘What do you see as the potential benefits of the technology?’: [The technology] could allow the patient to be with the OT when the assessment is taking place so that they can feed in their own thoughts and ideas and also to be able to provide an accurate picture of how they live and what they would wish to do when back at home. (Patient representative, PPI panel verbal feedback) [The technology and approach would be] helpful to engage patients in discharge planning, goal-planning and making them feel more empowered. (Occupational therapy staff member, online survey response) [If the patient can be with] the OT when the assessment is taking place … they can feed in their own thoughts and ideas and also be able to provide an accurate picture of how they live and what they would wish to do when back at home. (Occupational therapy staff member, online survey response)
Enhancing health and social care integration
Acceptability data from work stream 1 and 2 indicates that occupational therapy participants believe remote ‘virtual visits’ have the potential to enhance interagency working. It was felt that the addition of a function that allowed further agencies to participate in the visit could enhance health and social care integration by providing a conduit to aid collaborative working conversations. This is illustrated by the following responses to the question ‘What do you see as the potential benefits of the technology?’ [The technology would be] useful to problem-solve solutions with accident and emergency/other services. (Occupational therapy staff member, online survey response) When referring for adaptations or equipment, pictures of where the equipment/adaptation needs to be fitted could be sent to the fitters [using this technology]. (Occupational therapy staff member, online survey response)
Other applications
Findings indicate that the technology and virtual visit approach had a potential wider application. The PPI panel’s and occupational therapists’ prospective acceptability data suggest potential use within the following settings: inpatient palliative care facilities to enable patients to see their home, loved one or pet; the provision of a ‘virtual meeting’ option with family; within the home environment to monitor progress post discharge and prevent further admissions; use within housing and social services for assessment and integrated intra-agency service delivery.
Discussion and implications
The technology and ‘virtual visit’ approach was found to be feasible and acceptable if mechanisms were in place to address key concerns and barriers. The majority of the barriers highlighted were similar to those identified by Ninnis et al. (2019): availability of technology; potential for errors (for example measurements); Wi-Fi/network coverage difficulties and cost of data. However, this project identified additional concerns regarding the safety and abilities of the ‘trusted visitor’. The project addressed this by working with the occupational therapists engaged in the remote ‘virtual visits’ to create a pre-visit ‘trusted visitor’ risk assessment and training package, in addition to a locally standardised virtual visit protocol and electronic reporting proformas for the remote visits.
Data security and governance (including confidentiality and consent), the potential for technical failures, and perceived threats to the occupational therapy role were also identified as key barriers, but time and funding constraints prevented this project from exploring solutions.
Findings from this project supported Money et al.’s (2015) suggestions that occupational therapists are recognising and embracing their contribution to digital health care delivery. Participants were receptive to exploring how technological advances can support more efficient and effective service delivery, thereby facilitating better utilisation of resources.
The NHS Plan (NHS England, 2019) promotes a ‘what matters to me’ (personalised care) approach as business as usual. A key focus for the technology and digital agenda (NHS plan, 2019) is enabling patients to improve the management of their own health and social care. Project findings suggest that the use of digital technology for remote ‘virtual visits’ could facilitate personalised conversations about the home environment, which could engage the patient and family. Atwal et al. (2012) suggest that patient involvement in the home assessment process could improve ownership of their own care. With the technology at the ‘inpatient bedside’, patients, family members and friends could be engaged in the assessment where it may previously not have been possible. Occupational therapists perceived that this technology had the potential to empower patients to shape their own discharge by being more involved in the process by acting as a conduit to empower choice, positive risk-taking and co-ordination of their own care.
As a local service evaluation, the authors have identified limitations. Within the constraints of the project funding it was not possible or appropriate to carry out research. Results cannot be generalised and as such must be regarded as relevant to one particular context and time period. Participants were not representative of all stakeholders as snowballing and critical case sampling methods were used within a self-selecting sample. In addition, the number of patient and public participants was limited. Qualitative data from work stream 1 and 2 were not cross-coded by a second researcher, and data saturation (Mays and Pope, 1995) was not achieved. Many of the project’s participants were self-selecting and much of the project’s data was self-reported. In addition, despite attempts to maximise reflexivity, the project team may have imparted unintended bias resulting from their employment within the NHS foundation trust and role in technology development. Finally, the resource utilisation information gathered within work stream 4 were self-reported estimates.
Despite the shortcomings in the approach taken, the work does suggest gains are possible. Further collaborative academic and clinical occupational therapy research is needed to explore and develop the technology, deploy it within real-life health and social care situations, capture its economic and wider impacts, and explore barriers and solutions to implementation. Refinement of the project visitor safety, training and visit standardisation mechanisms is suggested, in addition to identification of additional implementation barriers and solutions to this digital approach. Crucially, the key issues regarding data governance, security, confidentiality and consent must be addressed.
Conclusion
This project has demonstrated that the application of a unique digital technology to the home assessment process is perceived to be feasible and acceptable for occupational therapists, patients and the public within the local context in which it was evaluated. However, concerns were noted about whether a ‘virtual visit’ would replace the traditional visit completely and this seemed to cause concern for professional practice. Fears about technology taking over were allayed by discussions about how the ‘virtual visit’ could be utilised as an adjunct to enhance service provision in cases where a visit is not physically or logistically possible or to provide rapid access to a visual of the property. Which circumstances require a virtual visit would need to be explored in future projects.
The four ‘real-world’ simulations were conducted successfully and clinical protocols developed iteratively. Occupational therapists engaged within the project were keen to explore the benefits of the ‘virtual visit’, especially where it enabled access to a home environment that would be otherwise inaccessible. However, they did have some concerns about the potential changes in role that would result. All participants said that data security was of paramount importance and critical to successful deployment. Trusted visitor risk assessments and training were essential, as were visit protocols and reporting proformas.
Patient representatives and occupational therapists perceived that this technology could enable person-centred care by enabling ‘quick remote access’ to the home environment, thereby facilitating timely patient-led conversations about discharge planning. Early findings also suggest the ‘virtual visit’ approach could facilitate improved resource utilisation by reducing the number of staff and resources required to conduct a home visit, particularly with regard to home visits at a considerable distance from the base.
Further rigorous research is recommended to explore and develop the technology, its application and effects within wider health and social care contexts. With this goal in mind, the project team have been successful in securing funding for two further projects (2018 and 2020) of increasing size, to build the evidence base and develop the next iteration of this exciting collaborative project.
Key findings
Remote home assessments using digital technology are perceived to be feasible and acceptable. This technology has potential to enhance personalisation and improve resource utilisation.
What the study has added
Digital technology was applied to occupational therapy home assessments. This technology was felt to be feasible and acceptable and has potential to address current policy agendas and improve resource utilisation.
Supplemental Material
sj-pdf-1-bjo-10.1177_0308022620921111 - Supplemental material for Remote Home Visit: Exploring the feasibility, acceptability and potential benefits of using digital technology to undertake occupational therapy home assessments
Supplemental material, sj-pdf-1-bjo-10.1177_0308022620921111 for Remote Home Visit: Exploring the feasibility, acceptability and potential benefits of using digital technology to undertake occupational therapy home assessments by Jennifer Read, Natalie Jones, Colette Fegan, Peter Cudd, Emma Simpson, Suvodeep Mazumdar and Fabio Ciravegna in British Journal of Occupational Therapy
Footnotes
Acknowledgements
The authors acknowledge the contribution and leadership of Laura Evans, Head of Occupational Therapy at Sheffield Teaching Hospitals NHS Foundation Trust (STHFT) in developing the original CABOT collaboration. The project would also like to thank and acknowledge staff and students from Sheffield STHFT, Sheffield Health and Social Care NHS Foundation Trust, Sheffield Churches Council for Community Care charity, members of the public and the STHFT Professional Services Patient and Public Involvement panel who participated in the project.
Research ethics
Scrutiny of the project’s methods and intended findings by the Medical Research Council and NHS Health Research Authority identified it as a service evaluation requiring no formal ethical approval. Full service evaluation approval and registration was obtained from Sheffield Teaching Hospitals NHS Foundation Trust (STHFT), which ensured principles of confidentiality, anonymity and right to withdraw were maintained at all times (STHFT Clinical Effectiveness Unit reference number 9323). The project adhered to the National Institute of Health Research Good Clinical Practice (GCP) standards.
Consent
All participants provided consent and took part this service evaluation voluntarily after project information was provided.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded using University of Sheffield internal awards from their Higher Education Innovation Fund allocation, and match funded by Sheffield Teaching Hospitals NHS Trust.
Contributorship
All named authors have contributed to and take shared responsibility and accountability for the published work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.