
Abstract
Introduction
Practice education is fundamental to pre-registration learning for many health and social care professions, yet finding sufficient opportunities for students is challenging. One-to-one student–educator pairings are common, and while different models could increase placement opportunities, the associated terminology is inconsistent and an overview of advantages, challenges and available evidence is missing. This mapping review identifies, categorises and critically considers the evidence for different models of practice education used by health and social care professions.
Method
Papers from 2008 onwards reporting on practice education approaches in allied health or social care profession courses were identified in three databases. Data was extracted, methodological quality categorised and a typology of practice education models developed.
Findings
Fifty-three papers were reviewed and developed into a typology of 14 models. Mapping indicated issues with a lack of high-quality research and limitations in available outcome indicators. Pre-requisites for the effective operation of different models include preparation, communication and allowing sufficient time for new ways of working.
Conclusions
Practice education discourse is characterised by varied terminology and practices. Various models for structuring practice education exist, though the evidence for their effectiveness and impact on capacity is limited. Using consistent language and considering wider impacts and outcomes is recommended in future study.
Introduction
Practice education is fundamental to the pre-registration curricula of many health and social care professions (Chambers et al., 2016). However, challenges in securing sufficient practice education opportunities to meet the growing demand for pre-registration education have been identified and persisted over the last 15 years, appearing to be common to different countries including, for example, the United Kingdom (UK) (Craik and Turner, 2005; Haig and Summerfield-Mann, 2016), United States of America (USA) (Roberts and Simon, 2012) and Australia (McBride et al., 2015). Rodgers et al.'s (2008) early work to examine this issue identified that allied health professions in several countries experienced challenges associated with providing sufficient placements for students. This has recently been reconfirmed as an issue affecting many of the health and social care professions in the UK, with funding availability and increased student numbers identified as increasing demand for placement opportunities (Chambers et al., 2016).
Papers identifying issues about placement capacity typically include calls to increase opportunities by encouraging professionals to offer placements. Rarely is the model of practice education considered as potentially increasing capacity. Many of the bodies that set standards for pre-registration health and social care professional education specify a minimum total duration for practice education but do not specify how this ought to be achieved. For instance, the World Federation of Occupational Therapists (WFOT, 2016) stipulates that students complete a minimum of 1000 hours of practice education prior to accreditation but do not specify how practice education should be delivered, only that an occupational therapist must be the supervisor and assessor. Similarly, regulatory bodies such as the UK’s Health and Care Professions Council (HCPC) state only that the structure, environment and support provided for practice education must be sufficient to ensure learning outcomes are met (HCPC, 2017). In contrast, in the USA the Accreditation Council for Occupational Therapy Education’s most recent set of standards provide parameters for acceptable fieldwork experiences corresponding to different levels of education (ACOTE, 2018).
The approach used in this mapping review (Grant and Booth, 2009) is intended to develop a current overview of trends and gaps by identifying and categorising different models of practice education that may be applicable to the provision of practice education for pre-registration occupational therapy students, and identifying reported benefits and contextual considerations associated with their use. While precise definitions for mapping reviews vary, they typically aim to search a broad field systematically to identify gaps in knowledge and future research needs (Cooper, 2016). Detailed critical appraisal is not normally an objective, as mapping reviews are used to characterise the key features of bodies of research that are characterised by high levels of heterogeneity, though this may include summarising quality indicators using frameworks for formal quality assessment (Grant and Booth, 2009). Similarly, an in-depth synthesis of results is replaced by the presentation of linkages as we identify and present the principal characteristics that enable a representation of activity related to a given topic to be presented (Cooper, 2016).
Method
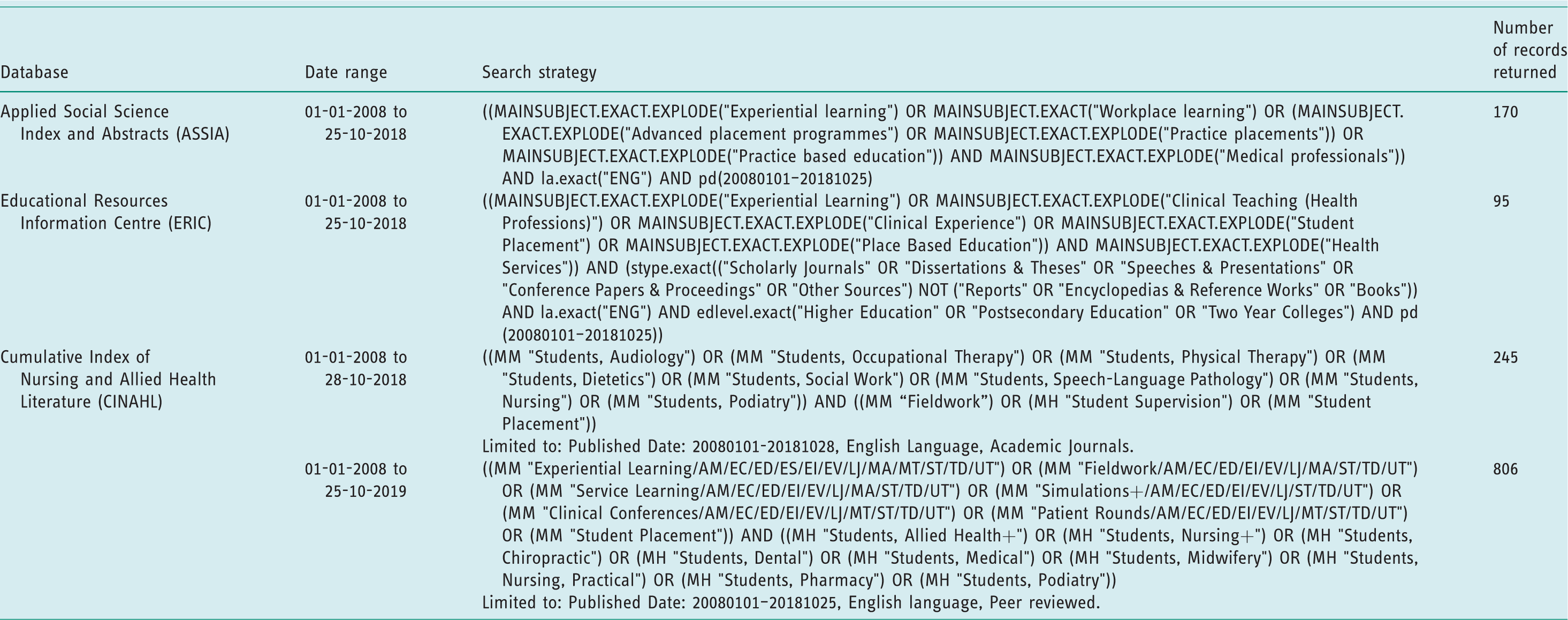
Papers published since January 1st 2008 were sought for review if they reported identifiable models of practice education used during study to become a recognised health or social care professional. This date range was chosen to include papers published since the review by Overton et al. (2009) of non-traditional occupational therapy practice education, to provide an updated and expanded account of potential practice education models. Papers had to be in English, but they were not excluded based on methodology and thus qualitative, quantitative and descriptive studies and peer-reviewed literature reviews were all eligible for inclusion. Opinion pieces and papers providing insufficient detail were excluded. This was intended to have the benefits of integrative reviewing suggested by Whittemore and Knafl (2005), particularly the idea that incorporating diverse methodologies can capture subjective elements, contextual details and information about novel approaches. Three databases were selected to ensure papers written from different perspectives were accessed, including the allied health professions, education and social sciences. Specific searches were developed and run for each database using combinations of indexed terms and subject headings (see Table 1 for details). An additional search was run in the Cumulative Index of Nursing and Allied Health Literature (CINAHL) with a selection of more specific student-related terms to ensure that relevant papers from different disciplines were included. All returned references were imported into RefWorks and screened for duplicates.
Search record.
The first author screened article titles and abstracts to assess eligibility. The full text of the article was retrieved if the study met the inclusion criteria or if eligibility was unclear from the abstract. Papers were sent to the second author for screening and discussion if eligibility remained unclear. A standard form for extracting data was developed including: reference information; details of the professional group studied; geographical location; study design; sample information; description of the practice education model used; summarised results or findings; notes on any methodological limitations or issues; and reference information for potential additional papers. To provide an accessible overview of types of research activity and the quality of the papers reviewed, each paper was ascribed an indicator of design category and given a quality score based on a review of the methods used. The National Service Framework: Long Term Conditions research typology was used (Turner-Stokes et al., 2006), allowing for the inclusion of multiple design types to be recorded, while also differentiating their key attributes.
Results
1316 records were returned. Four additional papers were identified for inclusion during the review of the included papers. Three further papers that studied the use of simulation for practice education, published after the searches took place, were included on the advice of members of the project’s steering group, due to their relevance to the topic. Two hundred and forty-seven duplicate records were removed, followed by 1010 that did not meet eligibility criteria. Thirteen of the remaining 66 papers were excluded on full-text review. In total, 53 papers were reviewed (see Figure 1 for details). Methodologically, just over half of the included papers (27/53) reported using a qualitative approach. Descriptive studies accounted for nine papers, with six quantitative studies, five literature reviews and six mixed-methods papers also included.
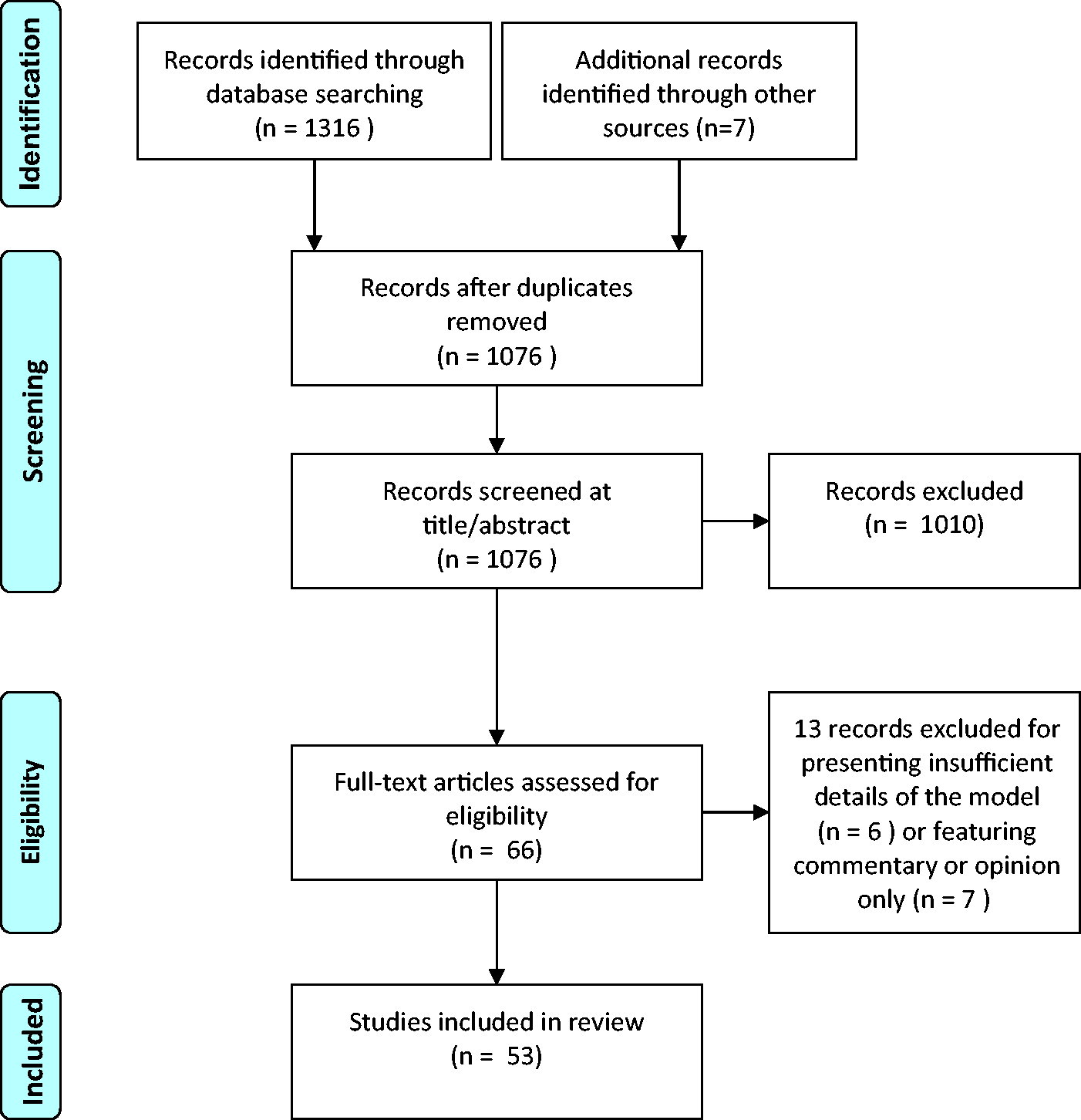
PRISMA flow diagram of article selection (Moher et al., 2009).
Fourteen different models of practice education were identified, along with five papers reporting on combinations of these into hybrid approaches. A range of professions were represented in studies, including in order of frequency of occurrence occupational therapy (30), nursing (7), physiotherapy (7), social work (5), dietetics (4), speech and language therapy (3), pharmacy (1), podiatry (1) and oral health (1). One paper with an inter-professional focus did not report sufficient detail of participants to allow individual professions to be identified. Details of reviewed papers are given in Table 2. The bubble chart detailed in Figure 2 provides a visual map to the reviewed research, representing research type, quality, volume and focus to help identify gaps.
Summary of reviewed papers.

National Services Framework – Long Term Conditions Evidence Typology (Turner-Stokes et al., 2006). Research type: opinion/experience of users and/or carers (E1) or professionals (E2). Primary research using quantitative methods (P1), qualitative methods (P2) or mixed methods (P3). Secondary research: meta-analysis (S1) or other secondary analysis (S2). Reviews: systematic (R1) or other descriptive reviews (R2). Quality assessment rated on five parameters (scored out of 10) and categorised into ‘high’ (7–10/10), ‘medium’ (4–6/10) and ‘low’ (0–3/10) quality ratings.
RCT: randomised controlled trial; ILA: inter-professional learning activity. Higher Education Institution (HEI). Peer-assisted learning (PAL).
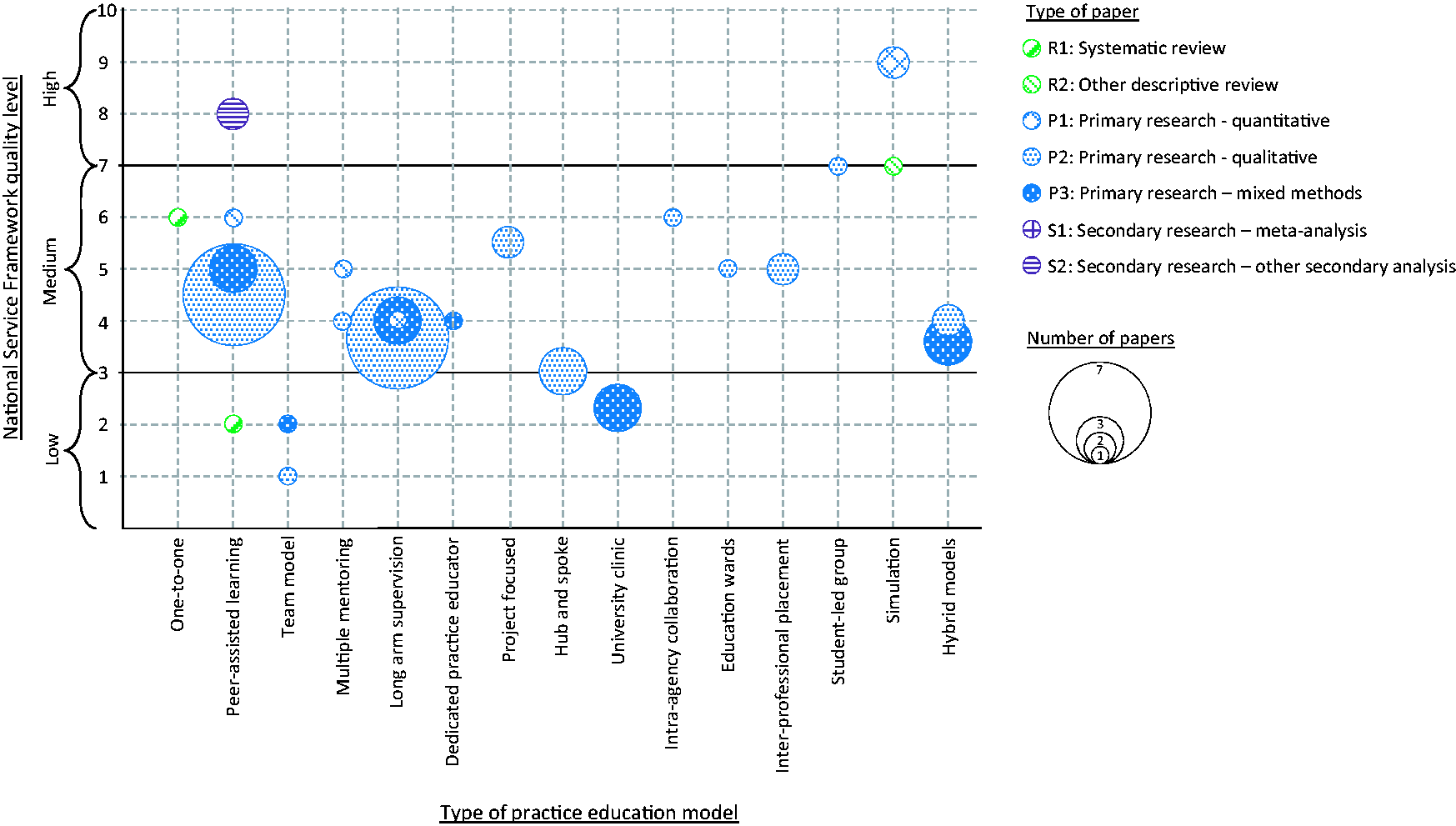
Evidence map for models of practice education.
Findings
One-to-one model
This easily recognised practice education model, in which one practice educator supervises and assesses one student, was the focus of one paper, by Luhanga et al. (2010), who reviewed 57 papers considering the preceptorship approach to nursing practice education. This reported that having a consistent and accessible educator created safe learning spaces in which individualised feedback and facilitation, and tailored learning opportunities, were more available. Several potential issues with the one-to-one model were noted, including the risk for limited learning if student–educator relationships are suboptimal, or if a student becomes dependent on a single role model. Luhanga et al. (2010) also noted issues with the increased workload that supervision using this model might bring, highlighting the need to put clinical priorities ahead of educating students and restricting the quality of education and supervision. The importance of support and training for practice educators was identified, with several reviewed papers noting this was often inadequate and therefore a significant cause of poor recruitment and retention of nurses into the practice educator role (Luhanga et al., 2010).
Peer-assisted learning
Peer-assisted learning models involve two or more students concurrently working with one educator, with an expectation that the students work together in ways that facilitate learning. This model was frequently referenced across professions, featuring in 13 primary research studies (eight qualitative, two quantitative and three mixed-methods designs) and two non-analytic reviews. Most of these identified benefits. Flood et al. (2010) noted that peer-assisted learning is an established approach associated with increased professional competence and confidence that results from a greater degree of active learning. Other papers corroborate these claims, with Secomb’s (2008) non-meta analytic systematic review reporting increased educational outcomes, and Briffa and Porter’s (2013) review noting consistent reports of improved student outcomes and satisfaction, albeit from methodologically limited studies. Kinsella and Piersol (2018) reported increased perceptions of self-confidence and clinical proficiency from both students and educators, while O’Connor et al. (2012) suggested that peer-learning models increased experiential learning. Roberts et al. (2009) reported that the model increased the number of placement hours provided by practice educators without negatively impacting student experience or service delivery.
Bhagwat et al. (2018), Reidlinger et al. (2017) and O’Connor et al. (2012) compared applications of the peer-assisted learning with the one-to-one model, identifying no conclusive advantages for either approach. Student experience and satisfaction with workload on peer-assisted placements were reported as equivalent to, or slightly higher than, one-to-one placements (Reidlinger et al., 2017), though final-year students favoured the latter as they felt it allowed clearer demonstrations of competency (O’Connor et al., 2012). Practice educators reported that the model might afford fewer learning opportunities (Briffa and Porter, 2013; Price and Whiteside, 2016), and required significantly more direct student supervision (Reidlinger et al., 2017), though a time-use survey by Bhagwat et al. (2018) suggested that this may not to be the case. Sevenhuysen et al. (2014, 2015) compared peer-assisted learning as a specific aspect of paired placements, finding no significant improvements to learning outcomes using this model, though both students and educators preferred practice placements that did not include specific peer-learning activities.
Some potential issues and concerns related to this model were identified as increased pressure on office space (Kinsella and Piersol, 2018), possible lack of opportunities to work with service users (Kinsella and Piersol, 2018; Price and Whiteside, 2016) and reduced time for individual student supervision (Briffa and Porter, 2013). However, a number of strategies to optimise the use of the peer-assisted model were reported. Preparing students and educators is important, and ought to include training in facilitative peer-feedback processes, as well as underpinning theories and principles (Blakely et al., 2009; Briffa and Porter, 2013; Lynam et al., 2015; Secomb, 2008). Advanced preparation ensures the effective organisation and achievement of day-to-day learning activities, and assessment of placement learning outcomes (Hanson and DeIuliis, 2015). Similarly, careful pre-placement consideration should be given to matching peers based on academic experience and performance, and potential personality clashes (Briffa and Porter, 2013; Kinsella and Piersol, 2018; Secomb, 2008). Price and Whiteside (2016) reported that educators developed strategies to support the use of this model including using evidence-based approaches, careful preparation, utilising organisational support, and being positive and pragmatic. However, Dawes and Lambert (2010) found that many practice educators had initially used the model due to short notice requests to take students, rather than a planned approach including training and support, as advocated by Hanson and DeIuliis (2015). Dawes and Lambert (2010) also suggest that success may depend more on the attitudes of educators than the specifics of their clinical setting.
Team model
Team-model placements involving two or more educators sharing the supervision of one student were considered in two papers, both lacking empirical study. Engel et al. (2013) described a team-model placement with a single student, while Beisbier and Johnson (2016) partially reported on a qualitative information-gathering exercise about this model with practice educators. Potential benefits were noted to include increased diversity of learning opportunities for students, increased provision of placements due to reduced impact from part-time work and scheduled days off, and opportunities to support the development of novice educators by including them in the supervisory team. Preparation was seen to be key to ensuring learning opportunities, as was effective communication and flexibility from those involved. Some consideration was given to issues associated with this model, including concerns about additional caseload management challenges and workload; educators being open, honest and prepared was noted as a way of managing this.
Multiple mentoring model
Multiple mentoring describes a team of educators supervising a team of students, essentially combining team and peer-assisted models. Two papers studied this approach, with occupational therapy practice educators (Copley and Nelson, 2012) and social work students (Zeira and Schiff, 2010). Planning to ensure sufficient support and monitoring for students was identified as important by practice educators in Copley and Nelson’s (2012) qualitative study, which also highlighted the importance of educators collaborating with colleagues so that different working practices did not restrict opportunities for student learning. Copley and Nelson (2012) noted that students needed well-developed time management skills to be able to articulate with educators’ differing schedules. As with team models, opportunities for part-time or less experienced therapists to contribute to placement provision were increased.
Zeira and Schiff (2010) followed social work students in a pilot multiple mentoring scheme over 2 years, comparing experiences and outcomes with those receiving the one-to-one model. The only significant differences between models were how students perceived the content of supervision and the relationships with their educators; learning experiences with clients and the development of professional values were unaffected. Zeira and Schiff (2010) reported that the model was ultimately abandoned by educators in favour of the one-to-one model, and that it had not proved cost effective over the 2-year period due to additional costs of training, and providing supervision for educators.
Long-arm supervision
Long-arm supervision is provided by an experienced clinician who is not based at the same location as the student. Examination of this model in 11 papers including three different professions reporting similar benefits associated with professional skills. These include self-confidence, interpersonal skills, and professional independence and identity (Clarke et al., 2014; Mantzourani et al., 2016; Rodger et al., 2009). Dancza et al. (2013) reported generally positive student experiences associated with improved opportunities for clinical reasoning by requiring less demonstration of procedural skills, and identified the development of a stronger professional identify, a claim also made by Thew et al. (2018). Wider benefits beyond student outcomes included the assertion that successful placements could encourage the future utilisation of occupational therapy services (Rodger et al., 2009) or lead to the creation of occupational therapy posts (Kearsley, 2012; Schmitz et al., 2018). Long-arm supervision may create more placement places (Maynard et al., 2015) and can be used intentionally to create placements in specific practice areas (Schmitz et al., 2018).
Limitations of this model included restricted opportunities for professional socialisation, reduced role clarity and increased communication challenges (Maynard et al., 2015; Thew et al., 2008). Collaborating with services unfamiliar with a profession’s role, along with the emotional challenges of practice-based learning, were reported to affect professional identity (Dancza et al., 2013), and Cleak and Smith (2012) found that social work students who experienced long-arm supervision were significantly less satisfied with the learning experience. Dancza et al. (2016) also identified that students receiving long-arm supervision needed additional support to compensate for less frequent contact with an educator. Linnane and Warren’s (2017) survey of occupational therapists and students indicated that while the model was felt to be effective, there was apprehension associated with the lack of access to profession-specific role models and misunderstandings from host services on the student’s role.
The model is often combined with other supervisory approaches, such as peer-assisted learning (Rodger et al., 2009) and project work (Thew et al., 2008). Peer support has been reported as being crucial for long-arm models (Dancza et al., 2013), while the findings of Zuchowski’s (2016) phenomenological study stressed the importance of relationship building, role clarity and ensuring supervisors understand specific placement contexts.
Dedicated practice educator model
Dedicated practice educators have time set aside from normal clinical caseloads so they can supervise several students or provide enhanced support for colleagues providing supervision. This model was only addressed in the paper by Ferguson et al. (2014), which reported its contribution to increased capacity to provide placements in dietetics by improving the support available to newly qualified or part-time practitioners, maintaining student satisfaction.
Project-focused model
This model of practice education sees a student work on a project as the focus of their placement. Student nurses stressed needing time to adjust to this type of experience, and reported initially fearing the scale of a project-focused placement (James et al., 2016). However, James et al. (2016) reported that after completing projects students acknowledged the development of personally and professionally transformative skills. Fortune and McKinstry’s (2012) evaluation of project placements indicated that students and host services both reported development of advanced communication, influencing and leadership skills, along with an increased sense of reciprocity between the education institution and host organisation. However, issues associated with the project models noted by Fortune and McKinstry (2012) included difficulty accessing university support and a perception that they may be less useful than clinically focused opportunities.
Hub and spoke model
Hub and spoke models provide a base (hub) for students with an identified practice educator (PE) but require the student to spend significant portions of a placement with different departments, organisations, institutions or agencies (spokes) who collaborate to provide learning opportunities. Three qualitative studies considered this model; two exclusively from a nursing perspective (Roxburgh, 2014; Roxburgh et al., 2012), and one involving nursing and social work students (McClimens and Brewster, 2017). Reported advantages of hub and spoke models included exposure to complex inter-agency care and deeper understanding of the patient journey, despite initial student concerns about changing location more frequently (McClimens and Brewster, 2017). Roxburgh et al. (2012) concluded that students developed deep learning, empathy and sensitivity to the individual at the centre of the care. Due to the increase in stakeholders, the model needed effective support from the partner education institution (McClimens and Brewster, 2017).
Student-led university-based clinics
In this model, students run clinics for specific populations in the university, with support and supervision from practice educators and academics. Three papers considered this model with both an inter-professional focus and mixed client group (O’Brien et al., 2013), and single profession clinics (Baril, 2013; Wilbur et al., 2017). Group supervision, peer-assisted learning and project work are all embedded in the clinic model, with various benefits being reported. A survey of inter-professional students reported improved understandings of other professional roles and enhanced integrated working skills (O’Brien et al., 2013). Two studies of occupational therapy clinics focused on how clinics were organised more than investigating experiences and outcomes; however, Baril (2013) noted that ensuring sufficient involvement from practising therapists was key to effective supervision and served to improve student experiences, despite initial concerns that the clinic was more like being at university than on placement. Wilbur et al. (2017) described a clinic-based placement, but did not report on outcomes or benefits.
Simulation
Simulated practice placements use mannequins, actors, simulated environments, video or interactive computer packages for learning. No papers considering simulation were initially included; however, the authors became aware of, and included, three papers reporting the development of a simulation framework (Chu et al., 2019), and a subsequent randomised controlled trial (Imms et al., 2018) and economic evaluation (Gospodarevskaya et al., 2019), published after the literature search. Chu et al. (2019) presented a conceptual framework for simulated placements intended to structure the organisation and application of learning and simulation theory. Imms et al. (2018) conducted an RCT with 570 students to investigate the effects of a 40-hour simulated placement, using the framework developed by Chu et al. (2019), compared to traditional placement. Short, high-quality, simulated placements were found to be as effective as traditional placements of equivalent duration in terms of student attainment (Imms et al., 2018). The economic evaluation conducted by Gospodarevskaya et al. (2019) concluded that simulations were more cost effective than traditional placements for healthcare providers, with the opposite being the case for universities. This evaluation also reported that students valued traditional placements ahead of simulations.
Intra-agency collaboration
Van der Riet et al. (2018) studied a model in which nursing students had all of their placements over 3 years within a single healthcare organisation. This model was developed to address a perceived lack of continuity in education experienced by students, while maintaining diversity of experience by attending placements in different specialties. Findings included students experiencing greater feelings of belonging and acceptance, increased confidence and improved learning experiences. Van der Riet et al. (2018) did note, however, that some students suggested they might have benefited from opportunities associated with working with different organisations.
Clinical education wards
Clinical education wards are situated within hospitals but are staffed primarily by students with appropriate support. Manninen et al. (2015) used an ethnographic approach to examine the experiences of nurse educators on a clinical education ward, finding that student learning was facilitated by increased independence, though educators experienced challenges balancing student autonomy, support for learning and patient safety. Manninen et al. (2015) concluded that the education ward model had value because it allowed an equal focus on care provision and student education, and was successful when educators worked effectively as a supervisory team.
Inter-professional placements
Inter-professional placements occur when students from different professional programmes learn collaboratively in practice. McCombe et al. (2008) completed a pilot study using action research methods with social work and nursing students, while Brault et al. (2015) used focus groups to discuss inter-professional placements with students, educators, placement coordinators and managers. Both studies highlighted the importance of partnership between universities and placement sites to ensure logistical issues were solved, such as timing of placements and ensuring sufficient facilitation. Improvements in team working were reported (Brault et al., 2015), along with increased understanding of professional roles and communication skills (McCombe et al., 2008).
Student-led groups
This approach, in which practice education is achieved by groups of students taking responsibility for providing therapy groups, typically for a specific population, was studied by van Patterson et al. (2017). In their paper, occupational therapy placements were focused on the continuing organisation and delivery of several therapy groups for inpatients recovering from brain injuries. Successive group placements were planned with a 1-week handover between student groups. Student groups were usually pairs or trios and supervision was shared by the wider occupational therapy team, using both group and one-to-one methods. Students reported opportunities to enhance communication skills, integrate theory with practice, and develop clinical reasoning and practice, though some felt they missed learning opportunities available in other placement models, such as working one-to-one with service users.
Hybrid approaches
Five papers reported on practice education experiences that used combinations of two or more other distinct approaches. Boniface et al. (2012) developed a pyramidal learning approach that combined peer-assisted learning between UK students and overseas exchange students with long-arm supervision, reporting development of professional autonomy and greater opportunities for experiential learning. A similar approach, combining peer-assisted and long-arm models for a project-focused placement (Thew et al., 2008), reported initial positive student experiences tempered by the need for significant preparation. However, a later evaluation of the same model (Thew et al., 2018) reported clearer benefits in terms of developing professional identity, self-belief enhanced skills and the facilitation of occupation-focused service development and delivery. Knightbridge (2014) also explored a peer-assisted, long-arm project combination, reporting similar areas of benefit: improved experiential learning; growing personal confidence; and enhanced awareness of, and ability to reflect on, wider influences on practice. Rindflesch et al. (2009) reported on a model that combines a dedicated practice educator (termed a clinical education coordinator) providing practice education for groups of occupational therapy and physiotherapy students. The model was reported to be cost effective and increased placement opportunities, while promoting professional development more effectively than the one-to-one model. Supporting people to transition into the dedicated practice educator role was seen as important and key to success.
Discussion and implications
The present mapping review analysed approaches to delivering practice education for health and social care professionals. Key findings from the 53 papers reviewed include notable gaps and limitations, and some clear trends that may be relevant for continuing efforts to increase practice education capacity.
The bubble chart presented in Figure 2 illustrates the sparsity of high-quality primary research and subsequent secondary reviews and analyses that could indicate convincing evidence bases upon which to make practice recommendations. Of the six papers in the high-quality band suggested by Turner-Stokes et al. (2006), three were descriptive reviews of peer-assisted learning, two referred to the same study examining simulation, and one was a well-designed phenomenology of student experience. Most papers were assessed as being moderate or poor quality qualitative and mixed-methods studies, with isolated examples of quantitative designs identified. Combined with the significant degree of diversity in the approaches to practice education reported in the reviewed papers, the current evidence base does not allow clear recommendation for specific models to be made.
A second significant set of limitations relates to how outcomes or effects are considered, specifically the heterogeneity of outcomes examined, the lack of use of validated measures, and limited selection of points at which effects were assessed. With the exception of the RCT by Imms et al. (2018) and its associated economic evaluation (Gospodarevskaya et al., 2019), measurement in quantitative studies focused on narrow outcomes. For instance, the RCT by Sevenhuysen et al. (2014) evaluated the time released for non-student activities and the volume of feedback provided to students, while Zeira and Schiff (2010) and Cleak and Smith (2012) used survey methods to assess satisfaction with the models used. Students’ and practice educators’ satisfaction with and/or opinion of different models also featured prominently in 10 of the 12 mixed methods reviewed. Most of the qualitative studies explored stakeholder experiences and included effects identified and reported by the students and practice educators. These typically related to perceived development of individual competencies or skills, the type and quality of different learning opportunities, and subjective appraisal of value. Overall, few validated methods were used to collect data, and while investigating satisfaction with a new model of practice education is important in establishing whether it is likely to be acceptable to a wider population, it does not provide sufficient evidence for the value of a new approach on other relevant constructs.
While this presents obvious issues with the production of high-quality evidence, it is worth noting that there are few tools available for assessing study outcomes, and it has been recognised that evaluating education methods in health and social care more broadly remains pragmatically and methodologically challenging (Attree, 2006). The work by Imms et al. (2018) comparing the effectiveness of simulation with traditional placements provides an example of perhaps the most well-developed set of outcomes measures, including as primary outcomes written examination results, placement grades and a standard measure of student performance on placement. However, this exemplifies the limits in current evaluation of practice education, which does not tend to extend beyond short-term effects and stakeholder perceptions. The study of new ways of providing practice education would be enhanced by the development of conceptually structured ways of investigating the impact of practice education models that consider wider outcomes, like whether learning transfers to other practice education experiences or environments, and whether there are tangible effects on the quality of service provision. These issues are not exclusive to allied health and social care professions. Authors considering the effects of education initiatives to enhance inter-professional (Freeth et al., 2002) and evidence-based medical practice (Tilson et al., 2011) have noted the lack of valid measurement tools and longitudinal evaluation. In both these examples, Kirkpatrick’s (1998) framework for evaluating training programmes was recommended as a structure to development assessment techniques. This framework proposes assessment of four levels, including reactions to the educational experience and associated learning or skill development, both constructs that were considered by papers in this review, but also behaviour change and results. These latter constructs, which in health and social care could include professional practices and associated benefits to services users, were reported infrequently in the reviewed papers. Various metrics limited to narrow indicators of productivity were reported, such as time spent with services users (Bhagwat et al., 2018), indicators of patient throughput such as the number of people admitted, treated and discharged from a service in a given time period (Dawes and Lambert, 2010; Ferguson et al., 2014) and subjective claims about departmental productivity (Hanson and DeIuliis, 2015).
Despite being the impetus for the development of alternative practice education approaches, whether a model increased individual, team or service capacity to provide practice education was only addressed in six studies. However, as with other outcomes, the different methods used were not sufficient to make convincing or consistent claims about the contribution of specific models. Approaches used to evaluate effects on placement capacity included comparing the number of students provided with a placement over a given time period (Ferguson et al., 2014; Reidlinger et al., 2017), collecting qualitative feedback from health professionals about capacity (McCombe et al., 2008; Maynard et al., 2015; Schmitz et al., 2018), and the authors’ opinions (Rindflesch et al., 2009). While observing the number of placements offered and asking stakeholders to estimate effects on capacity may be practical, and can be achieved with a good degree of reliability, focusing solely on capacity without concurrently considering the associated quality of practice education approaches is an issue. Significantly increasing the number of placement opportunities may come at the expense of learning outcomes, student and educator satisfaction, and ultimately service quality and related service user outcomes. Few reviewed papers consider this potential compromise, though the pilot study of long-arm supervision by Roberts et al. (2009) suggested that an increase in student placement hours compared to a traditional one-to-one model was not associated with negative impacts on student achievement or service resource demands. Two RCTs examining peer-assisted learning (Sevenhuysen et al., 2014) and simulation (Imms et al., 2018) both found that student performance was comparable with the one-to-one model, which was used as a control. While the study by Sevenhuysen et al. (2014) found no difference in educator workloads or service provision, its sample size (n = 24) may not have been sufficient to detect changes. Conversely, the RCT by Imms et al. (2018) was adequately powered, but the associated economic evaluation (Gospodarevskaya et al., 2019) did not examine changes in service productivity associated with the presence or absence of students.
While this review demonstrates there is no consistent high-quality evidence for the effectiveness of specific models of practice education, the range of different models used, their various descriptions and the degree of crossover between approaches suggests that there are many ways of delivering practice education, each of which has the potential to be effective. Most studies either reported positive findings or found the model being studied to be as effective as one-to-one supervision. While this may be attributable to publication bias, the results of qualitative methods, along with authors’ interpretations and discussion, provide some useful insights into the challenges associated with developing and implementing different practice education models.
The first of these insights is the importance of preparation. The use of different practice education models is typically associated with new ways of learning and practices for supporting this. Ensuring students and practice educators were informed of underlying theories, supervision and support methods, and had sufficient time to plan for alternative ways of working, were among the recommendations or discussions noted in 11 papers (see Table 2 for details). Effective communication between different stakeholders was noted to be a key component of these preparations. Second, the perceived benefits associated with using non one-to-one models typically reflect advanced professional skills, rather than specific technical competencies. Self-confidence or self-belief, personal and professional autonomy, independent learning skills, professional identify, interpersonal skills, and organisation and time management abilities were reported to be associated with different practice education models. Finally, initial concerns about adopting new models tend to dissipate over time for both students and practice educators. For students this occurred once initial unfamiliarity or uncertainty had passed (James et al., 2016; Knightbridge, 2014; McClimens and Brewster, 2017). For practice educators, it appears that concerns and issues can decrease once sufficient time has elapsed for them to develop the skills and experience needed for new forms of practice education (Beisbier and Johnson, 2016; Copley and Nelson, 2012; Rindflesch et al., 2009; Roberts et al., 2009). However, these tend to be anecdotal reflections on the implementation of new models, and one longitudinal study considering a multiple mentoring approach in social work education ended with this approach being abandoned after 2 years following difficulties managing a range of organisational and interpersonal issues (Zeira and Schiff, 2010).
However, it is also worth noting that, despite these possible benefits, it was more common for students to express preference for, or higher levels of satisfaction with, the traditional model of one-to-one supervision than an alternative. This trend was seen in the papers that explicitly addressed student preference of satisfaction between different approaches to practice-based learning, including simulation (Gospodarevskaya et al., 2019), peer-assisted learning (Kinsella and Piersol, 2018; Sevenhuysen et al., 2014) and long-arm supervision (Cleak and Smith, 2012; O’Connor et al., 2012). When reported, explanations for this preference included concerns about reduced quality and quantity of supervision when using alternative models (Kinsella and Piersol, 2018; Sevenhuysen et al., 2015), it being easier to demonstrate autonomous working in one-to-one relationships (O’Connor et al., 2012) and reduced opportunities to observe the practice educator. There would be value in developing further understanding of why this preference for the one-to-one student–educator model prevails. Most of the alternative models of practice education require different educator to student ratios, application of different learning theories, or changes to the relative location of students and educators. Understanding why these do not currently lead to the same level of satisfaction among students may inform how these models are developed and applied.
Limitations
Limitations of this review must be considered. First, while attempts were made to identify comprehensively papers examining practice education models used by relevant health and social care disciplines from a range of databases, inconsistencies in terminology required complicated search strategies that may not have captured all approaches used. Second, as the mapping review methodology enables categorisation of practice models, but does not offer in-depth appraisal and synthesis of included papers, the findings presented are not intended to indicate synthesised evidence supportive of practice recommendations. Finally, while the inclusion of a high number of disparate types of paper is important for identifying and organising potential models, there is risk of oversimplification, and interested readers may need to consider the original works for a full picture of the approaches and methods used.
Conclusions
Fourteen models of practice education were identified in the 53 reviewed papers, though the terms used to describe these, and the methods used to study them, vary and were typically of moderate or low methodological quality. Most approaches were reported to have benefits for students and/or practice educators and their services, although comparatively few high-quality objective studies were identified examining these outcomes. When experimental or observational designs were used, outcome measurement was narrow, reflecting wider, persisting issues associated with evaluating the effect of education and training initiatives. A variety of practice education approaches may increase capacity while maintaining quality, but the development of more effective ways of studying outcomes is needed, particularly those that allow for consideration of effect beyond immediate impact and measures of stakeholder reaction. From a practical perspective, the effectiveness of different models may be determined by the degree to which they can be operated within the constraints of local contexts. Although the articles included in this review present multiple ways of delivering practice education in disparate scenarios, the typology and associated evidence map provided may offer some structure for those who are involved in developing and evaluating methods to facilitate practice-based learning for health and social care professionals.
Key findings
Many different practice education models are used, but there is little high-quality research into their effectiveness. New methods for examining the effectiveness of practice education are needed. Further research is needed into why the one-to-one model is associated with higher levels of student satisfaction. Consistent terminology and expanded consideration of impact would support future study.
What the study had added
This review expands and updates previous work considering practice education models. It provides an up-to-date evidence map that represents approaches used in different disciplines, and presents an organising typology to support further discourse.
Footnotes
Research ethics and consent
Ethics review and consent were not relevant for this mapping review as it involved no participants.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: funding for this review was provided by the Royal College of Occupational Therapists as part of a contract awarded to Queen Margaret University to complete the project ‘Reviewing the Royal College of Occupational Therapists’ role in supporting practice education’.
Contributorship
Joanna Beveridge and Duncan Pentland developed and executed the search strategies, screened and reviewed the returned records, extracted information and drafted the manuscript. Both authors viewed and edited the manuscript and approved the final version.