
Abstract
Introduction
A national survey was conducted with United Kingdom (UK) occupational therapists to scope occupational therapy service provision for people with dementia and their family carers in the community.
Method
This was an online questionnaire with topics on occupational therapists’ roles, service provision, referral, assistive technology and assessment tools. Recruitment was through direct invitation, and promotion via occupational therapy networks, websites and newsletters.
Results
A total of 197 responded. Occupational therapy referrals most commonly came from the multidisciplinary team. Over half primarily undertook profession-specific work, with occupational therapy assessments the most common profession-specific task. Two-thirds of referrals for initial assessments were for people with mild-to-moderate dementia. A median of 2.5 hours for assessment/intervention was spent for each person with dementia. Almost two-thirds used the Model of Human Occupation Screening Tool. Most could prescribe personal activities of daily living equipment and Telecare, with few able to prescribe equipment for reminiscence or leisure.
Conclusion
This national survey increases knowledge of UK community occupational therapy practice and service provision for people with dementia and their family carers. It informs occupational therapists about national trends within this practice area, and development of the community occupational therapy intervention (COTiD-UK) as part of the Valuing Active Life in Dementia research programme.
Introduction
It is estimated that 835,000 people have dementia in the United Kingdom (UK) (Alzheimer’s Society, 2014). Approximately two-thirds of these live in the community (Knapp et al., 2007), with around 670,000 people in the UK providing unpaid, regular care and support for a person with dementia (Alzheimer’s Society, 2012). The National Institute for Health and Clinical Excellence/Social Care Institute for Excellence (NICE/SCIE, 2006) practice guideline for supporting people with dementia and their carers recommends occupational therapists provide skills training for activities of daily living (ADLs), as well as advising on environmental modification and assistive technology to help maintain independence. Furthermore, the Memory Services National Accreditation Programme (MSNAP) Standards (Royal College of Psychiatrists, 2014) state that people with dementia should have access to person-centred occupational therapy in order to help maintain their health and wellbeing. However, there is little information about the level and content of occupational therapy practice with this client group.
Few studies have evaluated the benefits of occupational therapy for people with dementia living in the community. In the Netherlands, Graff et al. (2006) used the Model of Human Occupation (MOHO) (Kielhofner, 2008) to underpin the development and evaluation of the Community Occupational Therapy in Dementia (COTiD) programme: ten, 1-hour sessions of home-based occupational therapy provided over 5 weeks. Benefits to ADL skills, quality of life and mood for people with dementia, and improved quality of life, enhanced mood and sense of competence in carers were demonstrated (Graff et al., 2006). It was also cost effective (Graff et al., 2008).
A trial of COTiD in Germany highlighted the importance of adapting complex interventions into a local context for cross-national comparison and evaluation to be effective (Voigt-Radloff et al., 2011). COTiD could potentially address key National Dementia Strategy objectives (Department of Health, 2009) and the Prime Minister’s Challenge on Dementia (Department of Health, 2015), but needs to be adapted to maximise its usefulness to the UK service context and culture. The Valuing Active Life in Dementia (VALID) research programme aims to develop and evaluate a community occupational therapy intervention for people with mild to moderate dementia and their family carers in the UK (COTiD-UK). In order to inform the development of the COTiD-UK training package and intervention as well as a forthcoming randomised controlled trial (RCT), a national survey was conducted with UK occupational therapists to scope occupational therapy service provision for people with dementia and their family carers living in the community.
Method
Design
Subsequent to the research study receiving ethical approval, a cross-sectional survey was conducted using an online questionnaire that was designed and hosted via a web-based service. The questionnaire was developed by reviewing relevant literature and feedback from occupational therapists in the research team as well as experienced practitioners. Closed and open questions focused on the role(s) of occupational therapists, service provision, referral routes, availability of equipment and assistive technology, and use of assessment tools. An additional and optional section designed to collect participants’ demographic and contact details was accessed via a link at the end of the questionnaire. Those that did complete this additional section were eligible to be entered into a gift vouchers prize draw.
The draft questionnaire was reviewed by the VALID expert occupational therapy reference group to confirm its face validity. It was piloted with a group of 26 local occupational therapists to assess ease of use, the clarity of questions and approximate time needed for completion. The pilot led to revisions: additional categories and remedying functional errors with online completion. The final version took approximately 20 minutes to complete.
Recruitment
A number of recruitment strategies were used to achieve the optimum number and range of responses from occupational therapy staff. Invitations were sent to National Health Service (NHS) Memory Services registered with the MSNAP database and over 400 Community Mental Health Teams (CMHTs) listed on the Personal Social Services Research Unit (PSSRU) database. The survey was also promoted online via the following websites: VALID, York St John University’s Research Centre for Occupation and Mental Health (RCOMH), the College of Occupational Therapists (COT) Specialist Section – Older People in addition to presentations at memory service networking days and OTnews, the magazine of the British Association/College of Occupational Therapists (BAOT/COT).
Procedure
Invitations to participate in the survey were predominantly sent electronically with a link to the questionnaire and an introductory message that outlined the study. Participants were required to read a Participant Information Sheet and confirm they were providing informed consent before proceeding to the questionnaire. The CMHTs on the PSSRU database were sent postal invitations which comprised a Participant Information Sheet and a covering letter that included the website address to access the survey. All invitations included the relevant contact details with details of how to obtain a print copy of the questionnaire should it be required. However, all responses were made online, with no print copy versions requested. The questionnaire was available for completion for 4 months between February and June 2013. Electronic reminders were sent after 8 and 14 weeks.
Data analysis
The responses were exported into a SPSS file (IBM SPSS Statistics Version 21) and screened for errors and omissions to ensure data integrity. Descriptive statistics were calculated, which included totals (n), percentages, as well as ranges, the median, means and standard deviations.
Results
Percentages of the total responses as well as totals (n) are reported.
Demographics
The optional demographics section was completed by 70% (138/197) of respondents. The majority were female, n = 124 (90%), with ages ranging from 18 to 60+, with the highest proportion of individuals in the 40–49 category (n = 55, 40%). Nearly all respondents worked in the NHS (n = 133, 96.4%), with others working in social enterprise or local authorities. Over half of respondents had been qualified for over 10 years (n = 84, 61%). All respondents worked for an organisation that used the ‘Agenda for Change’ banding criteria: Bands 5 (newly qualified, junior practitioner) to 8 (managerial or consultant level) therapists were represented, with three-quarters employed as Band 6 (experienced therapist) or 7 (clinical specialist therapist or team leader). Two-thirds of respondents were employed full-time (n = 93, 67%), with two-thirds of the part-time staff working 21+ hours per week. Respondents were primarily based in a number of different regions of England (n = 125, 91%), but Scotland (n = 7, 5%) and Wales (n = 6, 4%) also featured. Although a number of service bases were identified, the majority of respondents were based in CMHTs/Community Recovery Teams (n = 89, 65%), with just over a third based in a memory service (n = 48, 35%).
Referral to occupational therapy
Most indicated that people with dementia were allocated to occupational therapy by referral from within the multidisciplinary team (n = 113, 74%). Other allocation methods included allocation team meetings (n = 99, 65%), direct referral (for instance from a general practitioner (GP); n = 22, 14%), as a result of supervision (n = 13, 9%) and ‘Other’ (n = 14, 9%), which included duty triage (a designated health professional who screens new referrals; n = 4, 3%), allocation by a manager (n = 3, 2%) and blanket referral (whereby there is a prior agreement in place that any service user can be seen without the need for an individual referral; n = 3, 2%).
Occupational therapists’ roles
Occupational therapy-specific tasks
Occupational therapy-specific tasks undertaken by respondents.
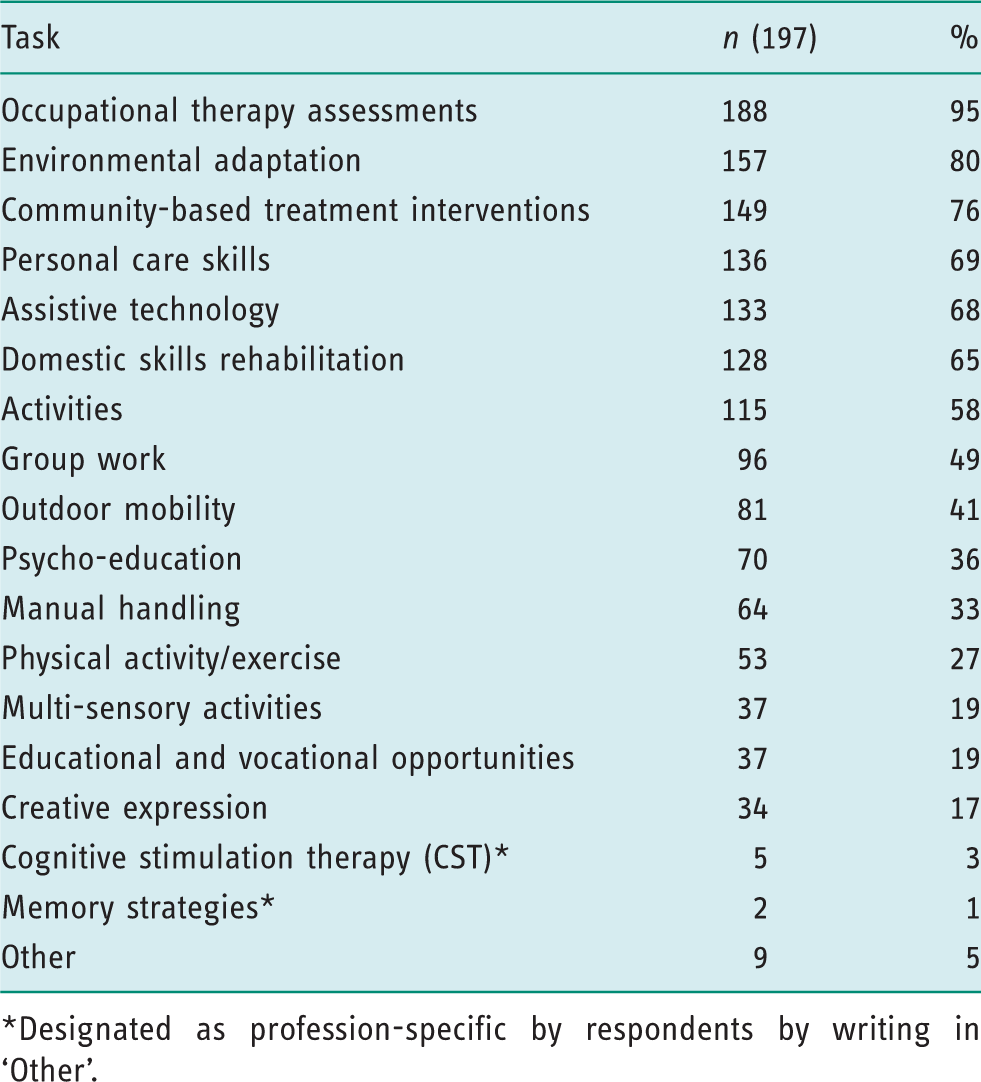
Designated as profession-specific by respondents by writing in ‘Other’.
Generic tasks
Generic tasks undertaken by respondents.
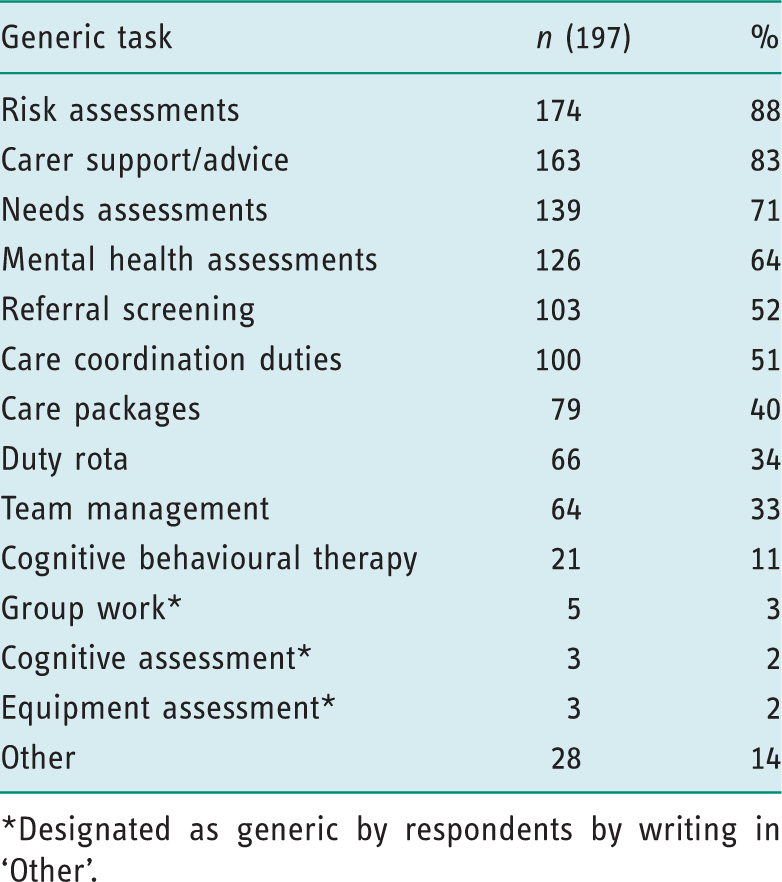
Designated as generic by respondents by writing in ‘Other’.
Generic: Specific work ratio
Over half of respondents (n = 112, 56%) spent the majority of their time undertaking profession-specific work. Nearly all respondents (n = 183, 93%) spent their time doing both generic and profession-specific work.
Occupational therapy provision
On average, respondents (n = 153) had seen 6.47 (range: 0–25; SD = 5.24) people with dementia for initial occupational therapy assessment in the preceding month. On average, 4.14 (range: 0–18; SD = 3.35) of these people were in the mild to moderate stages of dementia.
Data on the number of assessment and intervention sessions provided to people with dementia are shown in Figure 1.
Respondents indicated the average number of 30-minute occupational therapy assessment/intervention sessions provided to a person with dementia (n = 153).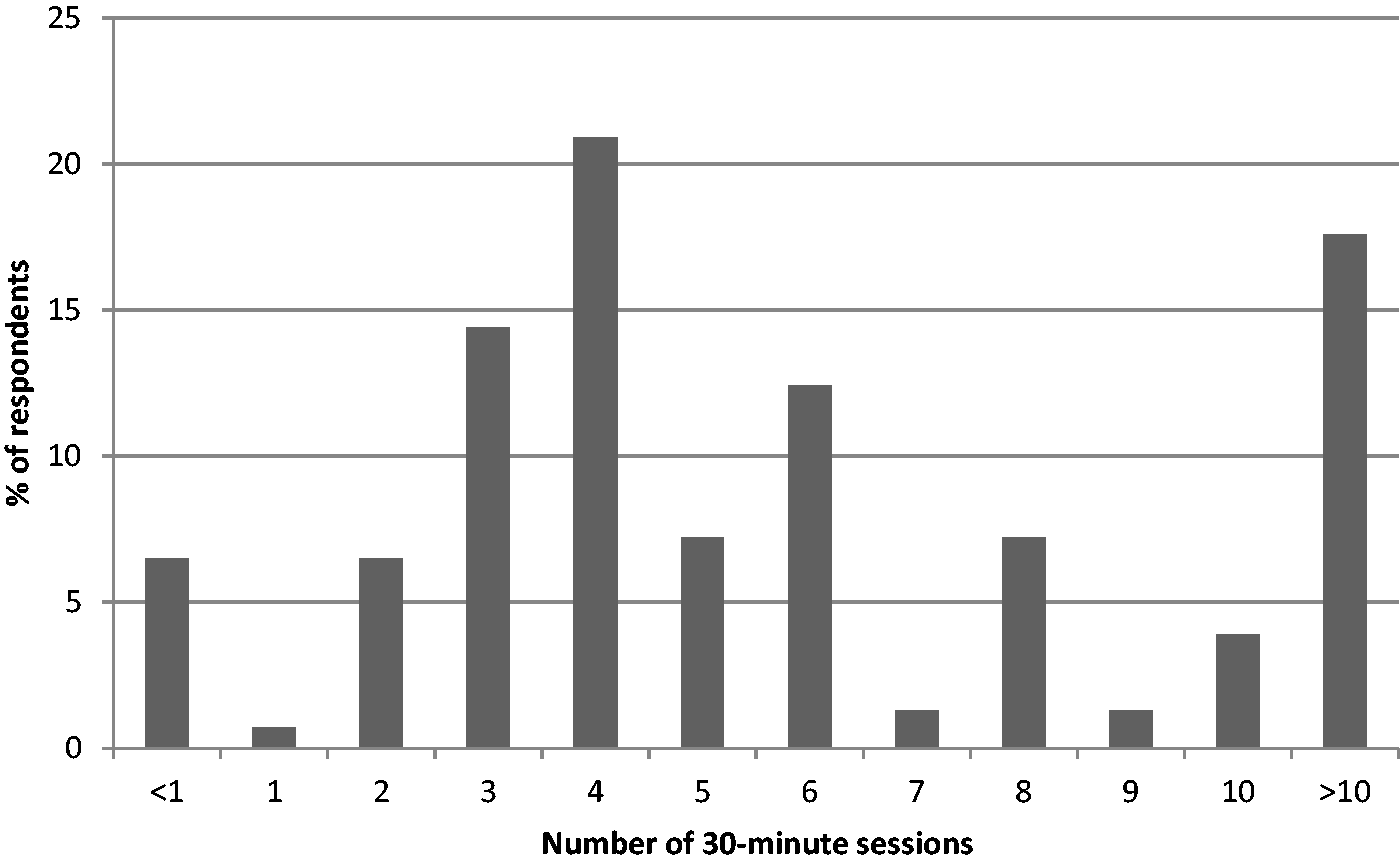
Assessment tools: Occupational therapy-specific
Occupational therapy-specific assessments used by respondents.
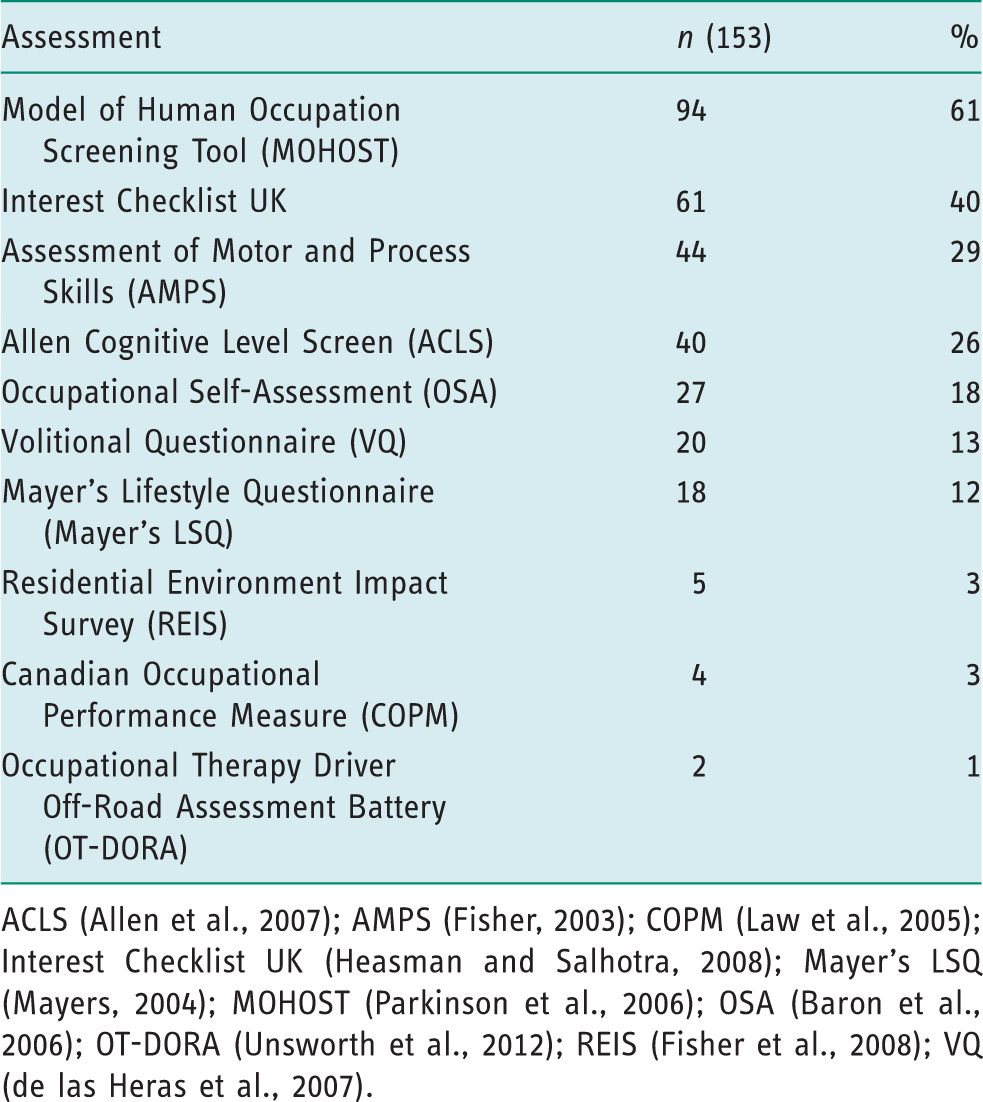
ACLS (Allen et al., 2007); AMPS (Fisher, 2003); COPM (Law et al., 2005); Interest Checklist UK (Heasman and Salhotra, 2008); Mayer’s LSQ (Mayers, 2004); MOHOST (Parkinson et al., 2006); OSA (Baron et al., 2006); OT-DORA (Unsworth et al., 2012); REIS (Fisher et al., 2008); VQ (de las Heras et al., 2007).
Assistive technology and equipment
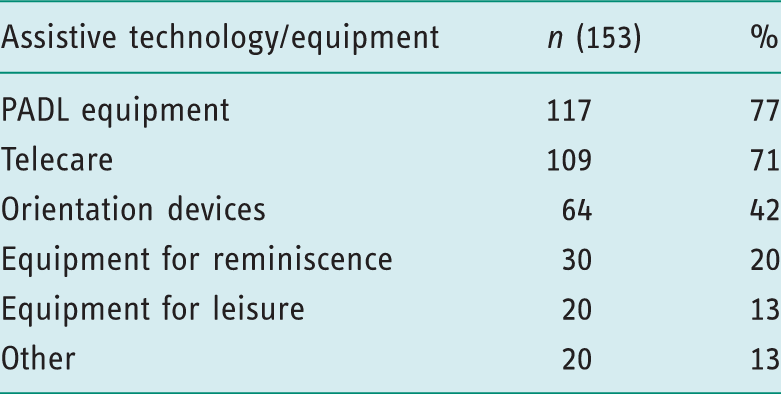
Nearly all respondents (n = 151, 98%) prescribed assistive technology or equipment.
Assistive technology and equipment available to prescribe.
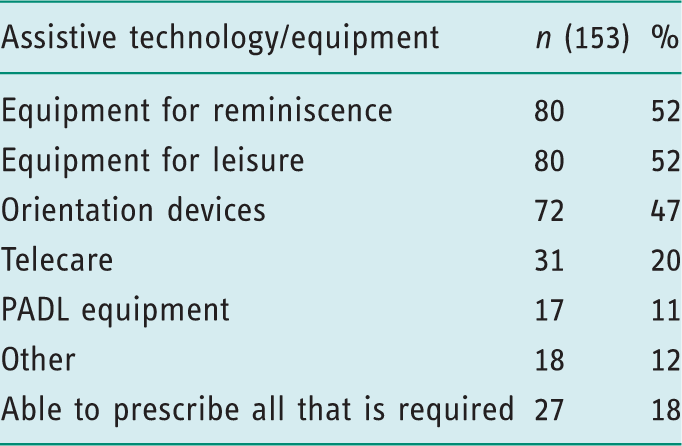
Assistive technology and equipment respondents would like to prescribe (but are unable to).
Discussion
This survey aimed to scope UK occupational therapy practice and service provision for people with dementia and their family carers living in the community.
The demographic data reveal some homogeneity in the respondents’ characteristics; unsurprisingly, most were female and working in the NHS. However, the sample was heterogeneous in other variables, such as age, banding, qualification length, working hours, geographical location and service base. As such, respondents were from a diverse population of occupational therapists working with people with dementia and family carers in the community, and so provide a broad picture of current UK practice and service provision.
As 74% of referrals to occupational therapists were made from within the multidisciplinary team, there is a need to ensure that other team members are well informed about the role of occupational therapy for people with dementia and their family carers in the community so that occupational therapists receive timely and appropriate referrals.
Most respondents carried out both generic and profession-specific work, which is similar to Harries and Gilhooly’s (2003) findings of occupational therapists’ work in CMHTs. Furthermore, although Reeves and Summerfield Mann (2004) identified a growing trend of generic working in CMHTs, in community dementia care at least there remains a considerable proportion of profession-specific working, with over half of respondents spending the majority of their time undertaking occupational therapy-specific work, as opposed to generic work. The higher ranked profession-specific tasks such as environmental adaptation, personal care skills and assistive technology reflect the role of occupational therapy as described in the NICE/SCIE guidance (2006) and MSNAP standards (Royal College of Psychiatrists, 2014). Importantly, this survey did not seek to assess the effectiveness or benefits of generic or profession-specific working in occupational therapy; rather, it aimed to identify trends as an addition to the statistical knowledge base for practice in this service area.
The results show that, on average, almost two-thirds of referrals for initial occupational therapy assessments were for people in the mild to moderate stages of dementia. This could indicate the shift towards earlier diagnosis as outlined in the National Dementia Strategy (Department of Health, 2009) and recognition of the potential role for occupational therapy in identifying and managing risk. There was variation in the responses regarding the time spent delivering assessment/intervention for people with dementia and their carers, with a median of 2.5 hours being provided. It is important to highlight that these data do not provide any detail about the percentage of time allocated for either assessment or intervention which would be expected to vary between service settings.
A variety of occupational therapy-specific assessment tools were used by respondents, with MOHO-based tools featuring most frequently; primarily the MOHOST, followed by the Interest Checklist UK and AMPS. There are few published data on the use of the MOHOST with people with dementia, but it is included within a study protocol for a RCT of Telecare (Leroi et al., 2013) and also research on the development of care pathways (Lee et al., 2011). The results reflect the recommendations in the COT’s position statement on the importance of using standardised assessments/outcome measures (COT, 2013). Moreover, they suggest that there has been progress since Unsworth’s (2011) summation of evidence that the use of standardised assessments in general is not widespread.
Previous work has identified discrepancies in the provision of the different types of equipment and assistive technology available (Audit Commission, 2000). Lett et al. (2006) found that despite the implementation of the Fair Access to Care Services (FACS) framework (Department of Health, 2002) it was rarely used as the sole eligibility criteria for equipment provision by local authorities in England, with a considerable proportion indicating that there was equipment that still would not be provided even if clients were eligible. This survey’s results indicate that PADL equipment and Telecare were most frequently available to prescribe, whereas other categories, including orientation devices and equipment for reminiscence and leisure, were less available. Furthermore, many respondents felt that prescription of this lesser available equipment and assistive technology should be a part of their practice. Indeed, the prescription of such equipment and assistive technology could support occupational therapists in adhering to best practice guidelines for dementia (NICE/SCIE, 2006; Royal College of Psychiatrists, 2014) with regard to environmental modification and reminiscence therapy delivery, and also in promoting healthy ageing by enabling participation in leisure (World Health Organization, 2015).
The survey also informed the VALID research programme in a number of areas, including the content of the COTiD-UK training and intervention, as well as research processes. When developing the training programme, it is relevant to note that many of the trainees are likely to already have experience of working with people in the mild to moderate stages of dementia and their carers and using the MOHOST in practice, and hence a working knowledge of the underpinning MOHO theory.
The median of 2.5 hours of assessment/intervention is in sharp contrast to COTiD-UK, which provides an average of 10 hours of occupational therapy contact time with both the person living with dementia and the family carer, highlighting a potential resource issue which will need to be discussed with participating occupational therapists, and authorised by their managers and services when recruiting trial sites. The fact that over half of respondents were undertaking primarily profession-specific work is encouraging for implementing an occupational therapy-specific intervention like COTiD-UK as this will require less of a shift in culture and resource allocation. The inconsistencies of equipment prescription may impact on the provision of COTiD-UK across the range of research sites depending on local policies and procedures, and occupational therapists will be asked to note this type of issue when submitting fidelity data.
In terms of informing research processes, the survey results supported development of a template that will be used to define ‘treatment as usual’ (TAU) in each research site involved in the forthcoming RCT, as the provision of TAU will inevitably vary between and within sites. Furthermore, as almost two-thirds of people referred to occupational therapists had a diagnosis of mild–moderate dementia, it suggests that there will be a suitable pool of people that can be recruited as part of the VALID RCT, and who may potentially benefit from COTiD-UK. As 74% of referrals to occupational therapists are made internally, there is also a need to ensure that other mental health team members are well informed about the intervention in terms of target clients, COTiD-UK aims and content, and how to refer potentially suitable people.
Limitations
Despite the usefulness of the data, there are some limitations to be considered. The majority of questions had predefined answers for respondents to select, resulting in a smaller amount of qualitative data for analysis. Using additional qualitative methodologies would allow the gathering of more in-depth information (Bowling, 2009) which may provide insights into occupational therapy provision not available through a primarily quantitative survey. On reflection, some response options such as ‘community-based treatment interventions’ proved to be somewhat ambiguous, highlighting the need to clearly define the terminology used in questionnaires.
Respondents were also able to leave a number of questions unanswered, meaning the number of responses varied across questions. Accordingly, this reduced the representativeness and consequent generalisability of any findings. Therefore, future questionnaires should ensure that, where appropriate, questions are mandatory in order to obtain a fuller set of data.
Finally, the categorisation of profession-specific and generic tasks could be open to debate. Respondents were asked about their ratio of generic and profession-specific working having been provided with examples in previous questions, and, as such, may have been influenced when indicating their generic and specific work ratios.
Conclusion
This national survey increases knowledge of UK community occupational therapy practice and service provision for people with dementia and their family carers. It informs occupational therapists about national trends within this practice area and the development of a community occupational therapy intervention (COTiD-UK) to be evaluated in a forthcoming RCT as part of the Valuing Active Life in Dementia research programme.
Key findings
Over half primarily undertook profession-specific work. Almost two-thirds used the MOHOST. Most could prescribe PADL equipment and Telecare, with few able to prescribe equipment for reminiscence or leisure.
What the study has added
This national survey has increased knowledge of occupational therapy practice and service provision in the UK for people with dementia and their family carers living in the community.
Footnotes
Acknowledgements
The VALID research team would like to thank the occupational therapists who responded to the survey and the organisations that promoted it. A special thanks also to the VALID external expert occupational therapy reference group and the occupational therapists who piloted the survey. The authors are grateful to William Pearson for his work on data collation. Finally, the VALID research team acknowledges the support of the National Institute for Health Research Clinical Research Network.
Research ethics
The study was approved by the Yorkshire and The Humber – Leeds West Research Ethics Committee, Reference number: 12/YH/0492. The study was also granted NHS Research & Development approval (Reference number 13762).
Declaration of conflicting interests
The authors confirm that there is no conflict of interest.
Funding
This paper presents independent research funded by the National Institute for Health Research’s Programme Grants for Applied Research Programme (RP-PG-0610-10108). The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.