
Abstract
For women in prison, having safe and supportive relationships is the greatest predictor of staying safely out of custodial systems, post-release. We describe the development and delivery of ‘Strengthening Connections’: an in-prison family therapy service in Victoria, Australia that supported women to strengthen their relationships with family and allies to reduce recidivism risk. We piloted a stepped-care model comprising three levels of service delivery to support women’s relational health: 1) group-level sessions, 2) single-session family therapy, and 3) systemic family therapy approaches involving women along with their family or allies. We developed a trauma-informed, culturally safe approach to practice, and evidence-enriched resources for use in service delivery. During the three-year service pilot, we continuously improved on the service based on clinical consultations and process evaluation findings. This article describes the development, refinement and delivery of the service with reflections on potential for broader application.
Introduction
In Australia and globally, the number of women in prison has been increasing at a faster rate than the number of men in prison (Australian Institute of Health and Welfare, 2020). Women in prison have complex health and wellbeing needs and require access to gender-specific services (Australian Institute of Health and Welfare, 2020; Bartlett & Hollins, 2018). For example, compared to male prisoners, women are more likely to have Acquired Brain Injuries (Woolhouse et al., 2018), a history of physical and sexual abuse, alcohol and other drug dependence, and higher rates of mental health challenges (Australian Institute of Health and Welfare, 2020). Women prisoners also have unique needs where support for recidivism risk is concerned. Importantly, for women in prison, safe and supportive relationships have been identified as the greatest predictor of the ability to stay safely out of corrections systems, post-release (Farmer, 2019).
Recidivism can be defined as a person’s episode of incarceration following a period of release from prison after prior incarceration. Typically, efforts to reduce recidivism for individuals in prison are focused on targeting ‘criminogenic needs.’ Criminogenic needs relate to ‘dynamic’ or modifiable risks based on factors such as substance use, education, employment, antisocial cognitions, leisure activities, and relationships with family or intimate partners (Kreis et al., 2014). There is evidence that criminogenic needs are gendered; that is to say, the interventions that work well to reduce recidivism for women are different from those that work well for men (Kreis et al., 2014). In a meta-analysis evaluating intervention programs for women in prison, programs focused on interpersonal criminogenic needs yielded the strongest positive associations with reduced reoffending of all targets considered (Dowden & Andrews, 1999). These interpersonal criminogenic needs involved family processes (specifically, characteristics of affection and appropriate supervision) and antisocial associates (increased contact with prosocial peers and decreased contact with antisocial peers). Factors related to family process were especially relevant to reduced reoffending in this study (Dowden & Andrews, 1999).
The key relational factors relevant to recidivism risk for women are summarized below from the available literature. Most are dynamic, i.e., modifiable, and some – i.e., family of origin factors and historic experiences of victimization – can be considered ‘static’ or unchangeable yet are also important targets for relationally focused intervention. Of course, relational risk factors exist alongside other factors such as mental health, substance use and self-efficacy and may influence and be influenced by these individual variables. Support for women in prison should be delivered with consideration of the complex interaction of these factors (Kreis et al., 2014).
Family of origin factors are related to women’s recidivism risk and include poor-quality family relationships including those characterized by low affection (Dowden & Andrews, 1999), poor-quality interparental relationships (Cobbina et al., 2012), and non-rewarding relationships with one’s parents and other relatives (van der Knaap et al., 2012). These factors are highly predictive of women’s chances of both incarceration and recidivism and are therefore key to consider in support or intervention work.
Current family support markedly reduces women’s recidivism risk and includes both emotional and practical support (Rettinger & Andrews, 2010). Maintaining contact with family members while in prison has been associated with women receiving more emotional and instrumental support after release, as well as a reduced chance of recidivism (Bales & Mears, 2008; Barrick et al., 2014).
Intimate partner relationship factors such as traumatic, conflictual or violent intimate partner relationships, and living with a criminal partner (Benda, 2005; Cobbina et al., 2012; Rettinger & Andrews, 2010; Salisbury & Van Voorhis, 2009; van der Knaap et al., 2012) are centrally relevant to women’s incarceration and recidivism risk.
For women who are parents, parenting concerns associated with recidivism include parental stress, not living with children after incarceration, and less frequent contact with children (Dowden & Andrews, 1999; McClure et al., 2015). There is evidence that correctional programs aimed at strengthening parent-child affectional bonds, supporting attachment maintenance, and supporting parenting sensitivity have a protective effect on offspring in this context (Goodwin & Davis, 2011; Perry et al., 2011).
Various forms of victimization are associated with recidivism risk among women and include adult abuse as a perpetrator or victim, trauma associated with family violence (Carlton & Segrave, 2015), and neglect and family breakdown.
Peer relationships are also relevant to women’s ability to stay safely out of prison post-release. Features of peer relationships that are detrimental here include relational tensions or problems with friends and acquaintances (van der Knaap et al., 2012); having ‘criminal peers’ (Benda, 2005; Rettinger & Andrews, 2010) and reduced engagement in prosocial activities (Cobbina et al., 2012).
Targeting criminogenic needs is the essence of the well-established Risk-Needs-Responsivity (RNR) model, which includes three core principles that guide intervention with offenders (Ward et al., 2007). The ‘risk’ principle assumes that offenders at higher risk for recidivism will benefit from higher levels of intervention, and that offenders at lower risk for recidivism should receive routine or no intervention. The ‘needs’ principle suggests that only criminogenic needs should be targeted in intervention. The ‘responsivity’ principle states that correctional programs should be tailored to individual characteristics including learning style, level of motivation, and personal and interpersonal circumstances (Ward et al., 2007).
According to the RNR model, correctional interventions should be primarily directed at reducing future risk of offending and are generally only indirectly related to improving the quality of clients’ lives (Ward & McDonald, 2022). A typical application of the RNR model prioritizes the values of caution for community wellbeing (reduced harm to the community) over the values of client fulfilment and wellbeing (Ward & McDonald, 2022). The RNR model therefore has gaps where cultural safety and personal identity are concerned and does not pay close attention to ‘non-criminogenic needs’ including self-esteem and distress, even though these are important to therapeutic process and the outcomes of correctional programs (Ward et al., 2007). More recent practice frameworks (Ward & Durrant, 2021; Ward & McDonald, 2022) acknowledge these limitations and suggest alternative or additional ways to approach interventions that see person-centered values as a reason for action, such as the human entitlement to a safe and meaningful life in the community and the value of helping people maximize their wellbeing in prison through learning and goal setting.
Care must be taken when designing and delivering gendered approaches to correctional interventions as they can result in the application of gender as a uniform category based on sex alone, with unintended consequences of further marginalizing diverse groups, including the gender diverse and racially diverse (Carlton & Segrave, 2015; Hannah-Moffat, 2009). Intersectional approaches are therefore needed whereby the interrelationships between gender, culture, language, class and ability are taken into consideration. In Australia, there is significant overrepresentation of First Nations women in prison: Aboriginal and Torres Strait Islander women make up around a third of the female prisoner population (Australian Institute of Health and Welfare, 2020). Culturally and Linguistically Diverse women are also overrepresented, especially Vietnamese women (Australian Institute of Health and Welfare, 2020). Developing models of care that are culturally safe is critical to meeting the diverse needs and lived experiences of these different groups. First Nations people in Australia and other colonized countries experience systemic disadvantage that perpetuates worse socioeconomic and health outcomes compared to non-Indigenous people (Australian Institute of Health and Welfare, 2020). To properly address this, culturally safe policy should be Indigenous led, with approaches that prioritize Indigenous experiences and ways of knowing (Fisher et al., 2021). Culturally safe practice in healthcare and other systems involves processes of decolonization that address racism and uphold Indigenous self-determination. Being culturally safe means engaging in meaningful dialogue and intentionally reducing power differences (Fisher et al., 2021), which can be difficult to achieve in correctional settings yet is critical to safe and equitable practice.
In response to the problems outlined above, we developed and piloted ‘Strengthening Connections,’ an in-prison stepped care family therapy service for supporting women to strengthen their relationships with family and other close supports, with the overall objective of reducing recidivism risk such that women may go on to have safe and meaningful lives in the community. The aim of this article is to provide an overview of the service in order to contribute to current theory and practice involving women in corrections. We first describe the development and refinement of the service model according to a) evidence enrichment and b) clinical and stakeholder consultancy processes. We then outline the structure of the stepped-care service model and describe its core features and guiding principles. Finally we describe our refinement of the Strengthening Connections service model via process evaluation findings across the three-year service pilot, and reflect on potential for broader application of similar therapeutic programs.
Program Setting
The Strengthening Connections service was developed and delivered by our team at The Bouverie Centre, a specialist family therapy clinic and research center of La Trobe University, within the following context.
Funding for an in-prison family therapy service was provided for a three-and a-half-year pilot period as part of a statewide service and sector initiative in Victoria, Australia, aiming to strengthen supports to women in custody, with the overall goal of reducing the number of women returning to prison post-release. The 2019–20 Victorian state budget provided $19.967 million over four years to reduce incarceration of which $14.5 million was dedicated to a Women’s Justice Diversion and Rehabilitation Strategy. The Strategy was designed to contribute to the reduction target of 200 prison beds for women by 2027 and included various initiatives to address the complex and often intersecting needs of women in the correctional system. The Strengthening Connections service was commissioned as part of this strategy to develop an in-prison, evidence informed family therapy service, via a tiered service framework that could support women in prison and their families or allies, to maintain or re-establish appropriate connections to enhance women prisoners’ reintegration into community and family life. The pilot was to include a culturally appropriate service response for First Nations women, who are vastly overrepresented in the Victorian state custodial system (Australian Bureau of Statistics, 2025). First Nations women are currently experiencing the fastest rates of growth in prison of any cultural group in Australia, with rates doubling between 2009 and 2019 (Australian Bureau of Statistics, 2019).
The Strengthening Connections service spanned two prisons: one maximum-security prison which is the entry point for all women in prison in Victoria, which manages both remanded (that is, not sentenced) and sentenced women, and one minimum-security prison, generally housing women nearing the end of a longer sentence.
The number of women remanded but not sentenced across the two sites increased dramatically in the five years prior to June 2019, from 20% to 47% of all women prisoners on remand. This contributed to a 42% growth in the female prison population over the same period. Figures from 2018–19 showed that following a period of remand, most women were released on bail, and 54% of women released spent less than one month in prison. The Strengthening Connections service was intentionally developed to be applicable to the short timeframe within which women can typically access services while in prison.
Development and Refinement of the Strengthening Connections Service Model
The broad requirements for the model of care were defined a priori by the funder, Corrections Victoria, according to the following criteria. The service needed to:
Be flexible and responsive to women prisoners and their families’ needs.
Be accessible to all remanded and sentenced women.
Be supported by a whole-of-family, evidence-based approach.
Provide throughcare referrals to community agencies for women and their families during and after custody.
Be integrated in existing prison service pathways that support family engagement.
To refine the design of the service and resources to be used in service delivery, we conducted two main processes prior to rollout of the service pilot: a) evidence enrichment supported by our research team and b) consultancy with and between family therapists, researchers, and key stakeholders, including Corrections Victoria. Both processes, described below, informed the refinement of the service model and its application, and the development of an embedded process evaluation framework.
Evidence Enrichment and Theory of Change
At the beginning of the project period, we sought to ground our service model in the current evidence base. To this end, we performed a systematic review of the literature on relational factors relevant to recidivism in women. Findings were integrated into the Strengthening Connections service model and translated into a suite of plain English resources prior to commencement of service delivery. The methodology of the evidence review is not the focus of the current article, but a summary is presented below.
We searched the following databases in April–June 2020: PsycINFO; CINAHL Complete; Medline Complete; Embase; Criminology and Criminal Justice; Criminal Justice Abstracts with Full Text; Criminal Justice Database; CINCH - Australian Criminology Database; Proquest Dissertations & Theses; and Google Scholar. The search generated a total of 2628 articles, of which 128 were eligible for full-text review. Sixty-five of these articles were then eligible for data extraction. The criteria for inclusion in the review were: (i) the paper reported on a sample of females aged 18 years or older; and (ii) participants in the study had been charged with a criminal offence and had either been (a) convicted and imprisoned or (b) held on remand. The criteria for exclusion were: (i) the paper reported on sample of males or other gender, aged <18 years of age; and (ii) participants in the study had not been imprisoned or held on remand.
The key exposure of interest was women’s involvement with the criminal justice system which was reviewed in relation to risk factors for recidivism. Of interest to this project were relational risk factors. Measures of effect included any reported quantitative associations between recidivism and indicators of relational risk. The review considered any/all lengths of time between release and recidivism, any/all incarceration and re-incarceration time periods, any/all types of incarceration (sentenced or remanded in custody) and both rates and incidence of recidivism.
Our review of the literature confirmed support for relational needs as the most impactful intervention for recidivism risk reduction for women, and therefore the theory of change underpinning our service model. The key relational factors implicated in women’s recidivism include both static (i.e., historical and relatively unchangeable) and dynamic (i.e., more changeable) factors. The more static of these factors are related to family of origin experiences and prior victimization (Dowden & Andrews, 1999) – though relationally focused intervention may have a positive impact where vulnerabilities arising from these historical experiences are concerned – and the more dynamic of these factors include current family support; characteristics of intimate partner relationships; parenting concerns for those who are mothers; and quality of peer relationships (Dowden & Andrews, 1999). The key relational risk factors identified via our evidence review are those that have been summarized in the Introduction section of this article.
Our distillation of findings from the review resulted in the identification of six key factors that the evidence base shows to be the most important for helping women stay safely out of prison. Translated for the women in our program resources, these themes were:
Strengthen safe relationships with people who support you;
Disconnect from unsafe relationships;
Care for your own emotional health;
Care for others;
Keep growing as a parent; and,
Set goals for the life you want.
The findings of this review were subsequently translated across all elements of the Strengthening Connections service, from psycho-educational material provided to all women in group sessions through to the therapeutic focus within family sessions.
Clinical and Stakeholder Consultancy
Prior to commencement of service delivery, consultations with and between family therapists, researchers, and key stakeholders in the custodial setting also informed the development of the service model and its planned application. This period of consultancy spanned February to June 2020, prior to the pilot commencing in July 2020, and took the form of site visits by the project team to the prisons; group discussions within the project team; focus groups hosted by the project team with women in prison about their lived experiences of the prison environment and their needs for a culturally safe, strengths-based, trauma-informed and gender-specific treatment model; and meetings between the project team and the funder about the needs of women prisoners at each of the two prisons and about considerations relevant to delivery of a new program within these service systems.
Important considerations arising from these consults pertained to the need for this new program to offer a distinct value-add alongside the offerings of existing mental health and support services within the prisons, the need for adequate preparation in terms of the safety and security needs of both prisoners and staff, and the need for a strengths-based approach such that the service model would enhance personal fulfilment and sense of meaning for the women participating in the program (Ward & McDonald, 2022).
Structure of the Service Model
Based on the findings and outcomes of the processes described above, we piloted a stepped-care family therapy service that comprised three levels of service delivery, including: Step 1) a group-level therapeutic and education session, Step 2) application of single-session family therapy approaches in two to three sessions to support women’s relational health one-on-one with a family therapist, and Step 3) application of systemic family therapy approaches to support women in therapy with their family or allies, across two to six sessions. This three-tiered service model is visualized in Figure 1 and described further below. The model was refined over time and commenced in its final form in July 2022.
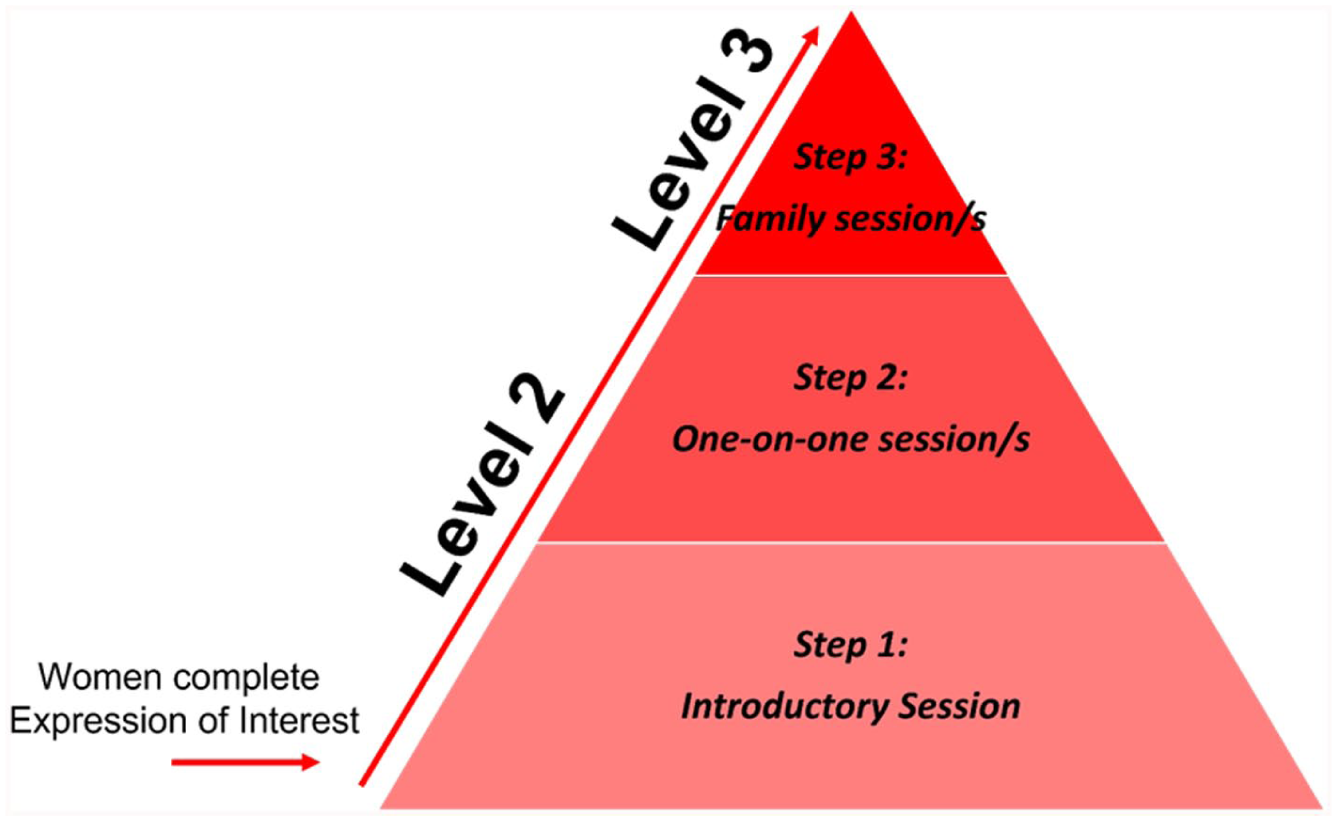
Strengthening Connections stepped care model.
Step 1: Small Group Introductory Session
The group session was conducted in-person by a family therapist and a First Nations cultural consultant to safely engage and support First Nations women when they attended. Up to two women per therapist (and up to two therapists per session) attended an introductory session in-person. We trialed multiple forms of group delivery during the pilot. This included all ‘live’ delivery, with separate First Nations and non-First Nations groups, and we also experimented with online (Zoom) delivery with Family Engagement Workers attending in-person. The decision was subsequently made to adopt the First Nations content for all attendees, and use content pre-recorded by a First Nations worker which could be supported by a non-First Nations worker at the group in-person.
We then settled on a unified set of images and content to translate the evidence review findings into both words and images. This was presented by a First Nations family therapist in a pre-recorded 20-minute video. The short video was shown by the therapist/s running the small group discussion, pausing as needed to facilitate conversation with the attending women. This was followed by the opportunity for women to map their own relational strengths and goals, in terms of the six themes outlined above. Two formats - written and drawn - were made available to women for this exercise, including a ‘family map’ and ‘tree of life’ mapping exercise.
Participation in research for our embedded process evaluation was discussed early in the group. Women were given the opportunity to consent to adding the data from their relational maps, de-identified, for evaluation purposes. The opportunity to action their goals through individual and family therapy sessions was then discussed. Interested women were invited to participate in a 20-minute one-on-one intake component after the group session, to assess eligibility and readiness to participate in Step 2: one-on-one session/s.
Step 2: One-on-One Session/s
This step involved continued in-person session/s with the same therapist the client met at the group introductory session. Step 2 included two to three sessions, where independent therapeutic work and joint scoping of family work (Step 3) occurred. Crucially, the strengths and challenges in the woman’s key relationships were identified. If the woman did not wish to progress to Step 3, then strategies to empower her to strengthen her supportive and safe relationships were discussed. Where appropriate, strategies for disconnecting from unsafe relationships were also considered. If the woman wished to advance to Step 3, an appropriate family member or ally (or allies) with whom to commence Step 3 work was identified. This required considerable clinical sensitivity. For example, some women expressed a strong desire to improve their connection with an abusive or unsafe partner or sought increased contact with their children where Child Protective Services had imposed limitations. In such instances, therapists supported the woman to realign with the program’s objectives about relational healing, which emphasize the importance of strengthening connections with individuals who were able to provide support for a safe transition out of prison. Once an appropriate family member or ally had been identified, a separate session between the therapist and the family member or ally was held. This ensured that the family member or ally had knowledge of the program’s purpose and had a chance to ask questions and express their willingness and ability to participate. Given the potential for longstanding relational difficulties, disappointments and/or mistrust within these relationships, this phase of the process involved considerable time and skill to navigate well.
Step 3: Family Session/s
If elected and appropriate after initial scoping sessions, two to six sessions with the woman and her family member/s or ally/ies were then held, including pre-session meetings with all attendees. All family work was conducted with videoconferencing software to support greater uptake, and to ensure family members could attend from any geographic location. Co-therapy was provided at this stage by family therapists where possible.
Core Features of the Strengthening Connections Service and Guiding Service Principles
While certain features of the service model were refined over the pilot, various core elements remained in place as central to the guiding service principles. These include 1. Foundational use of the family therapy model of ‘Single Session Thinking’ approaches (Hoyt et al., 2021) to make the most of the available individual and family therapy encounters; 2. Cultural safety; 3. Trauma-informed approaches; and 4. Delivery within a stepped care framework. Each are described in further detail below.
Single Session Thinking
As the contact Strengthening Connections therapists have with women is brief, the application of ‘Single Session Thinking’ was foundational to the evolving service approach. Single Session Thinking is responsive to the following three findings (Hoyt et al., 2021): i) The most common number of contacts that clients have with a service is one. That is, no matter the diagnosis, severity, or complexity of their presenting issue, in a large proportion of cases a client will only ever attend one session; ii) Most clients who attend only one session report the single session was adequate given their current circumstance; and iii) It is not often possible to predict who will attend only one session and who may attend more.
As such, the core principle of Single Session Thinking is to treat every clinical encounter as though it may be the last, while leaving room for further sessions should they occur. This thinking leads to the following core foundations of service delivery (Hoyt et al., 2021): making the most of every encounter; working from the client’s agenda, not the professional’s; being timely, respectful, transparent, and collaborative; and giving clients the option for future support, if needed. In the prison system, given the limited contact therapists had with women, and for some women, the chance they could be released from prison with little to no notice, these principles became fundamental to the design of our service, with Single Session principles underpinning every level of service delivery.
Cultural Safety
In the planning and pilot periods, First Nations therapists on the project team consulted and worked closely with existing staff supporting First Nations women in prison. These workers have a close relationship with and are trusted by the women, and their endorsement of Strengthening Connections was key to engaging First Nations women.
Following extensive piloting of separate mainstream and First Nations Step 1 group programs, the decision was made to merge the content of the two groups to be inclusive and culturally safe for all women. This process was led by a First Nations therapist, ensuring elements of First Nations cultural safety were incorporated into the final group content. Our fundamental principle became: What is safe for First Nations women is safe for all women.
A First Nations Cultural Advisor was also employed to work alongside the Strengthening Connections therapists in person at both sites, to ensure the cultural safety needs of First Nations women were identified, acknowledged and supported fully during all stages of program engagement. The Cultural Advisor assisted with Step 1 sessions whether First Nations women were present or not. The advisor was also present for Step 2 and 3 sessions with First Nations women to provide cultural support for both the woman, her family members and the Strengthening Connections therapist. As indicated during the therapeutic process, the Cultural Advisor also met individually with women and offered all Strengthening Connections therapists consultation about First Nations culturally relevant issues. Additionally, the Cultural Advisor supported broader engagement by First Nations women through connections with other First Nations services within and external to the prisons.
There were significant opportunities via the Strengthening Connections program for the First Nations cultural advisor to provide general information to First Nations participants, prison staff and other therapists about the suite of First Nations service offerings available to clients and their families, particularly with regards to social, cultural and justice specific initiatives which could be sources for additional post-release assistance.
Notably, in-person service delivery brought about some difficulties for First Nations workers on the Strengthening Connections team. With the trauma of personal connections and ongoing systems-wide difficulties associated with deaths in custody, cultural safety was sorely challenged for First Nations workers. As a result, some workers experienced significant discomfort with delivering in-person services. Through collaborative consultation with Corrections Victoria, additional First Nations workers were recruited, and flexibility in delivery mode was afforded to ensure First Nations workers felt safe and supported.
Within the prisons in the state of Victoria, Vietnamese women are also largely overrepresented, and for many, English is a second language. A Vietnamese Cultural Consultant joined the Strengthening Connections team to provide cultural and translational support to Vietnamese women at both sites. All Step 1 materials were translated, with necessary cultural adaptations made in the process, to ensure Vietnamese women could safely attend Step 1 sessions. If they chose to, our Vietnamese Strengthening Connections therapist worked with them through Steps 2 and 3. In addition, cultural consultation was offered to all Strengthening Connections therapists who were working with Vietnamese women. As appropriate, prison-based and external Vietnamese cultural advisors were consulted and attended sessions to support culturally safe connection for women and their family members.
Trauma-Informed Approach
Through its evolution, the service maintained a trauma-informed relational frame. Trauma-transformative care and relational family practice was established throughout the stepped care model using the following trauma-informed principles: Safety, Trust, Choice, Collaboration, and Empowerment (Fallot & Harris, 2009). As relational trauma can only be healed in the context of relationships that are the opposite of traumatizing (Elliott et al., 2005), the work of the therapists involved creating an environment of safety, so women felt able to tell and make sense of their story and its relational impact. The therapist would collaborate with the women to work through the layers of trauma, while allowing women to have choice over what was discussed, the therapeutic process and who would be involved in the sessions. This allowed women to reclaim a sense of self and to feel empowered to start to heal the relational bonds with their family. Consistency throughout the process was important too (Atkinson, 2002), ensuring continuity of therapy from Step 1 to throughcare.
The trauma-informed approach appreciates the high rates of trauma experienced by women in the custodial context and recognizes the need to work within service scope – that is, for therapists to be able to hear the women’s story, which most often is traumatic, and be able to hear many such stories while maintaining empathy and curiosity and at the same time remaining separate from the trauma story without losing optimism and hope (Figley, 1995).
Continued attention to the possibility for secondary traumatic stress and awareness of therapists’ coping strategies are important features of the Strengthening Connections model of care. This means being aware of the ways in which systems are impacted by individual and collective exposure to overwhelming stress, trauma and adversity (Bloom & Farragher, 2010). This was managed through creating culturally safe environments, and adopting collective care practices through peer supervision, clinical supervision and operational meetings where therapists could support each other.
Stepped Care
Of note, the three-tiered stepped care approach remained consistent, with the fundamental principle of provision of ‘something for everyone’ regardless of their circumstances. Step 1 (the group program) was always available to all women in the two prisons and there were never any eligibility restrictions to this part of the program. This enabled all women to start thinking about their relational context, where desired, at the outset. Steps 2 and 3 were consistently available to women nearing release and provided specialized service inputs across the course of the program pilot.
Other key objectives of each level of the stepped service delivery approach that remained consistent were the ongoing value of Step 2 work in offering tailored content to women based on identified need; and the unique offering of Step 3 work in providing a space that women may not have experienced previously, where connections with family were nurtured and considered at a pace that was safe for all. In many cases, Step 3 sessions led to enriching and important family dialogue. Even where this work did not result in an actual family session, the key goal was to provide meaningful and therapeutic conversations about relational experiences and healing at the family level. This was found to be valuable even when family members or allies would not or could not engage with the service, as it afforded women a chance to learn more deeply about their relational histories and an opportunity to be supported to live with the relational realities that had shaped their current circumstances.
Implementation of the Service and Continuous Improvement via Process Evaluation
A six-month development phase in 2020 involved the formation of the Strengthening Connections program; consultation with stakeholders as previously described; the evidence enrichment process via systematic review; and development of ethics submissions to enable research and evaluation. Service delivery of the pilot program commenced in November 2020 and concluded in June 2023, followed by a 12-month service extension.
During the service delivery phase, the Strengthening Connections project team engaged in monthly meetings to discuss operational considerations and fortnightly meetings for clinical case consultation, in addition to regular clinical supervision. Ongoing observations were independently recorded by a researcher who attended this series of operational and clinical consultations, providing a chronicle of the continuously developing service model. Observations were continuously documented and collated each quarter to offer iterative accounts of the evolution of the Strengthening Connections service, for discussion with the funding body. Continued refinement of the model included monitoring the service scope, reflections about various therapeutic modalities and optimization of outcomes for both clients and workers, refinements to operational considerations, the balance of good practice against available resources, attention to possible avenues for throughcare service planning, and reflections on alignment with other programs working in the custodial service space.
As part of our process evaluation, we collated program data across the pilot period to refine the model and its delivery. See Table 1 for an overview of data points collected. Review of these data afforded our team quarterly and annual opportunities to integrate feedback provided by both clients and therapists about the operation of the Strengthening Connections program. Core elements of the process evaluation are discussed below and include assessments of program fidelity, context and constraints, service use and reach, service quality, accessibility of the program, and resource management.
Overview of Data Points Collected for the Strengthening Connections Process Evaluation.
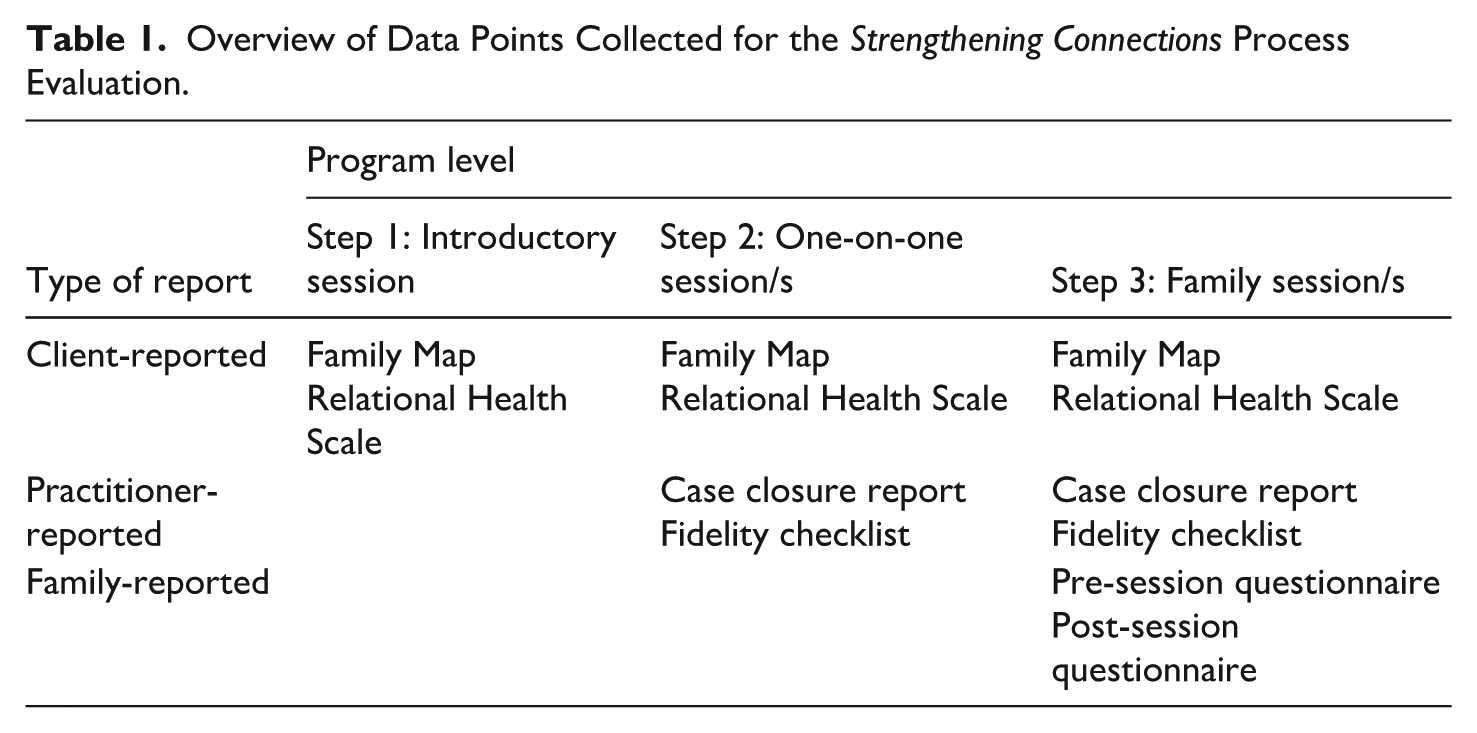
Program Fidelity
At the end of Level 2 and 3 sessions, therapists completed a standardized Session Fidelity Checklist designed to monitor the content of therapist input and to shape ongoing accountability to the aims and scope of the service. This checklist was developed specifically for the project and is particularly focused on the core elements of Single Session Thinking (Hoyt et al., 2021). The checklist contains 20 items pertaining to alignment of each session with the overall goals of the service, elements and themes of each session, and outcomes of each session. For example: To what extent did today’s session cover these aspects? ‘Emphasized the goal of Strengthening Connections to help the women establish a safe, permanent life outside prison’; ‘Follow-up call planned with each member.’ Each item is rated by the therapist on a six-point scale with response options of Fully, Mostly, Moderately, Somewhat, Minimally, Not at All, or Not Applicable.
A total of 341 fidelity checklists were completed across the pilot to May 2023. See Figure 2 for a summary of therapist-reported session fidelity data. Note that all items include a level of missing data likely due to the applicability of the item to the session (notwithstanding the ‘Not Applicable’ response option) and the accuracy of data recording by therapists. Evaluation data indicated a high level of fidelity overall to the central goals of the program. The clinical expertise of the Strengthening Connections therapists was seen as critical to best practice in therapeutic skills and documentation.
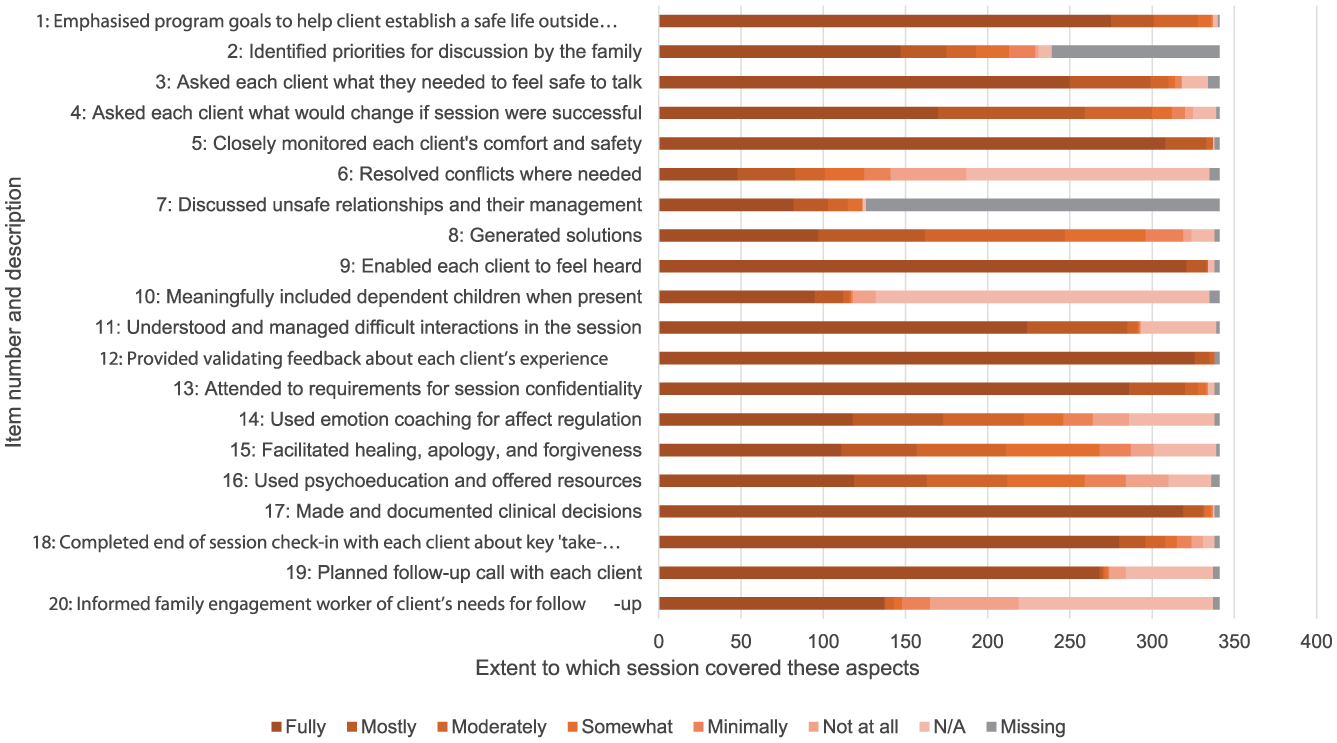
Therapist-reported session fidelity impressions.
Context and Constraints
Across 2020 and 2021, the COVID-19 pandemic presented numerous unexpected challenges that resulted in a variety of scope changes and program adaptations. In addition, unexpected operational complexities in the prison setting (such as room availability and support for appointment scheduling) influenced service delivery decision-making. Custodial environments were not historically designed for a family therapy service, and as such, a lack of devoted infrastructure proved to be an ongoing challenge impacting delivery of the service. Through collaboration with Corrections Victoria, we absorbed and responded to these challenges over the course of the pilot and emerged as an adaptive, flexible service that operated effectively in the context of ongoing challenges. This was a key strength of the service model and is essential when operating in these contexts.
We anticipated many of the operational constraints related to delivery of a service in a women’s prison context, including challenges related to women’s availability for sessions, the availability of relevant technology, and lack of devoted program infrastructure, all of which were particularly challenging for engaging families. The operational constraints of service delivery in the prisons had a continuous and considerable impact on the work being undertaken by Strengthening Connections therapists. While many of these reflect non-modifiable system-level features of the prisons, their impact on service planning and therapeutic work is notable, and this became an important part of our own service adaptation. For example, de-briefing about the building and scheduling constraints of the work became as important as reflecting on the traumatic content shared in session by many women.
Service Use and Reach
Across the pilot from October 2020 to May 2023, 183 Step 1 sessions (one-to-one or small group sessions) were delivered to 188 unique women. During the same period, 295 Step 2 sessions (individual work with a family therapist) and 324 Step 3 sessions (family therapy sessions for the client and her identified family members/allies) were delivered. See Table 2 for an overview of service access data and client information including diversity of referrals and health and wellbeing characteristics.
Service Reach and Client Characteristics.
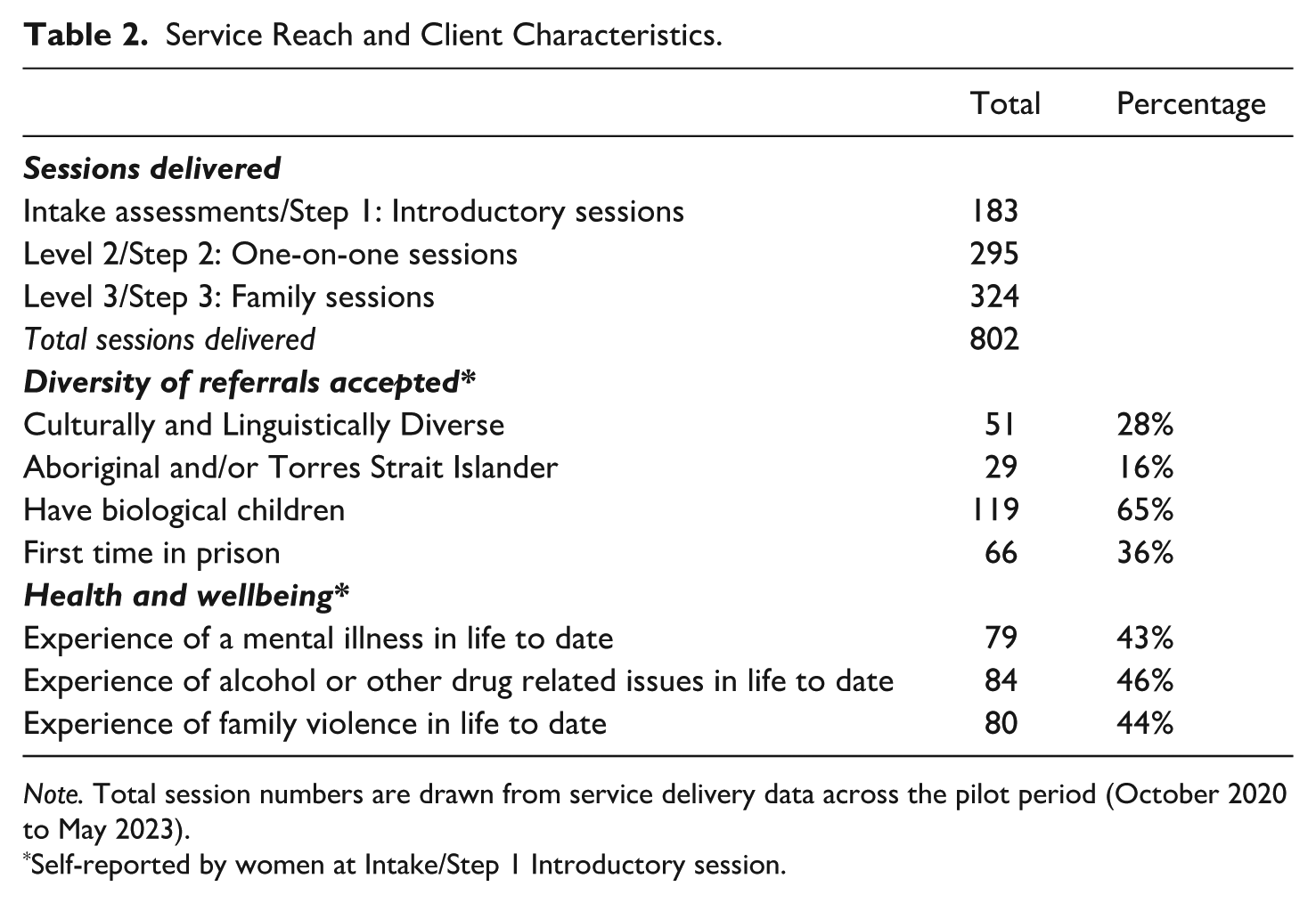
Note. Total session numbers are drawn from service delivery data across the pilot period (October 2020 to May 2023).
Self-reported by women at Intake/Step 1 Introductory session.
The Bouverie Centre also offers a free throughcare service for women and their families who have accessed the Strengthening Connections service while in prison, after their release. This involves family therapy for to up to 10 women and their family per year. Every woman who participates in Strengthening Connections is invited to contact The Bouverie Centre following their release to engage in this follow-up support. During the period October 2020 to May 2023, a total of four clients engaged in this service.
Service Quality
Data from pre-session (service entry) and post-session questionnaires were assessed as indicators of service quality reported by women. Women completed the project-designed 7-item ‘Relational Confidence Scale’ at service entry during the group session. This was then provided to therapists at referral to Level 2 and 3. On this scale, women indicated their levels of confidence in being able to remain connected to safe and positive people; in disconnecting from unsupportive relationships; and in looking after their own emotional health, caring for others, growing as a parent (if applicable), and setting goals for the lives they want after they leave prison. At service entry, most women reported that they already felt ‘mostly’ or ‘very’ confident in their capacity to stay connected to safe and positive people; to care for others; to continue to grow as a parent; to look after their emotional health; and, to set goals for the life they want. Self-reported confidence in the capacity to disconnect from unsupportive relationships was lower, with more than half of responses to this question being either ‘not at all’ (confident), ‘mostly not’ (confident), or mixed.
The post-session questionnaire then included a follow-up of the same scale. While we have insufficient data available for reliably examining pre- and post-therapy change over time by the same respondents on this scale, data offered an encouraging snapshot of client reflections on their relational confidence, post-therapy. Confidence in the capacity to disconnect from unsupportive relationships had improved, and a majority of respondents indicated that they were ‘mostly’ or ‘very’ confident that they would be able to stay safely out of prison after their release (an additional question at follow-up).
We also collected therapist-reported data on the program sessions to understand how therapists felt about each session, in order to refine the supervision structures to be made available to them and to ensure that ongoing work was sustainable. In the second section of the fidelity checklist mentioned earlier, five items enquired about how the therapist felt at the end of the session (e.g., ‘Confident the session made a positive difference’). Overall, data indicated that the team collectively felt competent in their capacity to facilitate complex therapeutic processes with women and were very confident that Strengthening Connections sessions had made a positive difference. See Figure 3 for an overview of therapist perceptions of sessions.
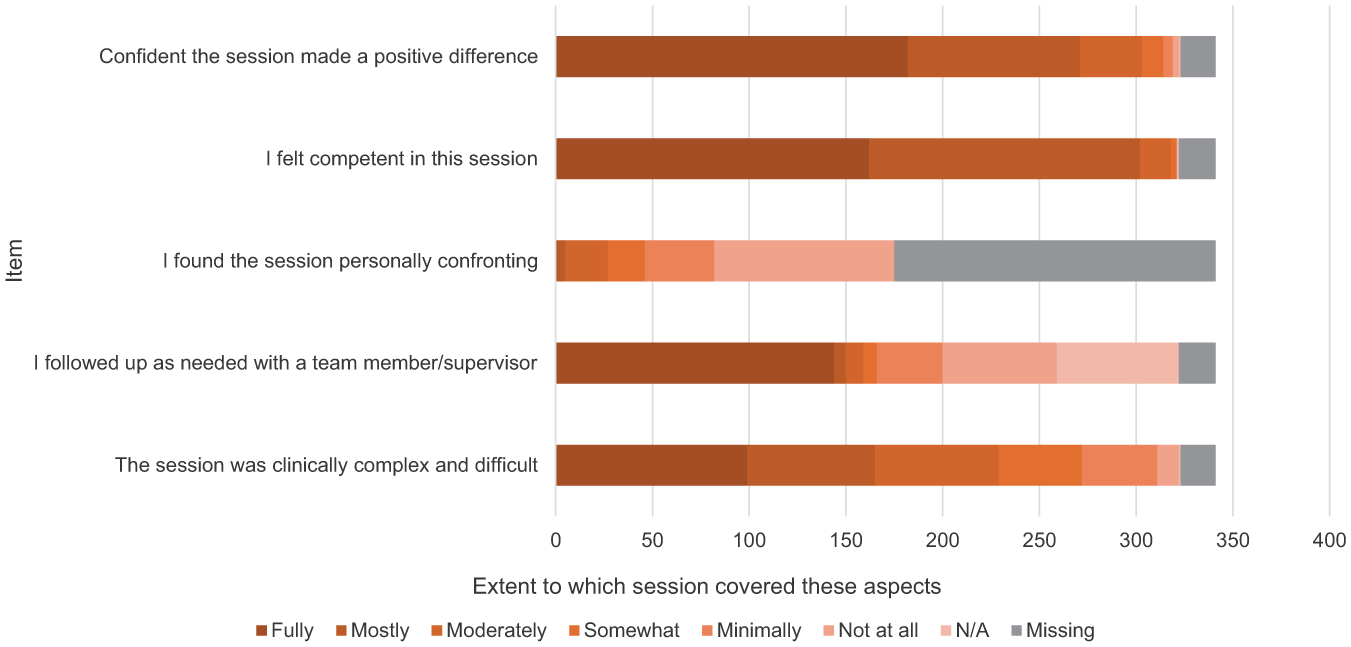
Therapist perceptions of sessions.
Staff training and supervision was also seen as a key indicator of service quality. Strengthening Connections therapists were all trained family therapists who received supportive onboarding and regular clinical supervision across the course of their involvement with the program. Each Strengthening Connections worker received monthly clinical supervision from a senior clinician on the project. This supported their clinical skill development and reflective practice, as well as supporting clinical decision making as needed. Senior clinicians were also available to advise on matters of personal or legal risk as they arose. In addition, monthly group clinical meetings were held with all members of the team to support clinical case consultation. Ultimately, clinical governance and risk management was held by the project director.
Accessibility of the Program
An important feature of the program was its overall accessibility and provision of ‘something for everyone’ regardless of their circumstances. For example, Step 1 (the group program) was always available to all women in the two prisons and there were never any eligibility restrictions to this part of the program. This enabled all women to start thinking about their relational context, where desired. Every attempt was made to make all women aware of the program through advertisement in the prisons.
Accessibility of the program to all cultural and linguistic backgrounds was also a key consideration. As described earlier, after piloting separate mainstream and First Nations group programs, the content of the two groups was merged to be inclusive and culturally safe for all women. A First Nations Cultural Advisor was employed to work alongside the Strengthening Connections therapists to ensure the cultural safety needs of First Nations women were identified, acknowledged and supported fully during all stages of engagement with the program.
Program staff reported that the tone and content of the group sessions felt accessible, warm and creative for women, which allowed them to connect with the work in a non-threatening and non-judgmental way. The visuals, music and breaks embedded in the sessions supported the women’s attentional, sensory and learning needs as many women in these cohorts have difficulty maintaining attention and have varying learning styles.
Resource Management
Delivery of the service occurred in the context of various COVID-19 related challenges. Both the service pilot and its process evaluation were affected. Specifically, service delivery was impacted by prison lockdowns and initially needed to occur via Telehealth/Zoom in place of in-person groups and sessions; when restrictions later eased, the program had not been allocated a dedicated location on-site and this impacted the team’s ability to carry out simple program tasks. Time on-site did not optimize therapists’ time on the project. Entering and exiting a prison environment are lengthy processes, and restrictions on women’s freedom of movement often limited how much could be achieved.
The Strengthening Connections team was heavily reliant on the Family Engagement Service – another service based in the two prisons that supports prisoner contact with their families, whose Family Engagement Workers worked alongside Strengthening Connections clinicians – for administrative support. A dedicated, physical presence of the Strengthening Connections team in the prisons would have helped to address this, but due to the relatively small staff load in our service this was not possible.
Discussion
‘Strengthening Connections’ was an in-prison stepped care family therapy service (2020–2024) for supporting women to strengthen their relationships with family and other close supports, with the overall goal of reducing their risk of recidivism. To the best of our knowledge, this was the first stepped care approach to in-prison delivery of family therapy-based support for improving women’s relational health.
Women in prison have multiple and complex needs that influence the likelihood of their recidivism or safe transition back into their community. The current focus has been on investing in the relational needs that are known to be associated with women’s risk of recidivism, with a focus on service delivery that is therapeutic, trauma-informed, strengths-based and culturally safe. Here we have described the basic architecture and guiding theoretical elements of a tri-level stepped care service for family-centered support of women in prison. The Strengthening Connections service was beneficial for promoting women’s identification of and connection with safe, supportive family members and allies, including in their families of origin and of procreation. The program emphasized relational self-efficacy through supporting women’s confidence in identifying who to seek support from and who to refrain from relying on once they exit prison. Women participating in Strengthening Connections at all program levels improved upon their capacity to attend to their own and others’ emotional wellbeing, including the health and wellbeing of their children for those who were parents.
Women in custodial systems need best practice opportunities to engage in relational therapy to support reflection and healing in ways that will enhance the safety and quality of their relationships after release from prison. Reintegration into the community post-release from prison can be risky and overwhelming, and many women face loss of housing and financial security, with attendant risk of returning to unsafe relationships. While the focus of this service was specifically on relational risk factors, ‘wraparound’ support for women in prison should be delivered with consideration of other criminogenic needs, individual factors such as mental health, and post-release circumstances related to housing and employment. Recidivism risk is influenced by a complex interaction of these factors (Kreis et al., 2014).
Our process evaluation data collated across the course of the service pilot indicated whether program activities were implemented as intended and what accommodations to process were indicated. With continual learning from data from both clients and therapists, we were able to understand and respond to the diversity of needs and experiences of the full profile of women accessing the service. Our learnings from the process evaluation allowed us to offer unique program inputs based on the emerging referral issues and themes arising in therapeutic work, and to set this in context of the broader array of supports currently available to women in prison in Victoria, Australia. Therapist-reported data allowed us to understand and optimize therapists’ experiences of working within Strengthening Connections and shaped our ongoing accountability to the aims and scope of the program based on model fidelity data across the pilot period.
Importantly, the structure and guiding principles of the Strengthening Connections service were designed to suit the needs of a diversity of clients. Cultural safety was a key consideration in all aspects of model development. This included provision for First Nations women to request to work with a First Nations therapist; consultation between First Nations and non-First Nations therapists to adequately support First Nations clients when they did not request a First Nations therapist; appointment of cultural advisors to the program team across stages of development and delivery; and translation of program resources into other languages wherever possible. While these provisions were designed with the Victorian state women’s prisons in mind, the basic principles of cultural safety outlined here are hoped to generalize more broadly to practice with Australian and international cohorts of women in various correctional settings.
There was significant complexity in the presenting clinical issues for women who engaged in this service. Delivery of the stepped care service by specialist family therapists was key to its success. Having experienced therapists who could readily identify and respond to dynamic challenges and retain a sharp focus on working to achieve relational outcomes was key to safe, sustainable, and productive work with clients and their families in this context. Cultures of specialist supervision and support are critical for the ongoing sustainability of such models of care in settings where clinical complexity is high, and the risk of secondary traumatic stress is pressing. While investment by correctional services in this level of clinical input is not always possible in the context of competing fiscal and policy priorities, we reiterate the significant benefit of the therapeutic work to women who participated in the Strengthening Connections service and situate this in context of the broader benefits to their surrounding families and communities when recidivism risk can be meaningfully reduced, especially if adequate throughcare support is available.
Given the transition between prison and community is a time of significant risk to women’s physical, mental and relational health (McLeod et al., 2020), barriers to continuity of care post-release must be addressed in the interests of meaningfully reducing recidivism risk. While women are often able to access a range of supports while in prison, investment in tailored throughcare services is needed to maintain any benefits secured inside (Abbott et al., 2016; Brown & Ross, 2010). This would reduce costs to both healthcare and justice departments and improve the wellbeing of this vulnerable cohort of women. The Strengthening Connections service provided free throughcare (i.e., post-release therapy session/s) for women who were interested and able to attend. While a small number of women accessed this service, barriers to access – including the difficulty of contacting the service in context of the stress- and bureaucracy-heavy transition from prison to the community – should be addressed in future iterations of this or similar services.
Humane and effective support of women in prison involves the provision of culturally safe, therapeutic and evidence-based programs that empower and connect the individual to safe and caring relationships. The overview of the Strengthening Connections service model presented here is hoped to inform program development and capacity building in other women’s prison settings both in Australia and internationally to improve outcomes for women, their families, and the broader communities that support them.
Footnotes
Acknowledgements
Vicki McMaster (Department of Justice and Community Safety) and The Strengthening Connections team (The Bouverie Centre, La Trobe University): Dale Needham, Sandy Jackson, Allie Bailey, Clarisse Slater, Thy Nguyen, Clemency Press, Nu Jayasinghe, Julieanne James, Darleen Christensen, Jessica Krummel, Tessa Petrides, Laura Moate and Leonard Linesbaum.
Ethical Considerations
Ethics approval was provided by The Department of Justice and Community Safety Human Research Ethics Committee (JHREC); project number CF/21/15914.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported with funding from the State Government of Victoria, under the Women’s Justice Diversion and Rehabilitation two-stage strategy.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.