
Abstract
Despite evidence that psychological treatments benefit from pre-treatment intervention, there remains no published research on the value of including a pre-treatment intervention in forensic mental health settings. The present study aimed to address this gap by examining the effects of adding a brief motivational preparatory program (MPP) to standard forensic psychiatric care. The MPP was based on hope theory and motivational interviewing within a cognitive-behavioral therapy approach. MPP participants and a waitlist control group completed a battery of self-report measures of hope and motivation to change, which were compared with respect to risk, demographic, offence history, and outcome variables. There was a significant increase in client motivation for change after completing the MPP. Additionally, those who completed the MPP evidenced modest reductions in aggressive behavior, but significantly increased engagement in subsequent forensic treatment and programming.
Therapeutic intervention is an essential part of risk management and recovery for those involved in the criminal justice system. However, motivation or readiness for change has been shown to be a key element of treatment efficacy and more enduring behavioural change (Lundahl & Burke, 2009; Melnick et al., 2001). In fact, interventions aimed at enhancing motivation contribute uniquely to important treatment outcomes, such as symptom reduction, improved quality of life, and recidivism (Feld et al., 2001; Westra et al., 2009; Marshall et al., 2008). These interventions are often delivered before the treatment/therapy proper, and are described as pre-treatment or preparatory treatment programs. Despite promising initial findings, these programs are limited, and the research evaluating them, even more so. This is particularly true within forensic mental health settings, where individuals are often characterized as difficult to engage in treatment due to complex psychiatric presentations and behavioral comorbidities. The present study evaluated a preparatory treatment program provided to adults within a forensic mental health program in Canada to determine what if any benefits were associated with participation compared to treatment as usual.
The forensic mental health system includes individuals found not criminally responsible on account of mental disorder (NCR-MD) and those determined to be unfit to stand trial. For the most part, these individuals are characterized by psychiatric and/or medical conditions that are implicated in criminal behavior. As in most countries, the Canadian forensic psychiatric system is under the jurisdiction of a quasi-judicial tribunal that regularly reviews and determines the appropriate disposition for an accused. However, the length of stay (LoS) is not determinate; rather, absolute discharge depends on whether or not the individual is deemed to have made sufficient progress so that they no longer present a significant threat of physical or psychological harm to members of the public (Bettridge & Barbaree, 2004), or in the case of unfit accused, now fit to stand trial. As a result, it is not unusual for individuals in the forensic system to be detained or supervised for longer periods of time than individuals in the correctional system, even for similar criminal offenses (Völlm et al., 2017). This comes at a great cost to both personal liberty and hospital resources, particularly if an individual has low motivation to engage in treatment aimed at modifying their risk of harm. Therefore, efforts aimed at improving treatment engagement and rehabilitation program efficacy have the potential to significantly improve individual recovery and risk management, as well as the efficiency of the forensic system.
Improving motivation can be a challenging task, especially among individuals who may resist the recommended interventions, or lack insight into the need for such treatment in the first place. Fortunately, a small, but growing body of literature in forensic psychology suggests that an effective way to enhance treatment engagement and efficacy is with the inclusion of brief preparatory interventions (see Marshall et al., 2008; Moulden & Marshall, 2005; Moulden & Marshall, 2009). Preparatory interventions aim to address potential barriers prior to the actual treatment, including premature attrition, limited or non-engagement, and treatment refusal. By identifying and targeting these issues, clients more rapidly and effectively engage in their subsequent treatment programs (Wechsberg et al., 2007). The approaches to pre-treatment intervention that have achieved the most reliable success are those that focus on client motivation.
Motivation is dynamic in nature and has been shown to be modifiable among justice involved individual by such preparatory programs (Stinson & Clark, 2017). Miller and Rollnick’s (1991) conceptualization of motivation acknowledges the important influence of therapist behavior on client motivation. Their description posits that therapeutic styles successful at enhancing client motivation should also increase treatment participation and reduce client attrition. Motivational Interviewing (MI; Miller & Rollnick, 1991), a therapeutic style originally developed in the field of addictions, has been shown to be particularly helpful for justice involved clients who present with a host of unique barriers to treatment engagement, such as distrust, stigma, and misinformation (Mann et al., 2013; Moulden & Marshall, 2009; see also Howells & Day, 2002). Relatedly, hope theory represents another means of facilitating change through increased motivation and agency, such that it posits treatment is most effective when therapists help clients develop future goals consistent with defined pathways, which they believe they are capable of achieving (Moulden & Marshall, 2005; Snyder, 2000). In one of the few applications to criminal behavior, Martin and Stermac (2010) found a significant negative relationship between hope and recidivism risk. Upon closer inspection, agency was the only aspect of hope to make a significant contribution to the prediction of risk. Despite the authors’ call for incorporating hope-based interventions into forensic rehabilitation, unfortunately little has been published over the past decade.
A corollary of low motivation for change among justice involved clients is that even if individuals initially attend, many therapy programs report high rates of subsequent attrition or drop out (Brunner et al., 2019). This is particularly problematic as research has found that those who can benefit the most from treatment (highest risk offenders) are the least likely to complete it (Brunner et al., 2019; Stinson & Clark, 2017). A meta-analysis of offender treatment found attrition rates of 27.1% amongst federally incarcerated individuals in Canada (Olver et al., 2011). In a different study looking at individuals with violent offending convictions taking part in a re-entry program, 69% of the participants failed to complete the program. The most common reason for program attrition was lack of compliance (Listwan, 2009). Two aspects of treatment compliance related to program attrition are the clients’ level of motivation to change, and whether they effectively engage in treatment (Proulx et al., 2004).
Many of the challenges associated with correctional and forensic rehabilitation can be addressed by pre-treatment intervention programs that target motivation. For example, a treatment review with justice-involved clients found evidence that MI techniques improved retention in treatment, enhanced motivation to change, and reduced re-offending in both incarcerated and community corrections settings (McMurran, 2009).
In their study, Marshall and his colleagues (2008) evaluated the effectiveness of a preparatory program for individuals with sexual offending convictions at the beginning of their federal prison sentence in Canada. The goals of the program were to reduce treatment refusal rates and attrition, and to prepare clients to achieve the goals of the subsequent recommended treatment program. To evaluate the program, they assessed the motivational effects (e.g., hope, self-efficacy, treatment readiness, and stage of change) and system effects (e.g., placement in lower security prison, allocation to lower intensity treatment, earlier release on parole, and reductions in recidivism) amongst program participants. Following completion of the preparatory program, the authors found that program participants were more motivated to complete the full treatment program and had higher rates of hope and self-esteem. Similarly, program participants were assessed by correctional staff (i.e., parole officers) as requiring less intensive treatment and were more likely to be assigned to lower security facilities. Upon follow-up 3 years later, and compared to a matched control group, the recidivism rates were significantly lower for individuals who completed the preparatory program.
In the forensic psychiatry literature, there remains a single example of a preparatory program included in forensic treatment (Renwick et al., 1997). In this now dated study, a small sample of patients with recurring anger and aggression problems participated in a new anger management treatment protocol. One of the components of this treatment protocol was a five-session preparatory phase, which included motivational enhancement. Unfortunately, the researchers decided not to evaluate the effects of the preparatory phase separately, and so conclusions regarding the success or failure of this particular program could not be offered. Despite promising findings for preparatory treatment in general, and with justice involved individuals more broadly, there has been very little clinical uptake within forensic and correctional arenas, and even less effort to evaluate such interventions.
Present Study
To date, there remains little to no published research on the effects of a motivational preparatory program (MPP) in a forensic mental health setting. The present study aims to address this gap in the literature by evaluating a brief MPP that is based on hope theory and motivational interviewing within a cognitive-behavioural therapy approach. The program is designed to help clients in the forensic psychiatric system understand the rationale for and process of change, and prepare to make changes with respect to management of illness and risk. The purpose of the present study is to determine if participation in the MPP improves outcomes among this unique client population. This was achieved using a combination of self-report questionnaires that evaluate various components of treatment readiness as well as systems level data regarding behavioural changes, such as aggression and program participation.
An individual is ready for treatment if they are motivated to change, hopeful about the prospects of treatment, and has the ability to meaningfully engage in and complete the treatment process. The following specific research questions were posed as part of the present study:
Does pre-treatment programming increase motivation to change and hope among individuals in the forensic mental health system compared to (i) before treatment and (ii) a matched comparison group of patients who did not participate in the treatment program?
Are there differences on self-, and team-evaluated risk as a function of participation in pre-treatment programming?
Does pre-treatment programming improve behavioral outcomes, including (i) aggression, and (ii) participation in subsequent rehabilitation?
It was hypothesized that compared to a matched waitlist control group, MPP participants would demonstrate increased motivation to change and hope following completion of the program. Secondly, MPP participants were expected to display positive behavioural changes measured by post-MPP incidents of inpatient aggression and subsequent enrollment in rehabilitative programs. Self-assessed risk and professional risk estimates were also assessed. The present study serves as an important first investigation into the potential benefits of pre-treatment interventions in forensic mental health settings.
Methods
Participants
A total of 60 adult males and females participated in this study. All participants were recruited from a forensic psychiatry program in a large Canadian city, and at the time of the study were under the jurisdiction of the Ontario Review Board 1 (ORB) having been found NCRMD (Criminal Code of Canada, Section 16).
Thirty individuals participated in the MPP, but six were removed due to incomplete follow-up data. The final sample included 22 males (92%) and 2 females (8%), with 17 from inpatient, and 7 from outpatient, units at the hospital. At the time of enrollment into the study participants were on average 35.93 years old (SD = 8.93) and the average LoS in the forensic system was 49.7 months (SD = 26.77). Participants were diagnosed with a range of DSM-5 mental disorders (American Psychiatric Association, 2013), including schizophrenia (50%), schizoaffective disorder (25%), bipolar disorder (8%), delusional disorder (8%), and psychosis not otherwise specified (8%). Many participants had a comorbid substance use-related disorder (71%). The majority of offenses for which they were found NCR were violent (63%), and participants had a mean of 15.2 prior convictions and 4.71 previous psychiatric hospital admissions.
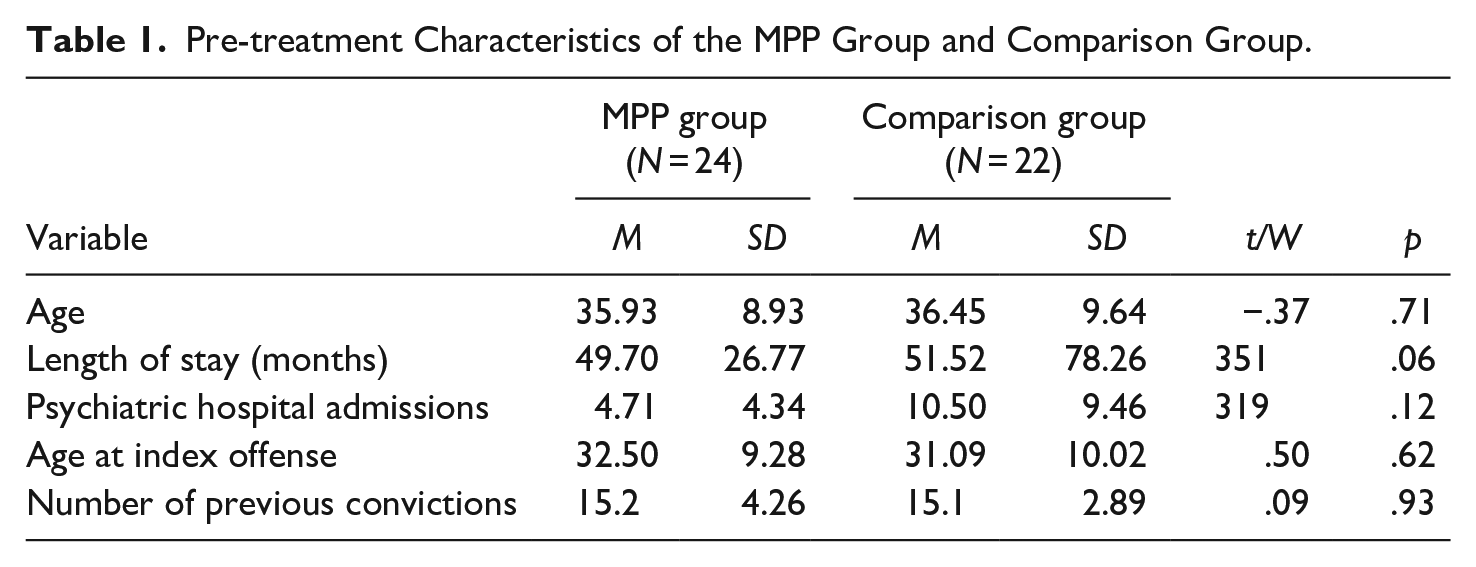
Thirty individuals comprised the matched waitlist control group, but eight were removed due to incomplete follow-up data. The final sample included 19 males (86%) and 3 females (14%) from inpatient units at the same hospital. Participants were on average 36.45 years old (SD = 9.64), and the average LoS in the forensic system was 51.52 months. Comparison group participants were diagnosed with a range of DSM-5 mental disorders (American Psychiatric Association, 2013), including schizophrenia (70%), schizoaffective disorder (22%), and substance induced psychotic disorders (9%), with similarly high rates of comorbid substance use related disorders (77%). The vast majority of index offenses were violent (86%), and participants had a mean of 15.1 prior convictions, and 10.5 previous psychiatric hospital admissions (Table 1).
Pre-treatment Characteristics of the MPP Group and Comparison Group.
Measures
Adult Dispositional Hope Scale (ADHS)
The ADHS is a 12-item measure of respondents’ trait hope (Snyder et al., 1991). It has two subscales that are based on Snyder’s model of hope: (1) agency (goal directed energy) and pathways (planning to accomplish goals). For each question respondents use a four-point Likert scale to rate the degree to which each statement describes them. A higher score indicates greater individual disposition to be hopeful about the future. The ADHS has displayed good internal reliability (alphas ranging from .75 to .88) and good test-retest reliability (r = .85 for 3 weeks to r = .82 for 10 weeks) across a wide range of populations (Gana et al., 2013; Snyder, 2002; Snyder et al., 1991). In the current study, the internal reliability was consistent with these findings (Chronbach’s α = .82).
Adult State Hope Scale (ASHS)
The ASHS is a six-item measure of the respondents’ current goal directed thinking (Snyder et al., 1996). The ASHS is similar to the ADHS, with the major difference being that the former focuses on an individuals’ present quality of agentic thinking, pathways identification, and goal definition. Depending on the time interval, the test-retest reliability ranges from r = .48 to .93 across a 4-week period. Internal reliability of the ASHS in the current study was also good (Chronbach’s α = .85).
University of Rhode Island Change Assessment (URICA)
The URICA is a 32-item self-report questionnaire designed to measure treatment readiness (McConnaughy et al., 1983). It is based on the transtheoretical model of change (DiClemente & Prochaska, 1998) and there are eight items for each of the model’s four stages of change: precontemplation, contemplation, action, and maintenance (McConnaughy et al., 1983). In completing the questionnaire respondents use a five-point Likert scale to indicate the extent to which they currently agree or disagree with each statement. A total score is compiled for each stage, and the stage with the highest score represents the respondent’s current position regarding their perceived need for change. Multiple studies have displayed good internal reliability of the overall URICA as well as each of the subscales (Dozois et al., 2004). This was replicated in the current study where the overall internal reliability was good (Chronbach’s α = .89). In addition, each of the subscales demonstrates acceptable convergent and divergent validity (Dozois et al., 2004). The URICA significantly predicts treatment retention (Brogan et al., 1999; McConnaughy et al., 1983) generally, but more importantly all of these psychometric properties also hold true in incarcerated samples (El-Bassel et al., 1998; McMurran et al., 2006).
Self Appraisal Questionnaire (SAQ)
The SAQ is a 72-item multi-dimensional questionnaire designed to predict violent and non-violent offender recidivism in forensic and correctional populations (Loza, 2005). It has both a theoretical and empirical basis, covering multiple areas related to the measurement of criminogenic factors (Loza, 2018). The items require a true-false based response, and the measure is comprised of eight subscales: criminal tendencies, antisocial personality, conduct problems, criminal history, alcohol and drug use, antisocial associates, anger, and validity. The SAQ displays excellent internal reliability (alpha = .92; a finding confirmed in the current study [Chronbach’s α = .97]), and good test-retest reliability (r = .83) in numerous research studies with incarcerated populations (Andreu-Rodríguez et al., 2016; Loza, 2005; Loza et al., 2000; Prinsloo & Hesselink, 2011). Scores on the SAQ have correlated with other measures of similar constructs, including recidivism and criminal history (Loza, 2018). Critically, there is a large body of evidence supporting the predictive validity of this measure (Loza, 2018; Loza & Green, 2003; Loza et al., 2004, 2005). In 2-year (Loza & Loza-Fanous, 2001), 5-year (Loza et al., 2003), and 9-year (Loza et al., 2007) follow up studies, SAQ scores significantly predicted various post-release outcomes.
Hamilton Anatomy of Risk Management—Forensic Version (HARM-FV)
The HARM-FV is a structured professional judgement instrument developed for use by trained mental health clinicians in inpatient forensic psychiatric settings (Chaimowitz & Mamak, 2011). Both historical risk factors (major mental illness, substance use, personality disorder, cognitive deficits, historical violence offence, historical non-violence offence) and dynamic risk factors (rule adherence, insight, psychotic symptoms, mood disorder, impulse control, social support, substance abuse, medication non-adherence, antisocial attitude, stress) are considered in the HARM-FV which then form the basis for a consensus opinion about a patient’s risk for aggression. An additional feature of the HARM-FV is the embedded risk management component, in which the clinical team formulates treatment and risk mitigating plans to address identified risk factors. Although the HARM-FV is relatively new, psychometric evaluations have suggested that it is both valid and reliable. It has demonstrated excellent inter-rater reliability (Healey et al., 2020), and promising predictive and concurrent validity (Cook et al., 2016; Healey et al., 2020). In one research study ratings on the HARM-FV were strongly correlated with ratings on the Historical, Clinical, Risk Management–20 (HCR-20; Douglas et al., 2013)—a well-established violence risk assessment tool (Cook et al., 2016). Embedded within the HARM-FV is the Aggressive Incidents Scale (AIS), which provides a standardized method for recording aggressive behavior. Incidents are recorded on a daily basis using a scale from one to nine, with higher scores reflecting higher severity incidents. The AIS has demonstrated strong concurrent validity with the Modified Overt Aggression Scale (MOAS; Sorgi et al., 1991), a widely used tool for documenting violent behaviors. The internal reliability of this instrument in the current study is considered good (Chronbach’s α = .80).
Procedure
All patients detained at the forensic psychiatry program at the time of data collection were invited to participate in the present study if they were able to provide consent, English speaking, and eligible to participate in the MPP. They were informed that study participation is voluntary and that choosing not to participate would not affect their ongoing treatment in any way. Individuals that expressed interest to participate in the study provided written informed consent for the study to access their medical record to collect additional participant information. For a period of 2 months individuals in the MPP group (N = 30) attended 2 weekly group therapy sessions. The comparison group (N = 30) did not participate in the MPP, but they still engaged in their usual rehabilitative activities, as did the treatment group. One week before this 2-month period, and within 1 week upon program completion, all individuals completed a battery of self-report psychometric assessments, including the SAQ, the URICA, the ADHS, and the ASHS. The order in which the tests were completed was counterbalanced. For each data collection session, comparison group participants were compensated with a $5 gift-card for the café located within the hospital. MPP group participants received compensation in the form of refreshments provided during each MPP group therapy session. This study was approved by a local research ethics board (HiREB #1138).
Motivational Preparatory Program
The MPP includes twice weekly 1.5-hour group therapy sessions for 8 weeks. Patients are encouraged to participate in the group regardless of whether or not they are ready to make changes. The program was adapted, delivered and/or supervised by the first author based on the Rockwood preparatory program (Marshall et al., 2008). The content of the program involved psychoeducation about the forensic psychiatry system, psychoeducation about behavioural change, psychoeducation about risk assessment and risk management, self-assessment of risk and factors related to risk and recovery, change readiness and values, and discussions about hope, including agency, goal setting, plan execution, evaluation, and modification. In addition, homework was assigned in the form of both written and non-written exercises. Active participation during group treatment allowed clients to become more aware of problem areas in their lives, and if ready, begin making positive life changes with respect to their recovery and risk management.
Data Treatment and Analysis Plan
Analyses were conducted using R statistical software (R Core Team, 2020) and SPSS (IBM, 2019). The data were checked, and appropriate parametric or non-parametric tests were performed. When a participant was missing data on a particular measure a pairwise deletion process was followed.
Results
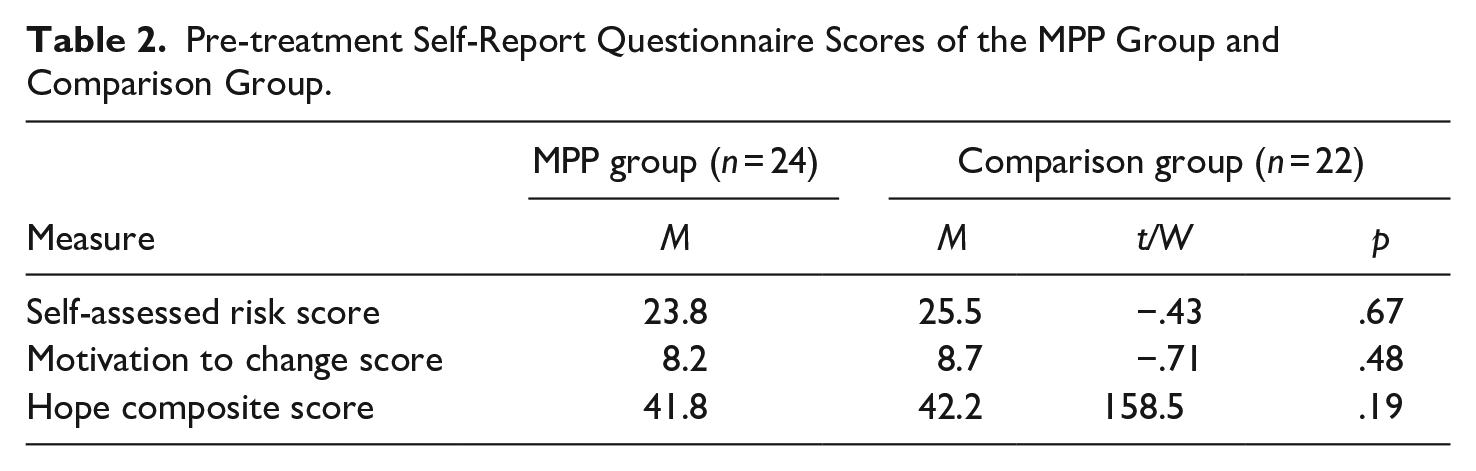
Members of the MPP and comparison groups did not differ statistically in terms of age, length of stay, number of previous hospitalizations, number of convictions, education, and age at index offense. Nor did they differ with respect to pre-treatment self-assessed risk, professional risk ratings, motivation to change continuous scores, and hope scores. The results of these analyses are presented in Tables 1 and 2.
Pre-treatment Self-Report Questionnaire Scores of the MPP Group and Comparison Group.
In order to answer the first research question regarding change as a function of MPP participation, state and trait hope scores were compared, as were URICA scores within the MPP group. While no differences were observed with respect to either dimension of hope, a significant shift in stage of change occurred over time, such that most participants (n = 12) fell in the contemplation stage at pre-treatment, but then moved to the action stage at post-treatment. A Mann–Whitney test confirmed that the difference in distribution from pre- to post-MPP was highly significant (W = 335, p = .007). Importantly, this observation was not mirrored in the comparison group who evidence no such motivational shift confirmed by a Mann–Whitney test of highest stage-of-change scores (Table 3). Despite this significant shift in the distribution of participants’ highest URICA stage-of-change, there was no significant difference between pre- and post-program URICA total continuous scores. This may be because both participants’ overall stage-of-change and URICA total scores are less sensitive at detecting change than participants’ highest stage-of-change.
Changes in Highest URICA Stage-of-Change.
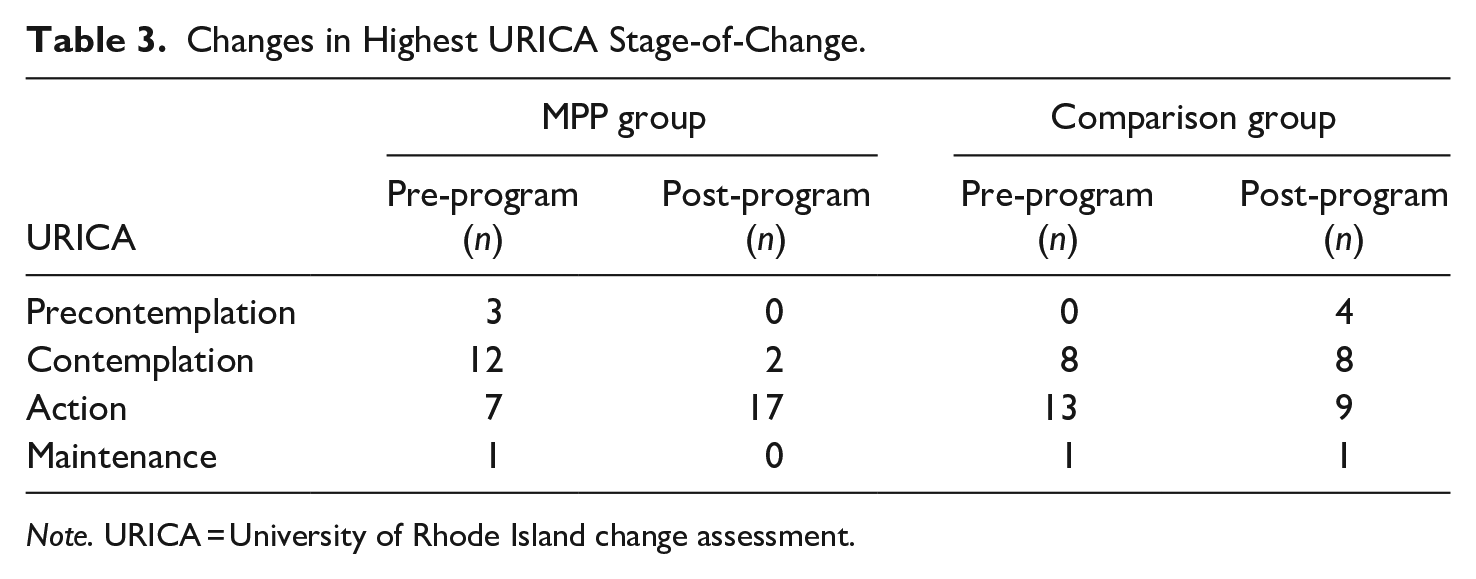
Note. URICA = University of Rhode Island change assessment.
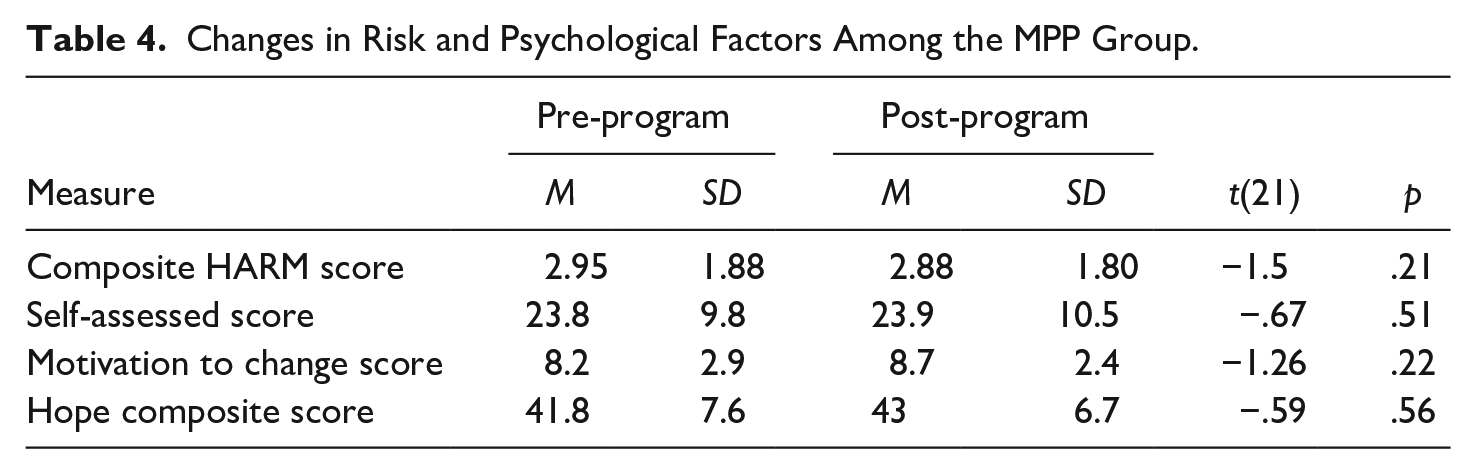
The second research question regarding changes associated with risk for violence did not reveal any effect for the MPP, both in terms of self-assessed risk and risk estimates based on clinical team consensus (Table 4).
Changes in Risk and Psychological Factors Among the MPP Group.
Finally, and perhaps most clinically relevant were the behavioral outcomes examined as a function of MPP participation. First, the aggressive incidents as measured by recorded AIS scores, revealed a promising, albeit insignificant, trend toward lower rates of aggression among the treated group (p = .10). However, consistent with our hypothesis, was a demonstrable increase in treatment participation following completion of the MPP. The number of rehabilitative treatment programs the participant was enrolled in or waiting to start at pre-treatment was compared 1 month after completion of the MPP treatment. While the comparison group showed virtually no change (M = .27, SD = .40), the treatment group’s engagement doubled (M = 2.21, SD = .15), t = −9.84 (45), p < .001.
Discussion
The purpose of the present study was to determine whether a motivational preparatory program improved treatment motivation and readiness in a sample of individuals in the forensic mental health system. To evaluate the utility of the MPP, factors related to treatment readiness were examined, including stages of change, and state and trait hope. We hypothesized that MPP participants would have improvements in motivation as measured by stages of change and hope following completion of the program. Consistent with this hypothesis, MPP participants’ motivation or readiness for change improved as reflected by both their within and between subject change compared to a matched waitlist control group. This increase in motivation was demonstrated by a significant shift in the distribution of participants’ highest stage-of-change on the URICA. However, contrary to our hypothesis and previous research on the role of hope in treatment motivation and preparatory programs (Marshall et al., 2008), MPP participation was not associated with significant changes in hope scores. These results indicate that those who participated in the MPP achieved some of the goals of the program, and these changes are likely attributable to the preparatory intervention.
Although psychometrically measured change is helpful in the evaluation of novel interventions, alone it is insufficient. Increasingly, behavioural outcomes are relied upon as more robust indicators of internalized and sustained change. Not only do these modes of evaluation have ecological validity, but they are likely a truer indication of impact given that they are free from the bias inherent in post-treatment evaluation. The patient wants to believe that they have improved as a function of the time and energy they have invested and so may be inclined, subconsciously to over endorse change and benefit. At a conscious level, particularly for justice involved individuals, they are aware that the extent to which they are evaluated as benefiting from rehabilitative programs often directly influences both the clinical and legal decision makers regarding liberties. For these reasons, outcome measures, such as aggressive incidents and subsequent program enrolment were included in the current study to provide an indicator of treatment relevant behavioral change.
In this domain, important trends and changes were observed on both indices. First, although modest, MPP participants demonstrated a trend toward lower levels of aggression 1-month post treatment completion. It is interesting that even though preparatory programs are not designed to directly impact psychopathology, there appears to be evidence that pre-treatment programming may initiate and/or potentiate such change. In both studies of preparatory interventions in correctional settings, lower recidivism was found among the individuals who had completed the preparatory program, even though the preparatory program did not directly address risk factors associated with sexual or violent reoffending (Marshall et al., 2008; McMurran, 2009). An inherent aspect of a motivational interviewing approach as defined by Miller and Rollnick is elicitation of behavior change, comprised of problem awareness, behavioral alternatives, and resolution of ambivalence. Perhaps the motivational interviewing approach to discussions of recovery and risk, and risk management resulted in increased awareness of the behavior, and early efforts to begin to modify aggression.
A second important indicator of change was the MPP participants’ higher rate of subsequent enrolment in additional rehabilitation, such as psychotherapy, vocational programs, and specialized treatments for addictions, as compared to the matched control group. The main objectives of preparatory treatment are to increase internalized motivation to change and reduce barriers to enrolment and engagement in the subsequent treatment of the problem. For individuals in the forensic system, treatment includes a host of psychiatric and criminogenic targets which must be addressed in order to reduce and manage risk of harm. This finding is consistent with previous work in corrections, which demonstrated that participation in pretreatment programming increased motivation to positively engage in subsequent targeted criminogenic rehabilitation programs (Marshall et al., 2008, McMurran, 2009).
Strengths, Limitations and Future Directions
Although the findings are promising, they are modest and must be interpreted with the following strengths and limitations in mind. The inclusion of a matched comparison group was a notable strength of our study as it allowed us to better estimate the true effects of the MPP. However, one could argue that simply engaging in a structured therapeutic activity with skilled therapists represented the mechanism underlying the changes observed. Notwithstanding this alternative hypothesis, and consistent with prior research examining pre-treatment interventions, only individuals that participated in the preparatory program showed the expected effects, which were themselves specifically hypothesized based on motivational theories of change, rather than global, or solely self-reported, indicators of improvement. Given the small sample size, any treatment attributable differences between the two groups would have needed to be large to reach statistical significance. However, larges sample sizes are a challenge for clinical recruitment, particularly in forensic settings. Given the sampling limitation, the findings should be interpreted cautiously and be subjected to replication, ideally with a larger sample size.
Another limitation relates to the psychological constructs measured. Although measures of hope and motivation to change provide useful information, there are additional mechanisms of change that may prove to better explain the preparatory treatment effect. The inclusion of measures that assess the barriers addressed, such as resistance, mistrust and stigma, as well as those that canvas participant’s own treatment engagement and insight (see Drieschner & Boomsma, 2008) may provide important information about other meaningful mechanisms of the observed change.
A major limitation of the present study is that data for both groups were collected at different time points, including overlap with COVID-19 pandemic related restrictions. Even though data were collected from both groups following the same procedure, it is possible the environmental differences, such as lockdowns, influenced the outcomes. However, it is important to note that referrals were counted as part of the rehabilitation outcome measure in order to account for this discrepancy. As long as the participant accepted the referral or self-referred to a program, regardless of its availability, this was included in data collection regarding engagement in rehabilitation. Finally, while the group were matched on important demographic, psychiatric, and risk relevant factors, they were heterogenous with respect to setting in that some participants were from inpatient units, while others were outpatients at the time of the study. These different life circumstances may have also accounted for change given previous findings which suggest that criminally involved individuals residing in the community are more hopeful (Martin & Stermac, 2010). The current study did not replicate this finding, and so it does not appear that setting via increased hope accounts for the changes in motivation, aggression, and treatment engagement observed in the MPP group.
The current findings are largely consistent with the small, but important previous studies on preparatory programs for justice involved individuals. However, to our knowledge, the current study is the first to evaluate a pretreatment program delivered to individuals within the forensic psychiatry system specifically. Therefore, there are important research questions that will hopefully confirm, but also help the field better understand, the role of motivation in behavioural change for those who have come into contact with the law. In addition to the issues raised above, future studies would benefit from including multiple data collection points, including follow-up periods, such as 6 month and 1-year reassessments, as well as qualitative methodologies to better understand the experience of pre-treatment interventions and elucidate additional factors contributing to behavioural change. The Rockwood program included naturalistic evaluations built into the participants’ progress through the correctional system, and a similar approach could be applied to studies with longer follow-up, such as annual review board decisions, length of stay, and recidivism. Finally, future research examining differential pre-treatment, subsequent treatment, and engagement effects based on risk stratification may help inform how best to match preparatory and motivational approaches to those most at risk of treatment refusal or drop-out.
Implications
Despite the aforementioned limitations, the current study has practical implications for practice and policy. Adding to the modest literature, these findings are consistent with a common theme, which is that attending to treatment readiness is related to observable and meaningful outcomes, whether it be improved therapeutic engagement, early conditional release, or lower recidivism risk (Marshall et al., 2008; Martin & Stermac, 2010). This conceptual framework is elegantly outlined in the Multifactorial Offender Readiness Model (Ward et al., 2004), which acknowledges the interplay between internal and external conditions impacting on program enrollment, engagement, and performance. The authors argue that change can result from modifications to the person, therapy, or setting. While the setting was not within our control to change, the MPP addresses treatment readiness by a specifically designed program to elicit change within the client. Therefore, by extension, if preparatory programs are associated with potentiated treatment effects, thereby reducing risk or periods of detainment, then it may be possible that they offset considerable legal and healthcare costs associated with inpatient hospitalization, and even intensive community case management within the forensic system.
Conclusion
Individuals involved in the criminal justice and forensic mental health systems face many barriers to change, motivation being perhaps the most fundamental. The present study was, to our knowledge, the first investigation of a pre-treatment intervention in a forensic mental health setting. Consistent with research from correctional rehabilitation (Marshall et al., 2008, McMurran, 2009), preparatory program participants endorsed increased motivation for change, and exhibited relevant behavioural change, reflected in modest decreases in aggression and meaningful increases in rehabilitative engagement. These findings support our conclusion that compared to untreated controls, MPP participants recognized the need for change and were beginning to take the necessary actions to reduce their risk for recidivism and relapse. Importantly, the results add to the growing recognition that addressing responsivity factors—plays a critical role in the ultimate outcome of rehabilitation efforts (Andrews & Bonta, 2016; Moulden & Myers, 2017; Skeem et al., 2015). Indeed, even without stand alone pre-treatment programs, attending to motivation for change, and incorporating MI into standard interventions is likely to yield positive results. These findings may also be interpreted to support the therapeutic approach of MI as much as the preparatory format. That being said, a group format is an efficient and impactful method of addressing motivation, and while preliminary, these data suggest that motivational pre-treatment is a step in the right direction for the forensic mental health system.
Footnotes
Acknowledgements
The authors would like to acknowledge the foundational work of the Rockwood Psychological Services clinical and research team, with special thanks to Dr. Bill Marshall and Dr. Liam Marshall. Additional thanks to Casey Myers who contributed to data collection and preliminary analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.