
Abstract
The link between schizophrenia and homicide has long been the subject of research with significant impact on mental health policy, clinical practice, and public perception of people with psychiatric disorders. The present study investigates factors contributing to completed homicides committed by offenders diagnosed with schizophrenia referred to a Swiss forensic institution, using machine learning algorithms. Data were collected from 370 inpatients at the Centre for Inpatient Forensic Therapy at the Zurich University Hospital of Psychiatry. A total of 519 variables were explored to differentiate homicidal and other (violent and non-violent) offenders. The dataset was split employing variable filtering, model building, and selection embedded in a nested resampling approach. Ten factors regarding criminal and psychiatric history and clinical factors were identified to be influential in differentiating between homicidal and other offenders. Findings expand the research on influential factors for completed homicide in patients with schizophrenia. Limitations, clinical relevance, and future directions are discussed.
Despite decades of research, it has not yet been conclusively clarified whether psychotic disorders are more strongly associated with violence than other mental disorders. Nevertheless, the link between schizophrenia spectrum disorders (SSD) and homicide is well documented (Simpson et al., 2021; Whiting et al., 2021). According to recent studies, the odds of homicidal offenses for individuals with SSD was higher than for other violent offenses with a odds ratio of 19.5 [95% CI 14·7, 25·8] compared to the general population (Whiting et al., 2020). Importantly, the incidence of SSD is only 1.1%, indicating an actual overrepresentation of people with SSD committing homicides. However, in general, homicide among persons with SSD remains rare, with an annual rate of 0.02 to 0.36 per 100,000 persons (Large et al., 2009). About 1 out of 600 patients commits homicide before undergoing antipsychotic treatment, implicating that the initial episode and the untreated symptomatology of the illness itself poses a high risk for homicidal acts. However, it must be noted that the majority of homicidal offenders do not suffer from SSD (Fazel, Gulati, et al., 2009) or engage in violence generally (Buchanan et al., 2019).
In cases of severe violence and homicide committed by persons with SSD, relatives, acquaintances, friends, or treating clinicians are more likely to be victims than strangers (Abreu et al., 2017; Golenkov et al., 2011). Although it is generally rare for people with SSD to exhibit extreme violence—including homicide—triggered by psychosis (O. Nielssen & Large, 2010), certain types of psychotic symptoms are more closely associated with violent behavior than others, such as paranoid delusions or auditory command hallucinations (Pflueger et al., 2015; Swanson et al., 2006; Ullrich et al., 2013). In addition, recent exposure to certain triggers, for example, intentional or unintentional injury, victimization, bereavement, and substance intoxication were found to be linked to a higher risk for violent offending (Sariaslan et al., 2016). Therefore, a closer look at manifestations of symptoms and influencing factors associated with homicide would be useful in assessing the risk of homicidal offenses by psychiatric patients.
The link between mental illness and homicidal behavior has considerable implications for mental health practice and policy, as it justifies allocation of (limited) resources to mental health and criminal justice systems. The findings on this relationship also provide the basis for detention measures to ensure public safety at the expense of the autonomy and freedom of patients (Elbogen & Johnson, 2009; Kirchebner, Günther, Sonnweber, et al., 2020). Focusing on the empirical association between homicide and SSD may potentially increase the stigmatization of people with this condition in the community. Nevertheless, the likelihood that some people with SSD may commit homicides and other violent offenses represents a considerable risk that lawmakers and practitioners are obliged to address. Hence, a more knowledgeable and nuanced approach is needed to understand how, why, and when homicidal behavior occurs in individuals with SSD and whether these individuals have certain characteristics and experiences that distinguish them from other offenders with SSD, because an accurate understanding of SSD-related violence may lead to improved treatment and ultimately reduce stigmatization.
Our definition of “homicide/manslaughter” refers to serious acts of violence against others with the intent to kill and only includes completed homicides and manslaughter. Measuring the relative influence of different variables on homicides committed by people with SSD poses a significant challenge in forensic psychiatry. Few studies have distinguished different types of violent offending behavior, for example, minor and severe offending (cf. Swanson et al., 2006). More often, all types of violent offending are aggregated into a composite variable due to the limited statistical power to differentiate between various forms of violence (Elbogen et al., 2006; Elbogen & Johnson, 2009). While these studies may have assumed that associations are the same irrespective of offense-severity, recent research has demonstrated that offenders accused of different types of offenses also exhibit different mental characteristics and psychopathological presentations (Fioritti et al., 2006; Hachtel et al., 2021; Matejkowski et al., 2008). Thus, there may be features that distinguish offenders who commit completed homicidal acts from offenders who commit non-fatal violent or non-violent offences. The present study aims to address this assumption exploratively using machine learning (ML)—a statistical approach, which has recently been identified as superior in comparison to classic statistical approaches in its sensitivity, specificity, accuracy, and predictive validity (Bzdok & Meyer-Lindenberg, 2018; Hotzy et al., 2018) and is increasingly being used in forensic psychiatry research (Gou et al., 2021; K. Z. Wang et al., 2020).
Employing machine learning algorithms, the objectives of this exploratory study were to investigate whether there exist any essential differences in characteristics between offenders with SSD, who have committed homicide/manslaughter and those who have engaged in other crimes. By incorporating an extensive set of variables (including characteristics of childhood and adolescence, of the time before the index-offense, and related to forensic psychiatric treatment) we aim to identify the most influential of these variables in distinguishing offenders and to quantify a measure of accuracy.
Method
Setting and Sample
This study is embedded in a large-scale project at The Centre for Inpatient Forensic Therapy at the BLINDED University Hospital of Psychiatry in which basic research is conducted on a homogeneous collective of offender patients with SSD. The Centre provides treatment for mentally ill offenders. Patients are admitted either for management of acute syndromes or for long-term detainment and treatment to reduce the risk of recidivism due to their mental illness. They were admitted to the forensic psychiatric institution for “treatment of a mental disorder” according to Article 59 of the Swiss Penal Code, meaning that they had committed an offense that was related to a mental disorder and that an expert evaluation had concluded that psychiatric treatment could reduce the risk of future offenses.
As part of this project, a database was created based on the patients’ extensive forensic medical records. For this purpose, all 1,694 medical records of the patients hospitalized in the clinic from 1982 to 2016 were screened. Individuals with a diagnosis of a SSD including schizophrenia, schizoaffective disorder, and delusional disorder given by their psychiatrist at discharge according to the ICD-9 chapters 295.0 to 295.9 and ICD-10 chapters F20.0 to F25.9 (World Health Organization, 1978, 2016) were identified and included into the study. The final population under investigation consisted of 370 offender patients with SSD with the majority being recorded after the year 2000 (296 cases). For full details on data collection and processing see Kirchebner, Günther, and Lau (2020), Kirchebner, Günther, Sonnweber, et al. (2020), Kirchebner, Sonnweber, et al. (2020), and Günther et al. (2020).
We conducted a retrospective content analysis of case records for all variables using a structured protocol based on Seifert’s extended (Habermeyer et al., 2010; Kutscher et al., 2009) list of criteria (Seifert & Leygraf, 1997). This is a coding protocol developed for the investigation of German offenders in the correctional system and collects a variety of different domains from the enforcement records of the individuals. These include: sociodemographic data, childhood/adolescent experiences, psychiatric history, criminal history, social and sexual functioning, details of the offense leading to forensic hospitalization, jail data, and specifics of the current hospitalization. Psychopathological symptoms were assessed with a close adaptation of the Positive and Negative Symptom Scale (PANSS; Kay et al., 1987) scoring the standard 30 items on a three-point scale (0 = totally absent, 1 = discretely present, and 2 = substantially present). In the process multidisciplinary patient records compiled during the patients’ hospitalization (these included forensic psychiatric reports, charge sheets, court judgments, nursing reports, annual reports, risk assessment reports, discharge reports, medication, etc.) were reviewed and coded by a trained physician. To evaluate inter-rater reliability, a second trained independent rater coded a random subsample of 10% of cases. Cohen’s kappa value (Brennan & Hays, 1992) was .78 and therefore substantial (Lambert et al., 2004).
Finally, the coding protocol was digitized and transferred into a database with over 500 different variables. This database is the source for several exploratory research questions. The present study aimed to exploratively investigate whether and how offender patients with SSD who have committed a homicide differ from the rest of the patients with respect to the 500 variables, and to identify the most important of these variables. Details on the exact operationalization can be found in the next section.
Statistical Methods: Machine Learning
An in-depth description of ML can be found in BLINDED and was partially adopted and extended here. An overview of the statistical steps can be seen in Figure 1 and are further described in the following. All steps were performed using R version 3.6.3. and the MLR package v2.171 (Bischl et al., 2016). CI calculations of the balanced accuracy were conducted using MATLAB R2019a (MATLAB and Statistics Toolbox Release 2012b, The MathWorks, Inc., Natick, Massachusetts, United States) with the add-on “computing the posterior balanced accuracy” v1.0 (Brodersen et al., 2010).
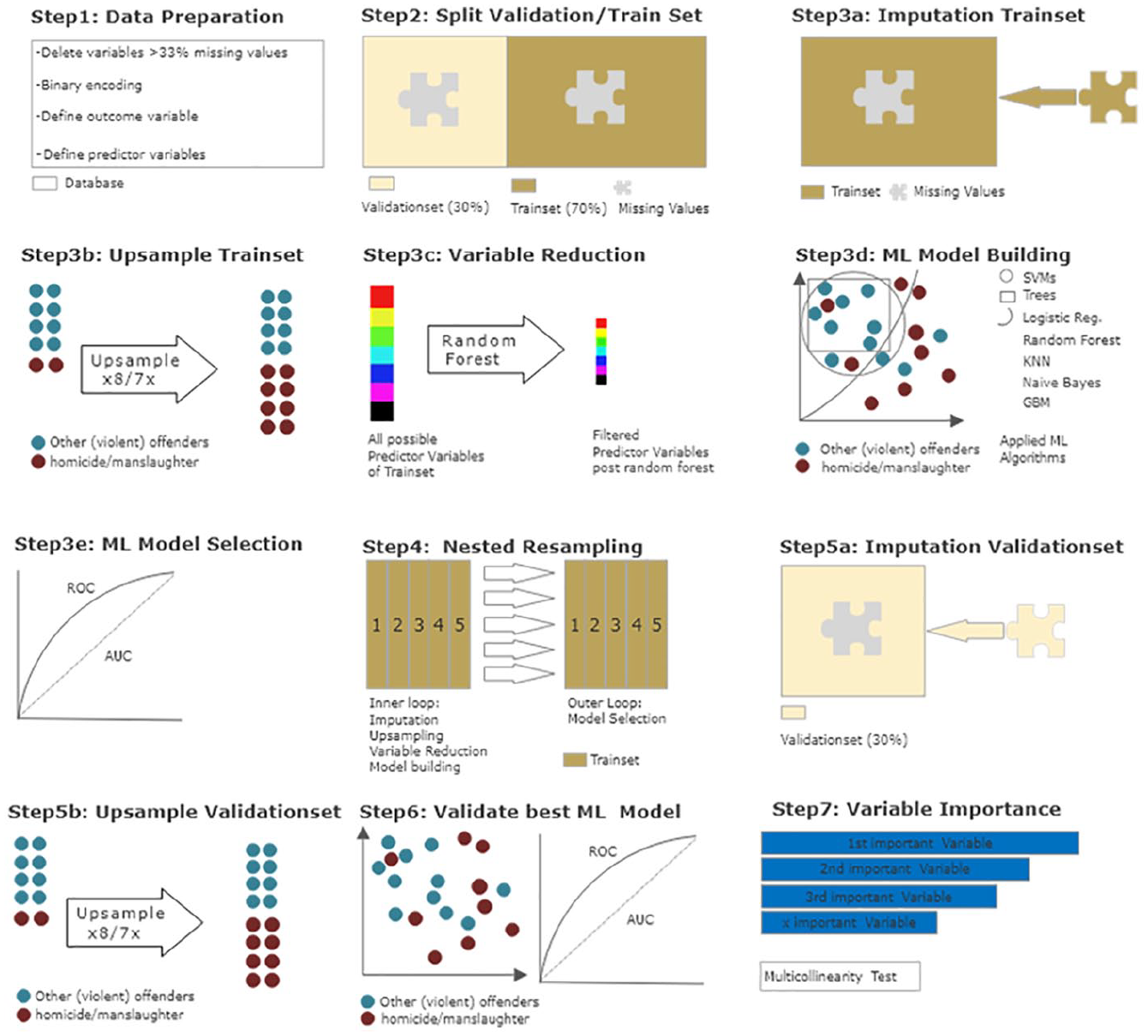
Overview of statistical procedures.
For the initial exploratory analysis (model 1), the outcome variable (type of index offense) was dichotomized into (1) completed homicide/manslaughter and (2) all other offenses (including violent and non-violent offenses). To examine the results of this first analysis in more detail, we have decided to conduct a second analysis (model 2) with (1) homicide/manslaughter and (3) other violent offenses as second outcome variables. The following offenses were considered as violent (based on Swiss law): attempted homicide, assault, rape, robbery, arson, and child abuse. Non-violent offenses included threat, theft, damage to property, minor sexual offenses (e.g., exhibitionism), drug offenses, illegal gun possession, and other minor offenses (e.g., triggering false alarms or emergency brakes). One patient showed missing data on his index offense and was therefore excluded from the study. Of the remaining patients, 40 (10.8%) had committed homicide/manslaughter, 254 (68.8%) had committed a violent index offense and 75 (20.4%) had committed a non-violent index offense. In both models, homicide/manslaughter was defined as the negative class, all other offenses (model 1) and all other violent offenses (model 2) as the respective positive class. A total of 519 dichotomous predictor variables remained. Next, the data set was divided into a training subset (70% of patients) and a validation subset (30% of patients). This was done to separate model building from model validation and reduce the risk of overfitting.
Initial ML modeling: Nested resampling
For model building only the training subset was used. To reduce overfitting and to avoid final model selection to be influenced by data processing, nested resampling (Moons et al., 2014; Studerus et al., 2017) was employed for initial modeling: In an inner loop data processing and model training are performed imbedded in fivefold-cross-validation and then in an outer loop the performance of these models is tested—also embedded in fivefold-cross-validation. Cross-validation is a technique to artificially create different subsamples of a data set (Browne, 2000).
Initial modeling: Data processing and model building
This step was performed within the inner loop of the nested resampling of the training subset. Because some ML algorithms need complete data sets, missing values were imputed via mean and mode algorithms implemented in the MLR package. Weights were stored and used in the validation subset. Due to the imbalance in the distribution of the outcome variable (in model 1 the distribution of homicide/manslaughter versus all other index offenses was 10.8% vs. 89.2% and in model 2 homicide/manslaughter versus violent index offenses was 13.6% vs. 85.4%), the less frequent state of “homicide/manslaughter” was randomly upsampled at a rate of 8 in model 1 and 7 in model 2, thus balancing the data subset, as is recommended for optimal model building (Wei & Dunbrack, 2013). Since the extraction of the most predictive variables without overfitting was a key objective of the current study, a random forest algorithm (Ishwaran & Kogalur, 2022) was used to filter the initial 519 variables. Hyperparameters were not tuned using the original hyperparameters of the MLR package. Finally, discriminative model building was applied with logistic regression, trees, random forest, gradient boosting, KNN (k-nearest neighbor), support vector machines (SVM), and naïve Bayes, as an easily applicable generative model (for a more detailed description see James et al., 2013).
Initial modeling: Model selection
In the outer loop of the nested resampling procedure, the final model was selected by assessing model performance of each model. Model performance was evaluated in terms of balanced accuracy (i.e., the average of true positive and true negative prediction rate, which is suggested for imbalanced data; Brodersen et al., 2010) and goodness of fit (measured with the receiver operating characteristic, balanced curve area under the curve method, and ROC balanced AUC). Moreover, specificity, sensitivity, positive predictive value (PPV), and negative predictive value (NPV) were evaluated. As our training dataset was artificially balanced, the model with the highest AUC was chosen for final model validation in the validation subset of the data (Campbell, 1994). The final set of identified predictor variables was tested for multicollinearity to avoid dependencies between the variables.
Final model evaluation
The validation subset of the original data set was not manipulated except for the imputation of missing values via the stored weights from initial model building (see above). The best performing final model was used and performance measures were reassessed. The predictor variables of the outcome variable in this final model were sorted by indicative power through means of a sensitivity analysis using the gbm package (Cortez & Embrechts, 2013).
Results
The majority of the sample was male (91.6%, n = 339), with a mean age of 34.1 years (SD = 10.2), single (80.8%, n = 299), unemployed (71.1%, n = 263), and not born in Switzerland (54.6%, n = 202), 78.6% (n = 291) of the participants met criteria for schizophrenia, 14.1% (n = 52) met criteria for persistent delusional disorder or an acute and transient psychotic disorder, and 7.3% (n = 27) met criteria for schizoaffective disorder. The patients’ most recent psychiatric placement (index offense) occurred for a violent offense in 79.5% of cases (n = 294).
The performance measures of all trained models during the nested resampling procedure on the initial training dataset (70% of the total dataset) can be seen in Tables 1 and 2. Gradient Boosting was identified as the best performing algorithm for both objectives with a balanced accuracy of 78.23% for the distinction between completed homicide/manslaughter and all other offenses, and a balanced accuracy of 77.45% for homicide/manslaughter versus violent offenses.
Machine Learning Models and Performance in Nested Cross-Validation—Homicide/Manslaughter vs. All Offenses.
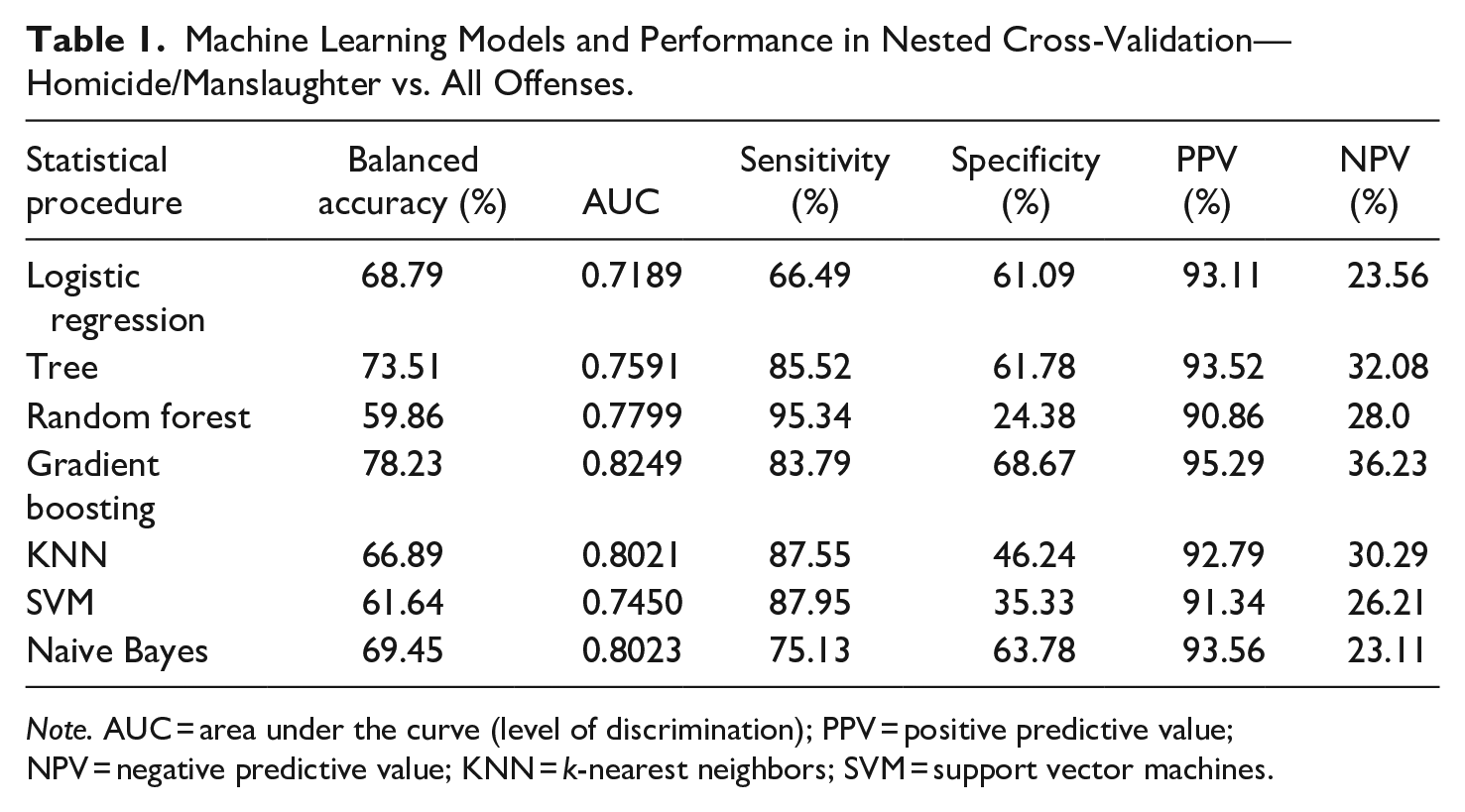
Note. AUC = area under the curve (level of discrimination); PPV = positive predictive value; NPV = negative predictive value; KNN = k-nearest neighbors; SVM = support vector machines.
Machine Learning Models and Performance in Nested Cross-Validation—Homicide/Manslaughter vs. Violent Offenses.
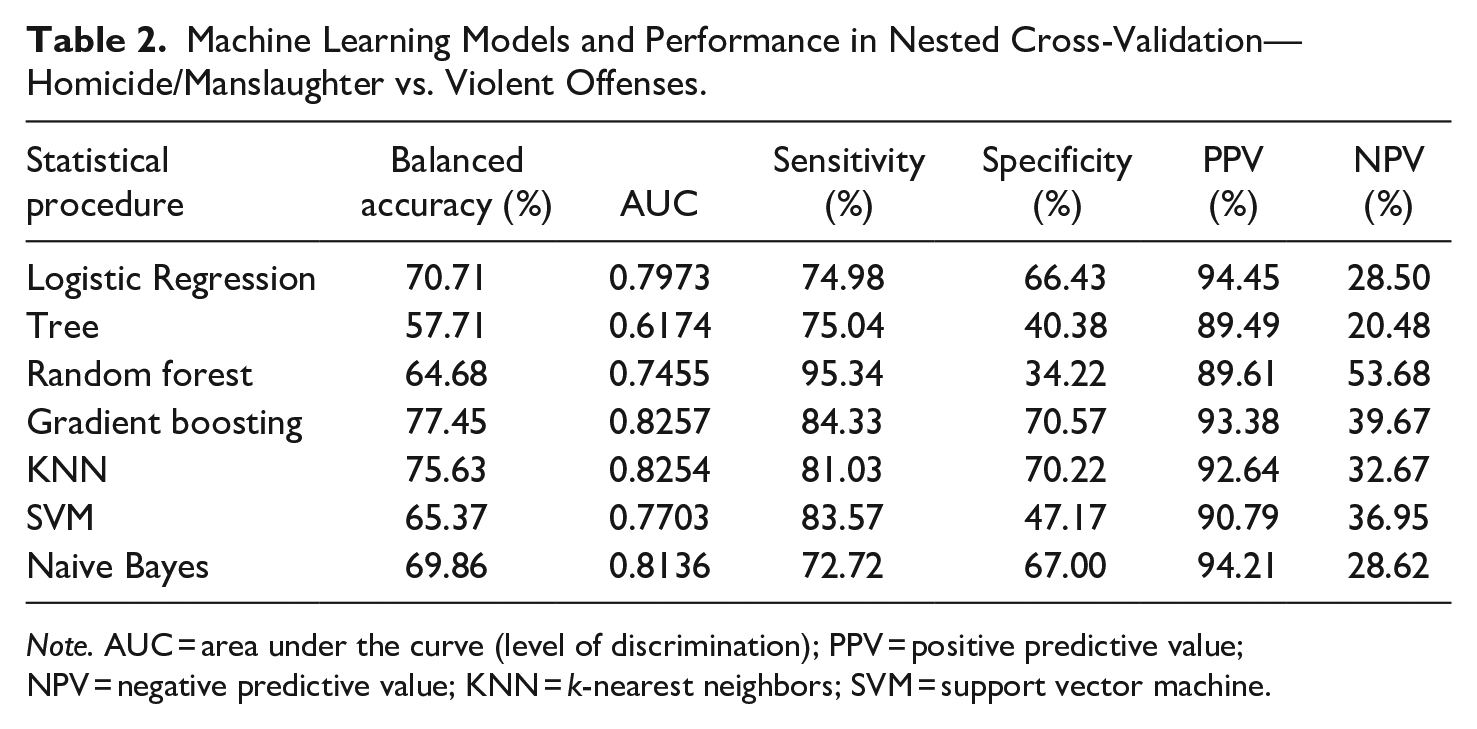
Note. AUC = area under the curve (level of discrimination); PPV = positive predictive value; NPV = negative predictive value; KNN = k-nearest neighbors; SVM = support vector machine.
The 10 most indicative variables (code, description, and distribution) for each objective, which were identified by random forest testing and subsequently used for model building, can be seen in Tables 3 and 4.
Absolute and Relative Distribution of Indicative Variables—Homicide/Manslaughter vs. All Offenses.
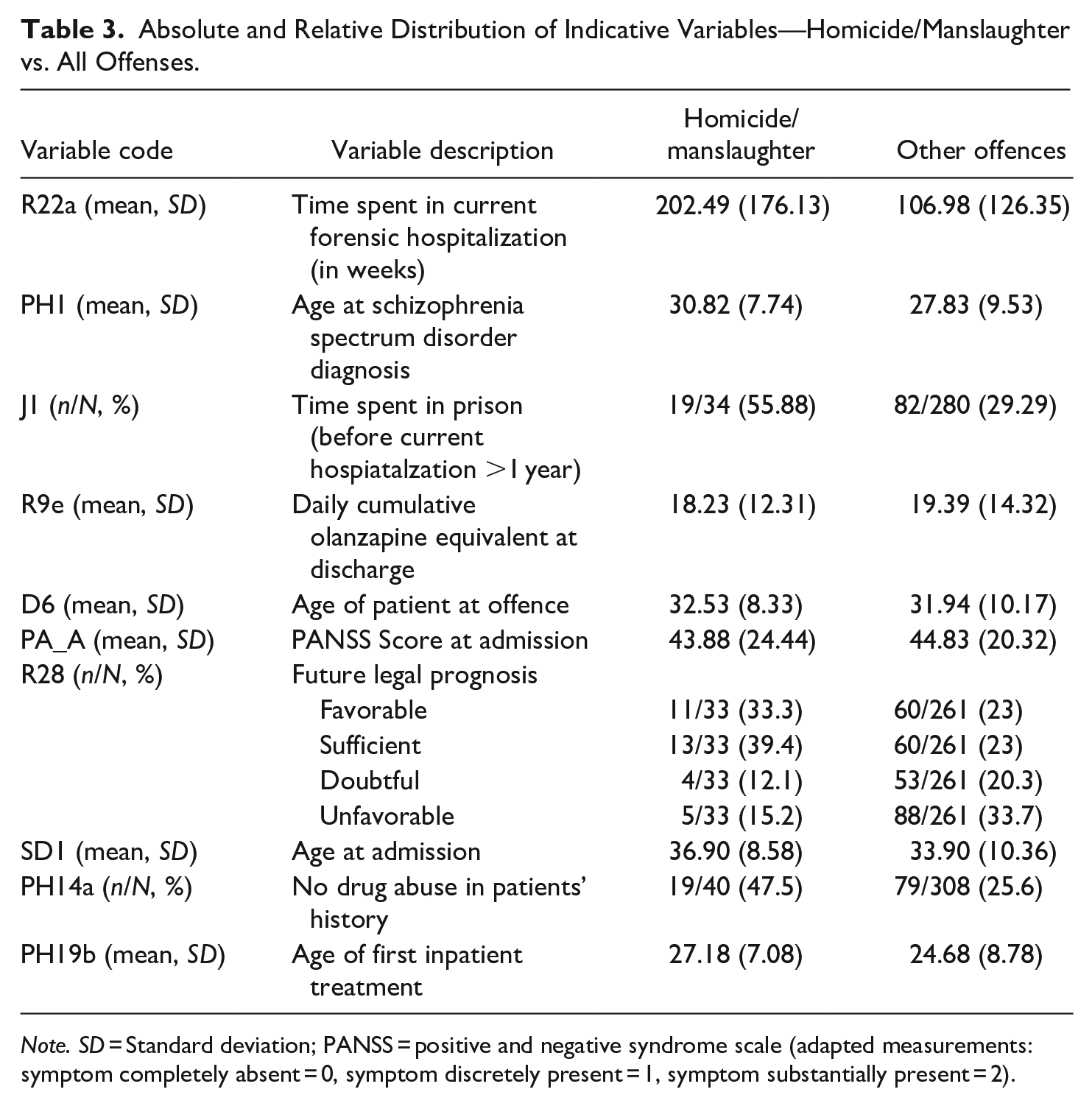
Note. SD = Standard deviation; PANSS = positive and negative syndrome scale (adapted measurements: symptom completely absent = 0, symptom discretely present = 1, symptom substantially present = 2).
Absolut and Relative Distribution of Indicative Variables—Homicide/Manslaughter vs. Violent offenses.
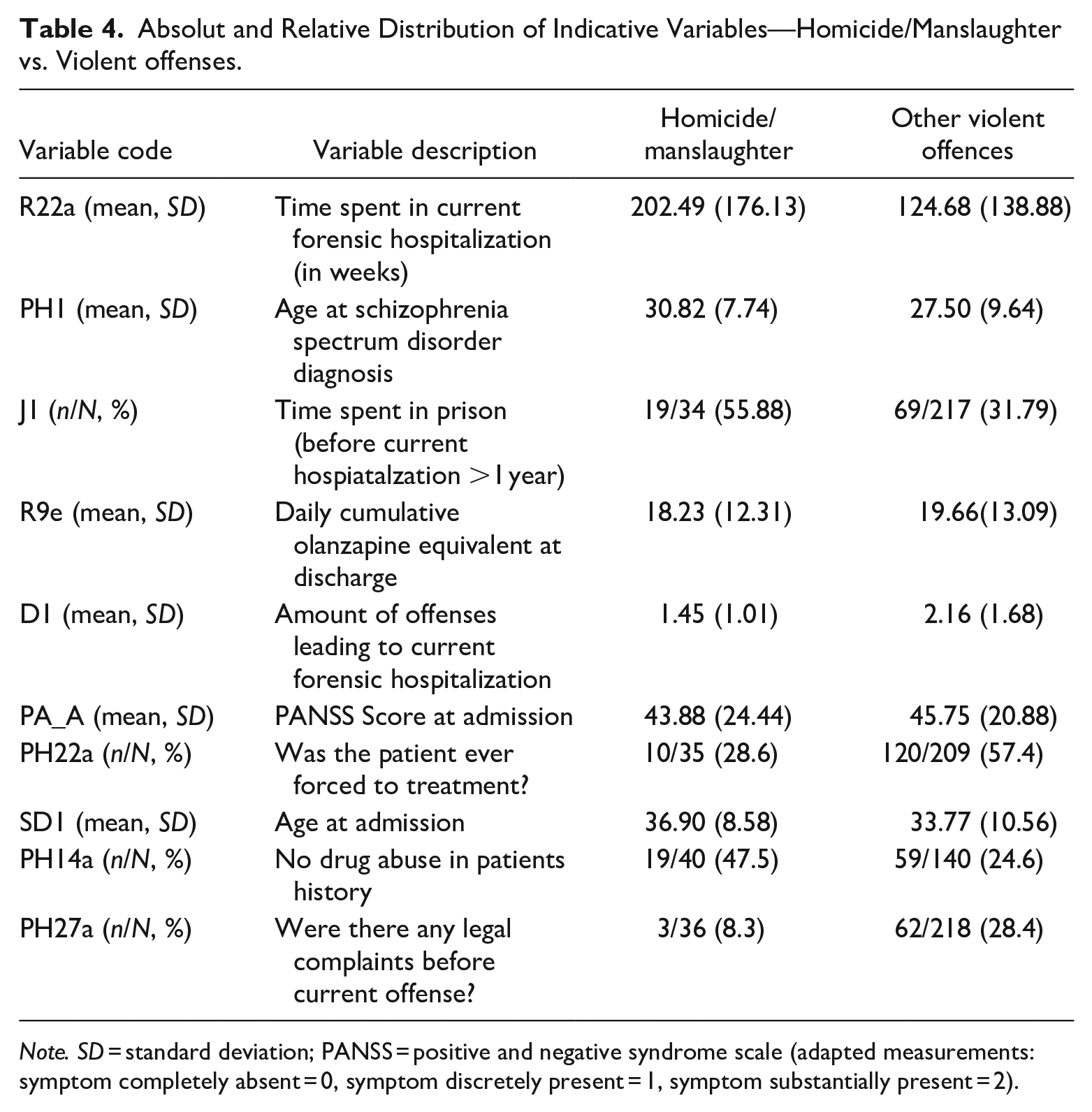
Note. SD = standard deviation; PANSS = positive and negative syndrome scale (adapted measurements: symptom completely absent = 0, symptom discretely present = 1, symptom substantially present = 2).
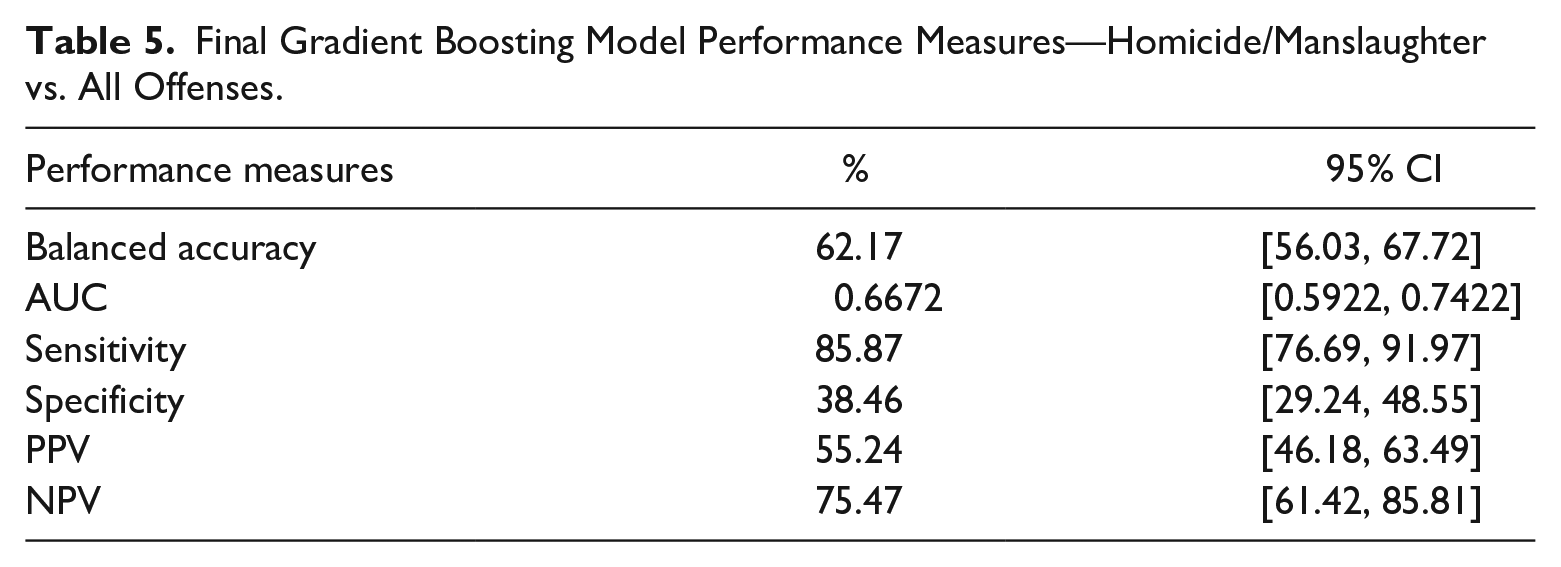
For the first objective (homicide/manslaughter vs. all other offenses), the final gradient boosting model using these variables applied to the validation subset (30% of the total data set) yielded a balanced accuracy of 62.17% and an AUC of 0.67 (see Table 5). This model showed a sensitivity of 85.78%, reflecting its ability to correctly classify other offenses and a lower specificity of 38.46%, indicating its ability to correctly identify the actual homicidal offenses.
Final Gradient Boosting Model Performance Measures—Homicide/Manslaughter vs. All Offenses.
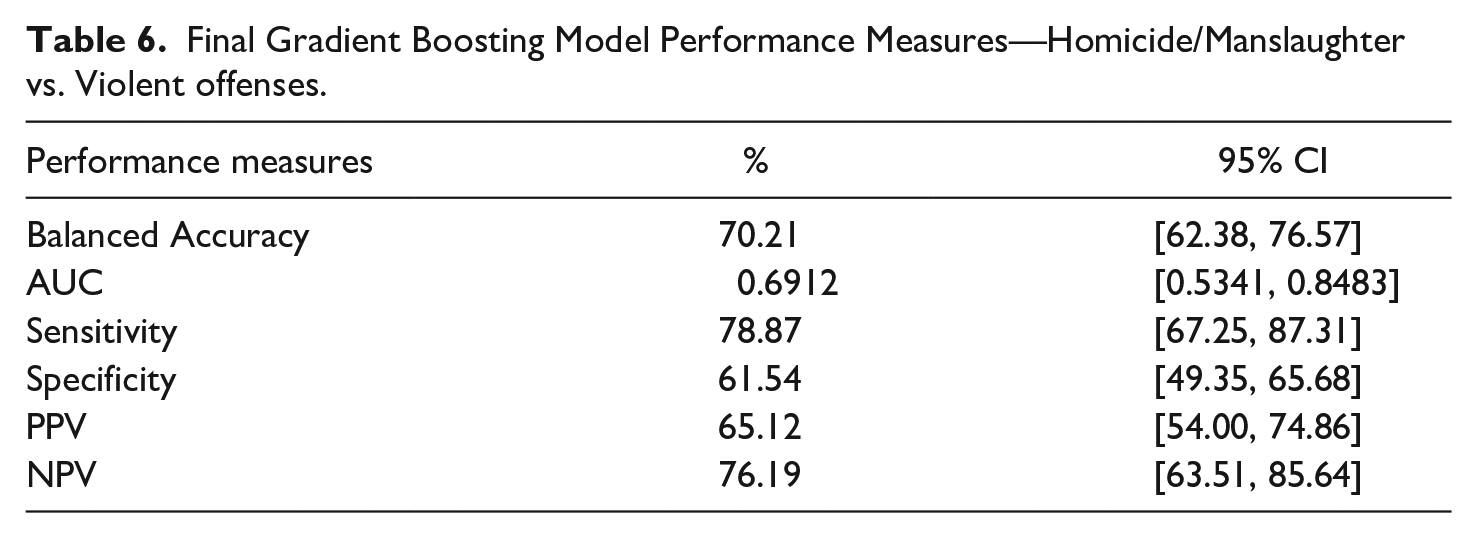
For our second objective (homicide/manslaughter vs. other violent offenses), the final gradient boosting model yielded a balanced accuracy of 70.21% and an AUC of 0.69 (see Table 6). This model showed a sensitivity of 78.87% (correctly identifying violent offenses) and a specificity of 61.54% (correctly identifying actual homicides).
Final Gradient Boosting Model Performance Measures—Homicide/Manslaughter vs. Violent offenses.
Testing for multicollinearity showed no dependencies between the variables. The importance of each variable in the gradient boosting model can be seen in Figures 2 and 3.
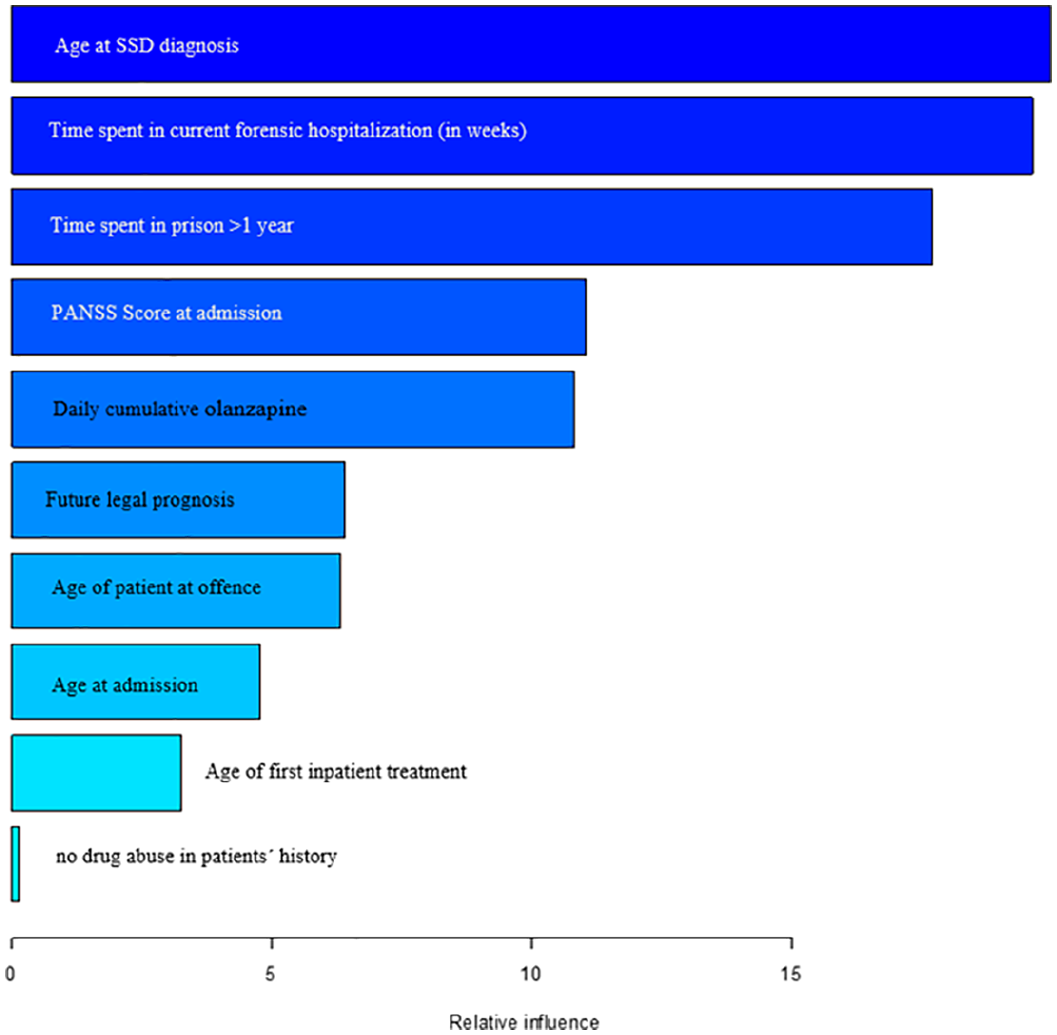
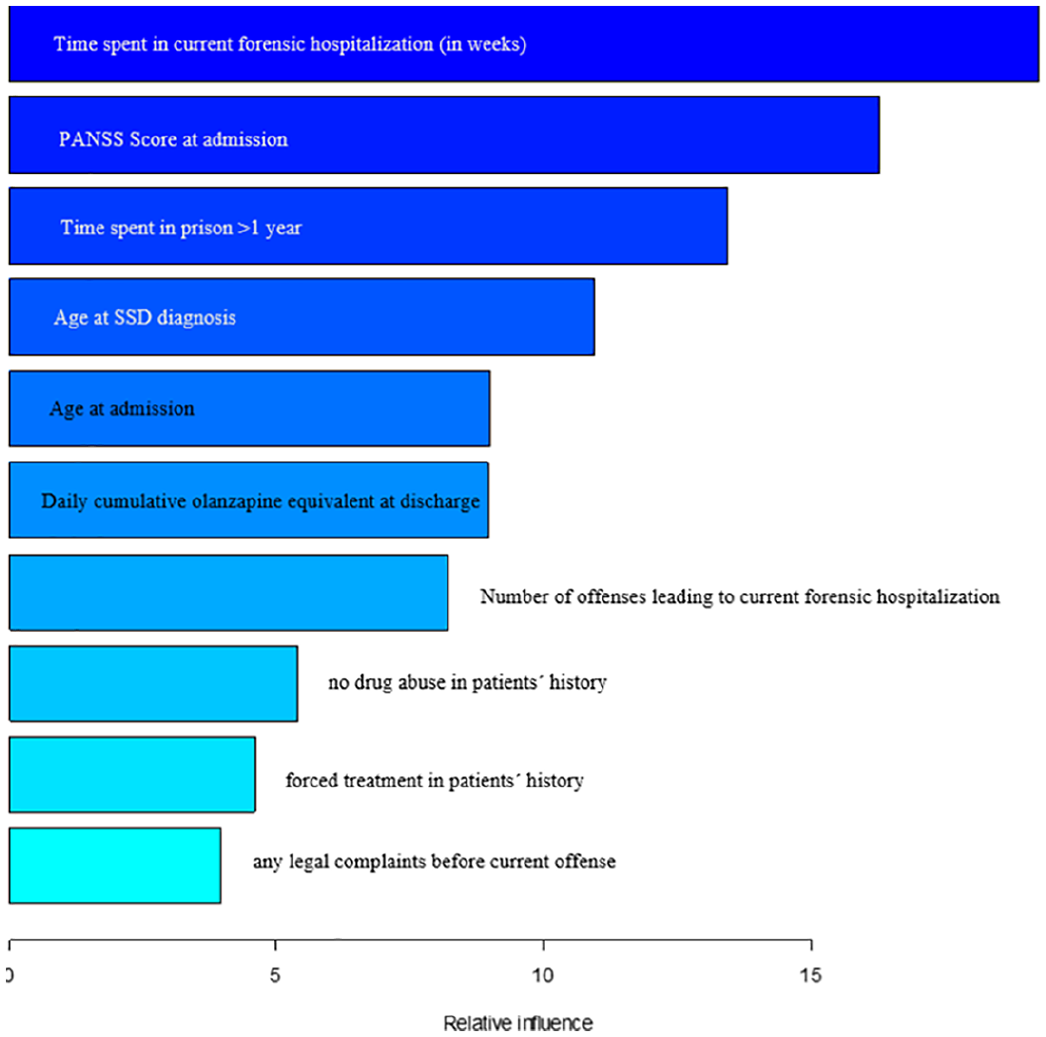
Variable importance of final model homicide/manslaughter versus all other offenses.
Variable importance of final model—homicide/manslaughter versus violent offenses.
Time spent in current forensic hospitalization (202.5 weeks for homicidal offenders vs. 107 weeks for other offenders), the age of first diagnosis of SSD (30.8 years vs. 27.8 years), and time spent in prison over 1 year (55.9% vs. 29.3%) were identified as the most indicative factors for the distinction between homicide/manslaughter and all other offenses. Olanzapine equivalent at discharge (18.2 vs. 19.4), age of patient at index offense (32.5 years vs. 31.9 years), age at admission (36.9 years vs. 33.9 years), and age at first inpatient treatment (27.2 years vs. 24.7 years), PANSS total score at admission (43.9 vs. 44.8) were also identified as factors influencing the model, as were no drug abuse (47.5% vs. 25.6%), and favorable legal prognosis (33.3% vs. 23%).
The most influential variables for the distinction between homicide/manslaughter and violent offenses were again time spent in current forensic hospitalization (202.5 weeks for homicidal offenders vs. 124.7 weeks for violent offenders), the age of first diagnosis of SSD (30.8 years vs. 27.5 years), time spent in prison over 1 year (55.9% vs. 31.8%), and olanzapine equivalent at discharge (18.2 vs. 19.7). Furthermore, the variables number of offenses leading to current forensic hospitalization (1.45 vs. 2.2), PANSS total score at admission (43.9 vs. 45.8), coercive treatment in patients’ history (28.6% vs. 57.4%), no drug abuse (47.5% vs. 24.6%), age at admission (36.9 years vs. 33.8 years), and any legal complaint before current admission (8.3% vs. 28.4%) were also identified as being highly influential.
Discussion
The aim of our exploratory study was to identify factors that distinguish between homicide/manslaughter and all other offenses committed by individuals with SSD in order to provide an initial exploratory overview. By employing ML algorithms and a unique database, we were able to build a model comprising 10 factors. To obtain an even more detailed picture of individuals who committed homicide, a second analysis was performed to distinguish between completed homicide/manslaughter and other (non-fatal) violent crimes. Variables related to criminal and psychiatric history as well as clinical factors have been identified to be highly influential and are described in more detail below.
In both models, homicidal patients were older at diagnosis of SSD, at committing the index offense, at admission to forensic treatment and at first inpatient treatment. In comparison to other violent offender patients, homicidal patients were less likely to have criminal records preceding their index offense. This finding supports previous research on offenders suffering from SSD, which identified a subgroup characterized by suddenly committing a very serious crime in their late 30’s and without any criminal history (“Type III” or “late late starters”; Hodgins et al., 2014; Simpson et al., 2015). J. Wang et al. (2019) report similar results: only 6.5% of their examined homicide offenders had committed offenses in the past and for most of them this was their first offense. Other studies (Fioritti et al., 2006; Meehan et al., 2006; O. B. Nielssen et al., 2007; O. Nielssen & Large, 2010) also found the average age to be over 30 years, which is older than the average age at full expression of the illness in most studies on SSD (Large et al., 2008) and also older than homicide offenders in the general population (O. Nielssen & Large, 2010). Patients in the first episode of psychosis might have a pattern of positive symptoms associated with violence (e.g., impulsivity, irritability, and hallucinations). By contrast, negative symptoms in the later course of SSD might decrease the occurrence of violence due to their drive-reducing effect. Furthermore, it is possible that a course of treatment with antipsychotic medication might have a lasting neurobiological effect that decreases the probability of violent behavior (O. Nielssen & Large, 2010).
In addition, a subgroup of offenders with SSD characterized by suddenly committing a very serious crime in their 30’s and without any criminal history was identified in recent research (Hodgins et al., 2014; Simpson et al., 2015). J. Wang et al. (2019) report similar results: only 6.5% of their examined homicide offenders had committed offenses in the past and for most of them this was their first offense. Therefore, the risk of homicide in patients with SSD without having committed any prior offenses should not be disregarded.
Homicidal patients seemed to exhibit less severe illness-specific factors than all other offender patients. They had lower PANNS scores at admission and required less medication upon discharge. We suspect that non-violent offenders are more likely to engage in inappropriate and bizarre social behavior that attracts negative attention and tend to commit minor offenses more frequently, which may cause more regular involvement with the legal system and a higher likelihood for coercive psychiatric measures (which occurred twice as frequent among other violent offender patients than among homicidal patients). This may also lead to further mandatory outpatient psychiatric treatment (e.g., for probation) and regular follow-up visits so that minor offenses might be identified more often. The fact that homicidal patients were older at the time of committing the index offense and had less prior contact with the legal system or mental health services than all other offenders could be an indication of a less pronounced but chronic pathology and better pre-morbid social functioning and may imply less severe neuropsychological impairments until the full clinical manifestation of the disorder is evident. This would be in line with findings suggesting that patients with SSD and a history of violence exhibit greater impairment of intellectual and executive functions than patients without such a history (Fioritti et al., 2006; Hodgins, 2017; Kumari et al., 2006). This could in turn indicate that acts involving serious violence represent higher levels of psychosocial organization.
In addition, homicidal patients in our sample were considerably less likely to have abused drugs in the past than all other offender patients, again suggesting less impaired brain structures, especially in comparison to patients with chronic and multiple substance abuse (Tracy et al., 1995). Nonetheless, neurocognitive function should be considered along with other clinical and social variables when assessing violent individuals with SSD, as previous studies found that neuroanatomical abnormalities and deficits in neuronal activation contribute to violent behavior in individuals with SSD (Kumari et al., 2006; Stratton et al., 2017). Clinicians should therefore be alert to a combination of factors, namely impaired attention and executive function, auditory hallucinations, paranoid delusions, and criminal history, that may pose a risk for homicidal acts, as suggested in previous research (Kumari et al., 2006; Stratton et al., 2017).
Furthermore, lifelong antisocial behavior, that is, frequently preceded by conduct disorder in childhood, was found to be a major risk factor for violent offending in adult life (Witt et al., 2013). However, that study did not provide a more detailed description of the construct of violence used. Thus, it should be investigated whether this also influences the incidence of homicides in individuals with SSD.
Homicidal patients remain longer in the legal system (prison, forensic psychiatry)—despite better legal prognosis. This is in line with previous findings arguing that the length of inpatient forensic treatment may be determined by factors that were apparently unalterable by treatment efforts (Fioritti et al., 2006; Kirchebner, Günther, Sonnweber, et al., 2020). Patients who have committed homicidal offenses may face more difficult obstacles to release, than patients who have shown less severe criminal behavior. Clinicians and courts may feel responsible for preventing similarly serious crimes by all means, incorporating public safety policy considerations and the individual views of clinical and public risk assessment decision-makers, and may discourage innovative treatment initiatives. Favorable therapeutic developments in offender patients that would justify discharge from forensic inpatient treatment for less serious crimes may be mistrusted in cases with serious index offenses. Whilst forensic psychiatry should not base treatment decisions merely on the severity of the index offense, but rather on risk evaluation and positive developments of offender patients, this seems to be difficult in criminal cases involving a high degree of emotion due to the severity of a crime.
No distal factors (such as childhood/adolescence and experiences of sexual or physical abuse) or social (e.g., victimization) and environmental (e.g., socio-economic status and ethnicity) factors could be identified, which is somewhat surprising, since these factors were found to be increasing violence risk (O’Reilly et al., 2015; Witt et al., 2013). Many of these difficulties are likely caused by cognitive impairment and decline in patients with SSD (O’Reilly et al., 2015; Soyka, 2011). This again points toward our consideration that homicidal patients show better cognitive performance and less impairment. Explanations may include better premorbid functioning, later onset of SSD and a shorter period of being untreated. Interestingly, the country of origin did not play a central role although more than half of the patients were not born in Switzerland. This is in line with the findings of a study on this specific population, which identified social and therapeutic factors, rather than the severity of the offense, as the decisive differences between Swiss and foreign individuals (Huber et al., 2020).
Regarding psychiatric co-diagnoses it is worth noting that neither personality disorders (including antisocial and conduct disorder) nor substance abuse were found as differentiating factors in this analysis. This is inconsistent with previous findings that have linked personality disorders and substance abuse to a higher likelihood of violence in SSD patients (Baird et al., 2020; Fazel, Langström, et al., 2009; Hodgins et al., 2005; Swanson et al., 2006; Walsh et al., 2002) and requires further clarification. This could be due to the fact that only about 10% of the studied population had received a co-diagnosis of personality disorder, which is due to the local diagnosis approach that follows ICD-10, which specifies that no diagnosis should be assigned if the behavior is due to another disorder, in this case SSD.
With the exception of factors regarding psychopathology (PANSS and medication), all factors identified were static in nature and thus hardly or not alterable by therapy. What can be changed though, is patients’ self-awareness through more individualized therapeutic approaches and more resources in prevention and early detection.
Limitations
In the present analysis, data was collected retrospectively, and although the files used in this study were of high quality, the possibility of distortions could not be completely excluded, including the use of a PANSS-adapted scale for the content analysis of psychopathological data, which in some cases were recorded before the publication of the instrument.
While some of the influencing factors found in this study may represent associations with the outcomes, they do not imply causality, and further prospective studies must be conducted before firm conclusions can be drawn about the influence of specific factors on homicidal behavior in patients with SSD.
In addition, due to the retrospective nature of the data, important variables that have previously been considered critically important factors influencing homicides of individuals with SSD, such as the presence of psychopathy (Fox & DeLisi, 2019) and adherence to (medication) therapy (Baird et al., 2020; Carabellese et al., 2021) at the time of the offense, could not be examined. Another limitation is the small number of homicidal patients compared to other violent or non-violent patients in our sample. To compensate for this imbalance, up-sampling, and balancing methods were applied.
It should be noted that ML achieves particularly good results with large-scale data sets, so that the 370 patients analyzed here represent a rather limited number in this context and thus, despite cross-validation, overfitting remains a limitation to the interpretive power of this study.
Future Research Directions
More attention should be paid to the measurement, operationalization, and context of serious violence and homicidal behavior. Since the outcome variable “violence” was not specified in more detail in many previous research studies (Kumari et al., 2006; Stratton et al., 2017; Witt et al., 2013), the comparability between different studies is limited. Consequently, the term “violence” should be clearly operationalized in future studies. Relying solely on records or self-reports often excludes the measurement of other characteristics of violence such as motivation, targets, or setting.
Clinical Implications
It is possible that the quality of mental health services provided and the lack of adequate (individualized) services may influence the risk of homicide, for example, in terms of earlier recognition of SSD and treatment adherence and compliance. More effective communication and education of professionals working in the (mental) health care sector could enable earlier intervention in the case of previously undetected risk factors for homicidal behavior in people suffering from SSD.
As SDD is one of the major causes of disease-related disability in the world (Świtaj et al., 2012; Tandon et al., 2008) and is widely associated with dangerousness, a better understanding of antecedents of homicides in individuals with SSD may be helpful in developing viable preventive and therapeutic approaches targeting at high-risk patients and could potentially reduce the prevalence of homicides.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed and approved by the Ethics Committee Zurich [Kanton Zürich] (committee’s reference number: KEK-ZH-NR 2014-0480). The study complied with the Helsinki Declaration of 1975, revised in 2008. This is a retrospective study. For this type of study formal consent is not required.