
Abstract
This study examined the influence of treatment motivation on posttreatment effectiveness of an outpatient, individual social skills training for juvenile delinquents imposed as a penal sanction. Propensity score matching was used to match a control group of juveniles receiving treatment as usual (n = 108 of total N = 354) to a treatment group of juveniles receiving Tools4U, a social skills training with a parental component (N = 115). Treatment motivation was examined as a moderator and predictor of treatment effects on impulsivity, social perspective-taking, social problem-solving, lack of critical reasoning, developmental task-related skills, and parenting skills. Treatment effects were mostly consistent across juveniles with different levels of treatment motivation. Only one moderating effect was found on active tackling (i.e., actively addressing problems), and predictive effects were found on seeking social support, cognitive empathy, hostile intent attribution, and self-centeredness. Implications for further research are discussed.
In the past decades, the focus of treatment effectiveness research has shifted from what works in general to what works under what conditions and for whom (Bonell, Fletcher, Morton, Lorenc, & Moore, 2012; Stoltz, Deković, Van Londen, Orobio de Castro, & Prinzie, 2013). As a result of this shift, several scholars have emphasized the importance of moderator analyses in treatment effectiveness studies (Kazdin, 2007; Kraemer, Wilson, Fairburn, & Agras, 2002). Moderator analyses are now conducted in a growing body of research to determine generalizability of treatment outcomes, to specify target groups for treatment delivery, to further investigate iatrogenic or non-significant treatment effects, and ultimately, to gain insights treatment effectiveness (MacKinnon, 2011).
While moderator analyses on demographic variables, such as age, gender, and ethnicity, have become fairly common, few studies have included other baseline measures in moderator analyses (Bonell et al., 2012; MacKinnon, 2011). Furthermore, few studies have distinguished between predictors and moderators of treatment effects, while this distinction is particularly important for the practical implications of treatment outcomes (Curry et al., 2006). That is, predictors are variables that predict treatment outcomes similarly for both the experimental and control treatment, whereas moderators specify for whom or under what conditions the specific treatment shows effects (Kraemer et al., 2002). Predictors are thereby indicative of a more general (un)treatability, whereas moderators identify groups for whom the treatment of interest is particularly (un)suitable.
In the present study, we examined the influence of treatment motivation (or amenability to treatment; Kazdin, 1995) as both a predictor and moderator of treatment effectiveness. Based on the Risk-Needs-Responsivity (RNR) principles, juvenile offender treatments need be tailored to the juveniles’ Risk, Needs, and Responsivity to be effective (Andrews & Bonta, 2010; Andrews, Bonta, & Hoge, 1990; Andrews & Dowden, 2007). The Responsivity principle specifically states that effective juvenile offender treatment should be tailored to offender characteristics including treatment motivation. Subsequently, several authors have stressed the importance of treatment motivation for treatment effects and its underrepresentation in the existing RNR model (Looman, Dickie, & Abracen, 2005; Miller & Rollnick, 2002; Ward, Melser, & Yates, 2007).
In the present literature, there is much ambivalence about the relation between treatment motivation and treatment outcomes. Several studies have found a positive relation between treatment motivation and treatment effects (Harder, Knorth, & Kalverboer, 2012; McMurran, 2009; Olver, Stockdale, & Wormith, 2011; Rosenkranz, Henderson, Muller, & Goodman, 2012). Other studies have found that treatment motivation does not affect treatment outcomes directly, but at most predicts treatment retention (De Leon, Melnick, Thomas, Kressel, & Wexler, 2000; Grella & Rodriguez, 2011; Melnick, De Leon, Thomas, Kressel, & Wexler, 2001; Snyder & Anderson, 2009). Consequently, some scholars have stressed the importance of baseline motivation (Cady, Winters, Jordan, Solberg, & Stinchfield, 1996) for effective treatment, whereas others have viewed motivation as a dynamic attribute that can develop during treatment (Prochaska, 1995). Even then, motivational changes have not always been associated with behavioral change (McMurran, 2009). Existing research on treatment motivation, however, has focused mainly on residential and/or drug treatment, but little on non-residential juvenile offender treatment (Breda & Riemer, 2012; Nock & Photos, 2006), and even less on the moderating effects of treatment motivation on treatment outcomes (Englebrecht, Peterson, Scherer, & Naccarato, 2008). This is surprising given the weight given to motivation by researchers and juvenile offender policy makers.
A frequently used model of treatment motivation is the transtheoretical motivation model of Prochaska and DiClemente (1986, 1994). This model distinguishes four phases of treatment motivation: precontemplation (not considering change), contemplation (considering change but not acting on it), decision-making (considering change and planning to act on it soon), and active change (acting on the desired behavior). Research has found precontemplators and contemplators to be the least motivated to change (DiClemente & Hughes, 1990). It has been argued that treatment needs to be tailored to the participants’ motivational phase to be effective, regardless of the specific phase (O’Hare, 1996; Prochaska, DiClemente, & Norcross, 1992; Snyder & Anderson, 2009). For instance, behavioral-oriented treatment techniques would be more appropriate for the active change phase, whereas cognitive-oriented treatment techniques would be more fitting for the precontemplation and contemplation phases. It is however generally acknowledged that these motivational phases do not occur in a fixed order (Morrison, Ross, Kemp, & Kalman, 2010; Verdonck & Jaspaert, 2009; West, 2005), and the model may lack empirical support (Whitelaw, Baldwin, Bunton, & Flynn, 2000). The usefulness of this model for offender treatment has therefore been questioned (Casey, Day, & Howells, 2005; Williams, McGregor, Zeldman, Freedman, & Deci, 2004).
In response to the constraints of the transtheoretical motivation model, Burrowes and Needs (2009) developed the context of change model. According to this model, a combination (and interaction) of individual, catalyst, and context factors will influence an individuals’ readiness to change. Individual factors are juveniles’ (personality) characteristics and beliefs that may enable or prohibit change. This factor could, for instance, explain why only intrinsic (and not external) motivation will lead to treatment effects (Breda & Heflinger, 2004; Chambers, Eccleston, Day, Ward, & Howells, 2008; McMurran, Theodosi, & Sellen, 2006). Furthermore, the catalyst is one or more (external) event(s) that enhances or facilitates an individual’s potential and readiness to change, such as treatment. Finally, the environment is the social and actual environment in which the juvenile is supposed to change, such as family and residence. According to this model (internal), treatment motivation could be an important individual factor to turn treatment potential (catalyst) into actual change. A certain level of (internal) treatment motivation during treatment, therefore, seems necessary to achieve and maintain juvenile offender treatment effects. This is also confirmed by previous research showing that positive treatment effects depend on high levels of treatment motivation, whereas low levels of treatment motivation may hinder a positive response or susceptibility to treatment (Olver et al., 2011).
To our knowledge, no studies to date have been conducted examining the influence of treatment motivation on social skills training (SST) treatment effects for juvenile delinquents. Treatment motivation may be limited for delinquent juveniles to begin with, because research has shown that increased problem severity and internalizing, but not externalizing problems, are associated with the highest levels of treatment motivation (DiGiuseppe, Linscott, & Jilton, 1996; Englebrecht et al., 2008; Leenarts, Hoeve, Van de Ven, Lodewijks, & Doreleijers, 2013; Phares & Danforth, 1994; Rosenkranz et al., 2012). Furthermore, mandated treatment would imply limited (internal) motivation (Wild, Newton-Taylor, & Alletto, 1998), although some have countered this assumption (Koehler, Lösel, Akoensi, & Humphreys, 2013; O’Hare, 1996). Arguably, internal “genuine” motivation is an important precondition for effective treatment (McMurran, 2002; Miller & Rollnick, 2002; Olver et al., 2011). The influence of treatment motivation for SST and juvenile offender populations is therefore unclear.
The Present Study
The aim of the present study is to examine the role of treatment motivation as a predictor and moderator of the effectiveness of a SST for juvenile delinquents, Tools4U. In line with most SSTs, Tools4U is a relatively brief and “light” intervention, specifically intended for adolescent onset delinquents with moderately severe delinquency trajectories (Loeber, Farrington, Stouthamer-Loeber, & Van Kammen, 1998). In addition, it has a parental component to improve positive parental involvement (Albrecht & Spanjaard, 2011).
The present study is part of a larger research project in which the implementation and effectiveness of Tools4U in The Netherlands were assessed in a matched control study on 223 juvenile offenders who received either SST Tools4U or Treatment as Usual (TAU; Van der Stouwe, Asscher, Hoeve, Van der Laan, & Stams, 2016). The results of this study showed that Tools4U is indeed successful in producing positive posttreatment changes in impulsivity, cognitive distortions (i.e., self-centeredness and assuming the worst), and social information processing (i.e., hostile intent attribution). There were, however, no treatment effects on protective factors (social problem-solving, behavioral adjustment), and the parental component only improved parenting skills in caretakers of girls. Finally, after Tools4U, juveniles reported significantly less social acceptance and self-worth than juveniles receiving TAU. Treatment effects on (re)offending will be investigated in a later follow-up study. Knowledge of the effectiveness of Tools4U for adolescents with different levels of treatment motivation could explain the (absence of) treatment effects and help indicate for whom this relatively brief and “light” intervention is effective. In addition, it might help to improve treatment effects by tailoring the intervention to their specific (motivational) needs.
We used a trichotomy of motivation, as literature suggests that treatment effects may vary for the extreme poles of motivation. Low motivation may result in the worst treatment outcomes (Harder, Knorth, & Kalverboer, 2011; Harder et al., 2012; Mulder, Vermunt, Brand, Bullens, & Van Marle, 2012), whereas juveniles with high motivation may show better treatment effects (McMurran, 2009). In addition, it is in line with existing literature about risk and protective factors for juvenile delinquency, which frequently uses either the negative or positive pole of predictive factors (see Lösel & Farrington, 2012). Finally, a taxonomic approach allows for better practical use of the outcomes. That is, using a cutoff point for low and high treatment motivation will better guide recommendations about for whom the intervention is appropriate and for whom it is not.
In line with the context of change model (Burrowes & Needs, 2009), we expected juveniles with the highest levels of treatment motivation to benefit the most from Tools4U, and those with the lowest levels to benefit the least. Furthermore, as treatment motivation has been associated with problem-solving skills in previous research (Raftery, Steinke, & Nickerson, 2010; Van der Helm, Beunk, Stams, & Van der Laan, 2014), and as the previous study found no treatment effects on social problem solving, we expected treatment motivation to moderate problem-solving skills outcomes in particular.
Methods
Participants
The majority of the sample were boys (n = 159, 71%), and almost a third girls (n = 64 girls, 29%) with an average age of M = 15.71 (SD = 1.53) years. Half of the juveniles had a Dutch ethnicity (n = 111, 50%). Of the ethnic minority group, most had a non-Western (i.e., South American or African) background (n = 97, 87%). Over half received their sentence for a property offense (n = 66, 30%) or person offense (n = 63, 28%), with an average of M = 31.74 (SD = 25.82) sentenced hours. Table 1 shows the distribution of gender, ethnicity, offense, and sentenced hours per level of treatment motivation for both treatment conditions.
Characteristics of Tools4U and TAU Group After Propensity Score Matching.
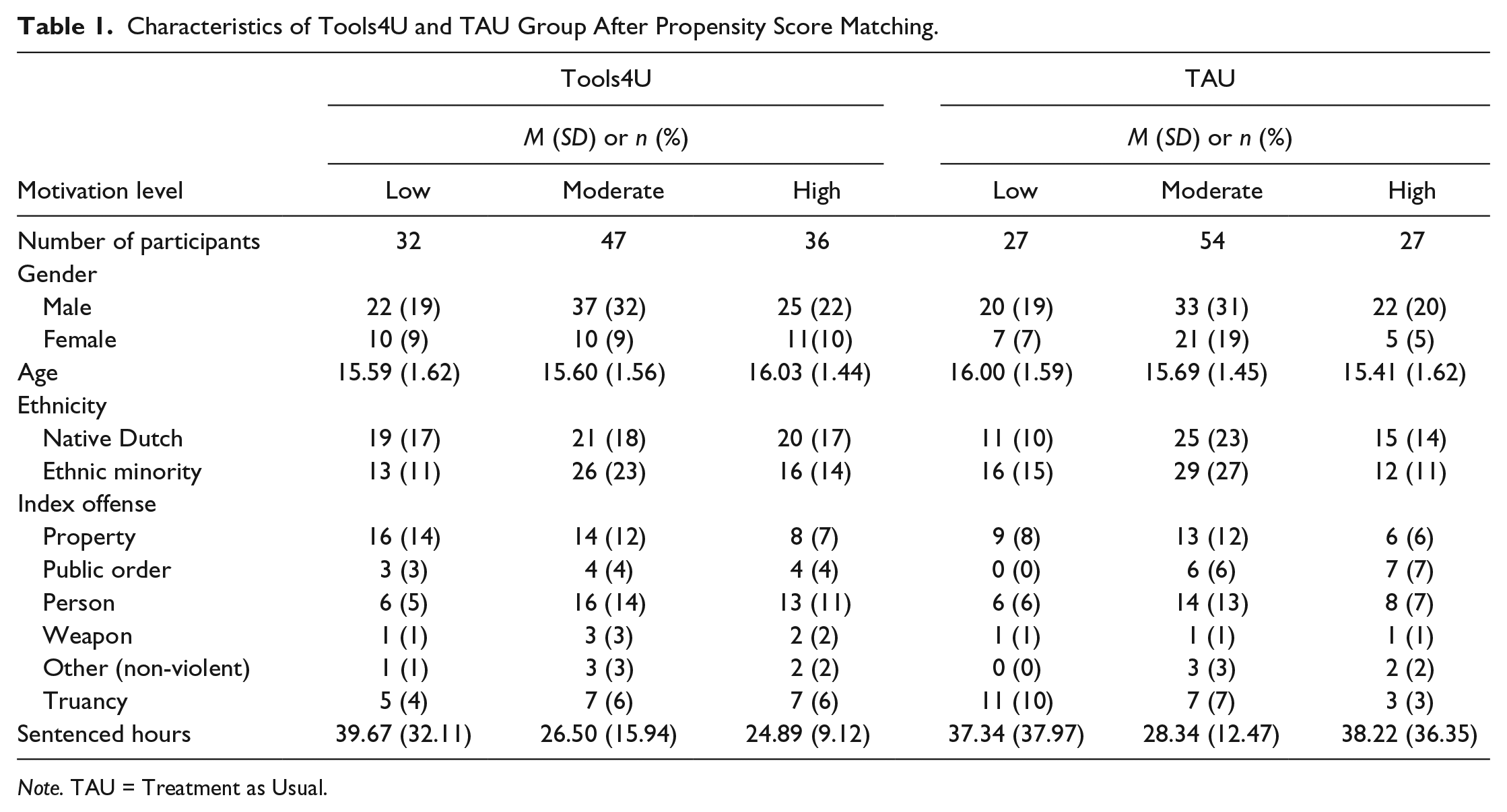
Note. TAU = Treatment as Usual.
Setting and Inclusion Criteria
The treatment group consisted of juveniles who attended Tools4U training in The Netherlands starting between May and August 2012. The control group was recruited among juveniles with a community service order or another behavioral training order similar to Tools4U in duration and intensity (TAU), starting between June 2013 and February 2014. For the effectiveness analyses, n = 108 control group juveniles (of total N = 354) were matched to the Tools4U juveniles (N = 115) by means of a propensity score.
Questionnaires about social skills and treatment integrity were administered to juveniles, parents, and trainers immediately after the first and last meeting of treatment. Juveniles received a 15 euro gift certificate for completing two assessments, whereas the parent received a 7.50 euro gift certificate for the assessments.
Matching Procedure
A comparison group was derived from the N = 354 control group juveniles by means of propensity score matching. To ensure that every juvenile could be included in the matching procedure, missing values at pretest were imputed using the expectation maximization algorithm (Graham, 2009). The propensity score was calculated for every juvenile based on gender, age, ethnicity, and all (non-overlapping) pretest outcome scales (self-perception and parenting excluded). Using a conventional caliper of .025 (Beal & Kupzyk, 2014), 108 control group juveniles could be matched to the 115 Tools4U juveniles. After matching, the missing values at posttest were imputed as well using the same approach.
After the matching procedure, differences between the Tools4U and control group were found in urbanity (χ 2 = 20.52, p = <.001), time between pre- and posttest (Tools4U M = 11.20, SD = 4.80; TAU M = 13.80, SD = 8.30; t = −2.53, p = .012), and self-perception of behavioral adjustment (t = −1.99, p = .048). There were no differences on any of the other characteristics, treatment motivation, and other outcome measures. All analyses were controlled for pretest differences between Tools4U and comparison group.
Treatment Conditions
SST Tools4U
Juveniles in the treatment group received Tools4U, an outpatient individual SST imposed as a (penal) sanction for juvenile delinquents (Albrecht & Spanjaard, 2011). The training is intended for delinquent juveniles (12 to 18 years old) for whom lack of cognitive and social skills is related to delinquent behavior. There are different Tools4U versions: the regular (individual) version (eight meetings), an extended version (12 meetings), and the plus-version, which trains parents in parental monitoring and problem solving (additional: two parent-only meetings and two combined parent–juvenile meetings).
The intervention uses techniques based on operant conditioning, cognitive and social learning theories, the self-management model, and the social interaction model (Albrecht & Spanjaard, 2011). Investigation of inclusion criteria and treatment integrity in the current study showed that inclusion and treatment integrity were sufficient according to the 60% standard of Durlak and DuPre (2008).
TAU
Control group juveniles received any suitable treatment other than Tools4U. The vast majority (n = 102, 94%) received a community service order, meaning that a juvenile is assigned to a work place to do voluntary work for the sentenced amount of hours under supervision of a community service coordination officer. Alternatively, juveniles received another behavioral training sentence (n = 6, 6%) with hours and training intensity similar to Tools4U, that is, an individual aggression regulation training (n = 5, 5%) or individual substance abuse training (n = 1, 1%).
Dropout and Attrition
Despite extensive tracing efforts, some juveniles were lost to postintervention assessment. These juveniles did not differ from juveniles who did complete the second assessment based on gender, age, education level, living situation, modality, offense, and being a first offender. There were, however, more treatment non-completers among the juveniles without posttest (Tools4U: χ 2 = 27.85, p = <.001; TAU: χ2 = 16.27, p = .043). In addition, control group juveniles were more often ethnic minority youth (χ2 = 9.37, p = .002), more often from urban cities (χ2 = 4.00, p = .045), had more sentenced hours (t = −2.15, p = .033), and differed according to juvenile justice region (χ2 = 27.66, p = .001).
Outcomes and Measures
Consistent with the aims of Tools4U, we measured skill deficits related to delinquency (impulsivity, lack of social problem-solving skills, lack of social perspective-taking, and a lack of critical reasoning), developmental task-related skills, and positive parenting behavior. These outcomes and the measures used to investigate treatment motivation are described below. A zero-order correlation matrix of associations between treatment motivation and the other outcome measures is presented in Table 2.
Zero-Order Correlation Matrix of Treatment Motivation and Outcome Measures.
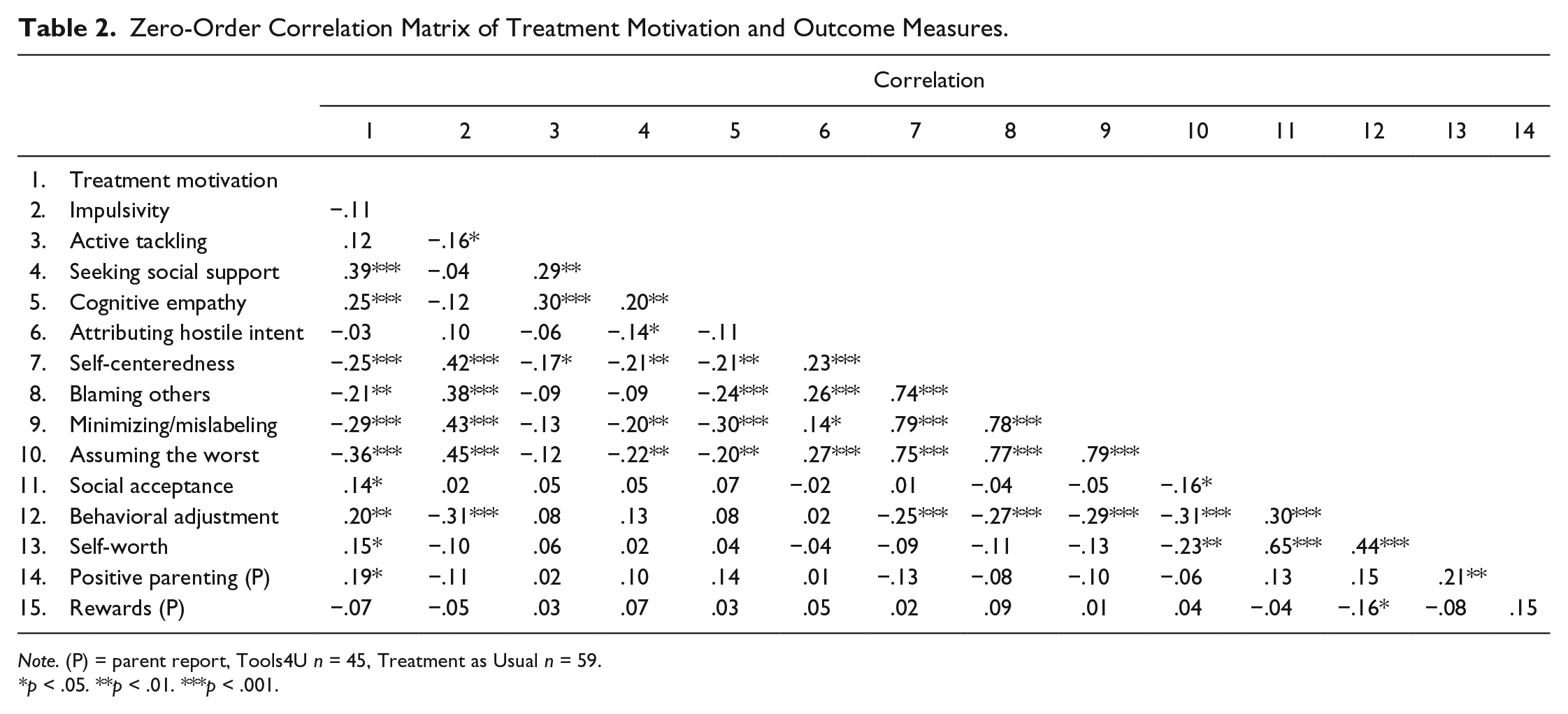
Note. (P) = parent report, Tools4U n = 45, Treatment as Usual n = 59.
p < .05. **p < .01. ***p < .001.
Treatment motivation
Treatment motivation was assessed with a shortened version of the Motivation for Treatment Questionnaire (Van Binsbergen, 2003). This questionnaire consists of 12 items about treatment motivation, which can be answered on a 3-point scale ranging from 0 = not true to 2 = true. This list originally measured four phases of treatment motivation according to the model of Prochaska and DiClemente (1994): precontemplation, contemplation, decision-making, and active change. In the present study, the separate scales for these phases provided insufficient reliability, and in line with a recent study (Van der Helm, Wissink, De Jongh, & Stams, 2013), a one-factor solution provided a better fit. We therefore recoded the items representing Phase 1 and Phase 2 to score the entire questionnaire on the degree of motivation. Cronbach’s α’s were α T1 = .56 and α T2 = .59.
Impulsivity
Impulsivity was measured using the Impulsivity subscale of the Antisocial Process Screening Device (APSD; Frick & Hare, 2001; Van Vugt et al., 2012). The five 4-point items of the Impulsivity subscale range from 0 = not at all to 3 = definitely true and Cronbach’s α’s were α T1 = .70 and α T2 = .66.
Social problem-solving
Social problem-solving skills were measured through assessment of pro-social coping styles. The subscales seeking social support (α T1 = .83; α T2 = .82) and active tackling (i.e., actively addressing problems; α T1 = .77; α T2 = .76) of the shortened version of the Utrechtse Coping Lijst (UCL; Schreurs, Van de Willige, Brosschot, Tellegen, & Graus, 1993; short version, Van den Akker, Buntinx, Metsemakers, & Knottnerus, 2000) were used. For these scales, eight items had to be answered on a 4-point Likert scale ranging from 0 = rarely or never applies to 3 = very often applies.
Social perspective-taking
Information on social perspective-taking was collected by measuring hostile intent attribution and cognitive empathy. To measure hostile intent attribution, the Hostile Intent subscale of the Social Information Processing and Emotional Response Questionnaire Short Version (SIP-AEQ; Coccaro, Noblett, & McCloskey, 2009) was used. The SIP-AEQ consists of vignettes about social situations with direct or relational aggression. Three vignettes were used in the present study. For every situation, juveniles could indicate on a 4-point scale how likely or unlikely (1 = very unlikely, 4 = very likely) they thought different motivations for the situation behaviors were. Because the two scales of hostile intent, direct and indirect hostile intent, separately proved to be unreliable, it was decided to group them under one overarching scale of hostile intent (α T1 = .77; α T2 = .81).
To measure empathy, juveniles were asked to fill out the Basic Empathy Scale (BES; Jolliffe & Farrington, 2006; Van Langen, Stams, & Wissink, 2012). This 20-item questionnaire with a 5-point scale ranging from 1 = strongly disagree to 5 = strongly agree measures both cognitive and affective empathy, but only cognitive empathy (i.e., understanding how the other feels; α T1 = .73; α T2 = .65) was used.
Lack of critical reasoning
Various cognitive distortions were measured using the How I Think Questionnaire (HIT; Gibbs, Barriga, & Potter, 2001; Nas, Brugman, & Koops, 2008). The HIT consists of 54 items that can be answered on a 6-point scale ranging from 1 = strongly disagree to 6 = strongly agree. The following cognitive distortions were assessed: self-centeredness (α T1 = .79; α T2 = .83), blaming others (α T1 = .75; α T2 = .78), minimizing/mislabeling (α T1 = .80; α T2 = .83), and assuming the worst (α T1 = .79; α T2 = .80).
Developmental task-related skills
Developmental task-related skills were measured using the self-perception profile for adolescents ([Competentie Belevingsschaal voor Adolescenten], CBSA; Treffers et al., 2002). CBSA items consist of two sentences: Juveniles first have to determine which sentence is most applicable to them and then choose whether this sentence is a little, or completely true for them. The 20 items assessing social acceptance (α T1 = .68; α T2 = .64), behavioral adjustment (α T1 = .73; α T2 = .76), and self-worth (α T1 = .76; α T2 = .74) were used.
Parenting skills
The Abbreviated Scale for Parenting Behavior ([Verkorte Schaal Opvoedersgedrag], VSOG; Vermulst, Kroes, De Meyer, Van Leeuwen, & Veerman, 2011) consists of 25 items with a 5-point scale ranging from 0 = almost never to 4 = almost always measuring positive parenting, rule setting, punishing, harsh punishment, and rewards. As Tools4U aims at improving positive parenting behavior, only the subscales for positive parenting and rewards were used. Cronbach’s alpha’s were α T1 = .64 and α T2 = .84 for positive parenting, and α T1 = .79 and α T2 = .74 for rewards.
Analytic Strategy
In the previous study, analyses of covariance (ANCOVAs) were conducted to examine overall effects of Tools4U on all outcomes (Van der Stouwe et al., 2016). For the present study, correlations between treatment motivation and Tools4U outcomes were analyzed first to determine dependence of motivation with the other outcomes at baseline. Then, the same ANCOVAs were performed, adding treatment motivation as a factor to test whether treatment motivation is a predictor and/or moderator of Tools4U outcomes.
Because treatment motivation was measured both at pre- and posttest, but showed no significant treatment effects nor significant differences between pre- and posttest for all juveniles, we decided to average the two measures into one measure of general treatment motivation. The sample was divided in a group of “low,” “moderate,” and “high” treatment motivation, using the lowest quartile of the scores to indicate “low treatment motivation” and the highest quartile of the scores to indicate “high treatment motivation” (see, for example, Wootton, Frick, Shelton, & Silverthorn, 1997). The remaining juveniles with scores above the lowest and under the highest quartile were considered the “moderate treatment motivation” group. A similar number of participants per treatment condition were in the separate motivation level groups (Tools4U, low n = 32, moderate n = 47, high n = 36; TAU, low n = 27, moderate n = 54, high n = 27). There were no significant differences in distribution of “low,” “moderate,” and “high” scoring juveniles between Tools4U and TAU for treatment motivation.
Each analysis examined the main effects of treatment motivation and the interaction effects of Treatment Motivation × Condition. As advised by several scholars (Kraemer et al., 2002; Supplee, Kelly, MacKinnon, & Barofsky, 2013; Wang, Lagakos, Ware, Hunter, & Drazen, 2007), a significant interaction effect indicates that treatment motivation is a moderator, whereas a significant main effect without a significant interaction effect indicates that treatment motivation is a predictor.
When treatment motivation was determined to be a moderator for a specific outcome, post hoc analyses were conducted by splitting the file according to motivation level and again conducting an ANCOVA. These analyses yielded effect sizes indicating the improvement in the Tools4U group relative to the control group for each level of treatment motivation separately. When treatment motivation was determined to be a predictor for a specific outcome, post hoc analyses were conducted by conducting an ANCOVA with only treatment motivation and not treatment condition as a factor.
Results
Preliminary Analyses
Correlations between treatment motivation and Tool4U outcomes
Table 2 shows that treatment motivation was negatively related to a lack of critical reasoning (self-centeredness, blaming others, minimizing/mislabeling, and assuming the worst). Furthermore, treatment motivation was positively related to seeking social support, cognitive empathy, social acceptance, behavioral adjustment, self-worth, and positive parenting. Finally, treatment motivation was unrelated to impulsivity, active tackling (i.e., actively addressing problems), hostile intent attribution, and parental rewarding.
Testing Hypotheses
Treatment motivation as a predictor and moderator of Tools4U effects
Table 3 summarizes analyses for predictive and moderating effects of treatment motivation. Only one moderating effect was found on active tackling. Furthermore, four predictive effects were found for seeking social support, cognitive empathy, attributing hostile intent, and self-centeredness. No moderator or predictor effects were found for the remaining nine of 14 outcome measures.
Treatment Motivation as Predictor and Moderator of Tools4U Treatment Effects.
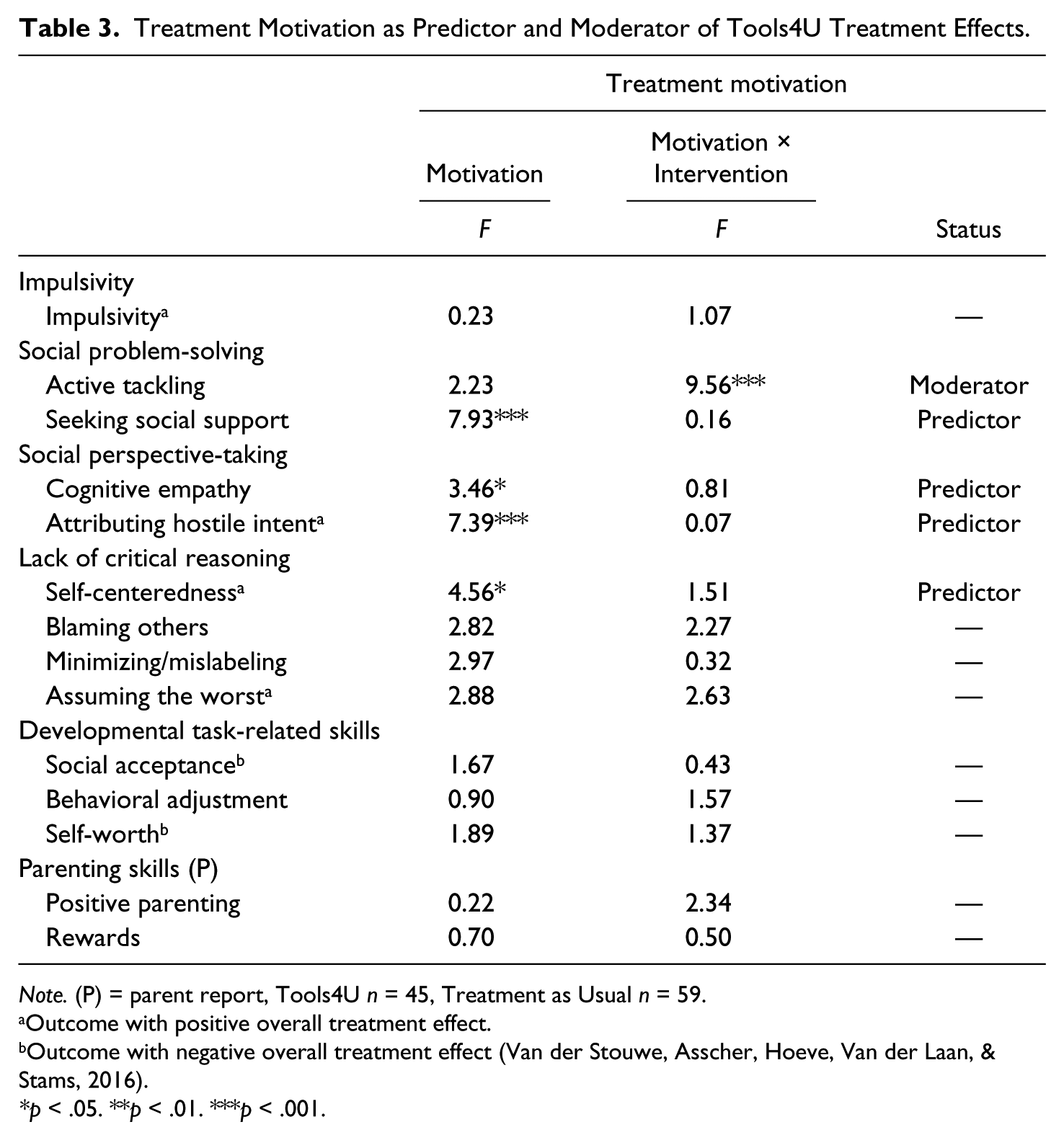
Note. (P) = parent report, Tools4U n = 45, Treatment as Usual n = 59.
Outcome with positive overall treatment effect.
Outcome with negative overall treatment effect (Van der Stouwe, Asscher, Hoeve, Van der Laan, & Stams, 2016).
p < .05. **p < .01. ***p < .001.
Post hoc analyses predictor and moderator effects
Post hoc analyses were conducted to further examine the moderating effects of treatment motivation for active tackling. It can be derived from Table 4 that juveniles with high treatment motivation showed no Tools4U treatment effects on active tackling, whereas only juveniles with moderate treatment motivation showed significantly more active tackling after Tools4U compared with TAU. In contrast, juveniles with low treatment motivation showed more active tackling after TAU compared with Tools4U.
Means and Standard Deviations for the Moderator and Predictor Effects.
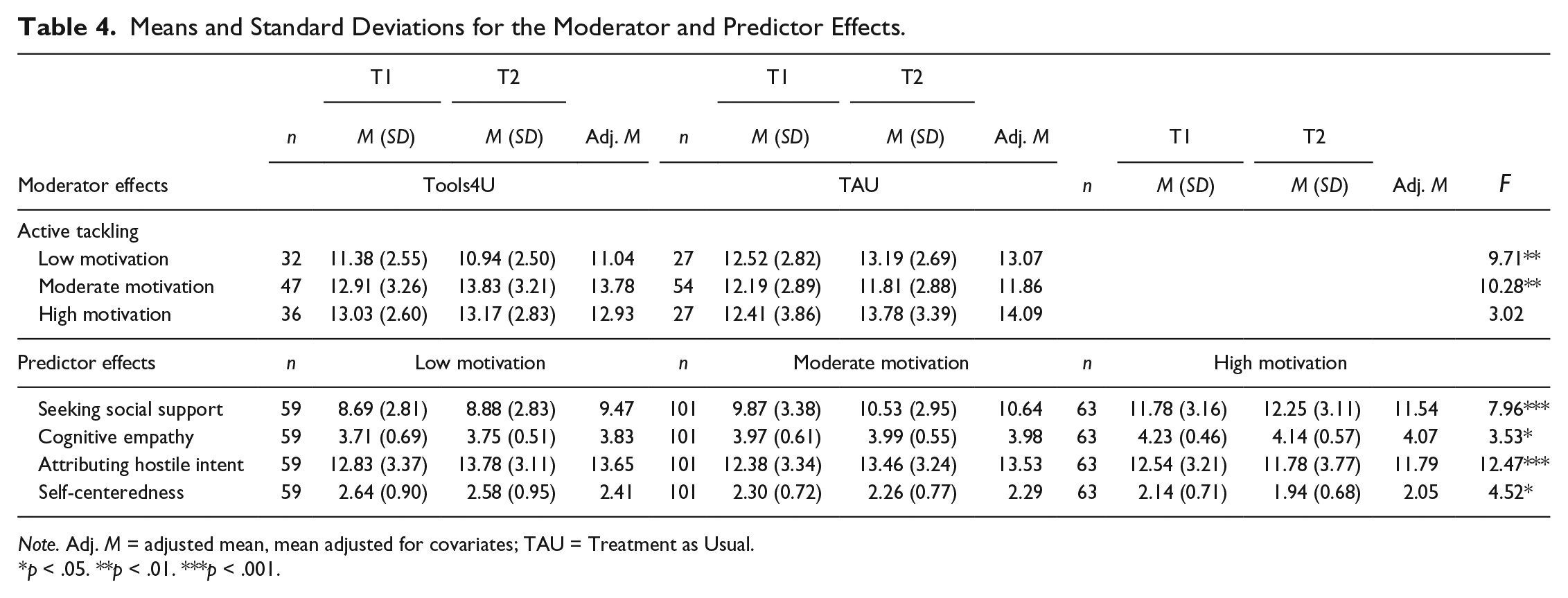
Note. Adj. M = adjusted mean, mean adjusted for covariates; TAU = Treatment as Usual.
p < .05. **p < .01. ***p < .001.
In addition, post hoc analyses were conducted for outcomes on which treatment motivation had a predictive effect. Table 4 shows that highly motivated juveniles showed larger improvements on seeking social support, cognitive empathy, attributing hostile intent, and being self-centered, regardless of treatment condition.
Discussion
The present study expanded existing research on juvenile delinquency treatment by investigating treatment motivation as a moderator and predictor of SST training effects. Treatment motivation had a moderating effect on just one outcome, and a predictive effect on only four out of 14 outcomes. Treatment motivation had a moderating effect on active tackling (i.e., actively addressing problems). Only juveniles with moderate treatment motivation showed more active tackling after Tools4U than after TAU, whereas juveniles with low treatment motivation showed less active tackling after Tools4U than after TAU. For highly motivated juveniles, there were no significant treatment effects. Furthermore, treatment motivation was predictive of seeking social support, cognitive empathy, hostile intent attribution, and self-centeredness. That is, for all these outcomes juveniles with higher motivation showed better results after treatment, regardless of treatment condition.
Interestingly, treatment motivation had no moderating effects on any other outcome. Neither on outcomes on which Tools4U showed significant overall treatment effects (i.e., impulsivity, assuming the worst, social acceptance, and self-worth) nor on outcomes without significant treatment effects. Consequently, this could indicate that Tools4U is appropriately tailored to individual levels of treatment motivation to facilitate treatment changes, as the degree of motivation did not differentiate the outcomes (for impulsivity, assuming the worst, social acceptance, and self-worth). In addition, the present outcomes indicate that a lack of treatment effects on the other outcomes could not be explained by (a lack of) treatment motivation. Alternatively, the lack of predictive and moderating effects could be attributed to homogeneity of treatment motivation in the Tools4U target population. Tools4U will only be imposed when the juvenile is expected to be willing to participate in the training, which implies a certain degree of motivation for treatment. On the other hand, the compulsory nature of the present intervention could have limited intrinsic motivation. The moderately severe adolescent onset delinquents in the current study might therefore all show moderate treatment motivation with extremes (i.e., low/high motivation) not extreme enough to be of clinical relevance.
The only outcome that showed treatment effects when taking treatment motivation into account is social problem-solving skill active tackling. First, highly motivated juveniles showed no significant treatment effects on active tackling, which is in line with Prochaska and DiClemente’s (1994) motivational phasing. That is, their highest motivational phase is that of “active change,” which already implies a certain amount of active tackling. It is therefore not surprising that an increase of active tackling could not be achieved for the group of highly motivated juveniles. However, treatment motivation and active tackling were unrelated at pretest, which is not in line with existing research (Raftery et al., 2010; Van der Helm et al., 2014), and does leave some questions unanswered. In line with the context of change model (Burrowes & Needs, 2009), the present results could indicate that with higher treatment motivation (individual factor), the content of treatment (catalyst) becomes less important, suggesting that mandatory treatment in general, and not the specific treatment provided, would lead to behavioral change for these juveniles.
Second, the least motivated juveniles showed more active tackling after TAU than after Tools4U. This could indicate that a lack of treatment motivation leads to specific resistance to therapeutic treatment (such as Tools4U), which in turn leads to more passive problem-solving, while a non-therapeutic, behavioral setting (such as the present TAU) does (covertly) stimulate juveniles to confront their own problems more actively. Finally, only moderately motivated juveniles showed treatment effects of Tools4U. For these juveniles, Tools4U does appear to act as the previously mentioned catalyst of change (see Burrowes & Needs, 2009). Alternatively, assuming that treatment needs to be tailored to the juveniles’ motivational phase (O’Hare, 1996; Prochaska et al., 1992; Snyder & Anderson, 2009), we argue that Tools4U may not be cognition-oriented enough to motivate precontemplators and contemplators for (active) change, and not behavior-oriented enough to substantially aid juveniles in the active change phase with their behavioral change. Its cognitive-behavioral approach would then be best suited for moderately motivated, decision-making-phase juveniles. Moreover, looking at the other outcome measures, active tackling might be the most behaviorally oriented outcome, thus reflecting active change most directly. However, the lack of influence of treatment motivation on other outcomes does not substantiate this view, and further research is needed to explore the appropriate matching of treatment techniques to motivational phases and treatment effects. It can be concluded juveniles need to be at least somewhat motivated for treatment for Tools4U to be effective in improving active tackling.
Treatment motivation was predictive of positive changes in social support seeking, cognitive empathy, hostile intent attribution, and self-centeredness. Juveniles with the lowest treatment motivation showed the least improvement on these outcomes, whereas juveniles with the highest treatment motivation showed the most improvement on these outcomes. This, again, could indicate less specific requirements for the aforementioned catalyst with higher treatment motivation. Furthermore, the compulsory nature of treatment (regardless of type) could increase juveniles’ awareness of their problems and thus increase (perceived) problem severity. This increased (perceived) problem severity could in turn increase treatment motivation, as is in line with existing literature (DiGiuseppe et al., 1996; Englebrecht et al., 2008; Leenarts et al., 2013; Phares & Danforth, 1994; Rosenkranz et al., 2012). Interestingly, Tool4U showed significant treatment effects for hostile intent attribution and self-centeredness, but there was no interaction effect between treatment condition and treatment motivation. That is, Tools4U was just as effective in decreasing hostile intent attribution and self-centeredness for juveniles with different levels of treatment motivation, while treatment motivation alone also predicted these outcomes. Moreover, different levels of treatment motivation could not explain a lack of overall treatment effects of Tools4U on the other measured component of social perspective-taking, that is, cognitive empathy, which could be considered a closer fit to this construct than hostile intent attribution.
Although this study has several methodological strengths (adequate treatment integrity, and assessment of both the predictive and moderating role of treatment motivation in an outpatient juveniles offender treatment setting), some limitations need to be mentioned. First, Cronbach’s α for the current motivation for treatment questionnaire could be considered low (<.60, Bijleveld, 2009), which means the present outcomes should be interpreted with caution. However, this relatively low reliability is not surprising given the multidimensionality of the construct of treatment motivation, which has led to questionable reliability and validity in measures of treatment motivation in general (Burrowes & Needs, 2009). Moreover, as reliability is highly dependent on the homogeneity of the construct under investigation, a reliability of >.50 would be sufficient, particularly for research purposes (Streiner, 2003). Second, the effects for the low and high treatment motivation groups were calculated on a smaller sample than for the moderate treatment motivation group, with even smaller groups for the parenting outcomes, which reduced the power to detect significant treatment effects. Third, we relied on sample-specific distributions of treatment motivation to determine low and high motivation groups, which may have limited generalizability. Fourth, the interaction of treatment motivation with other factors (e.g., gender, age) could not be investigated because of an insufficient number of participants. Fifth, because treatment motivation was only measured twice, simultaneously with the Tools4U outcomes, mediator effects of treatment motivation could not be examined. This has limited full exploration of the influence of treatment motivation on Tools4U treatment outcomes (e.g., Bonell et al., 2012; MacKinnon, 2011). Finally, based on the current study, no statements can be made about the influence of treatment motivation on Tools4U treatment effects on long-term and/or delinquency outcomes. Additional studies including long-term (recidivism) data are therefore needed to make a definite statement on the effectiveness of Tools4U and the influence of treatment motivation on the effects.
To our knowledge, the present study is the first to examine treatment motivation effects on outpatient juvenile offender treatment effects, and specifically for an SST. Taken together, the current study indicated that Tools4U treatment effects are mostly consistent across juveniles with different levels of treatment motivation. Only a lack of improvement in social problem solving could be explained by different levels of treatment motivation. Future research is needed to examine the appropriate matching of treatment techniques to motivational phases in relation to treatment effects. Moreover, future studies should investigate and refine the complex interaction of treatment motivation with other individual and environment factors (as suggested by Burrowes & Needs, 2009) and treatment changes for outpatient juvenile offender treatment specifically.
Footnotes
Acknowledgements
We would like to thank the WODC supervisory committee members for their valuable input and support with this project. Also, special thanks to the people at the Child Protection Council, the Tools4U trainers, and community service coordination officers for their support and cooperation. Finally, sincerest gratitude to all juveniles and parents who participated in this study. Without them, this study could not have been completed.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current study was funded by The Research and Documentation Centre of the Dutch Ministry of Justice (WODC).