
Abstract
Digital data are increasingly framed as essential resources in health and medicine, implicating diverse actors who work to transform them into different forms of value. In this article we focus on the diverse and contingent valuation practices that shaped an artificial intelligence-enabled ‘smart’ health technology and the data it generated at different moments in time, and the corresponding asset forms that were envisioned, developed, tested, and marketed. We also outline the role of assetization as a contested but essential design and marketing activity, and introduce the notion of proxy work as an intermediary between data generation and assetization, where people, infrastructures, and other material devices are arranged in such a way that data become capable of ‘standing in’ for something else, allowing accountable forms of value to be realized across multiple sites. We conclude with a discussion of the consequences of assetization as a dominant lens through which governments, firms, and other actors increasingly understand the value of digital health data, and the different health-related futures those practices make possible.
Digital health data sit at the nexus of multiple health care promises, policies, and priorities. These are more recent developments in the history of organized health systems, supported by the privilege of positivist epistemologies, expanding digital infrastructures, and popular imaginaries that increasingly approach data as essential to contemporary health systems (Chin-Yee & Upshur, 2019; Geiger & Gross, 2021; Hoeyer, 2023). Today, diverse actors work to transform data into different forms of value, which vary by jurisdiction but share many similar objectives, including enabling operational efficiency, improving clinical outcomes, and driving economic growth (Faulkner-Gurstein & Wyatt, 2023; Reutter & Åm, 2024; Vezyridis & Timmons, 2021). Corporate and financial actors are essential to these developments, providing infrastructures upon which data architectures can be built, and creating new technologies and services that shape digital health economies more broadly.
A variety of perspectives in the social sciences and humanities have been employed to make sense of these developments, particularly within the interdisciplinary fields of critical data studies and Science and Technology Studies (STS). Contributions focused on surveillance, for example, have emphasized the social sorting functions of data, including how processes of division and control have become dominant business models in their own right (Cinnamon, 2017; Zuboff, 2019). In health care, these models are often associated with efforts to promote self-management or personalization (Prainsack, 2020). Others have approached these developments as extensions of colonialism, emphasizing the extractivist and dispossessive characteristics of digital expansionism, both as unique phenomena (Couldry & Mejias, 2019; Ozalp et al., 2022) and in the context of longer legacies of colonial knowledge and power that act upon the body in new but familiar ways (Gray, 2023). Finally, some scholars focus specifically on ‘Big Tech’ and corporate monopolization in the wake of the dot-com bubble and subsequent global financial crisis, examining exactly what forms of value are at play. Sharon (2018), for example, outlines the multiple and sometimes competing orders of worth characterizing Big Tech’s involvement in health care beyond a simplistic focus on ‘market’ value, including civic, vitalist, and industrial logics. What is clear across all of these approaches, however, is that digital health data are different from other kinds of information (Birch, 2023; Hoeyer, 2023), and figure prominently in the activities and promises of a growing number of actors, from Big Tech to supra-national governments (Marelli et al., 2023). New theoretical and methodological approaches are therefore an important part of understanding their actual significance for broader health systems.
In this article we approach this task by engaging with and extending perspectives from science and technology studies, social studies of finance, and critical design studies to describe some of the challenges associated with generating viable data assets from an academic spin-off technology undergoing commercialization through a start-up. In particular, we focus on the diverse and contingent valuation practices that shaped the ‘smart’ health technology and the data it generated at different moments in time, and the corresponding asset forms that were envisioned, developed, tested, and marketed. We also reflect on the role of assetization itself as a contested but essential design and marketing activity, and outline the importance of proxy work, which involves the translation of digital health data into assets through value-laden practices of ‘standing in’ for something else. We then conclude with a review of the implications of these findings for broader health data assetization efforts, asking what kinds of health systems they rely on to succeed. Of particular relevance to our discussion is the suitability of health data assets for shared prosperity and collective governance, and the role of proxy work in generating different answers to this question. To summarize, the objectives of this article are as follows:
To describe the styles of valuation that characterized the development of an AI-enabled smart technology for health care, and the different uses of digital health data that resulted from it.
To outline the techniques, infrastructures, and other material devices implicated in the sociomaterial enclosure of evolving health data assets.
To illustrate the value of assetization itself as a contested but essential design and marketing activity.
Approaching assetization and valuation in digital health
Scholarship in STS, including social studies of finance, valuation studies, and constructivist political economy have explored how forms like ‘data’ are turned into something that can be owned or controlled (Birch & Muniesa, 2020; Mallard & Callon, 2022). These contributions emphasize that digital data and resulting relations of commercial and non-commercial exchange are made, performed, or enacted through diverse ideas, expectations, and collections of material devices that are significant for different actors in different ways at different moments in time (Chandrashekeran & Keele, 2022).
In particular, we engage with assetization in our empirical case, which entails a focus on practices that involve owning, controlling, trading, or capitalizing data as future revenue streams (Birch & Muniesa, 2020). Data assetization reflects both a conceptual approach and empirical observation that data are increasingly central to the business and financial strategies of modern firms across different domains (Birch & Ward, 2022), from agriculture (Hackfort et al., 2024; Sippel, 2023) to genomics (Geiger & Gross, 2021). Assetization represents a unique focal point in that assets are non-fungible (unique), non-rival (inexhaustible), and made to keep, meaning legal contracts entitle owners to extract value from the control of data potentially ad infinitum, rather than generating profits from the production or sale of a good itself, although this may also sometimes be the case (Birch & Ward, 2023). Assetization therefore relies on a variety of practices (e.g., data cleaning), priorities (e.g., investor expectations), and infrastructures (e.g., intellectual property laws), that allow an asset to fulfil its future-oriented obligations across different sites.
This focus on processes and practices of making health data into assets invites consideration of what they are meant to do, and who they are meant to serve. In this sense, valuation is essential to assetization (Birch, 2017; Doganova & Muniesa, 2015). Valuation reflects the position that value is performed through activities of worth attribution, in which something is selected, assessed, and made valuable, rather than being latent in a thing itself (Birch, 2017; Chiapello, 2015; Helgesson & Muniesa, 2014). In relation to assetization, valuation especially describes practices of creating or enclosing accountable forms of future financial value that allow something to be owned, controlled, traded, or capitalized. Often, multiple styles or logics of valuation are present simultaneously (Boltanski & Thévenot, 2006; Lee & Helgesson, 2020; Sharon, 2018), corresponding to different potential asset forms that require resolution in practices of design and market-making, highlighting the politics of different asset forms and the often empirically observable actors, objects, infrastructures, and governance practices they rely on (Ouma, 2024; Pallesen, 2015).
To clarify, by markets we do not mean natural phenomena guided by the interests and actions of rational agents. Rather, in line with our approach to valuation, we adopt the perspective of markets as sociotechnical ‘agencements’ (Çalışkan & Callon, 2010; Callon, 2008, 2021), or heterogenous assemblages where multiple forms of organization enact effects through networks that can be comprised of normative expectations, regulations, technology transfer offices, hardware, software, standards, business models, and more (Geiger & Bourgeron, 2023; Komljenovic & Robertson, 2016). More specifically, we engage with markets through the observation that practices of design, marketing, and market-making are reciprocal and co-constitutive (Araujo, 2007; Callon, 2016), pointing to relationships that are oriented toward generating transactions of some kind that generate certain forms of value for certain people. This often relies on the work of developers and engineers, but also implicates CEOs, policymakers, accountants, financiers, and the technical infrastructures that make different forms of value recognizable and commercially viable. The people, practices, and things implicated in the creation and sustainment of new and emerging health data markets is not only significant for understanding the practices of commercial enterprises, but also governments seeking to establish new market frontiers, such as the European Health Data Space Regulation and broader European Strategy for Data (European Commission, 2024).
Taken together, the more basic point we wish to advance in this section and in the empirical work that follows is that the enclosure of different forms of accountable value relies on practices of translation, which allow those forms of value to be pursued, claimed, and realized across multiple sites (Fochler, 2016; Sharon, 2018). With respect to digital data, we suggest that these processes of translation involve ‘proxy work’ (Mulvin, 2021), where people, infrastructures, and other material devices (e.g. patents, users, risk scores, data labels) are arranged in such a way that data become capable of ‘standing in’ for something else. The resulting assets are durable, but can be contested by new practices of valuation and new kinds of proxy work, as we see in our own case. Assets and the proxies they rely upon may also overflow their boundaries, giving rise to new arrangements that reflexively shape data valuation practices themselves (Figure 1). Assets are not merely passive phenomena, but actively shape the means by which they are governed, and the incentives and priorities that characterize the recognition of a resource (such as data) as having certain kinds of ‘value’ in the first place (Birch, 2024).
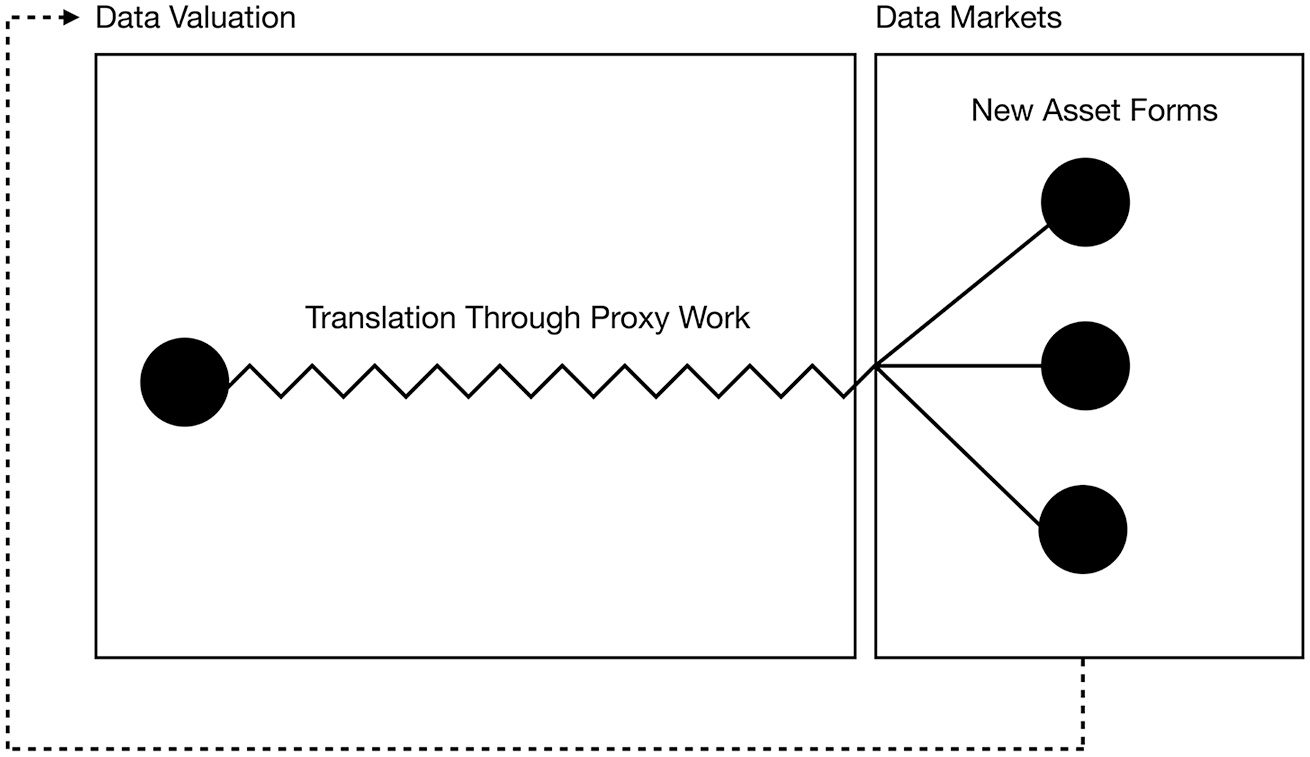
Making (health) data markets: Assetization, valuation, and proxy work.
Empirical case and methods
Digital health technologies originating in academic settings bring together scientific practices, clinical logics, and other parts of the health innovation ecosystem to produce different forms of value for different kinds of actors (Pinel, 2021). Our own case focuses on the development of an AI-enabled smart health technology undergoing commercialization through a start-up at a publicly funded academic health sciences centre. Like academic hospitals in many regions of the world, significant investments have been made to support of commercialization of scientific research, making these hospitals and research centres especially well-suited to studying practices of health data assetization and their consequences.
The specific technology that forms the empirical focus of this article is a commercial-grade smart watch employing supervised machine learning for the classification and monitoring of physical therapy exercises for shoulder injuries. The team of clinicians and engineers who developed the technology did so in response to widely reported deficits in patient performance of prescribed physiotherapy exercises at home. Accurately measuring at-home physiotherapy participation therefore promised a better understanding of predictors of at-home physiotherapy adherence, impacts of adherence on recovery, and potential barriers to effective home physiotherapy engagement. The development of the technology was initially funded by academic research grants. One such grant supported a collaboration between researchers with expertise in ethics and policy, and the development team, which produced the work described in this article (ethics approval #2020-0132-E). A commercial version of the technology was subsequently developed and marketed through a spin-off company created specifically for the technology, which was also funded by private sources.
Data collection for this project involved focus groups, qualitative interviews, and document review. Four focus groups were conducted: two sessions with physiotherapists familiar with the technology, and two sessions with patients who had used prototypes of the technology. Twenty-four interviews were also conducted with diverse actors, including the development and commercialization team, patients using prototypes of the technology, a physiotherapist who had used the technology with patients, health systems experts, policymakers, and technology ethicists. Documents included design briefs, blueprints, prototypes, and government policies pertaining to personal data, health information, and artificial intelligence (AI).
In the following sections, through three parts, we describe how the technology and its ‘data products’ progressed, each associated with distinct styles of valuation. In doing so we draw attention to contingent and contested moments through which the technology became a portfolio of evolving asset forms (Rushforth et al., 2019), each tied to different market ideals, world making practices, and health-related futures.
A portfolio of evolving assets: Health data valuation in three parts
Part 1: Innovating the future of care
Digital technologies play an increasingly important role in academic knowledge production, where AI, smart devices, sensors, and other software and hardware can be mobilized in pursuit of different goals (Delvenne et al., 2023; Falkenberg & Fochler, 2024; Lee & Helgesson, 2020; Pinel, 2021). The technology that became the focus of this particular case originated in doctoral coursework and eventually formed part of a dissertation in the biomedical sciences. As a trained MD/PhD, Daniel, the student-turned-investigator/founder noted that smart technologies and inertial sensors were increasingly used to address clinical problems, and one of the problems he regularly encountered in clinical practice was sub-standard performance of at-home physiotherapy exercises. Often, patients who did not complete their physiotherapy exercises frequently or effectively enough would require more invasive treatments, which were both harmful to the patient and costlier to the health care system. This has led to a system-wide emphasis on compliance, where patients are encouraged in different ways to perform their prescribed exercises, sometimes without success, as Daniel describes here: We were using smart watches in the lab for some other applications, for inertial sensors. There was one of the lab members, [name], a junior scientist who was using inertial sensors for assessing the knee kinematics of athletes who were at risk of or anterior cruciate ligament injury. I had some exposure to that technology and I thought this might be applicable .... It’s widely understood that the quality of treatment that patients receive, due to their own financial circumstances, or their own motivations, or beliefs about the quality of it really varies …. And so, that got me thinking about, what would be a good way to first of all, assess that, but also, to really make sure that patients got the most out of this treatment.
Here, Daniel shares his perspective on the potential value of the technology as a tool to support patients’ existing goals. The need for compliance with treatment regimens, and the perception that the technology could support those aims, represents the approach he brings to the project as a clinician-scientist. Already, we can appreciate the notions of care embedded in these conceptions of clinical value (Mol, 2008), such as the imperative to improve patients’ outcomes using the tools he has available, which represent some of the best his discipline has to offer. The problem informing Daniel’s approach is explicitly conceived of as a clinical challenge solvable by an already available technology, particularly as a more precise evidence-based intervention with the ability to ‘nudge’ patients when needed.
When an initial prototype was determined to be acceptable by research standards, the team applied for funding to clinically validate the technology with patients, eventually winning a grant competition sponsored by a large public insurer. The research team then leveraged that funding to secure additional research funding from a federal agency, while exploring commercialization avenues. As a ‘cutting-edge’ technology, the journey from clinical tool to commercial opportunity was a short one, buoyed by university and hospital translational research policies and resources supporting such efforts. Adam, one of the hospital’s business development executives, reflects on his role within the organization and the metrics used to track his office’s performance: I’d say our metrics really start with invention disclosures that come in, which is when scientists or clinicians or students create new technologies and see potential, and then they file an invention disclosure. That’s kind of a leading indicator of research that may have commercial potential. And then we track our patenting activities, so provisional patents [interim ‘patent pending’ filings] and then through to patent cooperation treaties and national phase filings [international patent filings made in specific countries]. And then at the end of the day, how many of those are issued. So, that’s the assets building stage. And then on the other side … we need that transfer piece … so where we look to actually have the intellectual property leave the institute and be put in the hands of people who are advancing it. So, on that front, we track active engagement. We track term sheets [a nonbinding agreement that sets out basic terms and conditions of an investment]. When we enter that phase of term sheets, we track how many weeks of contracting, and then at the end of the day, how many licensing deals we do … [Hospital name’s] vision or motto is [Innovating the Future of Care]. … We’re an academic institution effectively. We’re funded by the public sector. My feeling is the reason why the government funds things like universities and colleges and research institutions is not because there is some fundamental interest in basic research. It’s because it should have the potential to grow Canada’s economy at the end of the day. So, that’s, I think, a core piece there. If we look at a project that is taken on or a new company that’s formed, those will generally attract investment. It will lead to more job creation and help the Canadian ecosystem grow.
To Adam and others, academic research is a key pillar of economic growth, but practices of scientific production do not always map neatly onto commercial objectives. As such, a significant part of Adam’s day-to-day work involves finding partnerships, offering advice on commercialization pathways, supporting patent filing, and connecting researchers to commercial opportunities. Adam represents a first point of contact in the translation of research products from the lab to the clinic, which involves separate but increasingly overlapping activities in support of broader commercial objectives associated with contemporary biomedicine.
At these earliest phases in the lifecycle of the technology, the inertial data generated by the smartwatch and exercise scores generated by the algorithm were the primary data products, as the team called them. This move from the lab to the clinic impelled the team to think like entrepreneurs rather than investors (Birch & Muniesa, 2020), with a focus on creating mostly clinical value. This had important implications for the sustainability of the business, however, on which Jane, the teams’ strategy and finance consultant, reflects: It definitely is more focused on bringing in data-driven decision-making to physical therapy, right, and I’m sure you’ve heard this pitched many ways. … I think for me it was really surprising to learn that you can do all this research, you have all this data behind it saying, hey, this is actually going to help you, improve you, help you do a better job. And doctors just were like, no, I don’t want that, I know better, even though you can show them all the data in the world.
As Jane suggests, the disentanglement of the technology from a scientific milieu to a clinical one was not a straightforward process. Achieving commercial success would require a translation of clinical and scientific aims into commercial ones, while appealing to potential users. In the context of the transition from lab to patient care, this meant a focus on treatment adherence and data-driven decision-making. These successive translations enrolled a diverse and ever-growing number of actors and interests, each accompanied by competing practices of valuation. As these grew in number, so too did potential conflicts, including over the perceived usefulness of digital data in outpatient physiotherapy practice.
Still, in spite of its longer-term commercial objectives, conflicts at this phase were limited. Data products were primarily academic and aimed at defining an acceptable or desirable clinical outcome or scientific knowledge claim (Fuller, 2019). Accumulation strategies and ownership and control rights were primarily derived from and supportive of academic work, without the need to demonstrate value outside of the clinical encounter or the context of academic knowledge production. The technology does not yet rely on investors or even users to perform its intended functions. IP filings, publications, grants, or other new sources of funding were important primarily in relation to the activity of commercializing the data-generating technology as an outcome itself, in alignment with forms of value associated with contemporary academy (Fochler, 2016), particularly in health and biomedical technology. However, this was only a first step towards future translations, entailing other asset forms and valuations, as the following sections illustrate.
Part 2: From the lab to the clinic
Through the establishment of a start-up the core research group recruited a larger team, comprised of a Chief Executive Officer (CEO) and several other experts from across finance, tech, engineering, and corporate strategy. In this subsequent phase of commercialization, selling the technology directly to individual physiotherapists or patients was determined to be too difficult, and so the team pursued chains of clinics as potential buyers of the technology, as the CEO Ken describes in his outline of the company’s approach: I know from my background that it’s very difficult to identify recently injured patients, or people who have had surgeries, and try to market directly to them in some way, or to try to market to them through things they might be searching for. Some of our competition are now doing that. It’s an extraordinarily large marketing challenge. We will be focusing a lot of our marketing dollars on reaching those clinics, those physiotherapists, and they’re incredibly easy to identify online as a group and be able to be targeting them using social media, other targeted online techniques.
The team considered different approaches, including a ‘freemium’ model, where patients and providers could access certain features of the technology for free with paid upgrades. The team also simultaneously recognized that the potential value of the technology was not strictly clinical or scientific, and a clearer emphasis on its administrative benefits was articulated. This translation of clinical value to administrative value accompanied the team’s pivot in commercialization strategy, which also required a translation of the technology and the data it produced from a scientific product and clinical tool to an enabler of cost-effectiveness and transparency. The commercialization strategy that accompanied this shift also resulted in different data products, as described by one of the team’s commercialization experts: Data comes across, as far as I can tell, three scales. And user testing has revealed that effectively everyone is comfortable sharing all of their data with their care provider like the physiotherapist. We see that being the smallest scale data product. The physiotherapist sees what an individual person is doing and can use that information to inform that person’s treatment. So, the next scale up of that is the one where there is huge quantities of ethics and regulatory concern. And that is when you take individual data that is being fed to a physiotherapist and group that together like via a policy number or some type of larger bidding structure. Maybe they need to have some type of, take some type of action when it comes to Bob’s Wrench company because it turns out that everyone there is not doing their physiotherapy. Something else is going on. You need to have a conversation with Bob and say you need to provide additional time for employees to have their physiotherapy because they need to do this during working hours, no one is any doing physio at home. The next step up is all people just grouped together in what would be a totally de-identified data set. At that point you could then say certain parameters are available for de-identification, so you’re allowed to have age still by year. So, you could say alright, this is the average recovery pathway for a 42-year-old. It just has to be de-identified. So individual data great, that’s probably quite useful to just people on an individual scale. Is it going to be worth any more than a core product which is helping people to do physiotherapy exercises? Probably not.
In this passage, the commercialization expert clearly outlines the three possible data products envisioned for the technology, each of which implicates different ethical and regulatory regimes, data architectures, and valuation practices. For something to be assetized, it must be identified and framed by credible experts so that it can be governed effectively (Birch, 2024). Margaret, the team’s data monetization consultant, is aware of the controversies surrounding different data valuation and assetization practices, and situates these in relation to the task she has been assigned: I'm kind of constantly challenging and thinking through, if I was the consumer of this data or of this product on the corporate side, what is it that I would be looking for and how do we set the product up so that we continue to have trust by the customer and understand what kind of value we can provide to organizations?
While the earliest iterations of the technology exemplified forms of academic entrepreneurialism (i.e., patents, publications, grants, and eventually a spin-off company), subsequent phases brought about competing ideas about how best to produce financial value for more diverse actors, without losing sight of the other forms of value that made the technology desirable to those who were intended to use it. This required freeing the data from their associated milieu (Callon, 2021; Simondon et al., 1980) (in this case, a clinical-scientific one) so that they could become exchangeable while still being functionally useful in a clinical setting. This process of translation must be done in such a way that functionality is preserved, while facilitating a transaction and transfer of rights that commercial exchange requires. These exchanges could pertain to patients (who does or does not complete their exercises?), physiotherapists (whose patients improve faster?), companies (where are people getting injured?), clinics (which clinics perform better than others?), or all of the above. Achieving success this way would require larger actors, more users, more clinics, and more data, however. We elaborate on this below.
Part 3: Plug and play
The significance of large corporate actors in digital health ecosystems has been extensively discussed. These discussions typically focus on ‘Big Tech’ and the implications of monopolistic power and Silicon Valley logics for public health care systems (Anderson et al., 2022; Birch et al., 2021; Birch & Cochrane, 2022; Ozalp et al., 2022; Sharon, 2018). Less frequently examined in empirical work, however, is how the practices of large organizations, Big Tech and otherwise, practically shape the activities and valuation practices of other smaller organizations as they try to make a market for themselves. Generally, these dynamics have been represented in the existing literature in two distinct but complementary ways. First, is the observation that large organizations monopolize a particular arena in order to prevent other players from entering. This is often accomplished through the mobilization of existing resources and infrastructures which would be difficult or impossible to access by other actors in order to make a ‘first move’. Second, larger companies may pursue markets that have been ‘de-risked’ by government, start-ups, or other smaller players (Mazzucato, 2015), by either purchasing those companies, or forming their own divisions that compete with or control other players through ownership or control of essential infrastructure or resources.
Similarly, with respect to our own case, we found that as different commercialization strategies were considered and tested, it became clearer to the team that success through larger-scale adoption would require infrastructure and resources that depended on other, much larger players, as Sam, the co-founder explains: So, it started with physical therapy, it went onto insurers upon the realization that physical therapy wasn’t really going to work out as a direct sale approach. Then it went to wearable adoptions and adoption rates. Then it would have to go on to actual development costs, what did we think it would cost to build this thing out as a technology and would we be able to make enough money if we could get into any major insurers doors, to justify spinning up a company to do it. Those were the principal steps in getting to the key points for whether or not it was worth pursuing this in the size of the market for [company name].
As a co-founder, Sam was tasked with conducting market research, liaising with partners, and devising potential business models that reflected the ideas that other team members contributed. He was present for much of the technology’s journey, and recognized that a partnership with a large, vertically integrated United States-based insurer/provider could deliver what they wanted. This would involve linking algorithmically generated performance scores to other proprietary infrastructures, like electronic medical records and insurance claims records, to generate savings for the licensee. This would generate more financial security for the start-up, as they could plug in directly to that organization’s ecosystem. This, however, came with its own risks, as the CEO, Ken, outlines: The concern with that was from a business perspective that it’s kind of like a big bang thing, right? You can work with one guy for a year and you may or may not actually get through, so it’s a little more risky. But also, if you tend to work with one insurer, you can kind of be swayed by what they want. If you’re working with an insurer, they’re like your biggest customer, your main customer, and you don’t have many of them. And they ask you for, I want access to this or I want to build this or I want to do this a certain way, it’s really risky to say no to them.
The data assets generated by such an approach are distinct and associated with very different use cases for the technology. This new business model privileged the scrutability of clinical and administrative indicators for both individuals and groups, with the associated transfer of risk from the insurer or the provider, to an individual clinic, patient, or physiotherapist. These represent personalization at scale, where personalization can be used to individuate groups and populations through the creation of new risk categories or pools, and therefore new products and business strategies that transfer risk from the insurer to the individual (Cevolini & Esposito, 2020; Kampmann, 2024; McFall, 2019). By pursuing such partnerships, the team recognized that they could benefit from locked-in markets indirectly, through participation in ecosystems controlled by a small number of very large players, where contractual terms with those partners dictated access rights through licensing agreements. The potential pitfalls of such an approach, however, are also large. Patients would not use a technology if they thought that it could be to their disadvantage to do so, introducing challenges to the scale that would be needed to make a data asset viable in the first place (Geiger & Gross, 2021). Some patients also had personal reasons for not being able to use the technology, and if the technology was to become a condition of care, equity concerns also arose. Finally, the team also had its own attachments to the data and the technology and their uses, as an engineer, John, describes: You could easily see a situation where they roll out an app with one major feature. They acquire a ton of data through private clinics. But then they put a new feature in the app that says, if you want, click here if you’re not doing your exercises and you’re doing this other thing. Basically add a pathway for another label to the data basically and more data to be collected, they would have an easy way to collect a whole bunch of new data on another thing and they could use that to train a new model and grow the company. Add a new feature with this new model and so on, grow the company that way. I don’t actually think that’s a bad thing. I don’t see really privacy concerns with that. But I have this weird feeling about that kind of expansion that I can’t really articulate. That kind of thing and it does happen with a huge company, they can kind of easily create a monopoly on human activity data basically, because they have the means to collect it, it kind of snowballs, if that makes sense. Where they have this app that’s popular, they can add features by collecting data with the app. So, they get more features, they get more users, and it just keeps growing. I can’t articulate why but I feel like that’s not a great situation.
These controversies demonstrate that ‘thinking like an investor’ (Birch & Muniesa, 2020) rather than like an entrepreneur (i.e., a focus on investment return over the development of new products and services) required a shift than that not all team members, including John the engineer, were necessarily comfortable with or capable of pursuing. Moreover, the technology’s translation from one phase to another would only work if it could continue to maintain an appropriate set of relations amongst its basic parts, in this case, the core team, the functionality of the technology itself, the data resulting from its use, practical business requirements, and the assets those afforded.
Although the story continued to unfold beyond our three-year engagement, this latest phase best exemplifies the challenges associated with helping innovations ‘find their publics’ (Callon, 2021), particularly where competing valuations are at play. The technology, its data assets, and their perceived value regularly overflowed their boundaries, carrying traces of their past with them as they became enrolled in new and transformed ventures. For example, the team’s data monetization consultant, Margaret, was aware of the controversies surrounding different data valuation and assetization practices, and had to manage these conflicts while meeting the future-oriented expectations of the investors she was hired to attract. At the same time, this had to be accomplished without losing sight of the earlier forms of value that made the technology both desirable and useful to those who were intended to benefit from it, including patients and physiotherapists. This became increasingly difficult, however, as the data assets relied on and generated very different use cases for the technology, potentially breaking the set of relations that permitted the identification and pursuit of those assets to begin with.
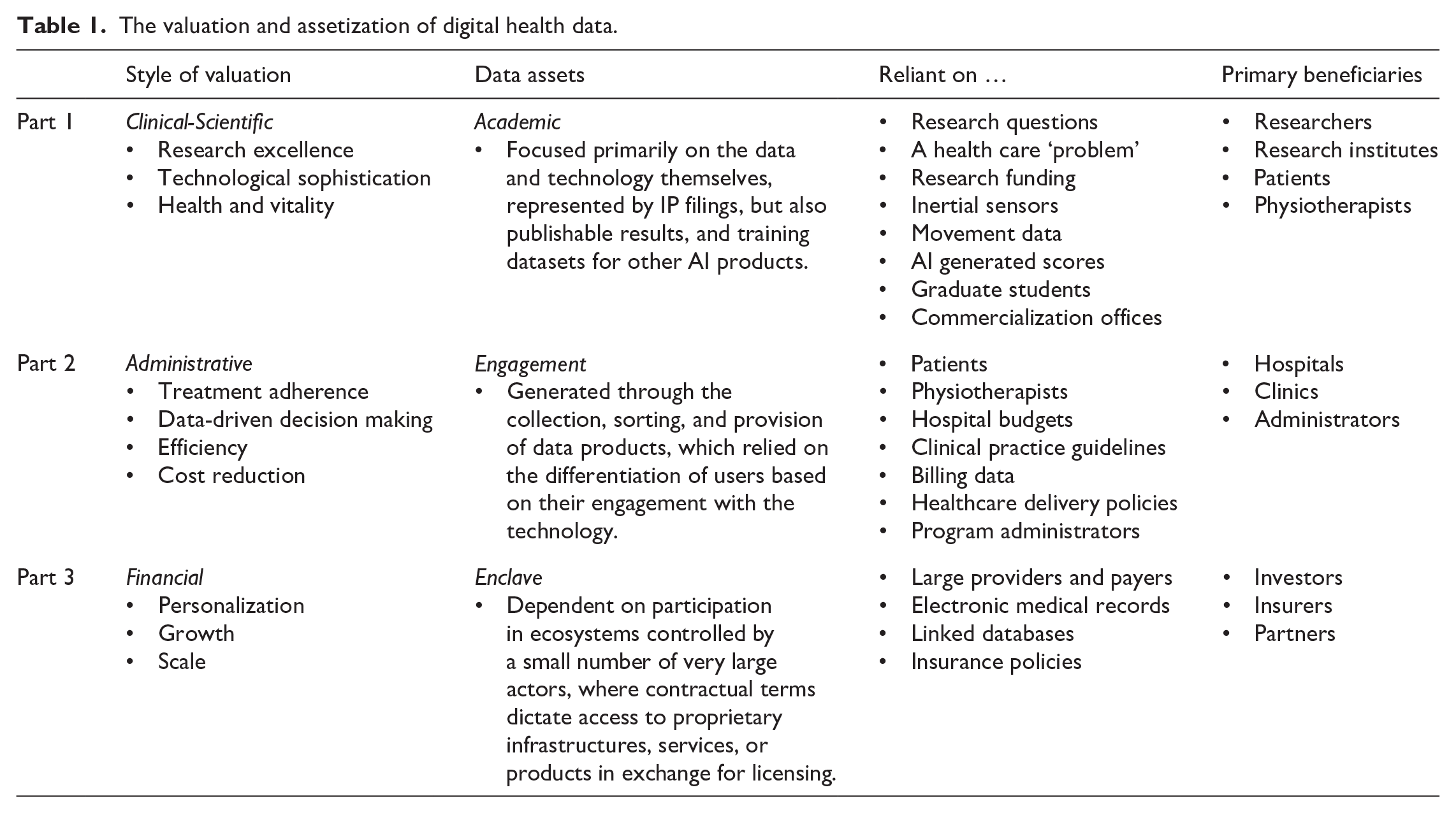
Put another way, while each style of valuation and its associated practices, beneficiaries, and data assets can be considered distinct (Table 1), they must also be considered in light of the activities that came before them. Clinical value was related to administrative value insofar as health, vitality, and research excellence were made to stand in for and support broader management goals, such as treatment adherence, or cost reduction. Clinical and administrative value also supported financial valuations, where investors would base their assessments of potential future growth on the technology’s ability to fulfil the clinical and administrative roles assigned to it, as well as the ‘added value’ made possible by combining new data with existing datasets made possible by large corporate actors. These overflows also signal that each style of valuation, and associated mode of assetization, always contains opportunities to intervene with different effects along the way. We discuss the implications of these framings and overflows in the discussion sections that follow.
The valuation and assetization of digital health data.
Proxy work as ‘sensing devices’ for digital health futures
The valuation and assetization of digital health data in the case we have described evolved considerably throughout the life of the technology. These practices relied on activities such as clinical validation, hiring staff, and developing and refining business models. It also involved patent filings, clinical standards, and other infrastructures in support of the enclosure of different forms of assetizable value (Coughlan, 2023). These different asset forms did not merely represent different uses of data, they created different data forms, each shaped by different styles of valuation. Reflecting on the contingency of these practices is important, as it can promote understanding of exactly how digital data enact different health-related futures based on what is expected of them, and how those futures are re-configured, re-envisioned, or discarded over time (Pinel & Svendsen, 2021, 2023; Prainsack, 2019; Vezyridis & Timmons, 2021). In contemporary health systems, this increasingly means attending to the entanglement of research products, especially data and digital technologies, and financial valuations, which have consequences for health care systems more broadly as different forms of techno-economic lock-in are pursued (Birch et al., 2021).
More specifically, we suggest that an essential component of translating digital health data into assets involves ‘proxy work’, where proxies are understood as useful fictions or ‘infrastructural analogies’ with the power to stand in for something else (Mulvin, 2021). Proxies are vital to the work of standardization (Mulvin, 2021) but also always carry traces of their past, being attached to prior people, places, and things (Pinel & Svendsen, 2021). Proxy work therefore allows data transformations, facilitating their movement away from where they were originally produced, and resolving competing styles of valuation through the enclosure of specific data assets. In doing so, it also allows those data assets to ‘find their addressees’ (Callon, 2021), whether patient, clinic, or insurer, at each step along the way. These practices of standing in through IP filings, user reports, and data labels, for example, can apply equally to researchers commercializing their technology through a start-up, or data brokers who ‘add value’ through processes of data aggregation and analysis (Mellet & Beauvisage, 2020).
In our case, the technology had to first identify desirable bodily movements and then represent those movements in quantitative scores. This process involved the training of an AI model on research participant exercise data generated by inertial sensors in a smart watch so that ‘good’ exercise movements could be distinguished from ‘bad’ exercise movements. Demonstrating accuracy and reliability through exercise-scores-as-proxies-for-movement was of course essential to the commercial success of the business, but first and foremost reflected evaluative criteria associated with the biomedical sciences, where specific notions of quality or research excellence are tied to academic performance (Rushforth et al., 2019). If the team could not demonstrate that their exercise-movement-score-as-proxy performed as well as or better than alternative products, or the status quo approach to treatment, there would be no innovation to market and no data assets to generate. These forms of proxy work involve mastery of both clinical research and technology development, each demanding different requirements and processes, but converging around a particular technoscientific artefact.
Second, the technology and its data products had to be situated within actually existing health care systems and not just hypothetical clinical scenarios. This required a re-configuration of the data to suit new administrative purposes, including integration with existing administrative processes and policy regimes. Data still represented bodily movements, but only as a higher-order proxy for other clinically-adjacent forms of value, such as efficiency. This act of delegation is itself highly significant, acting as a standardizing practice that facilitates the ‘temporary suspension of disbelief’ (Mulvin, 2021) as actors forget what the data and inertial sensors were intended to represent in the first place, and unwanted connections are cut and reframed in support of new goals (Berndt & Boeckler, 2023). Finding potential users (as proxies for patients and providers) and buyers (as proxies for clinics) became central to this endeavour. This move relied on an array of objects, processes, and valuation practices, each based on distinct notions of the human body and its associated clinical-administrative obligations (Goldenfein & McGuigan, 2023).
Third, the team had to consider what would be required to achieve success at scale. Digital health data became the stakes upon which the team could negotiate access to larger infrastructures and the corporate sponsors who owned them. This required yet another recursive loop, where data proxies were constructed in the most abstract form. Not only did data stand in as proxies for certain objective ‘truths’ about the body, a physiotherapist, or a clinic, but rather entire groups or populations with shared characteristics. Design work would need to maximize data collection in order to ensure that those associations were accurate and reliable, generating a form of lock-in that is distinct from the previous two. Algorithmic scores and movement data would be used in a setting and for a purpose that was really only possible by virtue of their participation in that ecosystem to begin with.
The contrasts between these different forms of proxy work are not only intended to highlight conflicting data epistemologies or representational harms associated with data profiling, as important as those are. Rather, we wish to point to the ways proxies make markets for data through design, and accordingly, their implications for value generation and assetization. Proxy work directs practical attention to design and market-making by connecting bodies, use cases, data, and more in unique ways over the life of a technology or a firm. Moreover, since not all health data futures have equal merit, proxies can be ‘sensors’ (Callon, 2021) for analysis, debate, or refusal, which leads to the focus of our next section.
Health data assetization, valuation, and collective governance
Presenting this case and its associated phases sequentially might seem to imply the inevitability of a lock-in model of assetization, where contemporary practices of innovation demand lock-in through the pursuit of success defined by scale. This raises questions of how health innovation ecosystems might reflect more pluralistic needs, under which conditions those valuations are possible, and what role assets themselves play in the pursuit and realization of different goals.
For example, the earliest iterations of the technology were primarily associated with institutions and practices of clinical, biomedical, and scientific valuation. The governance regimes suited to supporting more diverse valuations in these settings (e.g., funding priorities, training programs) would be very different from those in subsequent phases of commercialization (e.g., physiotherapy program design, data trusts). As valuations moved further away from the reach of formal scientific institutions, the need for broader conversations about infrastructural power increased. As an intermediary between data generation and their conversion into assets, proxy work focuses attention on how different practices of valuation shape data assets in-the-making, when such valuations occur, and where they are most likely to have impact.
With our own case, it was clear that alternatives were possible, but ambitions for growth led to particular commitments. In contemporary innovation ecosystems, small players often require larger ones to succeed, further entrenching those larger players’ positions in the process. There is therefore an argument to be made for approaching ‘Big Tech’ enclave-style assetization as a set of familiar practices. This is not to detract from or deny the immense power and influence of conventional Big Tech actors. These are immensely powerful actors that require differentiation. What we are suggesting is that their practices are increasingly mimicked by other actors in styles of lock-in that share problematic tendencies. Focusing on network effects, winner-takes-all dynamics, self-preferencing, and financial leverage (Birch & Bronson, 2022), and especially the simultaneous manipulation of assets and the associated milieus in which they are recognized and valued, we can approach ‘Big Tech’ as a type with different forms. This focuses attention on the empirical question of how and when Big Tech logics and practices shape health innovation ecosystems more broadly, the valuations they are predicated upon, and their consequences for collective governance.
Moreover, when assetization itself is a leading agent of change (Cordilha, 2022), the translation of clinical and scientific value into that which can be assetized reflects activities that ‘reflexively configure society itself’ (Birch & Ward, 2023). This work naturalizes certain practices of valuation and makes them seem inevitable, even though our own empirical example demonstrates that multiple visions, valuations, and conflicts lead to fragile accomplishments that prioritize different beneficiaries over time (Berndt & Boeckler, 2023). Proxies can bring to light exactly what kinds of relations, valuations, and infrastructures an asset form depends on, and who is prioritized in the performance of different health-related futures. Commercialization programs, economic policies, and imaginaries of data and digital transformation that understand data as assets increasingly make them so, but at different scales, and with different obligations for patients, clinicians, data users, and health systems more broadly, chasing some publics at the expense of others, and producing new forms of exclusion for those unable or unwilling to adjust to the conditions that emerging data markets require (Callon, 2008).
Conclusion
In this article we have outlined different phases of commercialization and modes of assetization associated with an AI-enabled smart technology intended for use in various health care settings. We have outlined how different valuations associated with the development and proposed uses the technology resulted in different asset forms, and described the techniques, infrastructures, and other objects implicated in the sociomaterial enclosure of different forms of assetizable value. These processes were not adjunct to practices of design and market-making, but constitutive of them, reflexively shaping the proposed uses of the technology and the data it generated, and the styles of obligation each relied upon.
In this sense, our case is not necessarily about data assets themselves. Rather, it is about the consequences of assetization as a dominant lens through which firms, governments and other actors increasingly attempt to perform, demonstrate, or realize value in practice. It is also about the disciplines that help those practices to succeed, including marketing and design. The apparent necessity of extractivist asset forms to the commercial success of digital health technologies, including those originating in academic settings, has consequences not just for health systems and those who work within and rely on them, but also the kinds of knowledge produced and who that knowledge is meant to serve (Fochler, 2016). In health innovation ecosystems where clinical value is interpreted primarily in terms of large-scale commercial potential, publics are unlikely to see short- or long-term benefits. Moreover, they are also increasingly unlikely to be able to have a say in any subsequent oversight and governance, where models of ownership and control are explicitly intended to obfuscate (Geiger & Gross, 2021).
We therefore suggest that in addition to questioning notions of value and property, attention should be paid to the conditions that assets advance in health care (Birch & Ward, 2022), including the forms of obligation and lock-in on which they rely, and their significance for collective health futures (Hummel et al., 2021). Equally, we suggest an emphasis on understanding the new disciplines, trades, knowledges, and practices that make this work possible. For example, what other functions does design fulfil, and which new practices might allow for alternative design futures? Finally, and related, at which moments or phases are these interventions most likely to fail or succeed, and who and what do they depend upon?
Footnotes
Acknowledgements
We wish to thank Kean Birch and the anonymous reviewers for their constructive feedback and detailed engagement with this work.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Collaborative Health Research Project special call: Artificial Intelligence, Health, and Society (Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council CPG-163963).
Ethics approval statement
This study received ethics approval from the University of Toronto Research Ethics Board (REB #00045774) and Women’s College Hospital Research Ethics Board (REB #2020-0132-E). Verbal or written informed consent was obtained from all study participants prior to their participation in the study, as outlined in the study protocol.