
Abstract
Artificial Intelligence (AI) tools are being developed to assist with increasingly complex diagnostic tasks in medicine. This produces epistemic disruption in diagnostic processes, even in the absence of AI itself, through the datafication and digitalization encouraged by the promissory discourses around AI. In this study of the digitization of an academic pathology department, we mobilize Barad’s agential realist framework to examine these epistemic disruptions. Narratives and expectations around AI-assisted diagnostics—which are inextricable from material changes—enact specific types of organizational change, and produce epistemic objects that facilitate to the emergence of some epistemic practices and subjects, but hinder others. Agential realism allows us to simultaneously study epistemic, ethical, and ontological changes enacted through digitization efforts, while keeping a close eye on the attendant organizational changes. Based on ethnographic analysis of pathologists’ changing work processes, we identify three different types of uncertainty produced by digitization: sensorial, intra-active, and fauxtomated uncertainty. Sensorial and intra-active uncertainty stem from the ontological otherness of digital objects, materialized in their affordances, and result in digital slides’ partial illegibility. Fauxtomated uncertainty stems from the quasi-automated digital slide-making, which complicates the question of responsibility for epistemic objects and related knowledge by marginalizing the human.
AI and data-driven technologies are increasingly being developed in the medical domain to assist professionals with complex diagnostic tasks (Keyes, 2021; Shastry & Sanjay, 2022). Though many of these technologies are still not in use in daily clinical practice, scholars within and beyond STS are investigating how they reconstitute organizations, professional relationships, knowledge, and responsibilities in the context of healthcare work (Bailey et al., 2020; Carboni et al., 2022; Elish & Watkins, 2020; Maiers, 2017).
Questions around knowledge and responsibility have emerged as particularly productive in a variety of academic debates concerned with decision-support systems. At the epistemic level, scholars have pushed against an exclusive reliance on ‘big’, quantitative data, casting qualitative, in-depth data as potentially better suited for some questions (e.g. Boyd & Crawford, 2012). Others have challenged AI and (big) data’s claims to objectivity by pointing to the omnipresence of interpretation, as well as to the fundamental issue of potentially ‘bad’ or biased data (e.g. Mittelstadt & Floridi, 2016). Not unrelated, questions of responsibility are often foregrounded in discussions of how professionals should incorporate algorithmic analyses in their decision-making, and who or what is to be held accountable when these decisions result in poor health outcomes (Gaube et al., 2021; Grote & Berens, 2020). However, this focus on bias, outcomes, and legal frameworks risks reducing ethical conversations to technical and legalistic ones (Scheuerman et al., 2021). In this article, we attempt to speak to these questions of responsibility and knowing through a different approach. Building on an ethnographic study of the digitization process undertaken by a pathology department in the Netherlands, we endeavor to unpack knowing and responsibility in digital and datafied healthcare by zooming in on the epistemic and ethical disruptions that AI (even in its absence) sets in motion in clinical practice.
Given the visual nature of its diagnostic processes, and recent developments in machine vision, pathology has become an obvious target for the application of AI-assisted diagnostics (Parwani, 2019). Currently, however, digitization is still only on the agenda of many clinical pathology departments. Pathology departments, anticipating a future in which AI-assisted diagnostics become the norm, embark on efforts to digitize the slides they produce through whole-slide imaging (WSI). We discuss the relationship between such digitization (i.e. the transformation of analog objects into digital ones) and other aspects of digitalization, (i.e. broader dynamics of datafication and introduction of digital analytic; see Trittin-Ulbrich et al., 2021) in our overview of pathological methods below. Currently, pathologists are increasingly requested to perform their diagnostic activity on digital, rather than glass, slides. Although one step removed from the actual application of AI software and thus considered fairly undisruptive (Ghaznavi et al., 2013), WSI nonetheless bears significant consequences for how pathologists make a diagnosis and for the (re)organization of the department itself.
To shed lights on epistemic disruptions produced by WSI, as well as on their material-semiotic foundations and on their ethical ramifications, we turn to Barad’s (2007) agential realist framework. Agential realism articulates how epistemic acts are generative of the reality they describe and, as such, inherently moral. By articulating the material-semiotic forces constituting the enactment of specific realities, agential realism, and specifically the concept of apparatus, lets us pin down how changes in organizational structures and epistemic practices are enabled by specific narratives and ambitions around digitization—which simultaneously disqualify the enactment of other types of change (Carboni et al., 2022; Giraud, 2019). In this frame, knowing emerges as intrinsically moral—an act that requires taking responsibility for the realities one co-enacts.
Attending to the different constellations of humans, technologies, materialities, and narratives constituting digital and non-digital apparatuses, in what follows we begin to catch a glimpse of the roots of the ontological otherness of the objects they produce. We then turn to our analysis of pathologists’ (digital) diagnostic practices. Building on pathologists’ expressed concerns around working on digital epistemic objects, we identify three issues: Sharpness, which we read as sensorial uncertainty, ontological depth, which we read as intra-active uncertainty, and fidelity, which we read as fauxtomated uncertainty. In our analysis, sensorial and intra-active uncertainty both stem from the ontological otherness of digital objects, materialized in their different affordances, and result in pathologists’ inability to meaningfully engage with slides. Though not unrelated, fauxtomated uncertainty emerges from an agential cut enacting a nonhuman subject position, which complicates the question of taking responsibility for epistemic objects. Because of the moral nature of knowing, we argue, experiencing uncertainty hinders pathologists’ use of digital slides in their diagnostic practices. To conclude, we elaborate on the relevance of agential realism for rethinking digitization and ‘good’ data in organizational settings.
Theoretical underpinnings
Particles of agential realism
Agential realism is a new-materialist, ‘posthumanist performative’ framework, committed to ‘a genealogical investigation into the practices through which “humans” and “nonhumans” are delineated and differentially constituted’ (Barad, 2007, p. 32). Through performativity, Barad offers an alternative to representationalism, the epistemological position that casts epistemic subjects and objects as pre-existing, separate entities, the relationship between which is mediated by representations. Conversely, performative frameworks insist that practices of representation (i.e. knowledge) are ontologically performative: They participate in the creation of reality—epistemic objects and subjects, their properties and boundaries are enacted in the act of knowing. Building on Bohr’s complementarity principle, Barad’s main contention is that knowing and being are intertwined. Performativity thus spans, simultaneously, the realm of matter and meaning. In Barad’s framework, the world is not made up of individual human or nonhuman entities, but of entangled agencies with multiple potentialities (‘phenomena’) that engage in and become determinate through specific intra-actions (a term Barard uses instead of ‘interactions’, to avoid presuming the existence of separable entities). Intra-actions crystallize human-nonhuman distinctions, as well as the boundaries of phenomena’s components, their properties, and the meanings associated with them. Intra-actions are respectively enabled or constrained by an apparatus—another Bohr-derived concept, here stretched to span boundary-making material-discursive practices. Apparatuses ‘produce, rather than merely describe, the subjects and objects in knowledge practices’ (p. 147).
In intra-actions, the boundaries between objects and subjects, humans and nonhumans, are defined through agential cuts. Just as human and nonhuman are not pre-determined substances, subject and object are not pre-determined positions that apply to individual entities with pre-defined boundaries. Barad, like Bohr, explains this through a thought experiment asking readers to picture a person holding a stick in a dark room. If the stick is held tight, it becomes an aid in navigating the room, and thus comes to occupy the subject position in the practice of knowing the dark room. If the person holds the stick loosely to sense its features, a different agential cut is enacted that relegates the stick to the object position. In agential realism, subject and object are mutually exclusive positions, enacted differentially in different practices (e.g. sensing the room vs sensing the stick). The boundaries of epistemic subjects do not coincide with the boundaries of what we assume to be ‘human’: ‘Human’ itself is a category emerging within intra-actions. Objects and subjects do not pre-exist their interrelating, and different intra-actions, through different apparatuses, will enact ontologically different subjects and objects.
Objects and subjects thus cannot be divorced from the intra-actions that enact both. Ontology and epistemology thus implicate each other: There are no entities and no knowable characteristics outside of practices of knowing them. Epistemic practices, with the apparatuses sustaining them, are implicated into crystallizing specific configurations of the world—at the expense of other possible ones. Agential cuts are for Barad a matter of ethics: Actors involved need take responsibility for the realities they do and do not enact.
Apparatus and epistemic cultures
The study of epistemic cultures (Knorr Cetina, 1999) foregrounds epistemic practices, the ‘logics and arrangements through which knowledge comes into being and is circulated, approached and collectively recognized’ (Nerland & Jensen, 2012, p. 104). Knorr Cetina postulates such practices as pivoting on a specific ‘epistemic machinery’ that constitutes, in a certain area, ‘how we know what we know’ (1999, p. 1). This concept resonates with Barad’s notion of apparatus. Like an apparatus, epistemic machinery shapes, enables, and constrains epistemic acts and the knowledge produced, creating the conditions under which ‘practitioners distinguish signal from noise, … or … decide which figure to trust when experimental outcomes are uncertain’ (Knorr Cetina & Reichmann, 2015, p. 18). The introduction of new technologies in an epistemic culture produces the rearrangement of epistemic machineries and their related cultures (Knorr Cetina & Amann, 1990; Stevens et al., 2022). The concept of apparatus, however, emphasizes how ‘machineries’ are simultaneously material and semiotic, enabling us to probe the material-discursive practices shaping both the knowledge produced in a specific culture, and the objects and subjects within the culture itself. Moreover, Baradian agential cuts do not always result in epistemic subjects that neatly line up with the boundaries of the human—and sometimes are not occupied by ‘the human’ at all (2007, p. 379).
As for epistemic objects, Knorr Cetina (2001) acknowledges they do not fully pre-exist the epistemic practices that investigate them: To some extent, their very ontology emerges within epistemic practices. Centering on intra-actions, agential realism enables us to specify how epistemic objects unfold. Intra-actions are moments of embodied engagement, through which subjects, objects and their representation are enacted. We usually think of these moments as instances of sensory knowing. Recent scholarship on the more-than-human sensorium has argued that knowing agencies are not confined within the boundaries of what we traditionally think of as human. Especially in digitized settings, healthcare professionals engage in a sense-making that is at once embodied and technological (Harris, 2021; Maslen, 2017; Maslen & Harris, 2021). However, increasing reliance on digital technologies in professionals’ sense-making 1 is often found to lead to a progressive devaluing of sensory knowing (Beaulieu, 2002; van Dijck, 2011), especially when under the pressure of organizational policies (Campbell & Rankin, 2017) or of personnel shortages (Maiers, 2017).
In this article, we simultaneously embrace and problematize the crucial role that senses play in medical diagnostics. We postulate that professionals’ expertise transcends the usually accepted boundaries of the human, by almost seamlessly incorporating devices in their sensing and sense-making. By foregrounding the specifics of how sensing with digital technologies is enacted in clinical pathology, we broaden the idea of professional sensing beyond the boundaries of perceiving, to span the enactment of diagnostic realities. By teasing out how pathologists and their microscopes, rather than just perceiving, actively enact the properties of the object they analyze, we argue that more-than-human sensing practices should not only be investigated in terms of their hybrid nature, but also of their enactment of specific realities—and thus of their intrinsically ethical nature.
Agential cuts, affordances, and automation
We propose thinking about epistemic objects’ enacted properties in terms of affordances emerging from an agential cut (Hollin et al., 2017). Affordances are usually mobilized to describe what an artifact enables or encourages users to do (Bucher & Helmond, 2018). However, since agential realism casts knowing and intervening as fundamentally entangled, here we expand the concept of affordances to include the possibilities for intra-acting with, and thus knowing, a specific (epistemic) object. In agential realist terms, objects’ affordances are consistent with the material-semiotic practices we are referring to as apparatus; they support the epistemic practices expected by the users enacted as epistemic subjects within that very apparatus.
For pathology, a crucial difference in the apparatuses enacting digital versus glass slides concerns a degree of automation that often comes with digitization. We argue that automation of this work qualifies as fauxtomation, that is, the practices around the ‘myth of human obsolescence’ mobilized around technologies that (promise to) automate work (Taylor, 2018). 2 Fauxtomation allows us to see that mainstream narratives around automation obliterate the amount of human labor that automation technologies still require. This ‘reinforces the perception that work has no value if it is unpaid and acclimates us to the idea that 1 day we won’t be needed’, leading to a devaluation of human, and especially menial, labor (Taylor, 2018).
Since apparatuses are performative of epistemic subjects, fauxtomation is also involved in agential cuts that have concrete consequences for who (or what) is enacted as a subject. The idea that human labor can be made obsolete and automated can result in an agential cut that enacts nonhuman epistemic subjects. If the fauxtomation of diagnosis is, in clinical practice, still confined to the realm of future possibilities, it often underpins the enactment of digitized epistemic objects—which thus are often produced by technologies in the first place. Although humans are not absent from the organizational configurations stemming from these agential cuts (we are talking of a fake automation, after all), they occupy a position ancillary to the technology and its needs. This has significant ethical consequences since, as we have seen, epistemic subjects need to be accountable for the realities they create, but machines are famously unable to do that (Floridi & Sanders, 2004). A representationalist critique of fauxtomation narratives might reject the agential cut those narratives draw between humans and supposedly automated work, but in this work we maintain an agential realist perspective by using these categories descriptively, rather than analytically. We trace how a self-contained machinic epistemic subject emerges through specific intra-actions that, being enabled by the fauxtomation narrative, are predicated on and enact a strong boundary between machines and the humans operating them. Thus, we call fauxtomation faux not because of the cuts it makes but because it imagines a particular cut to separate definite, a priori categories.
Fauxtomation provides us with an entry point into the dynamics of organizational change that underpin processes of digitization, and into their onto-epistemic performativity. It reminds us that myths and narratives have tangible consequences for how we design and implement the relationship between human and machinic labor. We thus mobilize fauxtomation to examine the intertwinement of organizational and epistemic dynamics, and to problematize the boundary between automation of menial and of knowledge work. We argue that ways in which some tasks are considered more automatable than others are predicated on a devaluing of the sensory and contextual knowledge inherent to those tasks. This bears serious consequences for the reliability of the epistemic objects produced in the department, as well as for professionals’ ability to take responsibility for the knowledge they produce.
The theoretical framework that we have brought together in this section suggests that the root of the ontological otherness of digital objects is to be found in changes in the workflow, materialities, rules, and people brought together to produce them, and simultaneously in the narratives and expectations steering these changes. Through this semiotic-material apparatus, specific agential cuts are enacted, resulting in specific distributions of affordances and responsibilities. This entails that, (1) ontological differences materialize in objects’ affordances, which are to be considered not only possibilities for acting on and with an object, but also possibilities for knowing the object; (2) if epistemic questions are never separated from ontological ones, we need to bring into focus the organizational conditions (both material and semiotic) of production of the epistemic objects at hand; and (3) because of the ethical dimension inherent to epistemic acts, responsibility for the realities that newly-configured epistemic subjects enact can be foregrounded in the analysis of digitization efforts and organizational change. In what follows, we attempt to apply these insights to gain a deeper understanding of the dynamics of change that digitization initiates in different locales of a pathology department.
Data and methods
This article builds on an ethnographic study of a hospital pathology department in the Netherlands. One of us (Carboni) engaged with the department in various ways over the course of six months in 2021, as the department purchased new scanners and endeavored to tighten its policies around digital diagnostics. Because of the relatively long duration of the data collection, we were able to analyze our data abductively (Tavory & Timmermans, 2014), moving back and forth between the ‘field’ and our analysis, and progressively refining our research design and strategy. The data collection started with 15 exploratory interviews with various members of the department, selected and recruited with the help of the department’s head. The participants included in this first phase were thus judged by the department’s head to be meaningfully involved in the digitization process. They included pathologists who were both users and non-users of digital slides, as well as the manager overseeing the process, the lab managers, and lab technicians involved in the purchasing, set-up, and validation of the scanners. These interviews had a broad focus on participants’ experience and expectations around digital pathology from different angles and were conducted via Microsoft Teams. Based on them, we were able to trace the current state of the digitization process within the department, as well as to get some insights into issues currently experienced by pathologists.
After this exploratory stage, Carboni started attending the weekly meetings of the working group responsible for the digitization process (consisting of a few clinical pathologists, two managers, a few lab technicians, the head secretary, the head of the tissue bank, and an image analysis specialist). During these meetings, relevant issues ranged from purchasing, to testing and validation, to pathologists’ needs and workflow reorganization, to machine learning in image analysis. Thanks to these observations, Carboni was introduced to the expectations and the most current issues experienced by the department in terms of digitalization, and could observe the strategies discussed and implemented to deal with them. At the end of each meeting, Carboni had an informal hour-long conversation with the senior pathologist leading the working group, during which she deepened her understanding of the technical issues that had been treated and discussed more general points about pathology. Scientific literature, both suggested by participants and retrieved by the authors, was also consulted to learn more about the history of pathology and the developments around WSI and AI.
Carboni also conducted ethnographic observations in the department, with the aim of mapping the various stages of the workflow and to gain an in-depth understanding of the practices and tasks involved in each step. To do this, she adopted a ‘follow the tissue’ methodology, which entailed tracing patients’ samples (and their metadata) as they got (re)processed and progressively turned into slides. She observed front-desk secretaries as they registered tissues coming into the department, assistant pathologists, technicians and trainees as they prepared samples, lab technicians mounting samples on slides and checking their quality, and secretaries scanning the slides. She also joined the morning handover meetings during which interesting cases were presented by either pathologists or trainees, and attended one training session for ophthalmic pathology.
Ethnographic observations enabled us to trace the distributed epistemic and material practices at the heart of the department. During the working group’s meetings and exploratory interviews, however, participants expressed concerns about whether pathologists could see ‘well’ enough to make a diagnosis when analyzing digital slides. To better understand what ‘seeing’ entails in clinical pathology, Carboni conducted five object-elicitation interviews, using digital and analog slides as concrete props to scaffold the conversation. These conversations circumvented a shortcoming of observation: Pathologists ‘see’ quickly, mostly while hunched over a microscope—an unfavorable situation for an external observer. As often found in qualitative research, graphic or object elicitation in interviews support participants in articulating their lived experiences (Woodward, 2016). In our case, discussing concrete cases with pathologists, probing them on which cues enabled them to make a diagnosis, and how they went about getting these cues, enabled us to reach a deeper understanding of the embodied practices underpinning slide analysis. Our interpretation was enthusiastically confirmed by pathologists themselves during the two presentations Carboni held at department-wide meetings. Drafts of this article were also shared with the research participants for a member check. Participants provided a few technical corrections but did not request the removal of any quotes or fieldnotes from the analysis.
‘Turning meat into information’: Pathology work as intra-actions
The profession of pathology, rooted in anatomical studies of disease processes through autopsies, has grown and differentiated into a complex and varied medical specialty, whose practitioners contribute to individual patient care, the detailed description of diseases, and even the ontology of disease itself (Van Den Tweel & Taylor, 2010). In this article, we focus on histopathology (henceforth, for simplicity’s sake, ‘pathology’), the examination of cellular structures under a microscope, since it is the subsection of pathology on which digitization efforts currently focus. Since the 1990s, pathology has entered an era of intense technological innovation through the gradual move to WSI (referred to here as digitization), automated image analysis, and development of AI for assisting diagnostics (Ghaznavi et al., 2013; Pantanowitz et al., 2020). These forms of digitalization promise increased quality of diagnosis, reduced work burden for pathologists, and a move towards personalized medicine.
Nonetheless, in practice, even digitization proves difficult. The department where we conducted our fieldwork had been engaging in this shift for more than ten years. Throughout our fieldwork, we witnessed the discomfort of pathologists and other actors, such as secretaries and lab technicians, with the changes digitization forces into their practices. This section explores the department’s workflow, with an eye on the intra-actions through which digital and non-digital slides are enacted. Crucially, albeit not being part of the diagnostic process in the strict sense, these intra-actions are both a testament to the distributed nature of diagnosis, and to the inextricability of matter and meaning. Knowledge is being applied and produced at every step of slide-making.
Much of a pathology department’s work revolves around creating (good) slides. This is a sort of datafication of human bodies, as explained by a senior pathologist who described his work as ‘turning meat into information’. In the hospital where we conducted our fieldwork, tissue samples of disparate sizes, from biopsies to entire organs, are collected from various wards and delivered to the department’s front desk several times a day. Front desk secretaries register the case in the department’s lab and information management system (LIMS). They connect the case file in the LIMS, which details the extent and nature of the sample, with the patient’s information in the hospital’s electronic health record, and assign to it a specific 2D barcode that is then printed out and stuck on each jar making up a case. Scanning this barcode automatically opens the case file in the LIMS.
Next, secretaries transfer tissue samples to the grossing room, where assistant pathologists, residents and lab technicians perform an examination of the samples and fix samples in formalin, making them hard and resistant to proteolysis. While small samples such as biopsies are directly embedded in blocks, larger samples must be dissected, put into a cassette, and embedded in paraffin, creating multiple blocks (Figure 1). This is a first kind of intra-action, a moment in which enacting an object and knowing it are inextricable. Pathologists and assistant pathologists describe how touching bones, cartilages and tumors in the specimen makes grossing an act of bodily engagement, steered but not determined by protocols, scalpels, pathology saws, and numbering practices. These forces also steer the selection of which parts of the specimens to turn into blocks, and which to reject. The process of inclusion and exclusion, of enacting only some properties as belonging to the epistemic object in question, is here extremely visible. Crucially, it is also painstakingly documented through pictures, reports in the LIMS and, in case of doubt, by involving more senior pathologists. Although no definitive cut is enacted (after sampling, large specimens are temporarily preserved in the grossing room in case pathologists request additional slides), the thorough documentation of this step enables accountability for the epistemic objects produced.

Small samples of tissues are embedded in paraffin and turned into a block. The different colors of the blocks flag different types of tissue. On trays, blocks are transferred from the grossing room to the lab, where technicians turn them into slides.
Blocks are taken to the lab, where technicians cut their content into very thin slices using rotary microtomes. They then mount these thin tissue slices onto small glass rectangles, to which they also apply labels with the case’s barcode. These half-slides are fed to an automated staining machine. Once processed by the staining machine, tissues are visible and coverslipped: A glass slide has been created. The agential cut in this second intra-action enacts a subject position that is less clearly ‘human’, since the process of staining is automated. Color, which as we shall see plays a fundamental role in epistemic practices, is thus enacted in an automated intra-action. When sliced, tissue samples appear transparent: Staining is thus an intra-action through which some of their parts emerge as colored, and thus legible. Through staining, tissue samples are enacted as containing specific cells, and structures with specific characteristics.
The automated staining machine does not document this intra-action. There are however systems in place to retrospectively check that the apparatus enacts consistent epistemic objects: In the case of ‘special’ stains, glasses are equipped with a control tissue, positioned next to the specimen. And once the staining machine has finished its operations, a lab technician collects the slides and checks them under the microscope, to examine the epistemic objects and certify the legibility of their enacted properties.
The digital workflow entails an additional step—digitizing the slides. The person assigned to this task varies from place to place: If elsewhere specifically-trained biotechnicians are in charge of this process (Kusta, personal communication), in this department a secretary was reassigned from the secretariat to a dedicated ‘digital pathology’ room. This ‘scanning’ secretary waited approximately 10 minutes during our first observations before stating how much she disliked her job. Her main task entails feeding the glass slides to the four big pathology scanners crowding the room. Of these, two are new-generation, highly automated scanners, one is a specialty scanner, used exclusively to scan dermatopathology slides, and the last one is an older, drastically less automated one. Operating the latter requires a great amount of work from the secretary (Figure 2), as emerges from the fieldnotes below (all names below are pseudonyms):
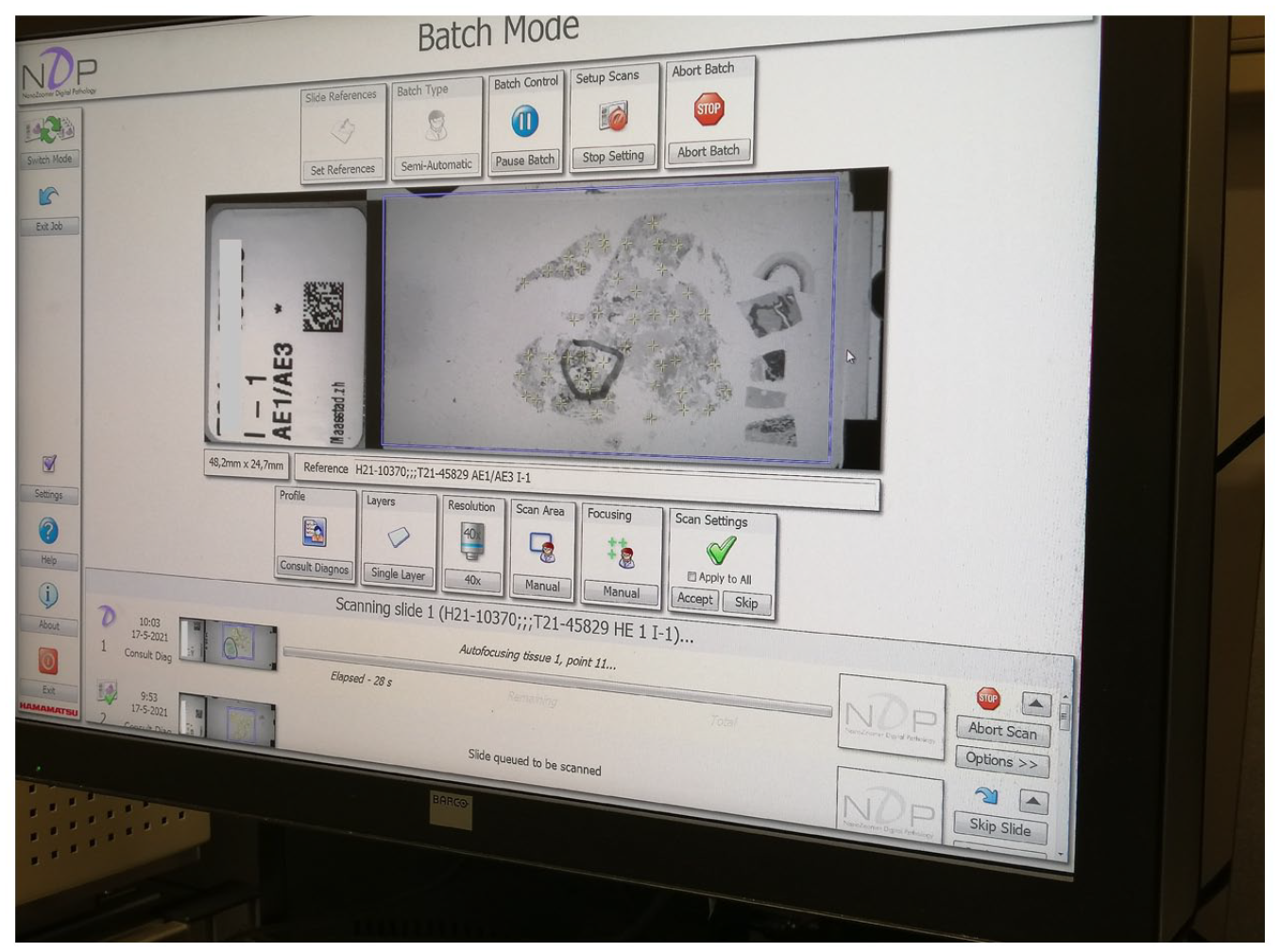
In the older scanner interface, scanner and secretary produce a digital slide: While the scanner implements an ‘autofocusing’ function, the secretary further directs it selecting areas of particular interest; in this case, part of the tissue has been circled by a pathologist: the secretary places more focal points around that area.
Jane fills up the scanner’s rack with the slides, paying attention to make them match the order of the trays, so it’s easier to put them back in the right trays when the scanning is completed. This older scanner is cumbersome, she explains, because it does not automatically focus on the tissue on a specific slide. So she needs to do this by hand: She enters case number associated with each slide, waits until the scanner takes a ‘picture’ of each slide, then opens each of them and starts clicking on the tissues, tracing both its contours and the body itself. With each click, a small asterisk appears on the picture of the slide. On this one, a pathologist has already drawn circles around areas of tissue of particular interest. Jane makes sure to put a bit more asterisks in those areas. On the side, there is some additional tissue, but she tells me they’re controls, and don’t need to be scanned, so she does not put any asterisks on them. It is a painstaking task, it takes a lot of time, and Jane jokes that sometimes it makes her fall asleep. Once she is done, the scanning starts. On the screen, the scanned asterisks turn green. (fieldnotes)
Despite reportedly a supremely unexciting task, it is clear how much work the scanning secretary needs to perform in order for the scanner to produce a good digital image. The agential cut, in the case of non-automated scanners, enacts a hybrid subject position, in which the scanning secretary and the machine are not easily distinguishable in the digital slide-making. Jane can lend her eyes and her contextualized seeing to the scanner: She is familiar with pathologists’ habit of circling parts of the specimen that require particular attention and knows that a circle drawn on a slide warrants more focal points, so that the image produced will be sharper in that area. She is also aware that control tissue is placed on the slide when it undergoes a specific staining process, is able to distinguish the control tissue from the specimen, and knows that there is no need to include it in the digital image. Her contextualized knowing and seeing enable the older scanner to produce good digital images.
Newer scanners, however, require less work on her part. They are part of an apparatus crucially informed by fauxtomation. New generation scanners (Figure 3) can identify the tissue’s position on the slide (and thus which areas do not need to be scanned). They also automatically select focal points on the slide, based on an automated scanning protocol, so Jane only needs to load them with glass slides and start the process. After the scanning is completed, the scanner also rates the quality (i.e. sharpness and contrast) of the image, assigning to it a number up to 100. In this intra-action, a largely nonhuman subject position is enacted: The fauxtomated apparatus makes Jane’s perceptions and tacit knowledge superfluous. This process of automation is faux-, however, because it still substantially relies on human labor. We observed that these scanners in practice run a lot less smoothly than expected: They reject some slides, and sometimes enact digital slides of insufficient quality. All of these cases call for Jane’s intervention.
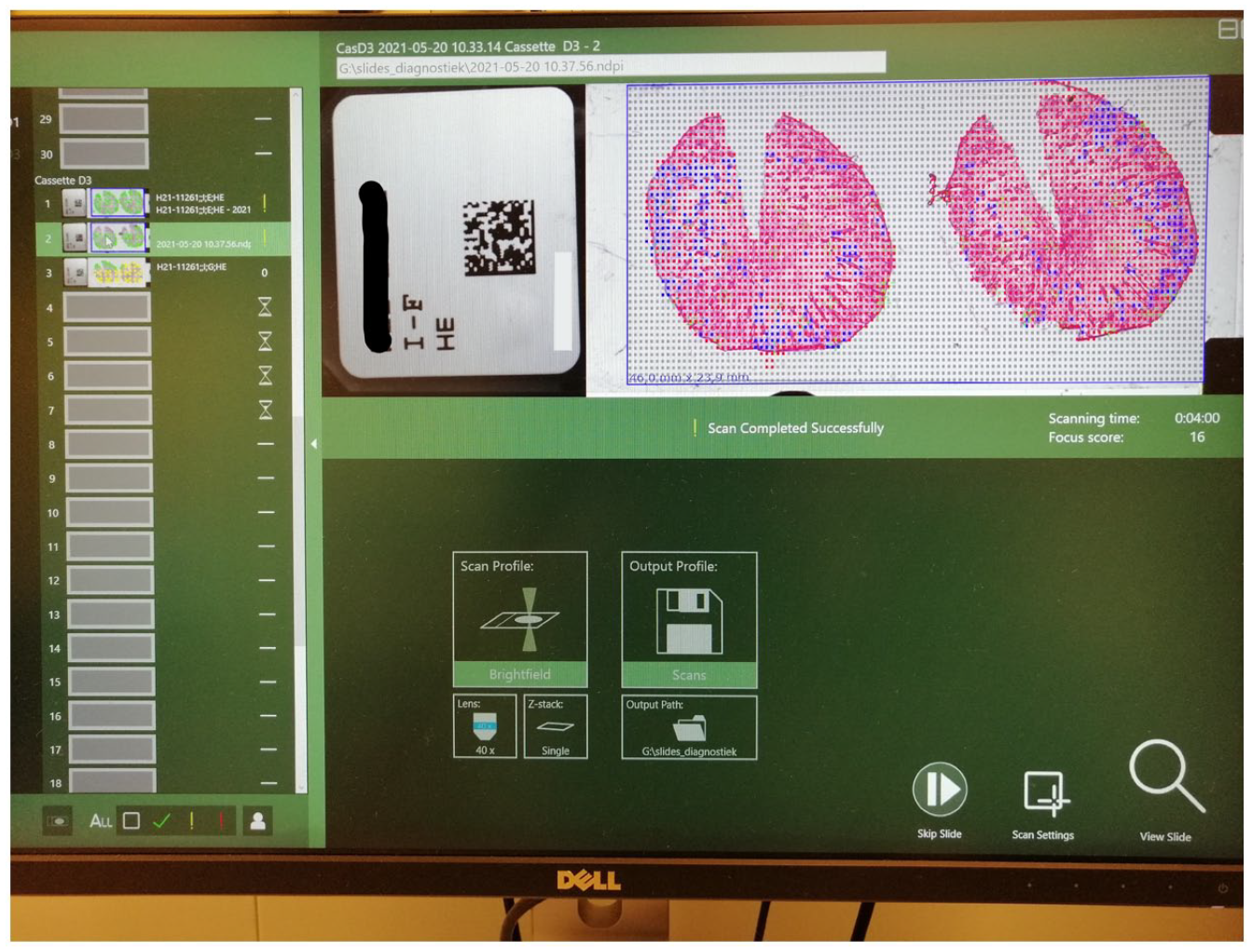
New-generation scanners are enacted, in faxutomated intra-actions, as firmly occupying the subject position. They autonomously select the boundaries of the tissue on the slide, and the areas on which more focal points (the blue and yellow crosses) are necessary. They also attribute a focus score to the resulting image, based on the contrast achieved in the scanning process. The secretary is only tasked with loading them, and restarting the scanning if the score is too low.
The digitizing intra-action is thus the only one in the department in which humans are only marginally enacted as epistemic subjects and of which there is no documentation. Crucially, digitization also entails a different apparatus, this time made up of scanners, their protocols, image recognition software and related algorithms, software for image quality control, rules for priority, inscription devices, secretaries supporting these operations, the need for sharpness, the fauxtomation myth, and the expectation of AI-driven diagnostics. As we show in the next section, this enacts epistemic objects with properties and affordances different from their analog counterparts, which in turn enable (and disable) different epistemic practices.
Diagnostic intra-actions
In this section we provide an agential-realist reading of pathologists’ diagnostic practices. We analyze diagnosis as an instance of intra-acting. If conceptualizing the lab’s workflow as a collection of intra-actions helped us understand how epistemic objects end up having specific properties, here we focus on how epistemic objects are enacted as legible for a specific epistemic culture, and on how they are involved in diagnostic processes. Specifically, we attend to how digital and non-digital objects afford different types of intra-active engagement from different epistemic subjects.
This operation entails unearthing diagnostic practices in pathology that, at a first glance, mainly concern seeing: Pathology labs work to make tissues and their microscopic structures visible, and pathologists themselves appear to spend their days carefully looking at slides. In this section, however, we attend to what it takes to see in (digital) pathology. We juxtapose digital and non-digital epistemic objects and the intra-actions they afford, endeavoring to tease out the epistemic implications of the ontological difference between the two. The ensuing epistemic dynamics produce, respectively, sensorial, intra-active, and fauxtomated uncertainty.
Situated seeing: Sensorial uncertainty
Haraway (1988) famously reminded us that a view is always from somewhere. This very concretely applies to our case, insofar as specific epistemic cultures develop particular ways of seeing (Friedrich, 2010), as well as epistemic objects that enable those ways of seeing. Apparatuses co-produce not only objects and subjects, but also objects that are legible within an epistemic culture and culturally specific practices of reading them. In pathology, traditional epistemic objects (i.e. glass slides) present affordances that can be meaningfully harnessed within pathologists’ intra-actions. They lend themselves to be known in a way that makes sense within pathology’s epistemic culture.
In their intra-actions, pathologists focus on histological structures (different types of cells, their subcomponents, and the architectures they make up), especially their qualitative aspects (Apfeldorfer et al., 2008). Color plays an important role, as Jody, a young pathologist specializing in pulmonary and dermatopathology, explained as we were looking at a glass slide through her microscope:
[Malignant cells] look different. I’m sorry, I don’t have metastases [on this slide]. But they are really pink. So, here everything is a little bit more purple, and they would be really pink. But I will show you the tumor. … they are enlarged, and they are quite pink.
Being the result of the staining process, color makes for an interesting visual cue: It has been enacted as the result of a previous intra-action. However, it is not the only relevant visual cue. Altered shapes and histological architectures, and the relationships among different cells are all important signals of pathogenic changes as Harold, a senior pathologist specializing in gynecological pathology, articulates:
[Y]ou can see that [cervical cancer cells] have less cytoplasm, so they are less pinkish. They do have dark, sometimes irregular nuclei, here the nuclei are more open. It is darker and … you have a change in nuclear size and shape.
The department’s non-digital apparatus thus enacts glass slides in which color, shapes and nature of lines are meaningful characteristics; pathologists and microscopes are enacted as prospective users of these epistemic objects, and qualitative detail as relevant in the department’s epistemic practices. 3
Since epistemic objects and epistemic practices are co-enacted through an apparatus, it may come as no surprise that the digital apparatus constitutes a disruptive element in the department’s diagnostic processes. Although they resemble each other, digital and glass slides are enacted through different apparatuses, and thus present different affordances. As a result, pathologists rarely perform their diagnostics on digital slides only. When in doubt, even pathologists who consider themselves enthusiastic adopters move back to the microscope to examine glass slides, as Laura, a young pathologist specializing in gastrointestinal pathology, did during our interview:
This is suspicious. Look, this is a lined lumen and there is a tumor cell. I have to be sure. And then … I have to find this in this slide again. I still prefer to see the slide as well, in this case. … Just to check, actually. To be certain. But it’s not really necessary, I mean, I can also—this would be sufficient to do it here.
Pathologists often brush off this widespread uncertainty as a matter of technical limitations, of insufficient image quality, bound to be overcome with technological developments. Here we attempt to take this uncertainty seriously, as rooted in the ontological difference between digital and non-digital objects, and in the lack of fit between digital objects’ affordances and pathologists’ intra-actions. Digital slides are enacted by an apparatus that also enacts AI as a potential epistemic subject. Subsequently, their affordances encourage epistemic practices less tied to the largely qualitative ways of articulation intrinsic to pathologists’ expert seeing. Pathologists articulate this shift when reflecting on what digital slides do not enable them to see, or what they discourage them from looking at. Consider, for instance, this quote by Hanna, a long-time user of digital sides, specializing in dermatopathology:
[Looking at digital slides] is something that you have to get used to. Because I mean, if you look at a granulocyte [under the microscope], for example, the nucleus looks like a pair of glasses, and it has a bit of red around it; normally, under the microscope, you can really see the granules—and [on digital slides] you just see it as … red dots, but not as granules. And you just have to get used to that and … adjust this in your head. … you still can recognize them, but it’s not fully in the same manner. For mitosis, I don’t have a solution. I think that I can now recognize granulocytes as easily on digital [slide] as under the microscope, with a good scanning. But the mitosis—you really miss it … And sometimes I still have to take the glass slide, because I’d have it anyway—and put it under the microscope.
Digital slides do not allow pathologists to examine the same amount of qualitative detail as glass slides would, especially when looking a cells’ nuclei. As Hanna explains, pathologists can learn to recognize specific features, even though they look different on a screen—but other features are still difficult to spot, even after years of practice.
At the same time, digital images and associated viewers afford increased precision in the quantitative mode of analyzing slides. The epistemic object comprising digital slides and imaging software lends itself to quantification much more than glass slides and microscopes, thanks to built-in quantification instruments, such as precise measuring devices. Besides ‘secondary advantages’ (Harold), like increased traceability of slides, shareability with colleagues and students, and remote accessibility, digital pathology also enables pathologists to perform more quantitatively precise measurements, which can significantly influence the recommended choice of treatment. We can thus think of digital pathology as fostering epistemic practices that prioritize quantitative precision (how many things are there, what they measure) over qualitative precision (the examination of how things look).
Though they do not fit with pathologists’ current epistemic practices, digital slides’ affordances are central for AI, a prospective user envisioned central in the department, as John explains:
We put a lot of money in machines and actually … your diagnosis doesn’t improve at this point. And it’s all to generate these slides images for future analysis, because you have to make the step to artificial intelligence. And you can only do it when you have a fully digitalized pathology department.
Automated image analysis, which at least in this department is still in the realm of future possibilities, would, in its infancy, mainly be concerned with quantification tasks, such as counting specific cells or mitotic figures (Ibrahim et al., 2022). As we learned during a demonstration given during one of the meetings of the department’s digitalization team, the level of qualitative detail machines and deep learning need in order recognize specific types of cells is limited to the presence of specific colors on the slide (e.g. the red of granulocytes Hanna mentions above). Further qualitative detail is, at least at this point, superfluous. By enacting AI as a potential prospective epistemic subject, the digital apparatus thus also enacts epistemic objects with affordances that do not always fit easily with pathologists’ intra-actions, giving rise to sensorial uncertainty.
More than looking: Intra-active uncertainty
While the section above testifies to the relevance of slides’ qualitative properties for pathologists’ epistemic practices, casting these properties as something inherently present or absent in slides would lead us back to the representationalist fallacy that agential realism seeks to overcome. In this section, we harness intra-action to conceptualize glass slides and the visual information on them as something that is enacted through the epistemic practice of light microscopy. Crucially, we argue that qualitative detail is not inherent to glass slides, waiting to be surfaced: An untrained observer cannot just look at a slide and see meaningful detail, no one can examine a slide without a microscope, and it is hard to engage meaningfully with a glass slide when someone else is using the microscope. Rather, qualitative detail is enacted as a property of glass slides during intra-actions.
A close observation of pathologists’ practices of engagement with microscopes and glass slides shows how this entails more than just zooming in and out. Seeing with a microscope is not just a matter of looking: It is about receiving ‘good’ specimens, about selecting the right lenses, about using the microscope’s light in the correct way, about inspecting the specimen without neglecting relevant areas. ‘Seeing’, for pathologists, is therefore not just about seeing. One becomes a pathologist with and through a microscope.
These intra-actions are such a fundamental part of the practice of pathology that it can be hard for both pathologist and ethnographer to pin them down. There are, however, specific operations that can provide us with a glimpse of the intra-active nature of the practice of light microscopy. As Jody explained, pathologists know how to ‘play a little bit with the microscope’, and this enables them to make specific characteristics of the slide visible, while backgrounding others:
So, for example, if I’m looking at the mitotic figures … it’s like this, [you get] this picture. But … if I turn this knob here, I can actually scroll through the nuclei. So now I’m getting this a little bit sharper, and if I [turn again], now, this gets a little [in] background and I’m getting this a little bit sharper. And if I’m not sure about the mitotic figures, I can use this technique to scroll through the nuclei to see how things are changing. And that’s something I can’t do with the computer.
We can think of the visibility of nuclei as a property of the slide that is not just surfaced but is enacted in this intra-action. In light microscopy, pathologists and microscopes are enacted as a joint subject, responsible for (and capable of) crystallizing as relevant specific properties of the glass slides. In the quote above, the glass slide emerges as an epistemic object with visible nuclei. Similarly, we can start to understand how qualitative detail, rather than being inherent to glass slides, is enacted within intra-actions in which pathologists and their microscopes share a hybrid subject position. In the following quote, Jody explains how light also participates in intra-action, not just in terms of making colors visible, but in a less deterministic and more tentative way:
And another thing I can’t do with the computer is—if we have foreign material in the lung, then we use … polarized light … This is probably some dirt, but you see … it shining up. So, if I have crystal structures, for example—some pleural diseases go paired with crystal structures—I can make them visible only with this technique. And I can’t … see them in the computer, because I can’t use this technique breaking the light in a special manner. … if I have an infection with a granulomatosis aspect, I always want to look in polarized light, because I want to know if there’s foreign material inside the granuloma … So if I only had the chance to look on the computer, I’d still have to ask the secretary to give me the [glass] slide, so that I can look at it. … I want to be sure, I don’t want to miss anything.
The possibility of engageing in intra-actions in such an embodied way is not shared by digital slides. Digital slides’ fixity and flatness bears crucial consequences for pathologists’ epistemic practices, as John, another dermatopathologist and long-term user, describes:
The biggest disadvantage is that sometimes the scanner cannot get the section into focus. … Because if …, for example, the tissue is a bit fragmented, then you have different layers of tissue. … One piece is little bit thicker than the other piece, and then the scanner really has trouble getting all the pieces into focus. It focuses on the higher piece and not on the other pieces, for example. And under the microscope, you can migrate through the tissue. … some scanners can also scan multiple planes … you just make [an image with] different layers. And then you can also do this migration through the sections in a scan. But the biggest disadvantage is that you need … a lot of storage.
Digital slides’ affordances are fixed upstream: The scanner, as an enacted epistemic subject, is responsible for making some properties visible and other invisible—once and for all. If pathologists’ seeing rests on the possibility of participating in an intra-action that enacts qualitative detail, digital slides clash with their practices not so much because qualitative detail is ‘absent’, but rather because they are ontologically ‘fixed’ epistemic objects. That is, pathologists can interact with them, zooming in and zooming out, annotating and measuring them with specific software. But they cannot intra-act with them: They cannot harness their affordances to enact properties that were not yet defined.
This points us towards a fundamental characteristic of digital epistemic objects: their ontological closure and their drastically limited possibility for intra-action. The impossibility of intra-acting with digital slides, and of enacting relevant qualitative detail, makes it harder for pathologists to take responsibility for their digital diagnoses—especially in complex cases. As we shall see in the next section, this has to do with the fact that digitization is supported by an apparatus that enacts a nonhuman subject position.
Digital artifacts: Fauxtomated uncertainty
As mentioned above, diagnostic intra-actions rest not only on pathologists’ practices, but also on the correct mounting of glass slides. In imaging-based medical specialties (Cartwright, 1995; van Dijck, 2011), slides are a proxied way of peering into human bodies and the tissue on the slide is manipulated throughout several iterations. Pathologists’ diagnostic practices rely on the (correct) performance of these manipulations: Tissues need to be cut in the right direction, applied on the glass with as few wrinkles as possible, and stained in the correct way. In agential realist terms, this means that the apparatuses underpinning the different intra-actions in the lab’s workflow need to perform consistently.
Deviations from apparatuses’ consistent performativity results in artifacts, ‘artificial structure[s] or tissue alteration[s] on a prepared microscopic slide as a result of an extraneous factor’ (Seoane et al., 2004, p. 113). Artifacts stem from errors in the way the tissue sample is handled since even before the time of excision, all the way through staining and mounting on the slide. Agential realism allows us to consider artifacts as a way of flagging deviations from the way different apparatuses are expected to perform, and the objects they enact are expected to be legible. Epistemic practices also entail identifying and rejecting epistemic objects with artifacts. Doubting whether something is an artifact can make a slide unknowable, as emerged during our interview with Laura:
Laura: Here, I have the impression that this is the vessel … and that there is a tumor in this vessel. But it’s not easy, because there is something called retraction artifacts and then it also looks like a clear space or lumen, so I’m not really sure if this is really a vessel wall with a tumor in it or that it’s just … a fixation retraction artifact, and that the shrinkage of the tissue makes that this looks like an empty space. Carboni: What is a retraction artifact? Laura: [It’s] because of the fixation of the tissue—you need to fix the tissue to be able to make a slide … And when [you fix it], the tissue shrinks, and sometimes this makes it tear a bit. And because this is dense stroma, then sometimes it can shrink or tear and then this looks like a space—but maybe it’s not a real space. But then I can do some immunohistochemical stains to prove if this is a luminal vessel, so lined by endothelial cells, or if this is just stroma. So then if I am in doubt—is it really a vessel or is it just a shrinkage artifact?—then I can do an additional stain to help me with that.
Laura knows that tears in the tissue are a possibility, and what tears would look like on a slide (they could be confused with a luminal vessel). In addition, although it is not always obvious whether a property of a slide is an artifact or not, she is aware of the conditions under which slides can be enacted with a similar artifact (during the intra-action in the grossing room). Crucially, solving this uncertainty means going back to the block, turning it into new slides, and staining them differently. It requires a new, additional intra-action that enables crystallizing different properties.
Glass slides are thus not trustworthy per se—but the intra-actions they undergo are well-known to pathologists, and thoroughly documented in the LIMS. Moreover, these intra-actions involve humans in different roles, both participating in them and checking their results. The quality control step, in particular, constitutes a formal evaluation of the correct processing of the slide. Although it does not always guarantee that the slides, even when enacted ‘correctly’, afford transparent images of diseases, nor that slides get to the pathologists completely free of artifacts, it features actors that can be held accountable for the artifacts that pathologists spot. Pathologists thus not only know the workflow and the semiotic-material apparatus scaffolding slide-making, but they can access the LIMS and identify the assistant pathologists who have performed the quality control and approved that glass slide as suitable for diagnostics. Most of these conditions do not apply where digital slides are concerned.
The affordances of fauxtomatically produced digital epistemic objects thus affect the epistemic practices of professionals and their ability to take responsibility for the knowledge they produce in the diagnostic process. As per Barad, onto-epistemology is also a matter of ethics: It is necessary, as epistemic subjects, to take responsibility for the realities that are enacted and for the ones that are not. However, this also means that one can only fully take responsibility for knowledge when one is meaningfully involved in the intra-action enacting epistemic objects—or, at the very least, when one has sufficient insight into the intra-action and its onto-epistemic consequences. Since fauxtomated intra-actions enact a nonhuman subject, neither of these conditions applies to the creation of digital slides.
This can make digital artifacts particularly tricky business. Some of them, such as the absence of the specimen from the digital slide, are easy to identify for pathologists because they make slides unequivocally illegible, thus clashing enough with the department’s epistemic culture and not generating any uncertainties or questions around epistemic responsibility. Other scanning artifacts, however, are not clear-cut and easy to spot. During our ethnographic observations, we had a chance to witness pathologists’ unease with some of them.
John takes the floor to warn the rest of the team about the risks that switching to digital diagnostics could entail. He explains that, if a biopsy is really small, sometimes the scanner will ignore it. Thus, if they stop distributing glass slides, and pathologists can’t compare digital slides to them, they won’t be able to tell if something is missing from a digital one. ‘Maybe there is a tumor, and you just don’t see it’, he explains. As Harry opens a random digital slide on the IMS, … Jesse exclaims: ‘This is such a good example!’ We look more closely: The tissue sample on the slide is made up by two round shapes next to each other. However, one of these pieces of tissue has very sharp and straight edges—straight in a way in which human tissues don’t grow. Harry zooms in and confirms that, apparently, a spot in the middle of the slide wasn’t scanned. Jesse comments that here you can easily tell that some tissue is missing, but that’s not always the case: ‘You don’t always see that something’s missing. That’s scary.’ No one seems to be able to explain what happened, not even Harry or Robert, the IT experts. It’s even more disconcerting for them because it turns out this slide was scanned in the 250 scanner, the special one for dermatopathology—which is supposed to produce very high-quality digital slides. (fieldnotes, eTeam meeting)
The idea of working fully digitally, and the risk of receiving incomplete digital slides without realizing, is obviously troubling for pathologists. In cases in which the scanners fail to enact parts of the tissue as belonging to the digital epistemic object, pathologists simply cannot know whether epistemically relevant characteristics of the tissue have not been enacted. As we have seen in the previous section, digital epistemic objects radically restrict the possibilities for intra-action: The properties that have not been enacted by the scanner are simply lost.
Fauxtomated intra-actions thus turn out to be problematic on two levels. First, because of the fauxtomation narrative that constitutes the apparatus underpinning them, they enact a nonhuman epistemic subject, preventing the ‘human’ from meaningfully intervening in the enactment and quality control of digital epistemic objects. Neither pathologists nor secretaries have a say in which and how properties of these objects are to be enacted, nor are they tasked to check whether the results of this performativity meet the epistemic requirements of the department. Fauxtomation thus obliterates the possibility of dealing with the uncertainty stemming from automation and its inherent decision-making.
Second, digitization, and its attendant fauxtomated intra-action, embraces a representationalist logic: It assumes relevant information to be intrinsic to epistemic objects, and casts the intra-actions that make up the diagnostic process as a simple matter of zooming in and out. As such, it disregards the performativity of both the apparatus crystallizing specific properties (and not others) in digital epistemic objects, and the performative, embodied engagement with epistemic objects that is the foundation of intra-actions. We can thus think of pathologists’ discomfort with performing diagnoses on digital slides as stemming from the fact that, while excluded from the intra-actions enacting slides’ properties, they are still required to take responsibility for the knowledge they produce based on them. The concluding section elaborates on the consequences of this insight for broader debates on knowing and automation.
Conclusion: Towards a new materialist agenda for digitization
In this article, we have examined digital and non-digital epistemic practices in pathology through an agential realist lens. We considered both digital and glass slides and diagnosis as the result of intra-actions in which knowledge, materialities and narratives are enacted. We thus shed light on ontological, epistemic, and ethical issues that complicate digitization in pathology. Digital and non-digital slides resemble each other but they afford different epistemic practices, since their respective apparatuses incorporate different narratives and make space for differently assembled epistemic subjects. In this section, we elaborate on how agential realism helps us to articulate a post-representationalist, new-materialist agenda for digitization. In concluding, we endeavor to tease out possible ways to materialize the political potential of the Baradian framework in this context.
Agential realism has enabled us to trace the epistemic disruptions produced by digitization back to digitization’s own representationalist assumptions. As we have argued, representationalism plagues digitization efforts whenever epistemic objects are considered self-contained entities, that is, when their properties are presumed to pre-exist their analysis. In our case, the attempt to replace glass slides with digital slides builds on a representationalist logic. It assumes that the relevant data is already present in epistemic objects, ready to be perceived, and that it can be captured satisfactorily without further intervening. This representationalist fallacy has implications for the work of both pathologists and secretaries: For pathologists, it affects the quality of care they can provide; for secretaries, it opens up the possibility of de-professionalization through partial automation. We will articulate these points in turn.
Representationalism casts glass and digital slides as interchangeable—as long as the representation is of sufficient quality. The whole idea of digitization rests fundamentally on this assumption of ontological sameness—or, at least, comparability. At the heart of this is the assumption that both analyzing and reproducing epistemic objects is something that can be done leaving their (presumed) original essence intact. As we have seen, the idea that scanning enables capturing without intervening fails to consider how the capture itself entails the intervention (and latent decision-making) of both scanners and (to varying degree) their secretary. Conversely, here we have teased out the more-than-human decision-making inherent to the scanning process, for instance in the selection of focal points.
Representationalist assumptions ignore not only the epistemic import of (digital) object making, but the material performativity of knowledge making (i.e. diagnosing). We have learned that not all relevant properties have necessarily been enacted in glass slides once they reach pathologists’ desks. Whereas tissues have been enacted as being of a specific color, additional properties, such as the presence or absence of crystal structures, have not been enacted. This taught us how diagnosing entails more than looking, and relevant information crystallizes in the slide through the embodied intra-action involving pathologists and their microscopes.
If the task of pathology is to ‘turn meat into information’, this process of turning is performed in more-than-human, embodied, and organizationally situated epistemic practices. Not considering the epistemic import of these practices increases the degree of uncertainty pathologists experience in the diagnostic process (e.g. has all the relevant tissue been scanned?), and introduces a potential threat to the quality of care provided. The potential false negatives rooted in intra-actions that are either hidden (e.g. the scanner deciding what the specimen is) or missed (e.g. the one involving microscope, pathologist, slide, and potential crystal structures) represent possible sources of error in the diagnostic process. As such, pathologists’ uncertainty and distrust of digital slides proves a crucial, yet by itself insufficient, protective mechanism. Requesting glass slides or additional stains enables them to multiply the number of intra-actions a tissue undergoes. Were this distrust to dwindle, as managers hope, once pathologists become more used to working digitally, the quality of care itself could come under threat—especially when complex cases are concerned.
At the organizational level, representationalism enables specific implementation choices. Casting (high quality) representations as innocent stand-ins for analog epistemic objects leads to two related erasures. First, it obliterates the degree of domain knowledge necessary for enacting good-quality digital objects. Second, it disentangles the knowing and doing that enable digital slides to come into existence. This disentangling serves the myth of fauxtomation, by enabling the obliteration of situated forms of knowing crucial even for allegedly menial tasks, as shown in our analysis of secretaries’ changing work. If the boundaries between humans and nonhumans are not predefined, but emerging within specific practices, the concept of fauxtomation enables us to probe the political potential of agential realism and of its move away from representationalism. It is to this point we now turn.
Social science literature on digitization and automation has long engaged with the question of whether the introduction of increasingly ‘smart’ technologies results in the de-skilling and de-professionalization of the workers operating or engaging with them (Findlay et al., 2017; Petrakaki et al., 2012). Recently, Delfanti and Frey (2021) have produced a compelling argument about the continued cultural acceptability of de-skilling in the context of automation. Our analysis resonates with much of this literature in finding that the work of digitizing is, for a great part, experienced as repetitive and isolating by the ones doing it (cf. Barrett et al., 2012). However, as we have argued, there is no intrinsic reason for fauxtomation to lead to the de-skilling of these workers. Although new-generation scanners’ functionalities and interfaces are conducive to a diminished involvement on the part of the secretaries, excluding them from the enactment of digital slides is a choice. Not making them responsible for the quality control of the digital slides, relinquishing that role to the scanner itself, is, as we argue, a move enabled by the fauxtomation myth. The directionality of the digitalization of (healthcare) work (Campbell & Rankin, 2017; Carboni et al., 2022), enabled by semiotic forces such as fauxtomation, is not always resisted at the level of local implementation policies. As we have shown, not only does compliance with the myth of fauxtomation make the secretaries’ work less meaningful, but it also produces frustration and uncertainty for pathologists. In times of soaring burn-out cases amongst healthcare workers, this might be something to consider more carefully.
Agential realism enables us not only to see the representationalism at the heart of digitization efforts, but also to envision alternatives to it. Starting from intra-action allows us to ask different questions of and for digitization efforts, and to reframe issues of data quality. Embracing the performative nature of diagnosis, and the enacted nature of data, we can see how technical questions (such as the ones around sharpness) fall dramatically short of guaranteeing ‘good’ data. In the case we examined here, the exclusive focus on sharpness fails to give due consideration to the embodied diagnostic practices underpinning pathologists’ certainty—practices connected to and enabled by the situated knowing of other human and nonhuman actors earlier in the workflow. What constitutes ‘good’ data, thus, becomes a question to be considered in the context of specific, interactional epistemic practices and organizational structures.
Conversely, uncritically foregrounding the promises of AI-assisted diagnostics and automation to boost workers’ enthusiasm around innovation (a strategy often suggested in the change management literature, e.g. Chiu, 2018) risks resulting in apparatuses that devalue pre-existing epistemic practices, generating either frustration or downright worse-quality jobs. Based on our analysis, taking seriously the different knowledges that make up epistemic cultures, and investing in supporting them with data (rather than trying to replace them; see Pedersen & Bossen, 2021), would arguably be conducive to improved digitization efforts. The challenge organizations face is thus both how to fruitfully mobilize undervalued domain knowledge, and how to ensure humans agencies are meaningfully included in the enactment of knowledge and materialities.
Similar points have been made in STS and Critical Data Studies (CDS), which have questioned forms of representationalism underpinning digitized knowing (boyd & Crawford, 2012; Stevens et al., 2018). As we have shown, a new-materialist approach contributes to these post-representationalist sensitivities. First, agential realism, and the ethnographic approach it suggests, enables us to examine data enactment at the organizational level with great granularity, tracing less visible moments of knowledge production beyond the boundaries of the diagnostic process narrowly conceived. This includes re-examining instances of more-than-human intra-action as moments of knowledge production—though they might fall outside of the scope of what is usually considered epistemic subjects and practices. Second, and related, agential realism sheds light on how data are enacted in more than-human, organizationally situated practices. Opening up intra-actions as moments of knowledge (and data) production, and as crucial for the diagnostic process, allows us to see the synergies between seemingly disconnected issues such as the automation of menial work, epistemic uncertainty and resistance, and quality of care. Finally, agential realism encourages us to center responsibility as an empirical question in thinking about digitization efforts’ epistemic disruptions. As we have seen, responsibility for data enactment is a relevant focus not only during the diagnostic process, but also at the point of digitization itself. What sort of agential cuts specific implementation policies enable, what sort of subjects they enact, and how those subjects can be held accountable for the realities they co-enact emerge as fundamental questions for researchers and managers alike.
Footnotes
Acknowledgements
We are grateful to the editor and to the two anonymous reviewers, whose generous engagement with our work helped us considerably improve this article. We thank all the participants who contributed to our research at various stages, especially Folkert van Kemenade and King Lam for helping us accessing and navigating our fieldwork. We thank Olsi Kusta for our informal conversations that helped us broaden our perspective on digital pathology beyond the Dutch healthcare system. We are also thankful to our colleagues at the Health Care Governance section of the Erasmus School of Health Policy and Management, and Roland Bal in particular, for providing valuable comments to improve our manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article, and the PhD project of which it is part, was made possible through the financial support of the Medical Delta program Journey from Prototype to Payment, and of the Erasmus School of Health Policy & Management.