
Abstract
Professional musicians are often confronted with multiple profession-related stressors, which may be associated with an increased risk of mental strain, but empirical evidence focusing on clinical samples of musicians is limited. The aim of this study was to examine clinically confirmed mental disorders and personality accentuations in musicians attending a musician-specific outpatient service, to better understand how occupational and person-related stressors may impact their mental health. We performed a cross-sectional secondary data analysis of diagnoses and sociodemographic data of 678 professional musicians (including music students) that were routinely collected in the outpatient clinic. Of the 678 patients, 110 (16.2%) received a tentative psychiatric diagnosis, and 46 presented themselves to the psychiatric outpatient clinic for extensive diagnostics (using ICD-10 and SKID-II). In these 46 musicians, depression (39%) and music performance anxiety (26%) were the most frequent diagnoses, followed by adjustment disorders (13%) and somatoform disorders (11%). Twenty-eight percent of the sample fulfilled the criteria of either a personality disorder or accentuation. The frequency rates emphasize the importance of targeting the mental health of professional musicians with preventive and therapeutic measures. Further research with larger sample sizes is needed to validate and extend our findings and develop individual preventive measures.
Sub-clinical or clinical symptoms of mental disorders—together with musculoskeletal complaints—seem to be the most important work-related reasons for professional musicians to seek medical help (Aalberg et al., 2019; Elam et al., 2022; Fernholz et al., 2019; Fishbein et al., 1988; Loveday et al., 2023; Musgrave, 2022; Vaag, Bjørngaard, et al., 2016; Vaag, Saksvik-Lehouillier, et al., 2016). In this context, musicians’ performance anxiety (MPA) is the most intensively studied mental disorder in musicians, with an estimated mean prevalence between 15% and 25% of the musician population (Fernholz al., 2019), whereas other mental disorders have been investigated in only a few studies to date. These studies predominantly utilized screening instruments to gauge symptoms rather than relying on professionally diagnosed disorders in musicians and often compared findings with general population samples. Such comparisons serve as a backdrop, providing a broader context to understand the overall landscape of psychopathological symptoms among musicians and indicating symptom clusters and stressors that might be particularly relevant in musicians, but should be interpreted with caution due to confounds and a lack of direct comparability.
A cross-sectional study from Norway (Vaag, Bjørngaard, et al., 2016) compared scores on the Hopkins Symptom Checklist in professional musicians (n = 1,067 members of the Norwegian music union) with a sample of the general workforce. The results indicated a 10% higher prevalence rate of psychological distress (symptoms of anxiety and depression) in musicians (18% vs. 8%). Additionally, in some studies, symptoms of sleep disorders (Vaag, Saksvik-Lehouillier, et al., 2016), eating disorders (Kapsetaki & Easmon, 2019), positive and negative schizotypal traits, and bipolar disorders (in rock musicians (Mason et al., 2005)) were more prevalent in musicians than in the general population. A survey of n = 377 Australian professional orchestra musicians, using self-report screening instruments (thus not constituting clinically confirmed diagnoses), found high rates of symptoms of social anxiety disorder (33%), posttraumatic stress disorder (22%), and depression (32%) (Kenny et al., 2014). On average, women reported higher psychological distress than men (Kenny et al., 2014; Vaag, Bjørngaard, et al., 2016); soloists, vocalists, keyboard, and string players in the genre of classical music showed the highest levels (Vaag, Bjørngaard, et al., 2016). Younger individuals tended to be more affected by MPA than older musicians (Kenny et al., 2014), and a substantial number of musicians drank more alcohol than recommended by national guidelines (Kenny et al., 2014). In a study in Brazil (n = 230) professional musicians were more affected by MPA (examined with a self-report scale) than amateur musicians (Medeiros Barbar et al., 2014). A study in the Netherlands (n = 64) using brief self-report instruments found symptoms of depression and anxiety in 39% of the examined professional musicians and in 61% of the music students; a lower degree of resilience was associated with more pronounced psychopathological symptoms (Kegelaers et al., 2021). Furthermore, musicians (particularly rock musicians) were observed to have an elevated use of substances and psychotropic medications, as well as (especially among vocalists) increased attendance at medical facilities and psychotherapy (Vaag, Bjørngaard, et al., 2016).
The first and, to our knowledge, only study focusing on a clinical sample of musicians has been conducted in the Netherlands (Van Fenema et al., 2013). Musicians who presented themselves to the outpatient clinic for psychiatric disorders in professional musicians, dancers, and actors at Leiden University Hospital were examined according to the criteria of DSM-IV. Of 50 patients, 41 were diagnosed with a former axis-I-disorder according to DSM-IV (all mental disorders except personality disorders and intellectual development disorders); the most frequent diagnoses were mixed anxiety and depressive disorder (20%), followed by unipolar depressive disorders (12%), and anxiety disorders (8%).
The authors are not aware of any study examining clinically diagnosed personality disorders (PD) in musicians. Yet, the only study focusing on PD in a professional group of performing artists was performed on professional actors using the Coolidge Axis-II inventory (Davison and Furnham, 2018). Actors scored significantly higher on narcissistic, borderline, histrionic, antisocial, and obsessive-compulsive personality disorders compared to a general population sample in the United States.
In contrast to personality disorders, personality traits—and their associations with mental disorders—are the focus of many studies (mainly with non-musician samples) (Bucher et al., 2019; Ormel et al., 2013). A meta-analysis examining major personality traits found that individuals with anxiety, depression, or substance use disorders scored high on neuroticism and low on conscientiousness (Kotov et al., 2010). Patients with social anxiety disorder and dysthymia scored low on extraversion; substance use disorders were related to higher disinhibition and disagreeableness (Kotov et al., 2010).
Several studies examined personality traits in musicians; the outcomes were heterogeneous, presumably due to differences in measuring instruments, studied population groups (e.g., instrument groups, music genres), and control groups (Gjermunds et al., 2020). A pioneer of the examination of musicians’ personality traits, the British psychologist Anthony Kemp (1996) described musicians as intelligent, introvert, anxious, and affectious, using Cattell and Eysenck’s questionnaire, postulating a “potential musical temperament”. Except for the trait of introversion, Mihajlovski (2016) confirmed Kemp’s findings by comparing musicians and non-musicians using different questionnaires. A Norwegian study using the five-factor model found increased levels of neuroticism and introversion (instrumentalists), greater openness to experience (singers), and lower levels of conscientiousness in musicians compared to a general workforce sample (Vaag et al., 2018). Turkish researchers compared the personality traits of music and art students: Music students reported higher scores for anxiety, negative self-concept, and neuroticism than art students (Yöndem et al., 2017). Van Fenema et al. (2013) screened musicians in an outpatient clinic with the self-report short form of the Dimensional Assessment of Personality Pathology-Basic Questionnaire (DAPP): The musician outpatient group showed significantly higher scores on the narcissism scale than other outpatients and non-patient controls. Personality styles seem to have a significant influence on how stressful musicians perceive their own work (Aalberg et al., 2019). Additionally, MPA is, among other factors, correlated with higher neuroticism, perfectionism, and extraversion (Butković et al., 2022; Kenny & Holmes, 2015; Langendörfer et al., 2006).
Some of the main causes for a potentially increased risk of (sub-)clinical psychopathological symptoms in professional musicians (rather than any inherent susceptibility or vulnerability) are work-related stress and musician-specific biographical aspects, that is, irregular working hours, frequent travels, financial insecurities, and high levels of competitive pressure (Musgrave, 2022; Musgrave & Gross, 2020; Newman et al., 2022). Additionally, starting musical training at a young age and social isolation due to many hours of practicing alone can be burdensome and can lead to physical overuse syndromes and pain, which in turn enhances the risk of depressive symptoms (Kenny & Ackermann, 2009).
While the existing research on psychopathological symptoms and personality accentuations in musicians is mainly based on brief self-report questionnaires, there is a significant need for information regarding more comprehensive diagnostics conducted by mental health professionals for greater validity and reliability. Additionally, previous studies often focused on single disorder categories, such as anxiety or depressive disorders, without considering the full spectrum of mental disorders. This gap underscores the necessity for an integrative approach to understanding the range of mental disorders in musicians. Accordingly, our study aims to provide a more holistic assessment by systematically examining a sample of musicians who sought support at our musician-specific outpatient service, with regard to clinical diagnoses. Thus, our core research question is: What specific patterns of professionally diagnosed mental disorders and personality accentuations are observed in musicians who seek support at an outpatient clinic? Additionally, we aim to explore the differences between musicians who completed the recommended full psychiatric examination and those who did not follow through with the referral. A crucial aspect of our research is establishing a foundation for comparisons with other (outpatient) groups, aiming to illuminate the unique mental health challenges faced by musicians and to inform the development and adjustment of tailored preventive and therapeutic strategies. Understanding the patterns of mental disorders in musicians seeking support, and examining the extent to which these differ from other populations, is essential for optimizing mental health care for this specific group.
Method
Study design, setting, and study population
We performed a cross-sectional secondary data analysis of diagnoses and sociodemographic data that were routinely collected during assessments of professional musicians (including music students) in outpatient medical care during the period from May 2015 to July 2019. No later data was examined due to possible bias emerging from the COVID-19 pandemic. Informed consent about data processing for scientific reasons was routinely obtained from all in- and outpatients at Charité – Universitätsmedizin Berlin. All data were analyzed anonymously. According to statutes of the ethics committee of the Medical Faculty of Charité – Universitätsmedizin Berlin (2019), secondary data analyses do not require ethical approval according to national guidelines (e.g., Regulation [EU] 2016/679 [General Data Protection Regulation], Official Journal of the European Union, 2016)).
The sample of musicians in outpatient care is drawn from the consultation hour of a specified center for musicians that unites various medical and therapeutic experts who are very familiar with the specific health needs of musicians due to having a musical background themselves and/or distinct experience in the treatment of musicians. The outpatient service operates as a part of the Department of Audiology and Phoniatrics at a large university hospital. Musicians access the specialized outpatient service through various pathways. Some find the service through active online searches, while others are referred by general practitioners, specialist physicians, or academic institutions, such as conservatories or music schools. Additionally, professional societies, labor unions, and directories of healthcare services also serve as referral sources, guiding musicians to the consultation hour. In the special consultation hour, musicians can present their current medical problems and receive individual consultation and treatment. Further examinations and therapeutic measures are coordinated and, if necessary, patients are referred to other specialists—within the established expert network for musicians.
The patient sample from the special consultation hour consisted of 678 individuals. Of these, 110 received the tentative diagnosis of a psychiatric disorder. These tentative diagnoses were made by a non-psychiatric physician of the specialized outpatient service using the criteria and checklists based on the ICD-10 (10th revision of the International Classification of Diseases). Of the 110 musicians with a tentative psychiatric diagnosis, 46 musicians presented themselves to a special psychiatric consultation hour for musicians, where they underwent a comprehensive diagnostic procedure.
These 46 musicians represented the final sample for detailed descriptive and inferential statistical analyses. Reasons for not pursuing the recommended full psychiatric examination at the psychiatric consultation may have included personal doubts and aversions, concerns about stigma, time constraints, and already having alternative psychiatric or psychotherapeutic care opportunities. Additionally, there may be unknown factors influencing the decision to forego further diagnostic evaluation, reflecting the complexity of individual circumstances among musicians in specialized outpatient care.
Diagnostic tools
In the psychiatric consultation hour, a detailed diagnostic assessment according to ICD-10 was performed by a licensed psychiatrist. If a personality accentuation or disorder was suspected, the SKID-II was additionally carried out. The SKID-II (Fydrich et al., 1997) is a two-step diagnostic instrument for the ten personality disorders on Axis-II of the DSM-IV; consisting of a self-report part (questionnaire completed by patients) and a professional-guided semi-structured interview. In addition to the categorical diagnosis of personality disorders, the results of the SKID-II can also be interpreted as dimensional expressions of personality traits. The more diagnostic criteria are met, the greater the expression of the corresponding personality characteristics, and the stronger an individual exhibits a tendency toward an accentuated personality or a manifest personality disorder. In our study, a personality accentuation was diagnosed when only one criterion for a personality disorder was missing or not completely fulfilled. The SKID-II is among the most established and widely used instruments for diagnosing personality disorders in clinical psychology, psychotherapy, and psychiatry; with interrater reliability of Cohen’s κ = .48–.98 and internal consistency of Cronbach’s α = .71–.94, satisfactory reliability is given (Maffeit al., 1997); its psychometric properties are satisfactory in terms of reliability, applicability, and efficiency (First et al., 1997; Fydrich et al., 1997).
Statistical analysis
Descriptive statistical analyses were performed to describe the sample and to determine the frequency of mental disorders among the assessed musicians. Furthermore, inferential chi-square tests were used to examine differences between female vs. male musicians regarding the prevalence rates of affective disorders, anxiety disorders, and personality accentuations/disorders (not for other mental disorders due to small sample sizes). In addition, differences between individual instrument groups (string vs. keyboard instruments) and current musician status (university/college student vs. professional musician) were tested by chi-square tests. There were no missing values. A significance level of α = .05 was set for all chi-square tests. All analyses were performed using IBM SPSS Statistics Version 28.0 (IBM Corp., Armonk, NY, USA).
Results
Sociodemographic characteristics and somatic concerns
Of the total 678 musicians who sought assistance from the specialized outpatient service due to somatic and/or mental health concerns, 47.7% identified as male, 52.1% as female, and 0.2% as other; their age ranged from 18 to 80 years (M = 34.64, SD = 15.40). The most frequently played instrument groups were string (38.9%) and keyboard instruments (21.9%); the majority of the sample (82.3%) identified themselves as belonging to the genre of classical music. Chronic pain (chronic myofascial pain syndrome) represented the most common reason for consultation, followed by acute pain due to overuse and trauma. Neurological conditions (such as nerve compression syndromes and focal dystonias), hearing impairments, voice disorders, orthodontic conditions, and dermatological complaints (e.g., contact allergies and hyperhidrosis) were other somatic reasons for seeking care. Accordingly, musicians were frequently referred to specialists in orthopedics, neurology, audiology/phoniatrics, rheumatology, physiotherapy, orthodontology, and dermatology. A subsample of 110 (16.2%) individuals received a preliminary diagnosis of a mental disorder, resulting in a referral for a full psychiatric evaluation and psychotherapeutic treatment. Of this subsample with tentative diagnosis, 52.7% identified as male, 47.3% as female, and the average age was M = 34.64 years (SD = 11.90; range: 18–58).
Detailed sociodemographic for the final subsample of 46 musicians, who underwent the full psychiatric examination, is presented in Table 1. Age ranged from 20 to 58 years (M = 34.54, SD = 11.80); 58.7% identified as male, and 41.3% as female. About half of the sample (52.0%) were from Germany, the other 48.0% from 17 different other countries.
Sociodemographic Characteristics of Musician Outpatients With Clinically Confirmed Diagnoses (After Attending Full Psychiatric Examination) of a Mental Disorder (N = 46).
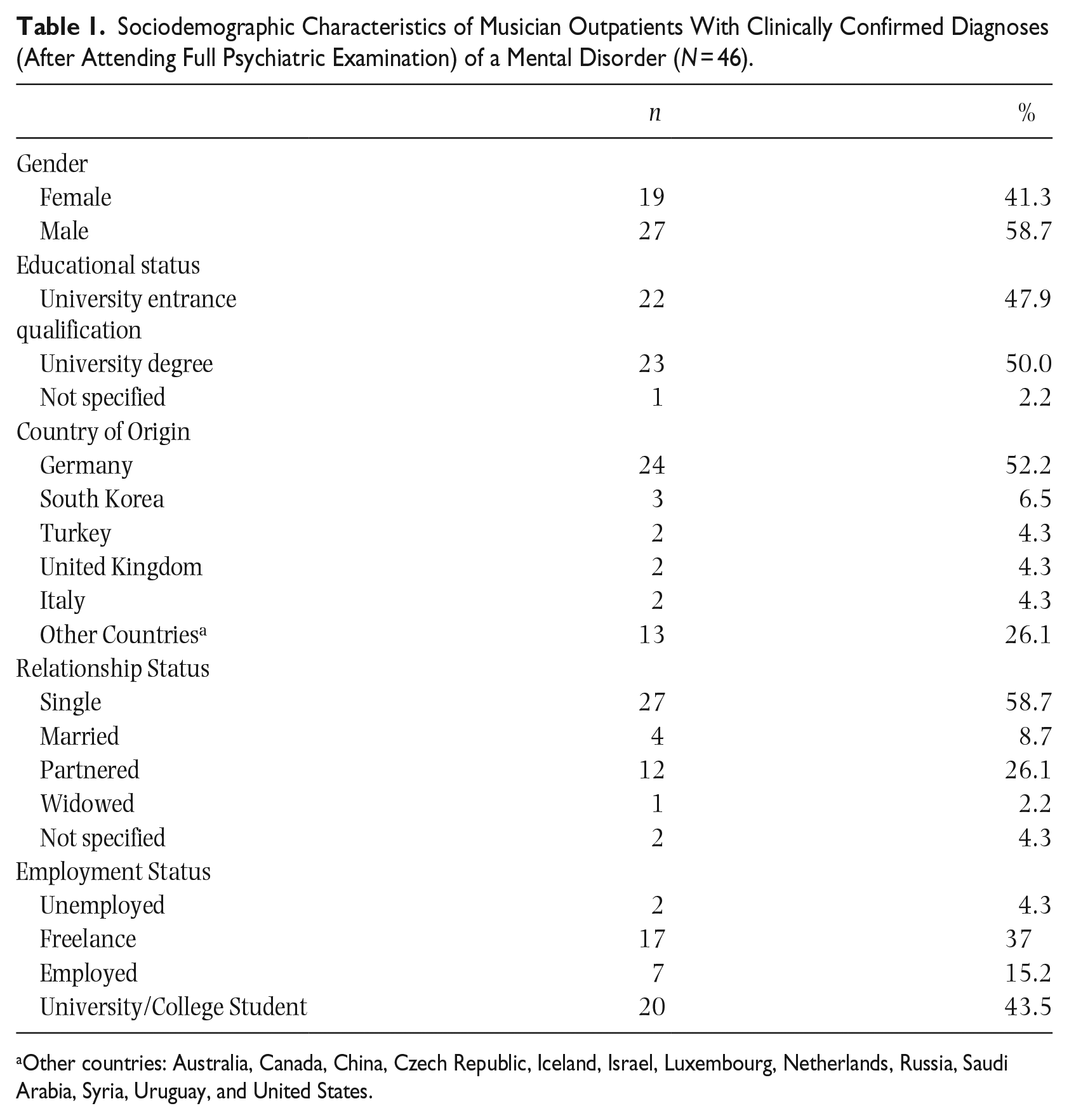
Other countries: Australia, Canada, China, Czech Republic, Iceland, Israel, Luxembourg, Netherlands, Russia, Saudi Arabia, Syria, Uruguay, and United States.
Table 2 depicts music-/profession-related information of the musician outpatients with tentative diagnoses (after attending preliminary assessment; N = 110) or clinically confirmed diagnoses (after attending full psychiatric examination; N = 46) of a mental disorder. 43.5% of the 46 musicians were students studying at a music conservatory; 37.0% worked as freelancers and 15.2% were employed. The majority (82.6%) identified themselves as in the genre of classical music; the most frequently represented instrument groups were string (37.0%) and keyboard instruments (21.7%). There were no marked differences in the relative proportions between individuals with a tentative diagnosis and those whose diagnosis was confirmed following the full psychiatric assessment.
Musical Characteristics of Musician Outpatients With Tentative Diagnoses (After Preliminary Assessment) or Clinically Confirmed Diagnoses (After Attending Full Psychiatric Examination) of a Mental Disorder.
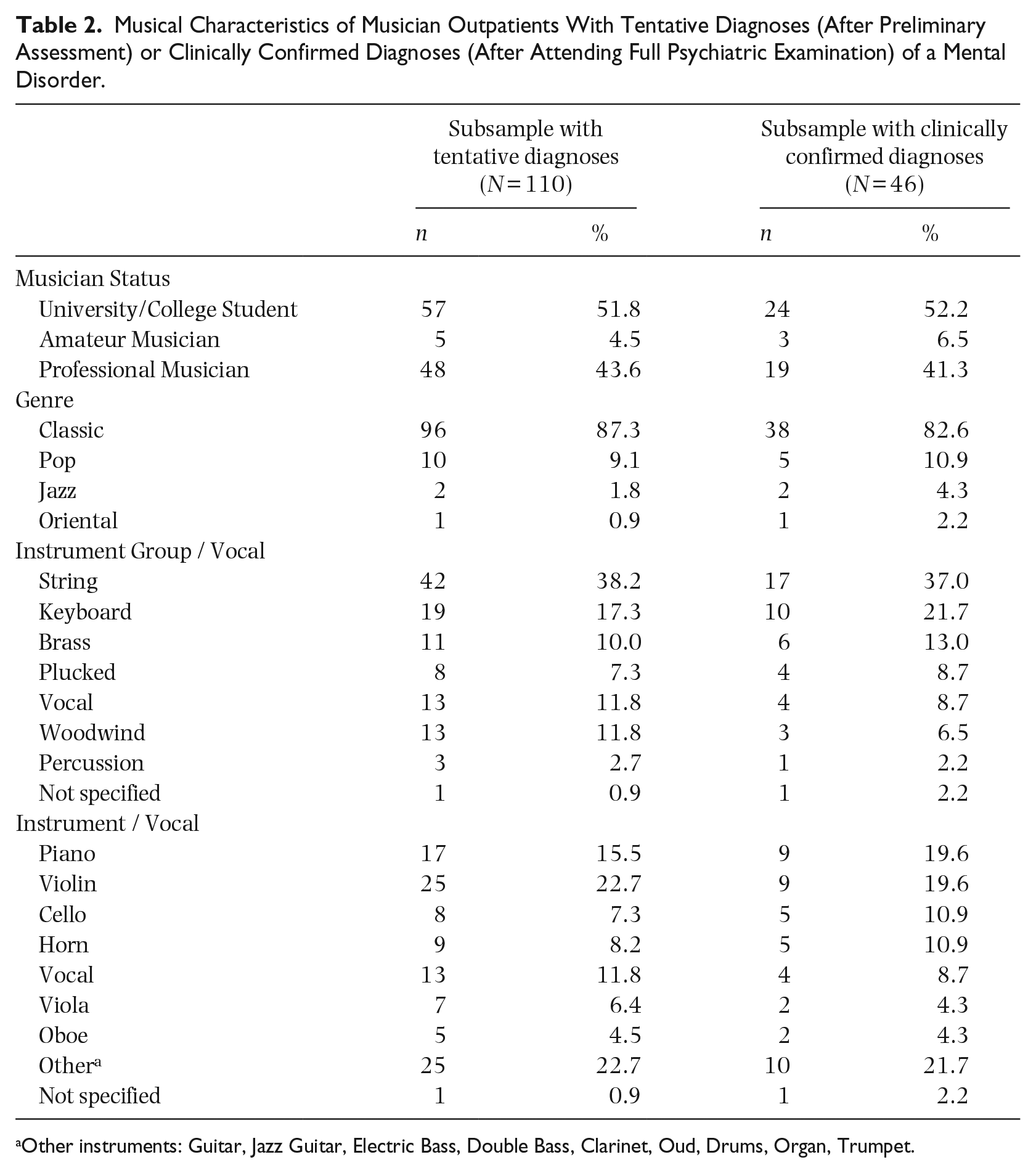
Other instruments: Guitar, Jazz Guitar, Electric Bass, Double Bass, Clarinet, Oud, Drums, Organ, Trumpet.
Frequency of mental disorders
Of the total of 678 musicians, 110 (16.2%) received the tentative diagnosis of a mental disorder (by a non-psychiatrist physician). The most common predictions were anxiety disorders, depressive disorders, and somatoform disorders (see Table 3).
Prevalence of Mental Disorders Among Musician Outpatients With Tentative Diagnoses (After Preliminary Assessment) or Clinically Confirmed Diagnoses (After Attending Full Psychiatric Examination) of a Mental Disorder.
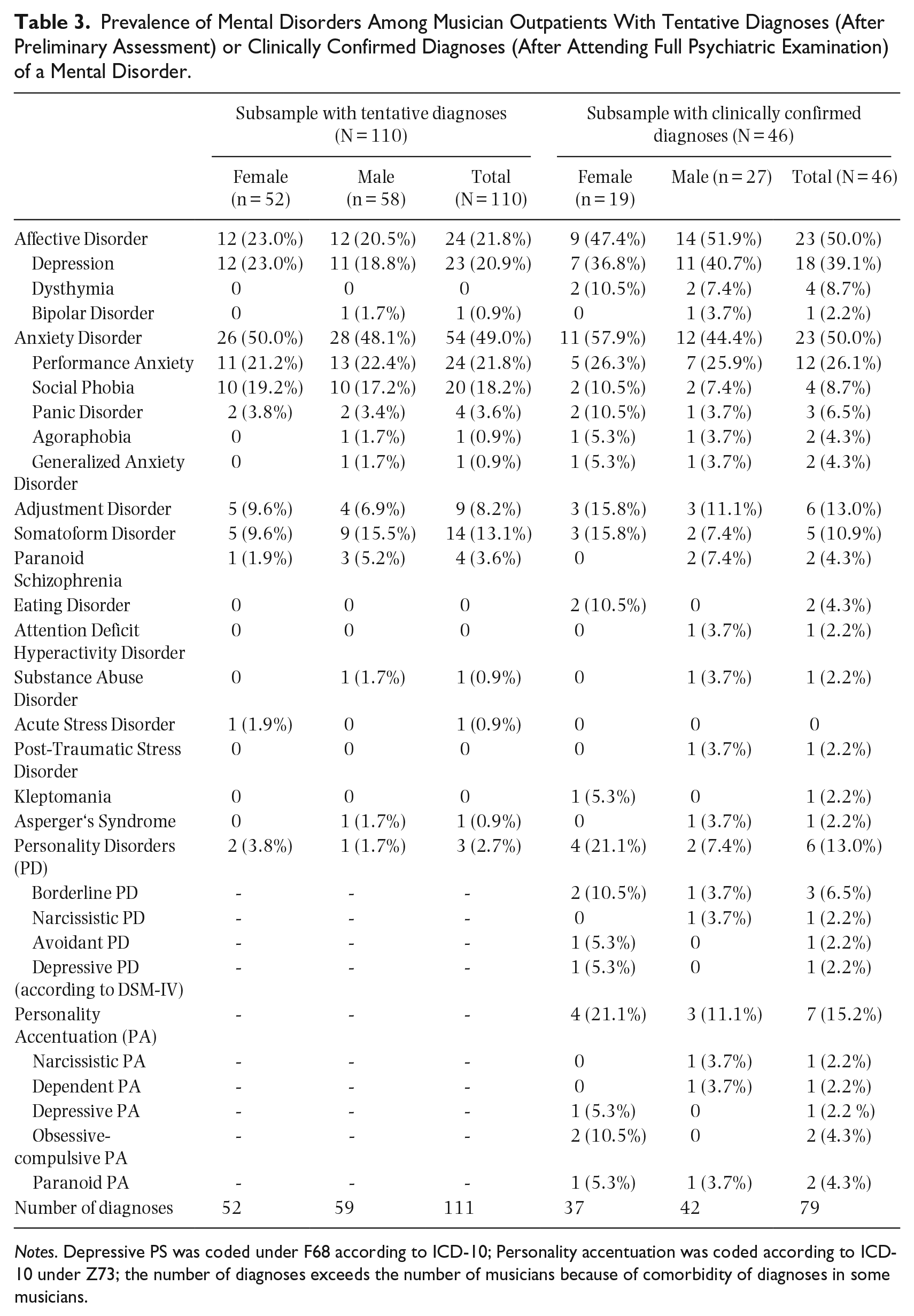
Notes. Depressive PS was coded under F68 according to ICD-10; Personality accentuation was coded according to ICD-10 under Z73; the number of diagnoses exceeds the number of musicians because of comorbidity of diagnoses in some musicians.
All of the 46 musicians who attended the full psychiatric examination (41.8% of the 110 musicians who were referred for further psychiatric examination) were diagnosed with at least one mental disorder. A total of 79 diagnoses were given, and two or more mental disorders were diagnosed in 41.3% of the patients. The most frequently assigned diagnoses were affective disorders and anxiety disorders (see Table 3). Among affective disorders, major depression, dysthymia, and recurrent depressive disorders were the most frequent diagnoses. Whereas male musicians showed a slightly higher rate of affective disorders, female musicians were more often affected by anxiety disorders. MPA represented the most frequent diagnosis, followed by social anxiety disorder, adjustment disorders, and somatoform disorders. Chi-square tests found no significant differences in the distribution of mental disorders between genders (affective disorders: χ² = 0.900, p = .765; anxiety disorders: χ² = 0.807, p = .369).
Overall, the comparison between tentative and clinically confirmed diagnoses (Table 3) reveals a pattern where common mental disorders like affective disorders and anxiety disorders were more frequently confirmed, whereas the more complex or less prevalent conditions show a discrepancy between initial prediction and final clinical confirmation.
Frequency of personality disorders and accentuations
A total of 28.2% of the musician sample showed either a personality disorder (13.0%) or a personality accentuation (15.2%; if only one criterion for a personality disorder was missing or not completely fulfilled). A higher percentage of women than men exhibited personality disorders (21.1% vs. 7.4%) and personality accentuation (21.1% vs. 11.1%), but this difference did not reach statistical significance (χ² = 3.062, p = .080). While this section provides a descriptive overview of the distribution of personality disorders/accentuations, it should be regarded only as a very rough impression and interpreted with caution due to the very small sample sizes. Borderline personality disorder was the most frequent diagnosis; narcissistic, avoidant, and depressive personality disorders were each identified once. The prevalence of personality accentuations was also higher in female musicians than in male musicians. The obsessive-compulsive personality accentuation was most frequently diagnosed in female musicians followed by depressive and paranoid personality accentuations. In men, narcissistic, dependent, and paranoid personality accentuations were observed.
Chi-square tests detected no significant differences in the distribution of diagnoses depending on musician status (student vs. professional musician; affective disorders: χ² = 004, p = .952; anxiety disorders: χ² = 4.207, p = .053) and the two largest instrument groups (string instruments vs. keyboard instruments; affective disorders: χ² = 0.004, p = .952; anxiety disorders: χ² = 0.556, p = .456).
Clinical characteristics
Approximately one-third of the musician outpatients had at least one somatic disorder comorbidly with a mental disorder (Table 4).
Clinically Relevant Characteristics of Musician Outpatients With Clinically Confirmed Diagnoses (After Attending Full Psychiatric Examination) of a Mental Disorder (N = 46).
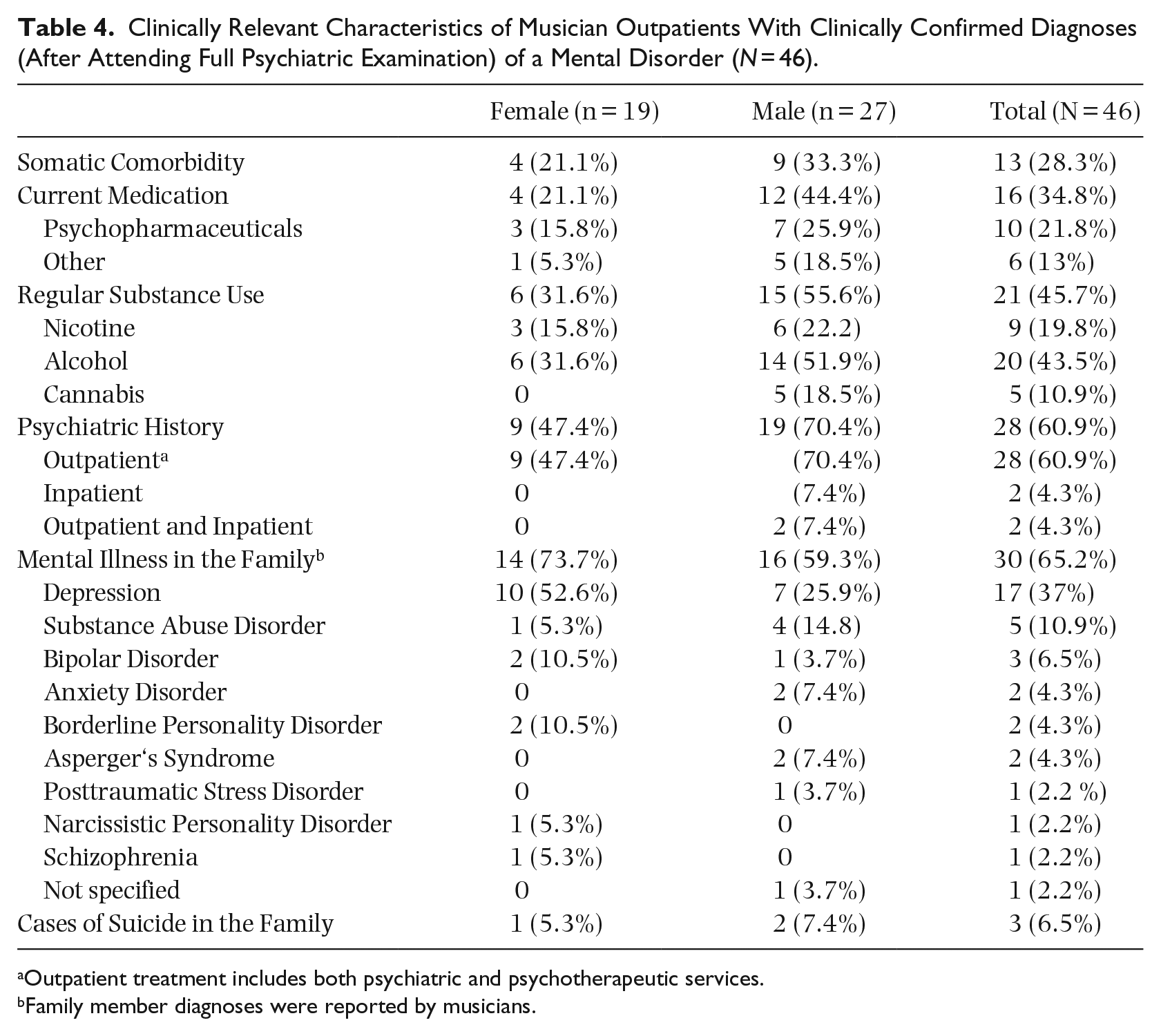
Outpatient treatment includes both psychiatric and psychotherapeutic services.
Family member diagnoses were reported by musicians.
About one-third received regular medication; most of the medication was to treat mental disorders. About half of the patients regularly consumed substances, mainly alcohol, followed by nicotine and cannabis. Men, on average, reported a higher substance use compared to women. Furthermore, half of the group had a psychiatric medical history and had received a minimum of outpatient treatment in the past. According to self-reported data, two-thirds of the musicians had mental disorders in their family history; depression (37.0%) and substance use disorders (10.9%) were most frequently reported. None of the reported frequencies of clinical characteristics differed significantly between genders.
Discussion
Summary and interpretation of the results
Our study aimed to investigate the frequency of mental disorders (with particular consideration of personality disorders and accentuations) in musicians who presented themselves to the outpatient service of a specialized consultation hour for musicians due to physical or psychological concerns. A total of 16% of the musicians in the outpatient clinic received the tentative diagnosis of a psychiatric disorder (Axis 1 according to DSM-IV). Notably, this rate is lower than the self-reported rates of anxiety and depression symptoms found in screening instruments among a sample of musicians in the general population in Norway (18%; Vaag, Bjørngaard, et al., 2016). This discrepancy may emphasize the importance of not conflating self-reported symptoms from screening instruments with manifest disorders.
Applying the diagnostic criteria of ICD-10 for mental disorders and SKID-II for personality disorders, affective disorder (39%) and MPA (26%) occurred to be the most frequent diagnoses in our outpatient sample of 46 musicians, followed by adjustment disorders (13%) and somatoform disorders (11%). Regarding the frequency of affective and anxiety disorders, there seem to be no substantial differences between the musician sample and a US-American psychiatric outpatient sample, except for a higher frequency of MPA (Zimmerman et al., 2005). Somatoform disorders were twice as prevalent in our musicians’ group compared to this clinical sample (11% vs. 6%); adjustment disorders were three times as prevalent (13% vs. 4%) (Zimmerman et al., 2005). With regard to the prevalence of MPA in musicians, our results support the self-reported estimations of Fernholz et al. (2019) and the observations in a clinical setting by Van Fenema et al. (2013). Regarding depression (12%), anxiety disorders symptoms (8%), anxiety and depression mixed (20%), and somatoform disorders (2%), Van Fenema et al. (2013) found lower prevalence rates. This may be partially explained by the fact that our final cohort was already filtered and had already passed a low-threshold service. Thus, more severely affected individuals presented at our psychiatric outpatient clinic.
In a representative probability sample of 3815 adults in Spain who presented at a primary care unit due to somatic or psychological complaints, 45% had experienced at least one mental disorder in their lifetime (according to structured clinical interviews), and 30% in the past year, with high comorbidity rates (Serrano-Blanco et al., 2010). Compared to this primary care sample, our musician outpatient sample presented with slightly lower rates of mental disorders while the pattern of diagnoses was similar, with depressive and anxiety disorders being the most common.
Due to a lack of further comparable non-musician-specific outpatient samples, we additionally draw on findings from large general population samples in Germany and Europe as a basis for a preliminary contextualization of our results. An overview and reanalysis of epidemiological studies conducted in the European general population (not restricted to outpatient or otherwise specialized samples) yielded an estimated 12-month prevalence rate of 38% of mental disorders (Wittchen et al., 2011). In a study in the German general population, a total of 28% exhibited mental disorders in the past 12 months (Jacobi et al., 2016). Though these prevalence rates, at first sight, seem higher than in our musician outpatient sample, it is not possible to conclude if musicians are more or less affected by mental disorders than the general population—due to methodical limitations and a lack of comparability of different studies (e.g., with regard to professional observation vs. self-report, prevalence intervals, etc.). The prevalence rates observed in individuals who have actively sought medical (or specific psychiatric evaluation) may be inherently higher due to self-selection.
Van Fenema et al. (2013) hypothesized that musicians have a higher prevalence of mental disorders than the general population but are less burdened compared to other psychiatric outpatients. A possible reason for the latter finding could be that musicians may seek medical support earlier than other outpatient groups because they often need to maintain a very high level of functioning to perform in their profession (Vaag, Bjørngaard, et al., 2016; Van Fenema et al., 2013). Thus, mental burden might be detected earlier, potentially stopping the progression into manifest mental disorders.
All 46 musicians with tentative mental disorders who attended the psychiatric outpatient clinic for a comprehensive diagnostic received a final diagnosis of at least one mental disorder. Thus, it is plausible to assume that in the majority of the 64 individuals who did not follow-up with the referred full psychiatric assessment, mental disorders would also have been confirmed. Furthermore, for a few more complex and less prevalent conditions, a discrepancy between initial prediction (by a non-psychiatrist physician) and final clinical diagnoses (by a psychiatrist) may have occurred. This underscores the importance of thorough psychiatric evaluation to differentiate between similar syndromes, transient symptoms, and persistent psychopathology and suggests that initial presentations (and non-psychiatric evaluations) may not meet the rigorous criteria for a confirmed diagnosis.
In contrast to typical findings in psychiatric outpatient settings (Zimmermant al., 2005), in our sample men were slightly more frequently affected by affective disorders than women. Among other reasons, this may possibly be attributable to differences in support-seeking behavior. Women, on average, might tend to seek professional psychiatric-psychotherapeutic support more rapidly (e.g., ambulatory psychotherapy) in the case of psychopathological symptoms. Thus, they may not have had further reason to present themselves at the outpatient clinic and were therefore not included in our sample. Men, in contrast, might tend to wait and only seek professional support in case of aggravation and chronification of symptoms (Harris et al., 2016). As a result, men might have been overrepresented in our sample. Nevertheless, considering the small sample size, these quantitative differences should not be overinterpreted.
A total of 40% of our musician sample regularly consumed substances and one male musician was diagnosed with a substance use disorder. The consumption of alcohol (52% vs. 32%) and cannabis (19% vs. 0%) was more common among male than female musicians, which is consistent with both observations in the general population and in psychiatric patients (Toftdahl et al., 2016). Regular and heavy substance use among musicians is a major risk for mental and physical health; frequently substances—especially alcohol—are used to cope with distress and psychopathological burden (Forsyth et al., 2016; Kenny et al., 2014; Stormer et al., 2017; Vaag, Bjørngaard, et al., 2016). Thus, it is important to raise awareness regarding the risks of substance use in musicians.
No significant differences occurred with regard to the frequency rates of affective and anxiety disorders in music students versus professional musicians and those playing string vs. keyboard instruments. This suggests that there is not a narrow specific group within musicians that needs particular mental health support but again the small sample sizes should be borne in mind.
A total of 13% of our musician sample fulfilled the criteria of a personality disorder (borderline, narcissistic, avoidant, and depressive personality disorders), and 15% the criteria of a personality accentuation (narcissistic, dependent, depressive, obsessive-compulsive, and paranoid accentuation). This lies within the range of point prevalence rates from the general population, which ranged from 10% to 15% in a review by Fiedler (2018). Among our musician sample, borderline personality disorder represented the most frequent personality disorder (7%) with a slightly lower point prevalence than in other psychiatric outpatients (9%; Zimmerman et al., 2005). Moreover, in clinical samples of psychiatric outpatients, the estimated prevalence rates of personality disorders were often substantially higher (45% - 51% for any personality disorder) (Beckwith et al., 2014). Most commonly diagnosed in these samples were former Cluster-C (22%; DSM-IV: anxious-avoidant, dependent, and obsessive-compulsive PD) and Cluster-B personality disorders (13%; antisocial, narcissistic, histrionic, and borderline PD; Zimmerman et al., 2005). In our musician sample, personality disorders and accentuations belonged most often to Cluster-B. This, for instance with regard to narcissistic personality, corresponds with findings by Van Fenema et al. (2013) who found significantly higher scores on the Narcissism Scale of the DAPP-SF in musician outpatients than in other outpatients and non-patient controls. Narcissistic traits may have beneficial effects on the music business (e.g., appearing self-confident and strong). Similar to Davison and Furnham’s (2018) study of professional actors, Cluster-B personalities were predominant, that is, borderline and narcissistic personalities, followed by Cluster-C, obsessive-compulsive, anxious-avoidant, and dependent personalities. Paranoid personality symptoms (Cluster-A) were found less frequently in actors. Among our musician sample, paranoid accentuation was only evident in two individuals (4%) and represented the only diagnosis from Cluster-A. Lower rates of personality disorders and personality accentuation in musicians might be partially explained by the high demands of their profession which make it less likely to succeed with a music career in case of a severe personality disorder. Nonetheless, it might also be a methodological artifact (e.g., due to confounds, sampling bias, underpowered sample sizes, stigma-related underreporting, or variability in diagnostic criteria and assessment methods).
Limitations and future research
Our study is a cross-sectional observational study, and thus it is not possible to draw any causal conclusions. Some previous research suggests that mental strain in musicians is the result of working as a professional musician rather than an inherent trait (Loveday, 2023), whereas a twin study with 5648 Swedish twins concluded that psychopathological symptoms in musicians may be partly explained by a preexisting genetic risk for affective disorders (Wesseldijk et al., 2022). In the future, longitudinal studies are desirable to clarify these ambiguities and hypotheses. Another limitation of our study is the small sample size which limits the statistical power and informative value of our findings. Maybe, in a larger sample, differences between subgroups—for example, female vs. male musicians; music students vs. professional musicians—would have reached statistical significance. Furthermore, the generalizability of our results is limited because we mainly examined classical musicians, especially keyboard and string players. Additionally, our study examined a narrowly selected sample, impacted by multiple layers of selection processes. The initial layer stems from self-selection, where the sample comprises only those musicians who actively sought assistance for physical and/or psychological issues at our outpatient service specialized in musicians’ health. As a consequence, our sample is likely not representative of all musicians; particularly skewed toward those more inclined to seek help or experiencing more severe symptoms A subsequent layer involves professional selection bias at the referral stage for a comprehensive psychiatric assessment. Here, only those musicians who received a preliminary diagnosis and exhibited at least moderate psychopathology were chosen for further evaluation. The third layer of selection bias is related again to self-selection. Not all individuals referred for the complete psychiatric assessment participated. This further skews our sample and may result in the findings not fully capturing the spectrum of psychopathological symptoms among musicians, especially those with milder symptoms or those less inclined to pursue or who were not referred for clinical evaluation.
The reasons why only 46 out of 110 patients with suspected mental disorders sought treatment at the psychiatric outpatient clinic likely encompass personal and external barriers as well as some individuals already receiving alternative outpatient or inpatient psychiatric/psychotherapeutic care (Heinig et al., 2021; Waumans et al., 2022). As a limitation, it is not possible to precisely disentangle and quantify these reasons.
Practical implications and recommendations
Associated with personal barriers, stigma might be relevant: Despite worldwide efforts to reduce it, psychiatric diagnoses still carry a stigma that could discourage patients from seeking help from mental health specialists (Heinig et al., 2021; Waumans et al., 2022). Individuals in public-facing roles may sometimes be particularly averse to stigma (Herman & Clark, 2023; Van Fenema et al., 2013). Therefore, campaigns aimed at promoting greater tolerance toward mental disorders among professional musicians, as has gradually been established in elite sports, could be of significant importance (Ströhle, 2023).
The estimated frequency of 16% (tentative) mental disorders emphasizes the relevance of targeting musicians with appropriate preventive and therapeutic support. Beyond the generally very prevalent and therefore notably relevant depressive and anxiety disorders, somatoform disorders might warrant special consideration due to their seemingly elevated prevalence within the musician outpatient sample. Although not found in our data, it would be sensible, given the evidence from other research (Kegelaers et al., 2021; Musgrave, 2022; Niarchou et al., 2021; Visser et al., 2022), showing that music students often exhibit particularly high levels of mental strain, to start adaptive strategies as early as possible (e.g., support opportunities in institutions like conservatories and universities).
Based on our data as an initial foundation, it could be beneficial to conduct more comprehensive assessments of personality styles among musicians. This would allow for tailored interventions and coping strategies to be designed specifically for this group. Additionally, directing attention toward the potential maladaptive expressions of personality traits and promoting adaptive traits may help mitigate the risk of developing mental disorders.
Future studies with larger and more heterogenous samples which better represent the whole population of musicians are needed to verify and extend the results. Further, the diagnostics in future research should be adapted to the current classification systems: DSM-5 and soon ICD-11. Moreover, additional relevant variables should be included, e.g., dimensional aspects of psychopathological symptoms; preferably using established and well-standardized instruments.
Conclusion
The present study provides an initial overview of the frequency of clinically diagnosed mental disorders (including personality disorders and accentuations) in professional musicians who presented themselves to a musician-specific outpatient service in Germany. The remarkably high rates emphasize the importance of targeting psychopathological symptoms in professional musicians with comprehensive and adaptive measures. Our results can serve as an orientation for future studies and the further development of preventive and therapeutic interventions to foster the mental health of musicians.
Footnotes
Author contributions
Isabel Fernholz: Methodology, Conceptualization, Writing – Original Draft
Christian Hering: Methodology, Formal analysis, Data curation, Visualization, Writing – Original Draft
Hagen Kunte: Supervision
Jennifer Mumm: Methodology, Conceptualization, Writing – Review & Editing
Andreas Ströhle: Supervision
Alexander Schmidt: Conceptualization, Supervision, Writing–Review & Editing
Antonia Bendau: Methodology, Conceptualization, Visualization, Writing – Original Draft
Jens Plag: Conceptualization, Supervision, Writing – Review & Editing
Data availability
Data are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical standards,ethics approval,and consent to participate
The authors carried out a cross-sectional secondary data analysis of clinical data obtained from May 2015 to July 2019. All data were provided and analyzed anonymously. According to statutes of the ethics committee of the Medical Faculty of Charité – Universitätsmedizin Berlin (2019), secondary data analyses do not require ethical approval according to national guidelines (e. g., Regulation [EU] 2016/679 [General Data Protection Regulation], Official Journal of the European Union, 2016).