
Abstract
Growing evidence shows that choirs improve the well-being of people experiencing chronic mental health conditions; however, the impact of performances by “recovery choirs” (i.e., singers with mental health conditions) on their community audience members has not been examined. In three studies, we explored whether performances foster positive emotions toward recovery choristers. In Study 1, we surveyed 50 audience members before and after a public concert and found that watching the recovery choir sing increased positive emotions and attitudes toward mental health recovery. In a randomized experiment, Study 2a (n = 322) and 2b (n = 403) found that watching a short film of both a recovery choir and an amateur community choir singing increased positive emotions toward the choristers in comparison with a control activity condition. There was mixed evidence for effects on social connectedness, acceptance, and belief in mental health recovery. The effects of watching the choirs singing on social connectedness and acceptance of the choristers were mediated by positive emotions. Our results provide new evidence of the audience’s responses to amateur choir performances, by demonstrating that witnessing both community and recovery choir performances can foster admiration, respect, and positive regard toward choristers regardless of their mental health status.
Choir singing has increasingly been used as a social intervention for people with chronic mental health conditions (CMHCs) to improve their mental well-being (Williams et al., 2018). However, although there is a growing focus on the experience of choir members with CMHC, there has been limited research into public performances by “recovery choirs”—that is, choirs comprising singers who are living with and recovering from episodes of mental ill health. The current research sought to explore the impact that recovery choir performances may have on their audience members.
Contact interventions
Recovery choir performances provide indirect contact between people with CMHCs and the broader community. People with CMHCs commonly experience mental health stigma (Thornicroft et al., 2009), which includes negative stereotypes (e.g., “people with mental health conditions are difficult to talk to, violent, and unable to recover,” Pinfold et al., 2003), emotions (e.g., fear, anger, Sadler et al., 2015), and discrimination (e.g., social exclusion in relationships and employment; Tew et al., 2012). Based on Allport’s (1954) intergroup contact hypothesis which posits that positive contact between different social groups can reduce prejudice by challenging negative stereotypes, recovery choir performances could be seen as a form of contact intervention.
Contact interventions, regardless of whether they are face-to-face, imagined, or via video, have been found to have small to moderate effects on reducing mental health stigma (Maunder & White, 2019). The effectiveness of campaigns using theater, film, and comedy to improve attitudes toward people with CMHC depends on the extent to which the production portrays a message of common humanity and recovery (Coyle et al., 2016; Quinn et al., 2011). Attending a recovery choir performance may allow audience members to become more aware of the recovery journey of the choristers, by showing the choristers developing their skills, experiencing joy, and connecting to a social group (Dingle et al., 2013). Therefore, we aimed to explore whether recovery choir performances could have an impact on audience’s positive beliefs in recovery (i.e., belief in people’s ability to recover, live a fulfilling life, and make a meaningful contribution to society), emotions toward choir members (i.e., admiration, inspiration, respect, fondness, affection), social connectedness with choir members (i.e., shared sense of belonging and group fellowship), and social acceptance of choir members (i.e., willingness to include in social groups and relationships).
Emotional and social connection with performers
Emotions are an important target of interventions to reduce stigma as a meta-analysis found that emotional prejudices predict discrimination more than stereotypes and beliefs (Talaska et al., 2008). Music performances may be particularly powerful at promoting positive emotions as music performances impart emotions onto audience members (Kayser et al., 2022). When people listen to music, they commonly experience aesthetic emotions associated with works of art (e.g., admiration, inspiration; Juslin, 2013). Specific emotions can be conveyed from the artist to listener through the musical structure of the composition (Koelsch, 2014). During performances, the intensity with which the music is performed, and facial expressions of the artists, also deepens listeners’ experience of emotional contagion from the artist (Nakra & BuSha, 2014). Consequently, the emotions expressed by the performers are empathically experienced by the listeners. Thus, we sought to explore whether audience members would experience positive emotions (e.g., admiration and affection) toward the recovery choristers when hearing them sing.
The emotional contagion between singers and their audience has been theorized to occur due to the singers and listeners synchronously sharing the activation of similar neural systems (Molnar-Szakacs & Overy, 2006), which could increase a sense of social connectedness between the listener and singer (Overy & Molnar-Szakacs, 2009). Listening to music can even reduce feelings of loneliness; thereby, music can be used as a social surrogate (Schäfer et al., 2020). Indeed, music ability is theorized to have evolved in humans to promote social cohesion and connectedness among large social groups through synchronization (Dunbar, 2012). Two studies to date have specifically demonstrated that musical performances can enhance perceived social connectedness between performers and their audience (van Mourik Broekman et al., 2015, 2018).
Positive emotional reactions to music performances may not only develop social connectedness but also promote social acceptance. Emotions tend to be processed quickly and lead directly to approach or avoidance behaviors, often bypassing conscious cognitive evaluations (Talaska et al., 2008). There is a growing body of research indicating that positive emotional states can promote prosocial behaviors, possibly by broadening an individual’s mindset toward other people (Aknin et al., 2018; Snippe et al., 2018). Work conducted in the context of the stereotype content model (Fiske et al., 2007) has also found that greater admiration toward a social group is associated with enhanced social acceptance, cooperation, and help provided to outgroup members (Cuddy et al., 2008; Onu et al., 2016). Furthermore, the effects of intergroup contact on reducing prejudice toward outgroups have been demonstrated to be mediated by feelings of admiration (Seger et al., 2017). Therefore, music performances by a recovery choir may elicit positive emotions toward the performers, and these emotions may mediate the impact of the music performances on social acceptance and connectedness.
The current research
In the current research, we explored the possible impacts of recovery choir performances on positive emotions, and social acceptance toward the choristers, as well as beliefs in mental health recovery more broadly. Initially we conducted a field study which surveyed audience members of a recovery choir before and after their performance (Study 1). We then further examined audience reactions experimentally (Study 2). In Study 2, based on the above reasoning, we also sought to explore whether positive emotions may mediate the effects of choir performances on social connectedness and social acceptance. To enhance the applicability of the research for reaching wider audiences (e.g., through social media), Study 2 used short video stimuli of the choir singing.
Study 1
Study 1 was conducted at a live performance of a recovery choir at a prominent performing arts center theater with 1,600 capacity. This study used a repeated-measures design where participants were surveyed before and after watching the concert. We hypothesized that (a) positive emotions toward choristers, (b) social acceptance toward people with CMHC, and (c) belief in mental health recovery would increase during the concert.
Methods
Participants
A random selection of 50 concert attendees completed the survey before and after the live concert. A further 15 participants were excluded from the analysis due to only completing one of the two surveys. The sample size had 80% power, at the standard .05 alpha error probability, to detect a small to moderate effect size of d = .35 for one-tailed repeated-measures t tests.
The majority of the participants (90%) were women. There was a wide spread of ages—36% were 18 to 39 years old, another 36% were 40 to 59 years old, and 28% were over 60 years old. Only 14% personally knew a member of the recovery choir. According to a multiple-choice item on frequency of contact with people with severe mental health conditions, 38% indicated no contact in the past year, 32% had contact less than once a week, 20% more than once a week, and 10% had a CMHC themselves.
Concert
In this live concert, the recovery choir were joined on stage by a massed community choir and professional soloists. In addition to a song program, the concert involved the master of ceremonies providing several anecdotes of the recovery journeys of individual choir members. The concert lasted for approximately 3 hr and was performed during Mental Health Week.
Data collection and measures
Attendees were recruited between when they arrived at the venue and when the doors opened. Three researchers approached the attendees to recruit participants. Those willing to participate were provided with information about the study and asked to provide their mobile numbers. A link to a brief electronic survey was sent to them by SMS before and after the concert. As there was limited time for participants to complete the survey before the concert and we were providing no reimbursement, the questionnaires contained brief measures and took 3 min to complete.
Positive emotions toward the choristers
Participants were asked to rate a subset of emotions used in previous research on emotions felt toward people with a mental illness (Sadler et al., 2015). In this study, participants were asked to rate the extent to which they felt admiration, respect, inspired, fondness, and affection toward the recovery choir, on a 7-point scale (1 = not at all, 7 = extremely). Items were high in internal reliability (α = .92) and were therefore combined.
Social acceptance of someone with a CMHC
A single item was used to measure social acceptance. Participants were asked to what extent they would be accepting of someone with a CMHC if they were a part of their lives. Answers were recorded on a 7-point scale (1 = not very accepting, 7 = very accepting).
Belief in mental health recovery
Participants were asked about their beliefs in recovery from CMHC. Two items asked how strongly they believed that people with CMHC can live a fulfilling life and can contribute meaningfully to society. These items were combined into one outcome measure (pre α = .90, post α = .92) and were responded to on a 7-point scale (1 = strongly disagree, 7 = strongly agree).
Results
We explored the hypothesis that (a) positive emotions, (b) social acceptance, and (c) belief in mental health recovery would increase from before to after the live concert using paired-samples t tests, see Figure 1. There was a moderately large increase in positive emotion from before (M = 5.05, SD = 1.43) to after (M = 5.72, SD = 1.22) the concert, t(49) = −4.41, p < .001, d = .50. Social acceptance intentions toward people with a CMHC were highly endorsed but did not significantly change from before (M = 6.18, SD = 1.21) to after (M = 6.36, SD = 6.36) the concert, t(49) = −1.27, p = .211, d = .20. Furthermore, recovery beliefs improved from before (M = 6.18, SD = 0.99) to after the concert (M = 6.48, SD = 0.68), t(49) = −2.25, p = .029, d = .28.
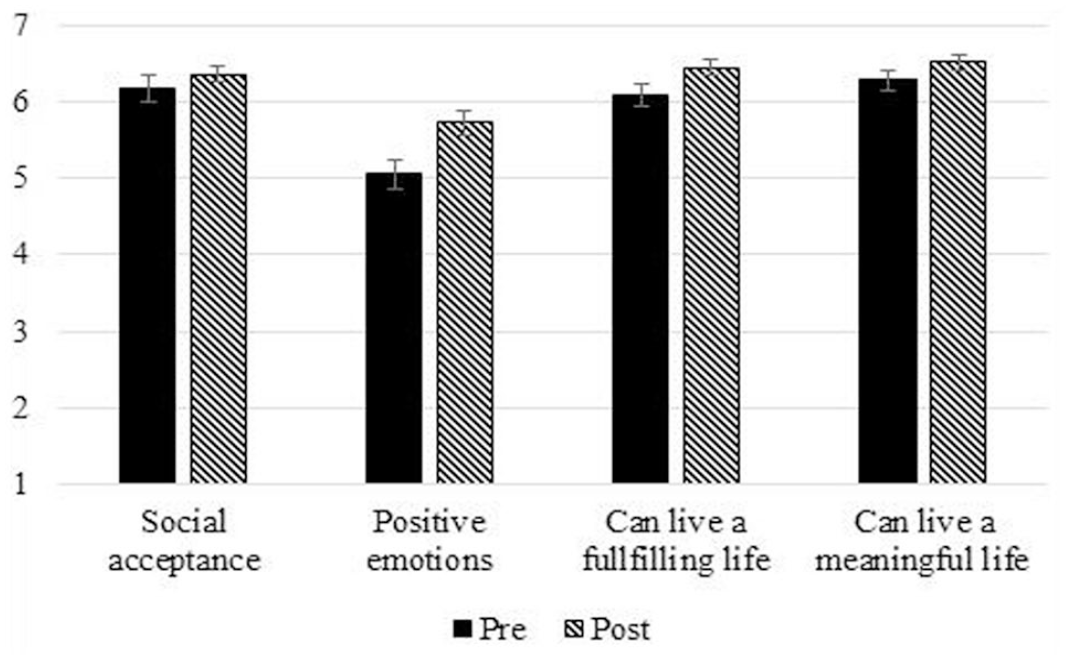
Positive Emotions, Social Acceptance, and Recovery Beliefs Before and After Watching the Performance in Study 1.
Discussion
Positive emotions toward the choristers improved significantly from before to after the concert, supporting the impact of music performers to draw in the audience emotionally (Overy & Molnar-Szakacs, 2009). Social acceptance of people with CMHC did not significantly change during the live concert. This is perhaps unsurprising because our participants had chosen to attend a concert of the recovery choir, and we found high a priori levels of social acceptance. The results also demonstrated that exposure to the recovery choir performance may increase positive beliefs in mental health recovery.
This study had high ecological validity as it recruited participants at a live concert. However, as the participants had chosen to attend the concert, it is likely that a priori support for the recovery choir members was high. This is also evident from the pre-concert survey for social acceptance—mean scores on this measure of over 6 out of 7 suggest that we are witnessing a ceiling effect limiting the extent to which further positive change could be observed. Another limitation of Study 1 was that we did not include a control where participants attended the concert of non-CMHC performers.
To overcome these limitations, we conducted an experimental study, examining emotional responses to watching recordings of a recovery choir singing. Although live performances may be more engaging than recordings (Swarbrick et al., 2019), watching short recordings may have more practical applications for reaching a broader audience of people who would not usually attend a recovery choir performance.
Study 2a
In Study 2, to assess the unique effects of watching a short recording of a recovery choir performance, we manipulated the type of choir that participants viewed. Participants watched either the recovery choir or a control amateur community choir singing the same song. To test the specificity of any effects of choir singing, some participants watched choir members singing, while other participants watched the choir members engaging in a control activity (i.e., eating lunch).
We predicted a main effect for activity, specifically that exposure to either choir singing would enhance (a) positive emotions and (b) social acceptance toward the choristers compared with these choirs engaging in the control activity (Hypothesis 1). We expected these effects to be similar for both choirs as we hypothesized that these effects would arise from musical performance more generally. As positive emotions may increase social acceptance, we also explored whether the effects of choir singing on social acceptance would be mediated by positive emotions (Hypothesis 2). Furthermore, we predicted that unique effects would flow from exposure to a choir of people with CMHC. Specifically, we predicted that the belief that people with CMHC can recover would be higher in the condition where participants watched choir members with CMHC compared with those who watched the control choir (Hypothesis 3). We also predicted that participants who saw the recovery choir sing would endorse belief in recovery more strongly than participants who viewed people with CMHC in the control activity (i.e., eating lunch; Hypothesis 4).
Methods
Participants and design
A total of 322 first-year psychology students participated in this study, in return for course credit. The majority of students were below 25 years of age (89.5%) and female (79.2%). To reduce sampling bias, the participants were unaware of the content of the films they would be presented with prior to the experiment. Previous contact with people diagnosed with a severe mental illness greatly varied in the sample. A third of the participants (31.3%) had no previous contact aside from having watched TV shows depicting people with mental health conditions. Other participants had contact in the workplace or on a frequent basis in the community (15.2%), had a friend or family member with a severe mental health condition (39.4%), lived with someone with a mental health condition (7.1%), or indicated having a severe mental health problem themselves (6.8%). The experiment was a 2 (group: recovery choir; control choir) × 2 (activity: choir singing; eating lunch) between-participants design, with 80 participants randomly allocated to each of the four conditions. The sample size had 80% power, at the standard .05 alpha error probability, to detect a small effect size of partial η2 = .025 for between-group effects (including interactions).
Group manipulation
The choir group was manipulated by providing a brief description of aims and activities of the choir followed by a short film clip (see Supplementary Materials online for stimuli text). The film stimuli were obtained by filming a recovery choir involved in the concert in Study 1 and a community non-auditioned control choir during a typical rehearsal day. All choir members gave written consent to be filmed. Both choirs were based in the same city, were instructed by the same conductor, and had been practicing the song for a couple of weeks prior to the filming. The film clips were comparable in the number of singers in the shot, the set-up of the rehearsal room, the lighting, and the style of conducting. In the films, there was a similar distribution of gender in the recovery choir (15 women and 10 men) and the control choir (15 women and seven men). There was a broad range of ages in both choirs (the recovery choir: Mage = 43.76, SD = 11.79; the control choir: Mage = 52.11, SD = 10.14).
Activity manipulation
The singing conditions were depicted in a short film clip of each choir singing “You’re the Voice,” a popular song from the 1980s written by Andy Qunta, Keith Reid, Maggie Ryder, and Chris Thompson and originally sung by John Farnham. The song was chosen due to the inspirational content and having well-known lyrics. A control non-singing group activity condition was recorded while the choir members were having lunch. The audio of the film had background noise of talking without distinguishing conversations.
Previous contact with people with CMHC
Because previous level of contact with mental illness has been found to have a significant effect on how people perceive people with mental illness, we measured this using the Level-of-Contact Report (Holmes et al., 1999). This scale provided 12 options on participants’ previous contact with mental illness. Each item had a rank from 1 (I have never seen someone with a severe mental illness) to 12 (I have a severe mental illness), where high scores indicated more intimate contact with people experiencing a CMHC. Participants marked all options that were true of themselves. The item chosen with the highest rank was used as the final score.
Positive emotions
The same items as in Study 1 were used to measure positive emotion (admiration, respect, inspired, fondness, affection; pre α = .92, post α = .94). However, in this study they were rated on a 5-point scale (1 = not at all, 5 = extremely).
Social acceptance of the choristers
The extent to which participants intended to be socially accepting of the choir members was measured using the Social Distance Scale (Lauber et al., 2004). Participants were asked to rate how accepting they would be of someone from the choir if they would be a part of their lives in the following roles: living in your neighborhood, an acquaintance making conversation with you, co-worker or classmate, next door neighbor, housemate, in law, friendship circle, or a childcare provider. Participants were asked the extent they would be accepting of someone from the choir in the film they just watched on a 7-point scale (1 = very not accepting, 7 = very accepting). In the current sample, this scale was reliable (α = .89).
Belief in mental health recovery
After participants had answered questions that related to the choir members, they were asked to rate how strongly they agreed that people with CMHC can recover from mental health problems (Pinfold et al., 2003). Participants responded on a 7-point scale (1 = strongly disagree, 7 = strongly agree).
Results
Positive emotions, social acceptance, and belief in recovery were analyzed using 2 (group) × 2 (activity) between-participants univariate analyses of variance (ANOVAs). The mean ratings in each condition are displayed in Table 1.
Means and Standard Deviations in Each Condition in Study 2a and 2b.
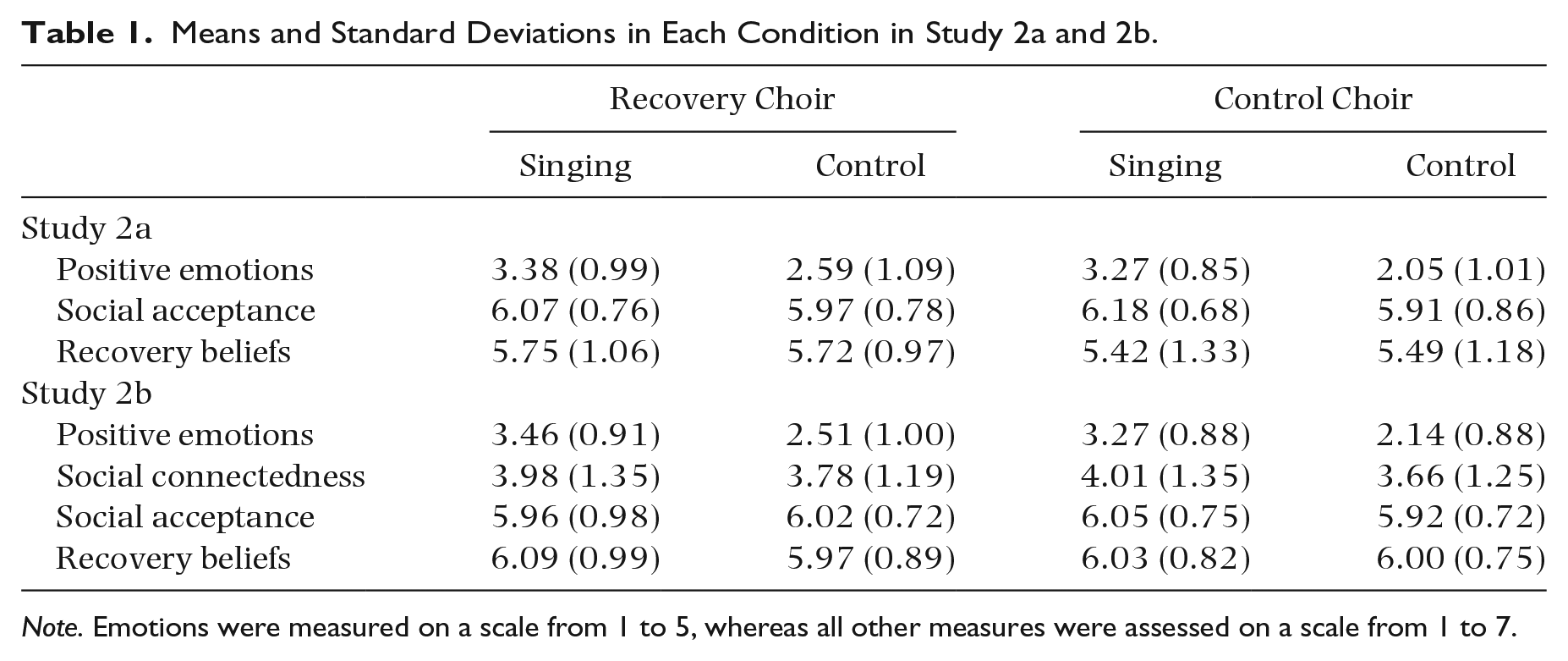
Note. Emotions were measured on a scale from 1 to 5, whereas all other measures were assessed on a scale from 1 to 7.
Positive emotions toward the choristers
In support of Hypothesis 1, a significant main effect was found of the activity conditions on positive emotion, where participants felt stronger emotions toward the choirs in the recording when they were singing (M = 3.33, SD = 0.92) than when they were having lunch (M = 2.32, SD = 1.08), F(1, 318) = 83.75, p < .001,
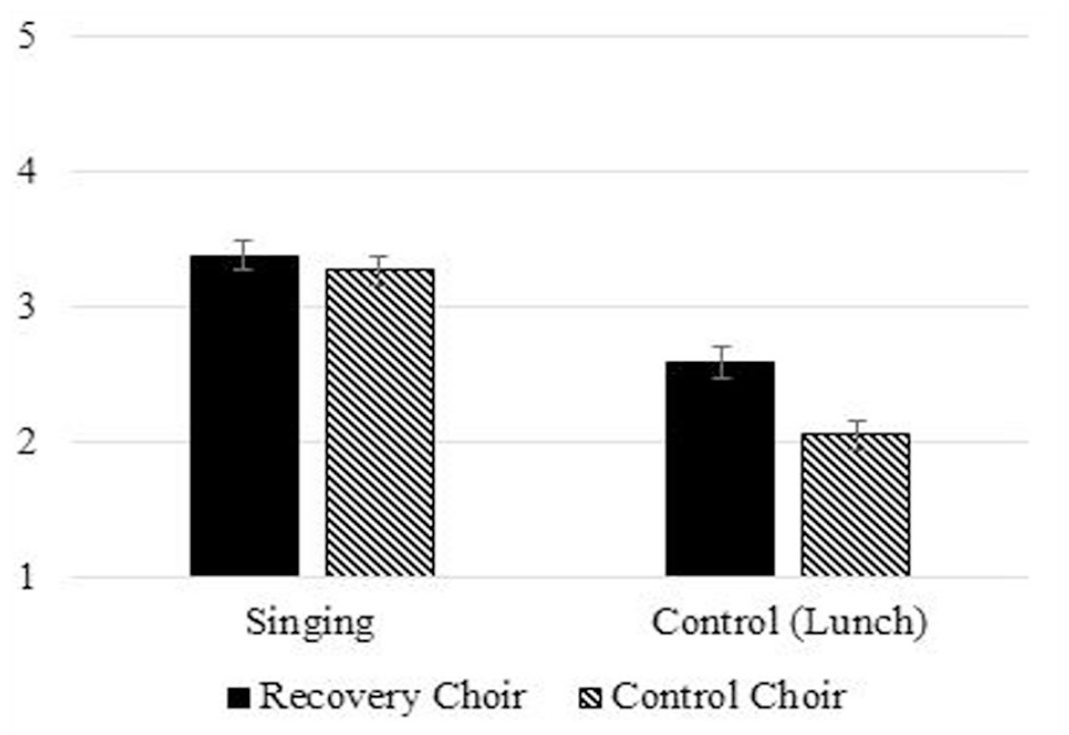
Positive Emotions Between Activity (Singing vs. Control Activity) and Group (Recovery vs. Control Choir) Conditions in Study 2a.
Social acceptance toward the choristers
In support of Hypothesis 1, a significant main effect was found for activity, whereby greater social acceptance was reported after viewing the recordings of the choirs singing (M = 6.13, SD = 0.72) than when watching the recordings of the choirs having lunch together (M = 5.94, SD = 0.82), F(1, 318) = 4.90, p = .028,
Positive emotions as a mediator of the impact of choir singing on social acceptance
The role of positive emotions as a mediator of the impact of choir singing on social acceptance (Hypothesis 2) was assessed using a PROCESS mediation model (Hayes, 2017; Model 4; 5,000 bootstrapped samples), see Figure 3. Participants who watched either choir were included in this analysis. The activity (singing vs. control) predicted positive emotions, b = 1.01, confidence interval (CI) = [0.79, 1.23], p < .001, demonstrating that participants experienced stronger positive emotions in the singing condition in comparison with the control activity condition. Furthermore, positive emotions predicted greater social acceptance, b = 0.29, CI = [0.21, 0.36], p < .001. When controlling for positive emotions, the direct relationship between activity (singing vs control) and social acceptance became nonsignificant, b = −0.10, CI = [−0.28, 0.08], p = .263. Overall, the indirect effect through positive emotions was significant, b = 0.29, CI = [0.20, 0.40]. Therefore, in support of Hypothesis 2, watching the recorded singing performance enhanced social acceptance toward the choristers through eliciting more positive emotions.
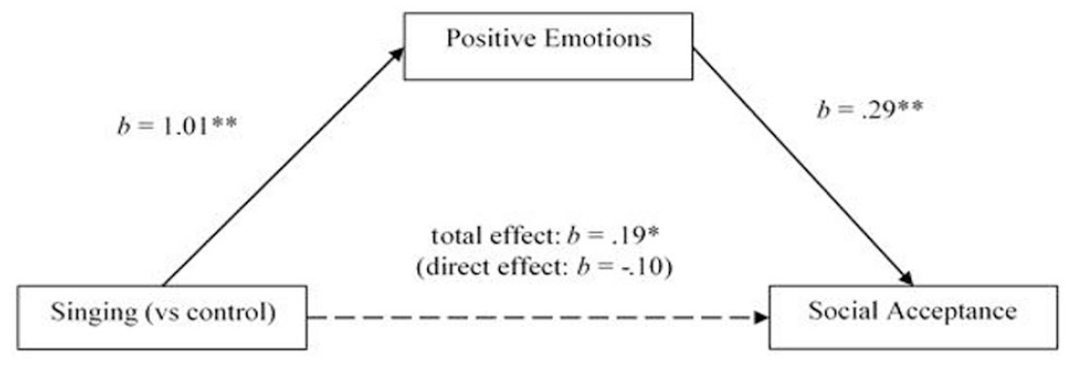
Positive Emotions Fully Mediated the Effect of Watching the Choir Sing (as Opposed to the Control Activity) on Social Acceptance (Indirect Effect: b = 0.29) in Study 2a.
Impact of recovery choir performance on audience’s belief in recovery
In support of Hypothesis 3, the main effect for group was significant, indicating that participants believed more strongly in recovery after viewing the recording of the recovery choir (M = 5.74, SD = 1.01) than when they watched the control choir (M = 5.46, SD = 1.26), F(1, 318) = 4.84, p < .029,
Study 2b
To test the robustness of Study 2a, a preregistered, highly powered study was conducted using the same methodology as Study 2a (see registration at: http://aspredicted.org/blind.php?x=wt4b5u). We added a measure of social connectedness with the choristers and a behavioral measure assessing whether exposure to the recovery choir singing would increase political support for government funding of arts-based programs in mental health.
We predicted that watching the recordings of choirs singing would enhance (a) positive emotions, (b) social acceptance, and (c) social connectedness compared with these choirs engaging in the control activity (Hypothesis 1). We explored whether the effects of choir singing on (a) social acceptance and (b) social connectedness would be mediated by positive emotions (Hypothesis 2). Furthermore, we predicted that (a) belief in mental health recovery and (b) support for government funding would be higher among participants who watched recordings of the choir members with CMHC compared with those who watched the control choir (Hypothesis 3), and more so when participants saw the recovery choir singing than participants who watched the recovery choir in the control activity (i.e., eating lunch; Hypothesis 4).
Method
Participants and design
A total of 403 people from the United Kingdom (96.5% current U.K. residents) were recruited through Prolific in return for a small monetary reward. These participants were reasonably matched for age (M = 41.60, SD = 11.14), gender (66.3% female), and ethnicity (93.1% Caucasian; 3.7% Asian; 1.4% African; 0.5% Hispanic, and 1.7% mixed) with the choristers in the stimuli. Again, to reduce sampling bias, participants were not informed of the type of films they would watch in the study advertisement. Previous contact with people diagnosed with a severe mental illness was similar to that of Study 2a. A third of the participants (33.1%) only had watched TV shows depicting people with mental health conditions. Other participants had contact in the workplace or on a frequent basis in the community (18.4%), had a friend or family member with a severe mental health condition (36.9%), lived with someone with a mental health condition (5.2%), or indicated having a severe mental health problem themselves (6.5%). The study was a direct replication of Study 2a—a 2 (group) × 2 (activity) between-subjects’ design, with 100 participants randomly allocated to each of the four conditions. This sample size was based on a calculation of needing 97 participants per group for 80% power to detect a small effect size of
Procedure
The experimental conditions were manipulated using the same stimuli as in Study 2a. After watching the video, participants completed a questionnaire which included the same measures as in Study 2a, including previous contact with CMHC, positive emotions toward the choristers (α = .94), and social acceptance of the choristers (α = .92). In addition, we included measures of social connectedness, belief in mental health recovery, and a behavioral measure.
Social connectedness with the choristers
We included a four-item scale which has been used previously when studying observers’ perceptions of shared social identity with the performers (van Mourik Broekman et al., 2018; for example, “I identify with the group of people in the video”; “I feel solidarity with the group of people in the video”). Participants rated their agreement with the statement on a 7-point scale (1 = strongly disagree; 7 = strongly agree; α = .86).
Belief in mental health recovery
In addition to the item included in Study 2a, we included two further items assessing beliefs in mental health recovery: “People with mental health problems can live a fulfilling life,” and “People with mental health problems can make a meaningful contribution to society.” All items were rated on a 7-point scale (1 = strongly disagree, 7 = strongly agree) and were combined into a single scale (α = .74).
Behavioral measure
Participants were also asked to indicate how they would vote if they were asked the question, “Even if it would mean having less financial support for other schemes to support people with mental health conditions, would you support the government of the United Kingdom providing increased and sustainable funding to develop arts programs (e.g., choir, drama, art, and creative writing groups) for people with mental health conditions?” with a yes/no response.
Results
As in Study 1, the dependent variables were analyzed using 2 (group) × 2 (activity) between-participants ANOVAs (see Table 1 for means of each condition).
Positive emotions toward the choristers
The findings of Study 2a regarding positive emotions were replicated. In support of Hypothesis 1a, a significant effect of the activity manipulation on positive emotion was found, where people felt stronger emotions toward the choirs when they watched the recording of the choirs singing (M = 3.36, SD = 0.90) than when they were having lunch (M = 2.33, SD = 0.96), F(1, 399) = 127.80, p < .001,
Social acceptance toward the choristers
Unlike Study 2a, no support was found for choir singing enhancing social acceptance of the choristers compared with the control activity condition (Hypothesis 1b). There was no main effect for activity, F(1, 399) = 0.17, p = .679,
Social connectedness with the choristers
As predicted by Hypothesis 1c, the activity manipulation had a significant main effect on social connectedness, where people felt closer toward the choristers when they were singing (M = 4.00, SD = 1.35) than when they were having lunch (M = 3.72, SD = 1.22), F(1, 399) = 4.73, p = .030,
Positive emotions as a mediator of the impact of choir singing on social acceptance
Although the singing condition did not have a significant impact on social acceptance, the indirect effects through positive emotions were still examined to test Hypothesis 2a using a PROCESS mediation model (Hayes, 2017; Model 4; 5,000 bootstrapped samples), see Figure 4. The activity (singing = 1; control = 0) predicted positive emotions, b = 1.03, CI = [0.85, 1.21], p < .001, such that participants experienced greater positive emotions in the singing condition as opposed to the control activity condition. Positive emotions, in turn, predicted social acceptance, b = 0.21, CI = [0.13, 0.29], p < .001. After controlling for the mediator (positive emotions), the direct relationship between activity (singing = 1; control = 0) and social acceptance became negative (the total effect had been non-significant), showing a suppression effect, b = −0.19, CI = [−0.36, −0.01], p = .035. This indicates that, if it were not for the positive emotions elicited by the performance, acceptance of the choristers would have been higher in the control activity condition than the singing condition. The indirect effect of watching the choir sing (as opposed to the control activity) on social acceptance through positive emotions was significant, b = 0.22, CI = [0.12, 0.34]. Therefore, in support of Hypothesis 2a, watching the recorded singing performance enhanced social acceptance of the choristers to the extent that the performance elicited positive emotions.
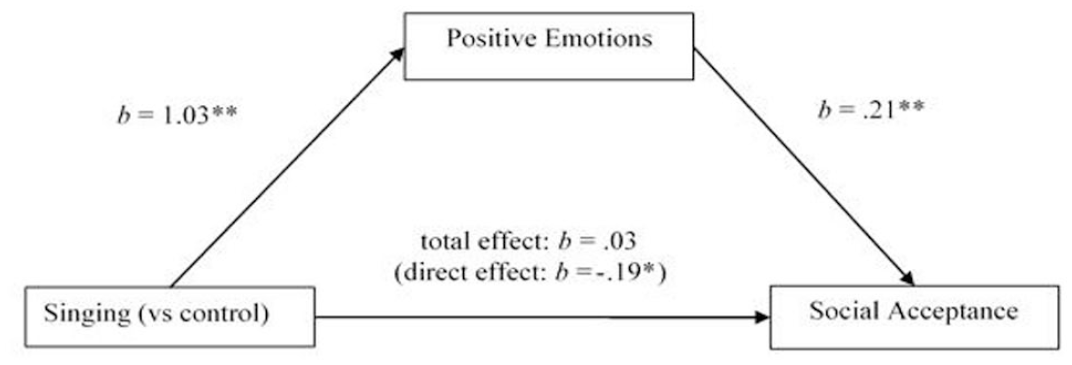
The Indirect Effect of Watching the Choir Sing (as Opposed to the Control Activity) on Social Acceptance Through Positive Emotions (Indirect Effect: b = 0.22) in Study 2b.
Positive emotions as a mediator of the impact of choir singing on social connectedness
As predicted by Hypothesis 2b, the role of positive emotions as a mediator of the relationship between watching a singing performance and increased social connectedness was assessed, see Figure 5. Positive emotions predicted social connectedness, b = 0.75, CI = [0.64, 0.87], p < .001. When the effects of positive emotions were controlled, the direct relationship between activity (singing = 1; control = 0) and social connectedness was negative, b = −0.50, CI = [−0.74, −0.26], p < .001. This indicates that positive emotions fully mediated the positive effects of singing (as opposed to the control activity) on connectedness. The indirect effect of the activity (singing = 1; control = 0) on social connectedness through positive emotions was significant, b = 0.78, CI = [0.60, 0.95]. Therefore, in support of Hypothesis 2b, watching the recorded singing performance enhanced a sense of social connectedness with the choristers through eliciting positive emotions.
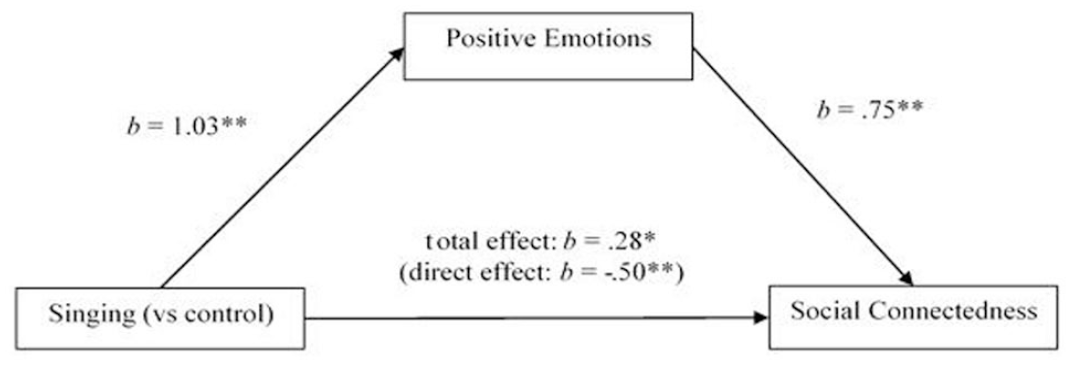
The Indirect Effect of Watching the Choir Sing (as Opposed to the Control Activity) on Social Connectedness Through Positive Emotions (Indirect Effect: b = 0.78) in Study 2b.
Belief in mental health recovery
No support was found for Hypotheses 3 or 4. There was no statistically significant main effect for activity, F(1, 399) = 0.663, p = .416,
Behavioral intention measure
The majority of participants (81.4%) indicated that they would vote in support of the U.K. government funding arts-based groups, even if the funding drew away resources from other mental health services. However, the proportion of people who supported the funding did not differ between activity conditions, χ2(1) = .070, p = .791, or group conditions, χ2(1) = .380, p = .538.
General discussion
The aim of this novel investigation was to explore the impacts of watching a choir performance by people affected by CMHC. The primary finding across all three studies was that audiences of choir performances—both recorded and live—felt admiration, respect, and positive regard toward the choristers. In the experimental study (Study 2), the participants indicated feeling these emotions moderately to very much when watching the choirs singing, as opposed to feeling the emotions slightly to moderately when watching them eat lunch. The effect of singing on emotions did not differ between the recovery choir and the community choir. Thus, the choir performances fostered positive emotions toward choristers regardless of the mental health status of the performers, despite previous findings that people often have negative emotional reactions (e.g., fear and anger) toward people diagnosed with CMHC (Angermeyer et al., 2013). Overall, these results support the role of music in eliciting aesthetic and social emotions.
Evidence for the effects of the choir performance on social acceptance was inconsistent across the three studies, overall indicating either null or modest effects. Likewise, the effects of the choir performance on social connectedness in the U.K. community sample (Study 2b) were small. Despite this, the experimental studies found that the effects of watching the recordings of the choirs singing—regardless of whether it was the recovery or control choir—on social acceptance and connectedness were mediated by positive emotions. This suggests that when performances have an impact on social outcomes, this may be explained by the effects of positive emotions. This finding is consistent with previous studies that indicate positive emotions, including admiration, can increase social acceptance and prosocial behaviors (Aknin et al., 2018; Onu et al., 2016). Further exploration of the effects of emotions as a mediator for music-induced social connectedness may be applied to music psychology research more broadly, such as research on music social interventions, music as a social surrogate (Schäfer & Eerola, 2020), and the social evolutionary function of music (Dunbar, 2012).
In both Australian samples (Studies 1 and 2a), we found a small increase in recovery beliefs after exposure to the recovery choir; however, this was not replicated in the U.K. sample (Study 2b). Furthermore, no effects were found on support for government funding of arts-based programs for mental health in the U.K. sample. Despite no effects being found between conditions, the U.K. sample did respond very favorably toward beliefs in recovery and supporting funding for arts-based programs, possibly indicating ceiling effects. The community samples from the United Kingdom (Study 2b) and Australia (Study 1) indicated stronger recovery beliefs than the student sample from Australia (Study 2a). Although closeness of contact with people with CMHC did not differ between the samples, younger people may lack the longevity of contact to have seen recovery from CMHC. Exposure to the recovery choir had some impact on recovery beliefs in the student sample.
However, in the student sample (Study 2a), recovery beliefs increased with exposure to the recovery choir, not only in the singing condition but also in the control condition. Furthermore, positive emotions were experienced more strongly toward the recovery choir than the control choir in the control activity condition. These results may be due to participants being exposed to information about the choir members working toward living a fulfilling life and connecting with others despite their difficulties. The reactions of the students toward the recovery choir, in the control activity condition, may reflect that the contextual information is the active component for changing recovery beliefs more so than witnessing the singing. This is consistent with Allport’s (1954) intergroup contact hypothesis as the contextual information challenges the negative stereotype that people with CMHC are unable to recover (Pinfold et al., 2003).
Overall, this research found little support for recovery choir performances as an indirect contact intervention to improve recovery beliefs and social acceptance of people with CMHC. However, although we tried to avoid a biased sample, scores for social acceptance and recovery beliefs were high, pointing to possible ceiling effects or social desirability bias. Social desirability bias can occur when people feel pressure to demonstrate support for a disadvantaged group; however, anonymity should mitigate this bias. Furthermore, as the studies focused on the immediate effects of performances, it is unclear how long-lasting these effects are. As attitudes toward mental health conditions often take time to change (Griffiths et al., 2014), future research may explore the impacts of accumulative video exposures (e.g., via social media) and long-term interventions, for example, including community members as choristers in recovery choirs.
In summary, the current results indicated that choir singing was associated with audience’s positive emotions toward amateur and recovery choirs alike. To our knowledge, this is the first empirical study to demonstrate the emotional impact of watching amateur choirs perform. Overall, evidence for using recovery choir performances to improve social acceptance toward the choristers and mental health recovery beliefs was weak. However, the contextual information on how the choir supports social recovery was more impactful than singing on improving recovery beliefs, demonstrating the potential benefit of including chorister’s recovery stories in performances. Furthermore, we provided preliminary evidence that the effects of music on social acceptance and connectedness may be mediated by music-induced emotions.
Supplemental Material
sj-docx-1-pom-10.1177_03057356231153065 – Supplemental material for Audiences’ emotional response to choir singing by people living with mental health conditions
Supplemental material, sj-docx-1-pom-10.1177_03057356231153065 for Audiences’ emotional response to choir singing by people living with mental health conditions by Elyse Williams, Jolanda Jetten and Genevieve A. Dingle in Psychology of Music
Footnotes
Acknowledgements
The authors thank Braden Trotter and Cameron Hawes for their help filming the videos used in Study 1, and the choirs, Absolutely Everybody and Musica, who featured in the films with their conductor Melissa Gill. They also thank Leah Sharman and Renee Calligeros for their assistance collecting data at the concert.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.