
Abstract
Background
Accurate assessment of root length, tip, and torque is essential for orthodontic diagnosis and treatment planning. Cone-beam computed tomography (CBCT) provides reliable three-dimensional visualization of tooth roots but is associated with radiation exposure. Recently, artificial intelligence (AI)-supported planning software has enabled virtual root reconstruction using intraoral scan data; however, the accuracy of such reconstructions compared with CBCT remains uncertain.
Objectives
To compare root length, tip, and torque measurements obtained from CBCT with those generated by AI-supported planning software (Maestro 3D) using intraoral scan data.
Methods
This cross-sectional observational study included 21 patients with existing pre-treatment CBCT records. Intraoral scanning was performed prior to orthodontic treatment. The maxillary left central incisor was selected as the reference tooth. CBCT Digital Imaging and Communications in Medicine (DICOM) data were segmented using 3D Slicer to generate STL files. Intraoral STL files were imported into Maestro 3D, where AI-based root reconstruction was performed. Root length, tip, and torque measurements were recorded and compared using paired samples t-tests and Bland–Altman analysis.
Results
CBCT-derived root length measurements were significantly greater than AI-generated measurements (mean difference = 5.01 mm; P < .001). The AI-supported software consistently produced a fixed root length value of approximately 12 mm with no variation, indicating a limitation of the algorithm and suggesting reliance on standardized templates rather than individualized root morphology. Tip measurements also showed a statistically significant difference between the two methods (mean difference = −0.85°; P < .001). Torque measurements demonstrated a small but statistically significant difference between CBCT and AI-generated models (mean difference = 0.67°; P = .045).
Conclusion
AI-supported planning software underestimated root length and slightly overestimated tip compared with CBCT, while torque measurements were comparable. CBCT remains the reference standard for root length assessment, whereas AI-based intraoral scan analysis may be clinically acceptable for torque evaluation.
Keywords
Introduction
Precise evaluation of both crown alignment and root position is fundamental for successful orthodontic diagnosis and treatment planning, as inadequate control of root position may compromise periodontal health, occlusal stability, and long-term treatment outcomes. Digital orthodontic treatment planning systems increasingly attempt to estimate root position during virtual setup; however, inaccuracies in predicted root position may influence clinical decision-making. 1 Conventional two-dimensional imaging techniques provide limited information regarding root morphology and spatial relationships among teeth. Cone-beam computed tomography (CBCT) has been demonstrated to provide reliable three-dimensional visualization of teeth and surrounding structures and enables accurate dental measurements for orthodontic assessment. 2
However, predicting root position based solely on crown morphology remains challenging. Previous studies have shown that estimation of the root axis or inclination using only crown morphology may introduce uncertainties, particularly when evaluating root length or angulation. 3 To improve the three-dimensional evaluation of tooth position, methods combining CBCT datasets with digital models have been developed. Superimposition techniques using CBCT and digital models have been used to monitor tooth movement and evaluate root position during orthodontic treatment. 4
Digital dental models obtained through intraoral scanning have become widely used in orthodontic practice because they provide accurate and reproducible representations of crown morphology. The diagnostic accuracy and measurement sensitivity of digital models for orthodontic purposes have been well documented in the literature. 5 In addition, CBCT imaging has been reported to provide accurate and reliable measurements of tooth and root lengths, making it an important reference standard for three-dimensional dental evaluation. 6
With the increasing adoption of digital workflows, intraoral scanners are now routinely used for orthodontic diagnosis and treatment planning, offering advantages such as improved patient comfort, reduced chairside time, and elimination of conventional impressions. 7 Despite these advances, the routine use of CBCT in orthodontics remains limited due to radiation exposure considerations and the need for judicious use according to diagnostic requirements. 8
Therefore, validation of artificial intelligence (AI)-generated root reconstructions from intraoral scan data against CBCT-derived measurements is essential before such technologies can be reliably incorporated into orthodontic treatment planning. The aim of the present study was to compare root length, tip, and torque measurements generated by AI-supported planning software using intraoral scan data with those obtained from CBCT, which served as the reference standard.
Materials and Methods
Study Design and Sample
This cross-sectional observational study included 21 patients. The sample size was calculated using the formula:

where Zα is the constant set according to the accepted alpha error (0.05), Z(1−β) corresponds to the statistical power of the study (90%), SD represents the standard deviation derived from the parent article, and d represents the clinically significant difference.
Based on this formula, the study required a minimum sample size of 21 subjects at 95% confidence level and 90% statistical power to compare root length, tip, and torque measurements obtained by superimposing CBCT (Digital Imaging and Communications in Medicine, DICOM) and intraoral scan (STL) datasets.
The parameters used for the calculation were derived from the study by Lee et al. 4
Patients aged 15-30 years were selected because permanent dentition with completed root formation is generally present in this age group, allowing accurate evaluation of root morphology and tooth inclination.4, 9
Tooth Selection
The maxillary left central incisor was selected as the reference tooth due to its: Relatively consistent morphology, Importance in orthodontic esthetics and torque control, and Frequent use as a reference tooth in orthodontic imaging studies.
Bilateral or multi-tooth sampling was avoided to reduce anatomical variability and standardize comparisons.
Inclusion Criteria
Patients aged 15-30 years,
Presence of permanent maxillary anterior teeth,
Availability of CBCT scans in DICOM format, and
No prior orthodontic treatment.
Exclusion Criteria
Patients with a history of trauma to the maxillary anterior teeth were excluded, as traumatic dental injuries may result in root resorption, arrested root development, or altered root morphology, which could influence root measurements. This has been previously reported in the literature. 10
Craniofacial anomalies or syndromes.
Severe crown restorations or fractures.
Periodontal disease or poor oral hygiene.
Fixed or removable prostheses affecting crown morphology.
Image Acquisition
CBCT scans were obtained using a standardized CBCT unit (Planmeca ProMax® 3D, Planmeca Oy, Helsinki, Finland) with imaging parameters of 120 kVp, 6.3 mA, field of view 6 × 6 cm, voxel size 0.07 mm 3 , and exposure time of 19 s. Intraoral scans were acquired using a SHINING 3D intraoral scanner (Aoralscan® 3, SHINING 3D, Hangzhou, China).
Intraoral scans were obtained prior to the initiation of orthodontic treatment, with a minimal time interval from the CBCT acquisition for each patient to ensure that no orthodontic intervention or positional changes of the teeth occurred between the two imaging procedures. Similar methodologies combining CBCT datasets with intraoral scan STL files for three-dimensional evaluation of tooth position have been reported in previous orthodontic studies.4, 11
CBCT Segmentation
CBCT DICOM files were imported into 3D Slicer (version 5.6.2). Tooth segmentation was performed using threshold-based selection followed by manual refinement with the sphere brush tool. The segmented tooth, including the root, was exported as an STL file (Figures 1 and 2).
Tooth Segmentation Performed in the Red Slice View Using 3D Slicer.

Segmented Cone-beam Computed Tomography (CBCT) Tooth Model Generated Using 3D Slicer Software.

AI-based Root Reconstruction
Intraoral STL scan files were imported into Maestro 3D software (version 6.0). The crowns were automatically segmented, and virtual roots were generated using the software’s AI-based reconstruction module (Figure 3). The system employs machine-learning-based statistical tooth models trained on population-based datasets to estimate root morphology and orientation from crown morphology. Similar machine-learning approaches integrating intraoral scans and CBCT datasets for three-dimensional evaluation of tooth morphology have been described in previous studies.11, 12
Artificial Intelligence (AI)-based Root Reconstruction Generated in Maestro 3D Software.

Superimposition and Measurements
Root length was defined as the linear distance from the cemento-enamel junction (CEJ) to the root apex along the long axis of the tooth. Measurements were obtained from the CBCT-derived STL models following segmentation in 3D Slicer. CBCT imaging allows accurate three-dimensional visualization of tooth morphology and has been widely used for reliable dental measurements in orthodontic research. 6
CBCT-derived and AI-generated STL files were superimposed in Maestro 3D using three anatomical crown landmarks (mesial, distal, and midpoint of the crown; Figure 4). Root length (Figure 5), tip (Figure 6), and torque (Figure 7) were measured for both datasets.
Superimposition of Cone-beam Computed Tomography (CBCT)-derived and Artificial Intelligence (AI)-generated Tooth Models Using Crown Landmarks.

Measurement of Root Length in Maestro 3D Software.

Measurement of Tooth Tip in Maestro 3D Software.

Measurement of Tooth Torque in Maestro 3D Software.

Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics version 26. Descriptive statistics were calculated. Normality testing supported the use of parametric analysis; therefore, paired samples t-tests were used to compare CBCT and AI-generated measurements. Agreement between methods was assessed using Bland–Altman plots. A P value < .05 was considered statistically significant.
Results
Descriptive Statistics
The descriptive statistics for root length, tip, and torque measurements obtained from CBCT and AI-generated models are presented in Table 1.
Paired Sample Descriptive Statistics Comparing Root Length, Tip, and Torque Measurements Obtained from Cone-beam Computed Tomography (CBCT) (1) and Intraoral Scan (2).

Note: *(1) CBCT and (2) intraoral scan.
Paired Comparisons
Paired samples t-test results are summarized in Table 2.
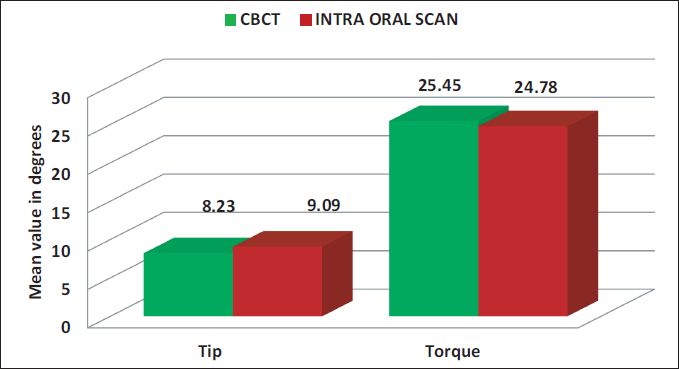
Root length: CBCT measurements were significantly higher than AI-generated measurements (mean difference = 5.01 mm; P < .001; Table 2; Graph 1). Tip: A small but statistically significant difference was observed between the two methods, with AI-generated models showing slightly higher tip values (mean difference = −0.85°; P < .001; Table 2; Graph 2). Torque: A small but statistically significant difference was also observed between CBCT and AI-generated torque measurements (mean difference = 0.67°; P = .045; Table 2; Graph 2). Agreement analysis Bland–Altman plots demonstrated systematic underestimation of root length by AI-generated models (Figure 8), minimal bias for torque (Figure 9), and slight bias for tip measurements (Figure 10).
Bland–Altman Plot Showing Agreement for Root Length Measurements.

Bland–Altman Plot Showing Agreement for Torque Measurements.

Bland–Altman Plot Showing Agreement for Tip Measurements.

Comparison of Mean Root Length Values Assessed by Cone-beam Computed Tomography (CBCT) and Intraoral Scan.

Comparison of Mean Tip and Torque Values Assessed by Cone-beam Computed Tomography (CBCT) and Intraoral Scan.
Results of Paired Samples t-test for Root Length, Tip, and Torque Measurements Between Cone-beam Computed Tomography (CBCT) (1) and Intraoral Scan (2).

Discussion
This study compared root length, tip, and torque measurements obtained from AI-supported planning software using intraoral scan data with CBCT-derived measurements, with CBCT serving as the reference standard.
Root Length
Root length measurements generated by the AI-supported software were significantly shorter than those obtained from CBCT (Tables 1 and 2; Graph 1; Figure 8). The AI software consistently estimated a root length of approximately 12 mm with no variation, suggesting that the software may rely on standardized anatomical templates rather than individualized patient-specific root reconstruction. Similar limitations have been reported by Lee et al., 1 who demonstrated that crown-based virtual orthodontic setups may inaccurately predict the true root position when only crown morphology is available.
Likewise, Lim et al. 3 emphasized that root length and root axis cannot be reliably inferred from crown morphology alone. Since intraoral scanners capture only the crown surface morphology, prediction of root morphology based solely on crown data remains limited. This limitation has also been highlighted in digital orthodontic model studies, which report that crown-based digital models cannot fully represent underlying root structures or anatomical variations. 5 The Bland–Altman analysis in the present study further demonstrated a proportional bias, with greater underestimation observed for longer roots, indicating that the discrepancy is more likely related to the AI-based root reconstruction algorithm rather than the intraoral scan itself. Therefore, CBCT continues to serve as the reference standard for accurate three-dimensional evaluation of root length and root morphology.
Tip
Tip measurements showed a statistically significant but clinically small difference between CBCT and AI-generated models (Table 2; Graph 2; Figure 10). This finding aligns with Lim et al., 3 who reported inherent uncertainty when estimating root inclination from crown morphology. Although the difference observed in this study was modest, such discrepancies may become relevant in cases requiring precise root positioning near cortical boundaries.
Torque
Torque measurements demonstrated good agreement between CBCT and AI-generated models, with no statistically significant difference (Table 2; Graph 2; Figure 9). This is consistent with Lee et al., 4 who showed that digital model superimposition can reliably capture torque changes when crown registration is accurate. These findings suggest that AI-supported software may be clinically acceptable for torque assessment, particularly when minimizing radiation exposure is desired.
Limitations
The present study has certain limitations. First, the analysis was limited to the maxillary left central incisor, which may restrict the generalizability of the findings to other teeth. Second, the AI-supported planning software generated a standardized root length value with no variation, suggesting reliance on predefined anatomical templates rather than patient-specific root morphology. This may limit the ability of the software to accurately evaluate individual variations in root length. Future studies, including multiple teeth and larger sample sizes, may provide further insights into the accuracy of AI-based root reconstruction. Results may not be generalizable to other teeth with different root morphologies.
Conclusion
Within the limitations of this study, the AI-supported planning software demonstrated significant underestimation of root length compared with CBCT. The software consistently generated a standardized root length value of approximately 12 mm, suggesting reliance on predefined anatomical templates rather than individualized patient-specific root reconstruction. Tip measurements showed a small but statistically significant difference, whereas torque measurements showed no statistically significant difference between the two methods. These findings indicate that AI-based reconstruction using intraoral scan data has limitations in accurately representing root length, and CBCT remains the reference standard for three-dimensional evaluation of root morphology and root length assessment.
Footnotes
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Ethics Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from all participants or their guardians.