
Abstract
Background
Malocclusion affects both functional and psychosocial aspects of oral health. While normative indices quantify treatment need, patient-reported measures reveal the quality-of-life implications. The treatment setting may influence these perceptions.
Objectives
To compare the difference in scores between patients attending a government (subsidized/free treatment) and private dental institution (paid treatment) regarding treatment need using the patient-reported measures such as the Malocclusion-Related Quality of Life Questionnaire (MRQoLQ) and the Psychosocial Impact of Dental Esthetics Questionnaire (PIDAQ), and the differences in the severity of malocclusion using the Peer Assessment Rating (PAR) index.
Methods
A multicenter cross-sectional comparative study was conducted among 242 patients (121 each from a Government Dental College (GDC)—Group 1 and a Private Dental College (PDC)—Group 2, aged 12-25 years. Malocclusion severity was assessed using the PAR index, while patient-reported outcomes were measured with PIDAQ and the MRQoLQ. Independent t-tests and chi-square tests assessed intergroup differences, and Pearson’s correlation examined associations between PAR and quality of life measures.
Results
Mean PAR scores were comparable between Group 1 and Group 2 (P > .05). However, PIDAQ and MRQoLQ scores were significantly higher among Group 2 patients (P < .01), indicating greater psychosocial and esthetic concerns despite similar malocclusion severity. Correlation analysis revealed stronger associations between PAR and patient-reported outcome measures (PROMs) in Group 1 patients, whereas Group 2 patients demonstrated higher expectations independent of normative severity.
Conclusion
While clinical malocclusion severity was similar across groups, orthodontic-specific quality of life impact was greater among PDC patients, reflecting heightened esthetic expectations. A combined approach incorporating both normative indices and patient-reported measures is essential for the assessment of orthodontic treatment need.
Keywords
Introduction
Malocclusion is one of the most prevalent oral health problems worldwide, and it has been shown not only to affect functional aspects of the dentition but also an individual’s psychosocial well-being and overall quality of life. Malocclusion is strongly associated with impairments in mastication, speech, and oral health maintenance. It can also cause dissatisfaction with dental appearance, reduced self-esteem, and social challenges, particularly during adolescence and young adulthood, when self-image is critical.1–5
Over the past two decades, patient-reported outcome measures (PROMs) have gained increasing importance in orthodontics, complementing traditional clinical indices such as the Peer Assessment Rating (PAR). 6 Among these, condition-specific outcome measures for orthodontics like the Malocclusion-Related Quality of Life Questionnaire (MRQoLQ), 7 and the Psychosocial Impact of Dental Esthetics Questionnaire (PIDAQ), 8 have been widely validated for capturing the subjective experience of malocclusion. These tools enable clinicians to better understand the psychological and social burdens associated with malocclusion, which may not be fully captured by objective measures alone.9–13
An additional dimension influencing the perception of malocclusion and treatment need is the socio-economic status and institutional context of care delivery.14, 15 In government-funded dental institutions, orthodontic treatment is typically provided at a subsidized rate or free of cost, but the accessibility depends on the case selection criteria and not on the patients’ esthetic concerns, potentially lowering patient expectations regarding esthetic outcomes. In contrast, in private institutions, treatment is paid for by patients, often representing a substantial financial investment. This financial outflow may heighten patient awareness and concerns of esthetics and psychosocial implications of malocclusion, thereby shaping their perception of treatment need and quality of life, which leads to more expectations for esthetic outcomes. To date, few studies have compared the psychosocial impact of malocclusion across patients seeking care in government versus private institutions, despite the important implications for health equity and the planning of health care delivery.16, 17
Against this background, the present study aims to compare the difference in scores between patients attending a government and a private tertiary care dental institution regarding the patient-reported measures of treatment need using MRQoLQ and PIDAQ, and the differences in the severity of malocclusion using the PAR index. The study also aimed to evaluate the correlation between PAR as reported by the operator and quality-of-life measures as reported by the patients. By integrating clinical and patient-reported outcomes across different treatment settings, this study sought to provide a more comprehensive understanding of the burden of malocclusion and also to find if there is any role for socio-economic norms and treatment settings in shaping patient expectations.
Materials and Methods
Study Design and Setting
This multicenter cross-sectional comparative study was conducted in the Department of Orthodontics and Dentofacial Orthopedics at two tertiary care dental institutions: a Government Dental College (GDC)—Group 1, where orthodontic treatment is provided at a subsidized rate/free of cost, and a Private Dental College (PDC)—Group 2, where treatment is fee-based. The study was registered with CTRI with the number CTRI/2022/12/048605. All procedures adhered to the Declaration of Helsinki (2013). 18
Sample Size
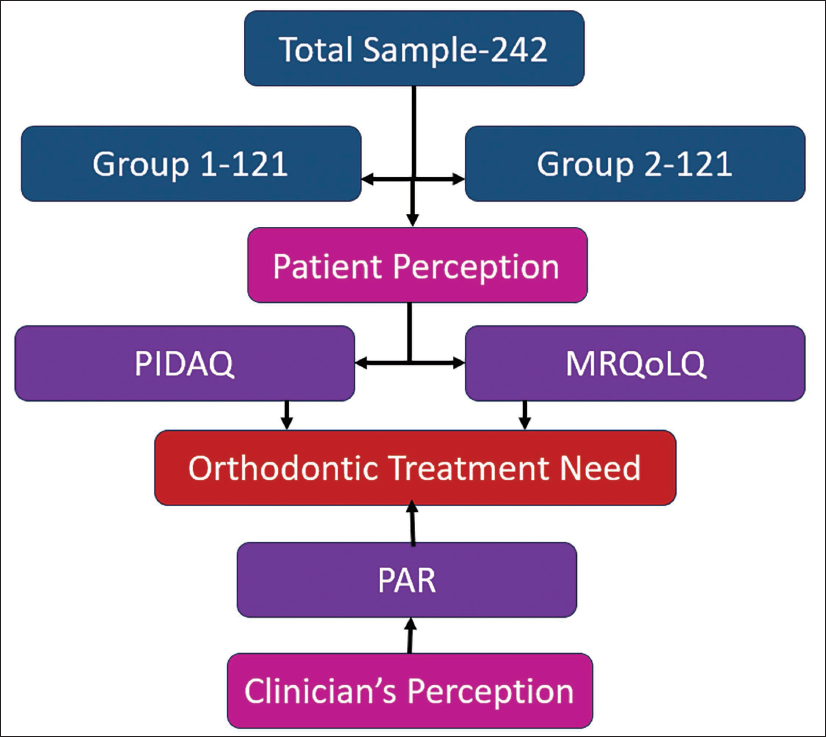
Based on a standard deviation of 10.5, an effect size of 3.66, a significance level of 5%, and a power of 90%, a minimum total of 216 patients was to be included in this multicenter study. 19 The final sample size included 242 patients, who were equally divided between groups so that there were 121 patients each in Group 1 and Group 2 (Figure 1).
Flow Chart Depicting the Study Design.
Selection of Participants
A total of 242 patients seeking orthodontic treatment were recruited consecutively, with 121 participants in each group from January 2023 till the desired samples were collected. Inclusion criteria were: age between 12 and 25 years, presence of permanent dentition, indication for fixed orthodontic treatment as per the institutional protocol, no prior history of orthodontic therapy, and consent to participate in the study. Exclusion criteria included patients with craniofacial anomalies, those indicated for orthognathic surgery, those with systemic conditions affecting bone and periodontal health, and those unable to complete self-administered questionnaires.
Data Collection
At baseline (prior to the initiation of orthodontic treatment), participants completed two validated PROMs:
MRQoLQ: Assessing psychological, socio-economic, orthodontic self-confidence, social, and functional impairment. PIDAQ: Assessing dental self-confidence, social impact, psychological impact, and esthetic concern.
Both instruments were self-administered in the participants’ native language, with assistance provided when necessary to clarify items.
Clinical Assessment
The severity of malocclusion was assessed using the PAR index. The PAR index scale uses the components: (a) upper and lower anterior segments, (b) left and right buccal occlusion, (c) overjet, (d) overbite, and (e) centerline, to get the total PAR score, which was then modified with a specific weightage for each component to get the final score. Impressions and orthodontic study models were obtained for each participant, and PAR scoring was performed by a calibrated examiner with a kappa value = 0.85.
Statistical Analysis
Data were entered into Statistical Package for the Social Sciences (SPSS) (version 26, IBM Corp., Armonk, NY, USA). Descriptive statistics were calculated for demographic and outcome variables. Group comparisons were performed using independent t-tests for continuous variables and chi-square tests for categorical variables. Pearson’s correlation coefficients (r) were used to assess relationships between PAR scores and MRQoLQ/PIDAQ scores in each group. A significance level of α = 0.05 was set for all tests.
Results
Sample Characteristics
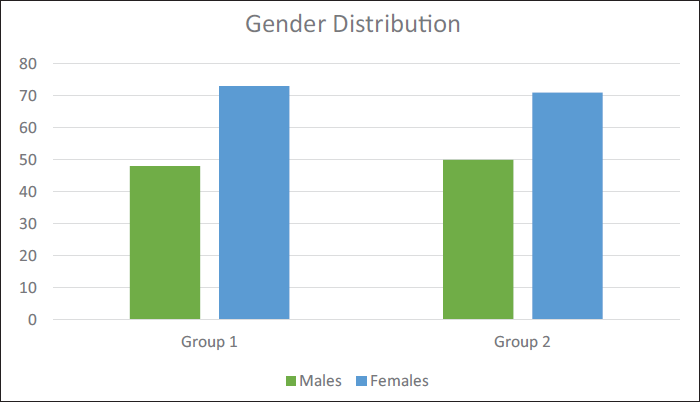
A total of 242 participants were included, with 121 each in Group 1 (GDC) and Group 2 (PDC). Gender distribution was comparable between the groups (Group 1: 48 males, 73 females; Group 2: 50 males, 71 females), with no significant difference (χ2, P = .793) (Figure 2). The age range was 12–25 years in both groups. The mean age was slightly lower in Group 1 (18.00 ± 3.04 years) compared to Group 2 (18.63 ± 3.03 years), showing a statistically significant difference (P = .018) (Table 1).
Gender Distribution of Participants in Group 1 and Group 2.
Basic Sample Characteristics, Including Gender Distribution and Age of the Participants, in Group 1 and Group 2.

MRQoLQ Scores
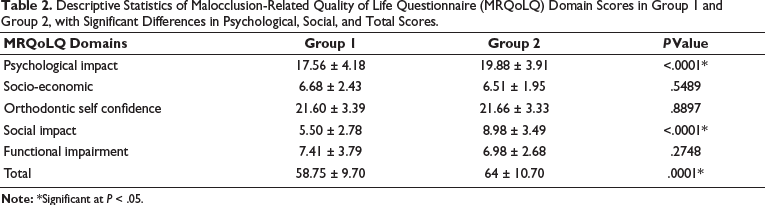
The comparison of MRQoLQ domains between groups showed significant differences in psychological impact and social impact. As compared to Group 1 (17.56 ± 4.18), Group 2 participants reported higher psychological impact (19.88 ± 3.91, P < .001) and higher social impact (8.98 ± 3.49 vs. 5.50 ± 2.78, P < .001). No significant differences were observed for socio-economic impact (P = .549), orthodontic self-confidence (P = .890), or functional impairment (P = .275). The total MRQoLQ score was significantly higher in Group 2 (64.00 ± 10.70) compared to Group 1 (58.75 ± 9.70, P = .001) (Table 2).
Descriptive Statistics of Malocclusion-Related Quality of Life Questionnaire (MRQoLQ) Domain Scores in Group 1 and Group 2, with Significant Differences in Psychological, Social, and Total Scores.
PIDAQ Scores
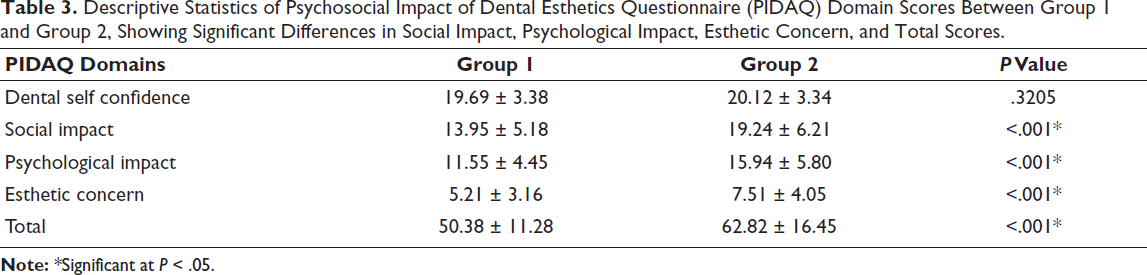
Analysis of PIDAQ domains revealed significantly higher negative impacts in Group 2 compared to Group 1 for social impact (19.24 ± 6.21 vs. 13.95 ± 5.18, P < .001), psychological impact (15.94 ± 5.80 vs. 11.55 ± 4.45, P < .001), and esthetic concern (7.51 ± 4.05 vs. 5.21 ± 3.16, P < .001). Dental self-confidence scores did not differ significantly between groups (P = .321) (Table 3). The total PIDAQ score was also significantly higher in Group 2 (62.82 ± 16.45) than in Group 1 (50.38 ± 11.28, P < .001).
Descriptive Statistics of Psychosocial Impact of Dental Esthetics Questionnaire (PIDAQ) Domain Scores Between Group 1 and Group 2, Showing Significant Differences in Social Impact, Psychological Impact, Esthetic Concern, and Total Scores.
PAR Scores
Baseline PAR scores were similar between groups (Group 1: 36.04 ± 12.60; Group 2: 36.68 ± 10.66), with no significant difference (P = .670) (Table 4).
Baseline Peer Assessment Rating (PAR) Scores of Group 1 and Group 2, with No Statistically Significant Difference Between the Groups.

Correlation Between PAR and MRQoLQ
A positive correlation was observed between PAR scores and MRQoLQ scores in both groups. In Group 1, the correlation was weak but significant (r = 0.24, P < .009) (Table 5). In Group 2, a moderately significant correlation was observed (r = 0.43, P < .00001).
Correlation of Peer Assessment Rating (PAR) with Malocclusion-Related Quality of Life Questionnaire (MRQoLQ) and Psychosocial Impact of Dental Esthetics Questionnaire (PIDAQ) in Group 1 and Group 2.

Correlation Between PAR and PIDAQ
Similarly, PAR scores correlated positively with PIDAQ scores. In Group 1, the correlation was weak but significant (r = 0.30, P < .001) (Table 5). In Group 2, the correlation was moderate and significant (r = 0.36, P < .0001).
Discussion
The present study compared MRQoLQ and PIDAQ with normative orthodontic treatment need, using the PAR index, among patients attending a government (GDC—Group 1) and a private (PDC—Group 2) dental institution.
The demographic profile of participants showed no significant differences in gender distribution. A statistically significant but small difference in mean age between the two groups may be explained by institutional and socio-economic factors influencing treatment-seeking behavior. Patients reporting to government institutions are often younger, as these centers provide low- or no-cost treatment and are centers to which adolescents are referred directly from schools or community dental services. In contrast, patients in private institutions may initiate treatment slightly later, often after family financial planning or when esthetic concerns become more prominent in late adolescence or early adulthood. Although statistically significant, the age difference of less than 1 year is unlikely to have any meaningful clinical impact on the overall findings. This suggests that the groups were largely comparable in terms of baseline characteristics.
Both the MRQoLQ and the PIDAQ were employed to provide a comprehensive assessment of the patients’ quality of life and psychosocial well-being in relation to their malocclusion. While the MRQoLQ is a condition-specific instrument designed to evaluate the functional and emotional impact directly attributable to malocclusion, the PIDAQ specifically measures the psychosocial consequences of dental esthetics. By incorporating both instruments, the study captures a broader spectrum of patient-centered outcomes, ranging from functional limitations to self-perceived social and emotional impacts. These subjective measures were then correlated with the PAR index, an objective clinical measure of malocclusion severity, to explore the relationship between clinical orthodontic treatment needs and the patient’s perceived orthodontic treatment need, based on its effect on quality of life. The combined use of these questionnaires strengthens the validity of the study by ensuring that both functional and psychosocial dimensions of malocclusion are addressed alongside objective clinical parameters.
Analysis of MRQoLQ revealed that patients in Group 2 reported significantly greater psychological and social impacts compared to Group 1, while other domains, such as socio-economic, orthodontic self-confidence, and functional impairment, did not differ significantly. Socio-economic impact evaluation was done with MRQoLQ, as it has an incorporated socio-economic domain. In the socio-economic domain, a question is about whether family income reduces the chances of treatment options. The response to this question was not significantly different between both groups. When considering the total MRQoLQ scores between groups, it was higher among the PDC patients. This indicates that the psychological and social dimensions of malocclusion exerted a stronger influence on the perceived quality of life in Group 2 subjects. Previous studies have consistently highlighted that psychosocial domains are more affected by malocclusion than functional aspects, especially during adolescence and early adulthood when self-image and peer perception are most critical.1, 14, 17, 20
The PIDAQ results further support this interpretation.21, 22 Group 2 participants reported significantly greater social impact, psychological impact, and esthetic concern, while dental self-confidence did not differ between the groups. The higher total PIDAQ scores in Group 2 indicate that malocclusion exerted a more pronounced negative psychosocial effect in this population. These findings align with earlier reports that malocclusion severity is strongly associated with diminished psychosocial well-being and esthetic self-perception.2, 10, 23
An important factor that may explain these differences is the institutional setting. In the government institute (GDC), orthodontic treatment is offered at a subsidized rate or free of cost, while in the private institution (PDC), patients incur direct financial expenditures. This economic dimension may heighten patient expectations and awareness of esthetics in the private setting, thereby amplifying the psychosocial impact of malocclusion. Patients who seek treatment in private institutions may also be coming from socio-economic backgrounds where esthetics and social image are highly valued, increasing the likelihood of reporting greater psychological and social distress associated with malocclusion. In contrast, patients at government centers may prioritize accessibility and affordability, as they are given accessibility according to the set norms for patient selection, over esthetic concerns, potentially explaining the relatively lower MRQoLQ and PIDAQ scores despite similar objective severity of malocclusion. This interpretation resonates with earlier findings that treatment expectations, socio-economic context, and cost considerations can significantly influence perceived quality of life outcomes.14, 24, 25
The PAR index was calculated by incorporating all relevant components of malocclusion assessment, namely, the upper and lower anterior segments, left and right buccal occlusion, overjet, overbite, and midline deviation. The PAR scores, 26 which reflect objective malocclusion severity, were similar between the two groups. The similarity in PAR index scores between patients treated in government and private dental colleges (PDCs) may be explained by the fact that only patients with moderate to severe malocclusions, requiring specialized orthodontic care, are generally managed in both these tertiary care institutions. Consequently, the baseline severity of malocclusion is comparable across both settings, which minimizes variability in PAR scores between the two groups. This indicates that the observed differences in psychosocial impact were not due to clinical differences in malocclusion, but rather to differences in perception shaped by institutional factors. 27 Such discrepancies between objective orthodontic indices and patient-reported outcomes have been well documented by Sun et al. and Dimberg et al.28, 29
Correlation analysis provided further insight into this relationship. Both MRQoLQ and PIDAQ scores showed a positive association with PAR scores in Group 1 and Group 2, although the strength of the association varied. Notably, Group 2 demonstrated a stronger correlation, suggesting that malocclusion severity was more closely aligned with self-perceived and psychosocial concerns in this cohort. This may again reflect the influence of treatment costs and higher esthetic expectations in the private setting, where malocclusion is perceived as a more significant psychosocial burden. This may further be explained by the fact that subsidized care in GDC is given according to a set case selection criterion rather than just the self-perceived psychosocial concern.
Taken together, these findings highlight the complex interplay between clinical severity, psychosocial impact, and socio-economic context of orthodontic treatment.30, 31 While objective indices such as the PAR score remain essential for assessing treatment need, patient-reported outcomes provide critical insights into the psychological and social burden of malocclusion in society that comes to an institution for orthodontic treatment. The results suggest that clinicians should give greater weight to psychosocial measures and patient expectations when prioritizing and planning orthodontic care, particularly in private institution settings where esthetic concerns and financial investment are often more pronounced.
While this study has certain limitations, its findings provide valuable insights. The cross-sectional design limits the causal interpretation of the relationship between malocclusion severity and quality of life; however, it offers a meaningful snapshot of patients’ perceptions at the start of treatment. Differences in cultural, socio-economic, and institutional contexts between government and private colleges may have influenced subjective responses, yet the inclusion of both settings adds depth and diversity to the analysis. Expanding the sample to include more institutions with geographic and cultural matching would further enhance the generalizability of the results.
Conclusion
The findings of this study demonstrate that
Despite comparable clinical severity of malocclusion, patients attending a private institution (PDC) reported significantly higher psychosocial and quality-of-life impacts compared to those at a government institution (GDC). Malocclusion severity, as measured by the PAR index, correlated positively with MRQoLQ and PIDAQ scores, with stronger associations observed in the private setting. These results emphasize the importance of considering both objective orthodontic indices and subjective patient-reported measures to determine an individual’s perceptions for seeking orthodontic treatment, particularly within the broader socio-economic and institutional context of orthodontic care. A future longitudinal study is ongoing to build on these findings by assessing changes in quality of life after orthodontic treatment and examining how factors such as treatment costs, expectations, and satisfaction after treatment influence psychosocial outcomes.
Footnotes
Acknowledgments
The authors would like to acknowledge the Kerala University of Health Sciences.
Authors Contribution
Prathapan Parayaruthottam: Conceived the research idea, designed the study, collected data, conducted data analysis, and drafted the manuscript.
Shobha Sundareswaran: Contributed to manuscript writing and provided supervision throughout the project.
Vincy Antony: Reviewed literature, contributed to manuscript drafting, and provided critical revisions.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was approved by the Institutional Ethics Committees of both institutions-IEC numbers from two centers (multicenter study): 220/2021/DCC and IEC/MES/74/22.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from SBMR, Kerala State.
Informed Consent
Written informed consent was obtained from all participants (or parents/guardians for those under 18 years).
Patient Release
Images obtained do not contain identifiable patients or human subjects.