
Abstract
Objectives
Orthodontic root resorption is a common, unavoidable, and undesirable side effect of orthodontic treatment, particularly during anterior tooth retraction and intrusion. Early identification of patients at risk can guide treatment planning and reduce complications. Biomarkers such as cementum protein-1 (CEMP-1), dentin sialophosphoprotein (DSPP), and matrix metalloproteinase-9 (MMP-9) have been proposed as potential diagnostic tools for assessing root resorption risk. The objectives of this study were to evaluate and compare the diagnostic accuracy of CEMP-1, DSPP, and MMP-9 in predicting severe orthodontically-induced root resorption using receiver operating characteristic (ROC) analysis.
Materials and Methods
This prospective observational study involved forty patients undergoing fixed orthodontic treatment with either retraction alone (Group 1) or combined retraction and intrusion using skeletal anchorage (Group 2). Gingival crevicular fluid (GCF) samples were collected and analyzed for CEMP-1, DSPP, and MMP-9 levels at designated time points. Root resorption severity was assessed radiographically and graded. ROC curve analysis was performed to determine the area under the curve (AUC), sensitivity, specificity, and diagnostic capability of each biomarker in identifying severe (grading ≥2) root resorption.
Results
CEMP-1 demonstrated the highest diagnostic accuracy with an AUC of 0.757, followed by DSPP with an AUC of 0.729. MMP-9 showed no significant predictive ability (AUC = 0.583).
Conclusion
Among the three biomarkers tested, CEMP-1 demonstrated the most promising diagnostic potential for identifying patients at risk for severe root resorption. Incorporating biochemical monitoring with traditional radiographic assessment may enhance early detection and allow for more personalized orthodontic interventions.
Keywords
Introduction
Root resorption is an undesirable but unavoidable consequence of orthodontic treatment and can range from mild to severe root resorption (>2 mm).1, 2 The prevalence of severe root resorption ranges from 2% to 5% and this can have clinically significant consequences, like reduced crown-to-root ratio, which may affect the long-term viability of the dentition.3, 4 Risk factors causing orthodontic root resorption have been categorized in scientific literature as general and local factors.5, 6
Radiographs and cone-beam computed tomography (CBCT) are currently being used to evaluate root resorption during orthodontic treatment.7–9 Recent research has revealed the use of Gingival crevicular fluid (GCF) to analyze protein biomarkers as it potentially offers numerous benefits, including non-invasiveness, ease of use, and earlier determination of severity of resorptive activity.10, 11 The outcome of previous studies has proved that certain biomarkers, such as dentin sialoprotein (DSP), are found to be associated with root resorption.12–14 DSP and dentin phosphoprotein (DPP) are components of the larger dentin sialophosphoprotein (DSPP) protein, cleaved into its functional domains, DPP and DSP, by matrix metalloproteinase-9 (MMP-9).15, 16 Additionally, cementum protein-1 (CEMP-1) serves as a marker for cementoblast-related cells. 17 A gap exists in the current literature regarding the quantification of specific protein biomarkers in GCF, in relation to the severity of orthodontic root resorption, particularly when assessed at multiple clinical stages in patients treated with fixed orthodontic appliances.
While several biomarkers have been implicated in the pathogenesis of orthodontically-induced inflammatory root resorption (OIIRR), their diagnostic utility remains to be clearly defined. Receiver operating characteristic (ROC) analysis provides a comprehensive approach to evaluate diagnostic performance. Therefore, the present study aimed to assess the diagnostic accuracy of DSPP, CEMP-1, and MMP-9 in identifying severe root resorption using ROC analysis.
Materials and Methods
Study Design
This prospective cohort study was approved by the Institutional Ethical Committee (IEC/MES/73/2022) and adhered to the Declaration of Helsinki 2013. The study was registered with the Clinical Trials Registry of India (CTRI/2022/12/048605).
Sample Size Estimation
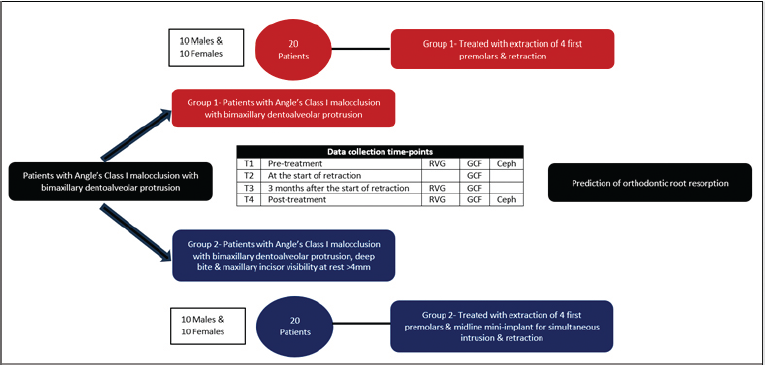
Based on a standard deviation of 0.05, an effect size of 0.097, a significance level of 5%, a power of 90%, and a 20% loss to follow-up, a minimum of seven patients were to be included in each group. 18 Sampling was carried out using a consecutive sampling approach, involving patients who presented to the Department of Orthodontics at the affiliated institution. Forty patients were divided into two groups of 20 each (Groups 1 and 2) with equal gender distribution, as illustrated in Figure 1 and Table 1. Groups 1 and 2 underwent anterior teeth retraction using active tie-backs following first four premolar extractions; additionally, Group 2 underwent simultaneous intrusion of the maxillary anterior teeth using midline mini-implants.
Distribution of Study Participants.

Study Design Flow Chart.
Selection of Participants
The inclusion criteria were defined as patients aged 13-25 years with Angle’s class I bimaxillary dentoalveolar protrusion, requiring therapeutic extraction of maxillary first premolars, complete dentition (excluding third molars), and no radiographic evidence of prior root resorption. Group 2 patients met the same criteria, with the addition of increased maxillary incisor visibility at rest (>4 mm), and were treated with simultaneous intrusion and retraction using midline mini-implants (Table 1).
Exclusion criteria included missing molars or anterior teeth, prior orthodontic treatment, supernumerary teeth in the maxillary anterior region, impacted canines, endodontically-treated teeth, upper anterior crowding of 4 mm or more, and history of systemic diseases/medications/trauma.
Method
At the beginning of treatment, the patients received oral prophylaxis and oral hygiene instructions. All patients in both groups underwent fixed orthodontic treatment using pre-adjusted edgewise brackets 0.022″ MBT prescription (Ormco Mini 2000, Ormco Corporation, Glendora, CA) after the extraction of first four premolars. A uniform bonding protocol was applied to all patients. 19 The alignment phase began with 0.016″ Nitinol wires, progressing to 0.017″ × 0.025″ Nitinol, 0.019″ × 0.025″ Nitinol, and finally 0.019″ × 0.025″ rectangular stainless-steel wires for the en masse retraction of the anterior teeth. In Group 2 patients, following alignment, a self-drilling mini-implant (Implant Genesis, 1.4 × 8 mm) was placed between the root tips of the maxillary central incisors, positioned 6-8 mm from the midline of the alveolar crest. A retraction force of 200 g was applied to both groups using active tie-backs. 20 A light force of 50 g was applied for intrusion using an elastomeric chain in the midline mini-implant group. 21 All clinical procedures were carried out by the same investigator. Instructions for maintaining oral hygiene were given to all the patients, along with mid-treatment oral prophylaxis. 22 All methods were reported in accordance with the STROBE (strengthening the reporting of observational studies in epidemiology) guidelines.
Outcome Assessment
The time-points for outcome assessment, both radiovisiography (RVG) as well as GCF collection, are shown in Figure 1.
GCF Collection
The maxillary incisors were isolated using cotton rolls, and GCF was collected by inserting PerioPaper strips (Oraflow Inc., Hewlett, New York, USA) into the mesio-buccal and disto-buccal regions of the gingival sulcus for 30 s. 23 At intervals of 1 min, new strips were placed. Strips contaminated with blood were excluded from the study. The strips containing GCF were placed in sterile Eppendorf vials containing phosphate-buffered saline, centrifuged at 4°C for 10 min, and subsequently stored at −80°C in the Department of Microbiology at the affiliated institution until further analysis. Biomarker concentrations were determined using a sandwich enzyme immunoassay with an ELISA kit (96T, Origin Diagnostics and Research) following the manufacturer’s protocol for testing each biomarker. The specific biomarker levels were quantified by comparing the optical density readings to the standard curve.
RVG
Digital intraoral periapical radiographs were taken using an RVG machine (RVG-4, Trophy Radiologie S.A., Croissy-Beaubourg, France) with exposure parameters set at 65 kVp, 8 mA, and an exposure time of 0.2 s. An RVG sensor positioner was used for standardization, and the paralleling cone technique was employed to maintain a consistent object-to-sensor distance. 24 Pre-treatment RVG images were used as a baseline, and the degree of root resorption for each maxillary incisor was assessed and recorded by the same investigator using the grading system of the Malmgren classification modified by Beck and Harris (Table 2).25, 26 The values of the four incisors were then tabulated, and the average was taken.
Modified Malmgren Grading Scale-index for Grading Root Resorption.

Statistical Analysis
To minimize potential bias and ensure operator blinding during treatment, participants were assigned unique identification numbers, and all data collection and assessments were conducted using these coded identifiers. Although blinding of participants was not feasible, outcome data were anonymized and coded prior to statistical analysis to reduce the risk of bias during data interpretation. The statistical analyses were performed using International Business Machine (IBM) Statistical Package for the Social Sciences (SPSS) Statistics version 26.0 (IBM Corp., Armonk, NY), with a significance threshold set at P < .05. Descriptive statistics were conducted to evaluate the mean and standard deviation of each group. The normality of the data was assessed using the Shapiro–Wilk test. Inferential statistics to find out the difference between the groups was done using repeated-measures ANOVA comparing the multiple time points. An independent t-test was used to compare the differences between the groups when assessing the grades of root resorption. To evaluate the diagnostic performance of the biomarkers, ROC curve analysis was conducted. The area under the curve (AUC) was calculated for DSPP, CEMP-1, and MMP-9 to determine their sensitivity and specificity in discriminating between severe (grading ≥ 2) and non-severe (grading < 2) root resorption using the grading system of the modified Malmgren classification.25, 26 An AUC value closer to 1.0 indicated higher diagnostic accuracy.
Results
Demographic Characteristics
A total of 40 participants were included in the analysis, divided into two groups of 20 each (Groups 1 and 2). Participants ranged in age from 13 to 25 years, and the mean age of patients in Groups 1 and 2 was 18.1 ± 2.13 years and 18.2 ± 3.11 years, respectively. The independent-samples t-test revealed no statistically significant difference in the mean age between the two groups (P > .05), confirming age-matching between cohorts. The sample consisted of both male and female subjects, with equal gender distribution, and was coded as one (male) and two (female). Shapiro–Wilk test indicated that the variables were normally distributed (P > .05).
Comparison of Biomarkers
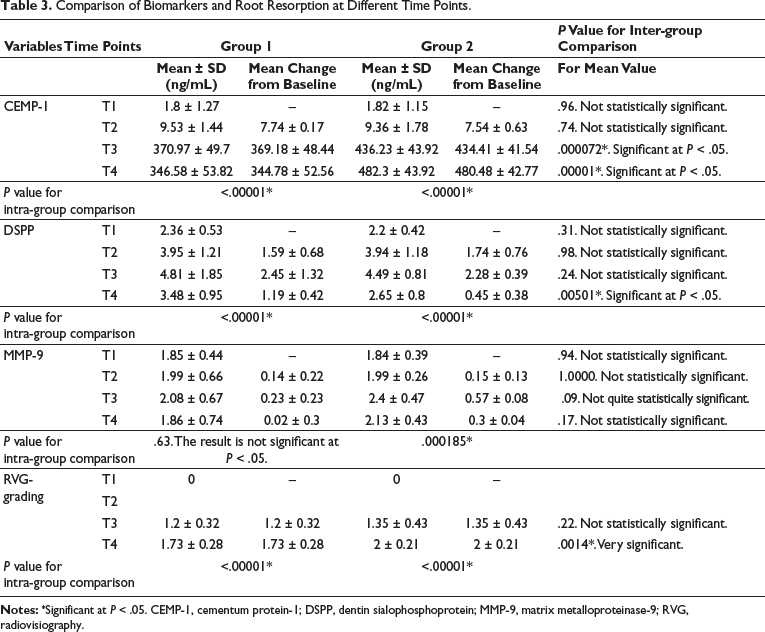
Comparison of Groups 1 and 2 within each group revealed that CEMP-1 levels were significantly higher in Group 2 at T4 (P < .001), suggesting a greater degree of cementum remodeling associated with intrusive mechanics. DSPP levels showed a significant change in Groups 1 and 2. MMP-9 levels increased significantly from T1 to T4 in Group 2 (P = .01), while Group 1 showed no significant change (P = .63).
Comparison of Grades of Root Resorption
Grading variables, which represent the severity or extent of root resorption, were assessed. At T1, the grading of root resorption was consistently zero across all participants, while T3 and T4 showed some variation between groups, with Group 2 tending to have slightly higher mean grading values. RVG at T4 revealed a statistically significant increase in root resorption in both groups (P < .05). The mean difference of grading of root resorption was higher in Group 2 at T4 (2 ± 0.21) compared to Group 1 (1.73 ± 0.28) (Table 3).
Comparison of Biomarkers and Root Resorption at Different Time Points.
Severity of root resorption was categorized as severe (≥2) and not severe (<2) using the grading system of the Malmgren system modified by Beck and Harris25, 26 (Table 4). A Chi-square test was conducted to compare the distribution of grading of root resorption severity between Groups 1 and 2. The results revealed a statistically significant difference between the groups (χ2 = 6.67, df = 1, P = .010). Group 2 exhibited a higher proportion of severe resorption cases (80%) compared to Group 1 (40%).
Comparison of Root Resorption Severity Between Groups.

Diagnostic Performance of Biomarkers
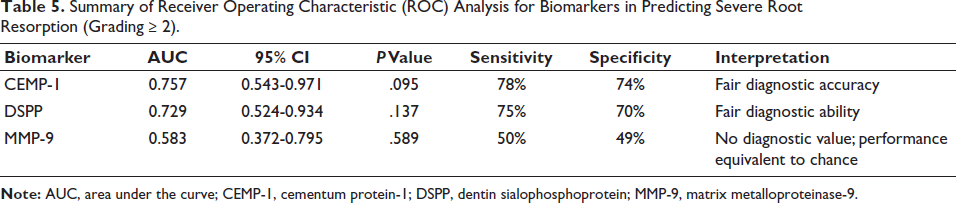
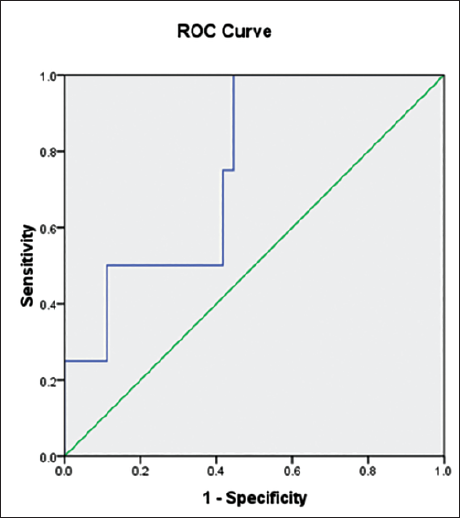
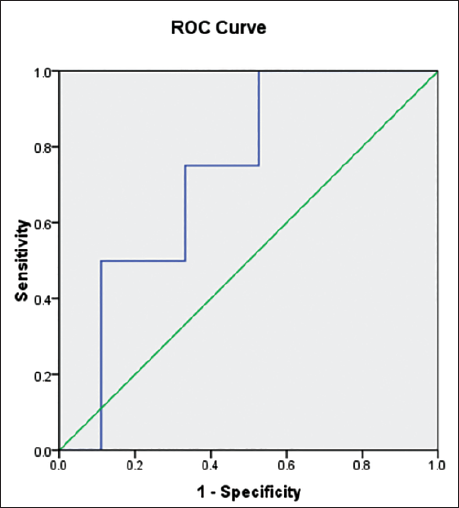
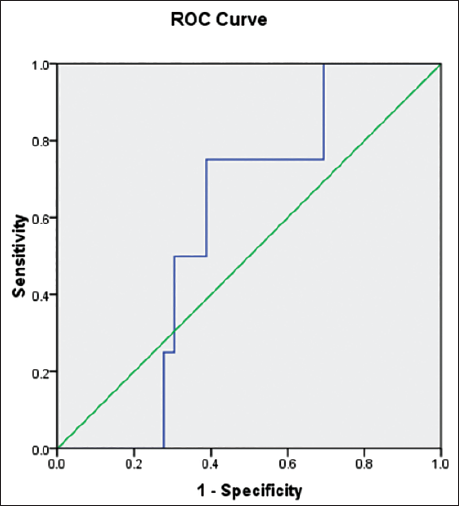
ROC analysis was used to evaluate the diagnostic accuracy of biomarkers in predicting severe root resorption (Grade ≥2). Among the three biomarkers assessed, CEMP-1 demonstrated the highest diagnostic accuracy with an AUC of 0.757 (95% CI: 0.543-0.971; P = .095), suggesting fair discriminative ability. DSPP also showed a fair level of diagnostic utility, with an AUC of 0.729 (95% CI: 0.524-0.934; P = .137), though this result did not reach statistical significance. In contrast, MMP-9 showed poor diagnostic performance with an AUC of 0.583 (95% CI: 0.372-0.795; P = .589), indicating no better accuracy than random chance (Table 5). The ROC curve in Figures 2–4 visually represent these findings, illustrating the diagnostic performance of each biomarker.
Summary of Receiver Operating Characteristic (ROC) Analysis for Biomarkers in Predicting Severe Root Resorption (Grading ≥ 2).
Receiver Operating Characteristic (ROC) Curve Comparing the Diagnostic Performance of Cementum Protein-1 (CEMP-1).
Receiver Operating Characteristic (ROC) Curve Comparing the Diagnostic Performance of Dentin Sialophosphoprotein (DSPP).
Receiver Operating Characteristic (ROC) Curve Comparing the Diagnostic Performance of Matrix Metalloproteinase-9 (MMP-9).
Discussion
This pioneering observational study uniquely examines how three distinct tissue-specific biomarkers impact orthodontic root resorption at different clinical time-points in patients undergoing fixed orthodontic treatment. A comprehensive evaluation was performed to rigorously test the study’s hypothesis. This study evaluated the clinical and diagnostic utility of three biomarkers—CEMP-1, DSPP, and MMP-9—in OIIRR. As per Taba et al., 27 a biomarker is a measurable indicator of physiological or pathological processes. In orthodontics, where subclinical tissue changes precede radiographic evidence, biomarkers offer a promising avenue for early detection.
In the present study, patients were divided into two groups: those with and without orthodontic intrusion using midline mini-implants. This grouping was intended to determine whether any significant changes in biomarker levels and RVG findings could be attributed specifically to intrusion forces, which have been previously associated with an increased risk of orthodontically-induced root resorption.28, 29 Data collection were performed at four distinct time-points in both groups, each corresponding to critical phases of the orthodontic treatment process (Figure 1). These time-points were selected for their clinical relevance, as they represent key milestones reflecting changes in biological response and treatment progression.
Biological Relevance of Biomarkers
MMP-9 plays a pivotal role in extracellular matrix degradation and osteoclastic activity, thus being implicated in root resorption.30, 31 DSPP, a dentin-specific protein, is cleaved into DPP and DSP and is linked to dentin matrix turnover.16, 32 CEMP-1 is secreted by cementoblasts and reflects cementum remodeling.17, 33
Temporal and Group-wise Trends
The temporal expression of these biomarkers revealed distinct patterns. CEMP-1 showed a significant increase in both groups, particularly in Group 2, consistent with its role in cementum remodeling during intrusive forces. DSPP increased significantly in Group 1, indicating a possible protective or reactive dentin response in patients not subjected to intrusive forces. Moreover, DSP and DPP are components of the larger DSPP protein, cleaved into its functional domains, DPP and DSP, by MMP-9. 34 This could be another explanation for the reduction of DSPP observed in Group 2 patients. In concordance with this, it was observed that MMP-9 increased significantly only in Group 2, aligning with greater tissue remodeling and potential resorption.
ROC analysis provides a robust statistical framework for evaluating the diagnostic accuracy of biomarkers. It quantifies the ability of a test to correctly classify cases (e.g., severe vs. not-severe root resorption) by plotting Sensitivity (True positive rate) against 1- Specificity (False positive rate) across various thresholds. 35 The AUC serves as a summary measure of overall test performance: values closer to 1 indicate high diagnostic accuracy, while values near 0.5 imply no discriminative capability. ROC analysis is particularly valuable in comparative studies, as it enables the ranking of multiple candidate biomarkers based on objective performance metrics.10, 36
ROC curve analysis emphasized the clinical relevance of these biomarkers. CEMP-1 exhibited the highest diagnostic performance, with an AUC of 0.757, indicating fair discriminative ability. The identification of a specific cut-off value (439.82) further enhanced the clinical applicability of CEMP-1 for differentiating cases of severe root resorption. An AUC between 0.7 and 0.8 suggests that the biomarker can be reliably used for diagnostic purposes in a clinical setting, though values closer to 1 are desired for excellent discrimination. 37 The superior performance of CEMP-1 was likely due to its direct role in cementum repair, making it a promising candidate for early detection of resorptive activity. In the absence of statistical significance, the current evidence does not justify the clinical adoption of CEMP-1 as a standalone diagnostic tool for severe root resorption. The fair discriminatory ability observed should be considered as hypothesis-generating rather than confirmatory. DSPP yielded an AUC of 0.729, also indicating fair discriminative power. This result suggests DSPP is a valuable adjunctive marker; although its performance is slightly lower than CEMP-1, it may still contribute meaningfully to risk assessment if used in combination with other markers. MMP-9, with an AUC of 0.583, showed poor discriminatory ability for severe root resorption.
The diagnostic performance of each biomarker must be interpreted in light of its expression kinetics, biological half-life, and metabolic turnover. In particular, the relatively poor discriminative ability of MMP-9 (AUC = 0.583) observed in this study may be attributable to its known temporal expression profile. MMP-9 plays a key role in later stages of the inflammatory cascade and extracellular matrix degradation, often exhibiting delayed or variable expression in response to mechanical loading. 30 Therefore, the sampling time-point may not have coincided with its peak activity, potentially leading to underestimation of its clinical utility. In contrast, CEMP-1 and DSPP are associated with cementoblast function and active tissue remodeling. Their kinetic profiles may therefore better match the timing of biomarker sampling in this study, contributing to their superior diagnostic performance. These results suggested that CEMP-1 and DSPP may have potential utility as biomarkers for identifying patients at risk of severe root resorption during orthodontic treatment, whereas MMP-9 appeared to be less reliable in this capacity.
The findings align with earlier reports that dentin- and cementum-specific markers provide higher specificity than general inflammatory markers.12, 38 Kereshanan et al., 13 Balducci et al., 12 and Ghaleb et al. 18 found DSP and DPP in GCF to be associated with root resorption. Other studies, including those by Kunii et al. 39 have validated inflammatory cytokines like IL-6, but these lack specificity.
Comparison of Orthodontic Root Resorption Severity Between Groups
Radiographic grading showed significantly higher root resorption scores in Group 2 at T3 and T4 time-points, reinforcing the impact of increased intrusive forces. Chi-square analysis indicated that 80% of Group 2 participants experienced a grading of ≥2 resorption compared to 40% in Group 1. These findings suggested that subjects in Group 2 were significantly more likely to experience greater root resorption, highlighting the potential impact of treatment mechanics associated with that group. This aligns with the observations of Linge and Linge, 40 Dermaut and De Munck, 41 and Zhou et al., 42 who found intrusion particularly damaging due to apical force concentration. The increased resorptive severity in Group 2 may be attributed to the combined intrusion-retraction mechanics, which impose concentrated forces on the apical regions of the roots. These types of forces create areas of hyalinization and intense osteoclastic activity, which are hallmarks of resorptive processes. Moreover, Group 2 may have experienced a longer duration of sustained force, a factor known to exacerbate root damage. 5 This observation aligns with the findings of Smale et al., 43 who reported greater root shortening in cases involving significant incisor movement, particularly in patients with pre-treatment incisor proclination and thin cortical bone support. Conversely, Parayaruthottam and Antony 44 in their case report demonstrated minimal resorption with carefully controlled intrusion.
Clinical Implications
These findings validate the association between force vectors and root resorption severity and highlight the value of CEMP-1 as a diagnostic biomarker. Integrating biomarker analysis with clinical evaluation can refine treatment planning, especially in high-risk individuals for OIIRR or those requiring complex movements like intrusion.
Limitations and Future Direction
This study has certain limitations that should be acknowledged. The relatively modest sample size may limit the generalizability of the findings and the statistical power to detect smaller effect sizes. In addition, the use of two-dimensional RVG for assessing root resorption, while practical and commonly used in clinical settings, may underestimate the true extent of OIIRR due to its limited ability to capture changes on non-visible root surfaces. Future research incorporating larger, more diverse patient cohorts and advanced three-dimensional imaging, such as CBCT, is recommended to validate these preliminary observations and enhance diagnostic accuracy before clinical implementation. Chairside biomarker kits could revolutionize diagnosis by enabling real-time monitoring. Expansion of the biomarker panel and mechanistic studies is warranted to enhance predictive models.
Conclusion
A biomarker-based approach can enhance early detection and personalization in orthodontic care, reducing the burden of irreversible root damage. This study identifies CEMP-1 as a promising biomarker with fair diagnostic accuracy for predicting severe orthodontic root resorption, while DSPP shows potential, albeit with less definitive predictive power. The limited utility of MMP-9 in this context suggests that relying on a single biomarker may be insufficient for accurate risk assessment.
Clinically, incorporating biomarker evaluation—particularly CEMP-1—into routine orthodontic monitoring could facilitate earlier identification of patients at higher risk of significant root resorption. This, in turn, would enable timely modification of treatment mechanics, such as adjusting force magnitude or treatment duration, to mitigate adverse outcomes. Ultimately, a multi-marker diagnostic approach, combined with advanced imaging and personalized treatment planning, holds promise for enhancing patient safety and improving long-term orthodontic treatment success.
Footnotes
Acknowledgment
The authors would like to acknowledge the support of the Department of Microbiology, MES Medical College, Perinthalmanna, Kerala, India.
Declaration of Conflict of Interests
The authors declared no potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Indian Orthodontic Society-Research Fund 2022-23 (IOS-RF-LM).
Informed Consent
Written informed consent/assent was obtained from all subjects who participated in this study.