
Abstract
Background
Temporomandibular disorders (TMD) involve dysfunction and pain in the temporomandibular joint (TMJ) and its associated structures. Although multifactorial, the influence of occlusal factors on TMD remains controversial. This study aimed to assess the prevalence of TMD in young adults and to examine its association with functional and static occlusal parameters.
Aim
To determine the prevalence of TMD and evaluate the relationship between TMD and occlusal characteristics in university students.
Materials and Methods
A cross-sectional study was conducted among 200 university students aged between 18 and 28 years. TMD was diagnosed using the diagnostic criteria (DC)/TMD Axis I Pain Screener and a clinical examination. Functional and static occlusal parameters, including centric relation-maximum intercuspation (CR-MIP) discrepancy, excursive movements, mouth opening, overjet, overbite, midline deviation, and molar relationship, were clinically assessed in an equal number of participants with signs and symptoms of TMD and non-TMD. Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) Version 25, applying descriptive statistics and one-way analysis of variance (ANOVA), with significance set at P < .05.
Results
The overall prevalence of TMD was reported to be 19%. Functional discrepancies, such as CR-MIP position shift and limited lateral excursive movements, were significantly more common in individuals with TMD (P < .0001). Reduced maximum mouth opening was also observed. Among static traits, overbite showed a significant correlation (P = .021), whereas overjet, molar relationship, and crossbites did not. A cumulative effect was noted in participants with multiple occlusal discrepancies.
Conclusion
TMD is prevalent among young adults, with functional occlusal discrepancies showing a stronger association than static traits.
Keywords
Introduction
Temporomandibular disorders (TMD) are defined as conditions that impair the functional integrity of the temporomandibular joint (TMJ) and associated musculature, often resulting in pain, restricted movement, and joint sounds. 1 TMD represents a multifactorial condition, with proposed etiological factors including structural irregularities, trauma, muscular hyperactivity, psychological stress, and occlusal interference.2, 3 Despite the growing literature, the precise role of occlusion in TMD remains contentious, largely due to individual adaptive capacities and the multifaceted nature of the disorder. 4
Epidemiological studies across different populations are essential, as prevalence and symptom expression are influenced by regional, environmental, and cultural factors. 5
The prevalence of TMD among individuals with malocclusion ranges from 15.6% to 78.9%, as demonstrated by a systematic review and meta-analysis that evaluated 18 studies involving 11,348 participants. This wide range is primarily due to variations in sample sources, diagnostic criteria (DC), and study methodologies. 6 Clinical assessments often yield lower prevalence rates compared to self-reported questionnaires. 7 In India, limited large-scale epidemiological studies using standardized criteria such as the DC/TMD exist, creating a gap in reliable prevalence data. 8
Diagnostic challenges have historically complicated TMD research, prompting the development of structured tools such as the DC/TMD Axis I, which offers standardized protocols for identifying muscle disorders, joint conditions, and disc displacements. 1 This has allowed greater consistency across clinical investigations, improving the comparability of findings.
Occlusion, particularly functional factors like centric relation-maximum intercuspation (CR-MIP) discrepancy and lateral excursive movement, has been implicated in TMD development. Theories such as canine guidance, group function, and balanced occlusion explain variations in mandibular movement and contact points, each influencing load distribution on the TMJ.9, 10 Static occlusal traits, including overbite, overjet, midline deviation, and Angle’s classification, have also been investigated for their possible association with TMD. 11 However, conclusions have been inconsistent, with some studies indicating negligible correlations. 12
Additionally, psychological stress and parafunctional habits such as clenching or bruxism have been independently associated with TMD, complicating attempts to isolate occlusion as a primary etiological factor. 13 Stress can also serve as a confounder, mimicking or exacerbating TMJ-related symptoms in affected individuals. 14
Given the rising awareness of TMD among the general population and advancements in diagnostic approaches within dentistry, early identification of risk modifiers, especially in younger populations, is critical. This study focused on university students aged 18-28 years, a group undergoing significant biological and behavioral transitions, making them susceptible to developing TMD-related symptoms.
Thus, the current study aimed to assess the prevalence of TMD among young adults using the DC/TMD Axis I criteria and to examine its association with functional and static occlusal parameters. This research aims to provide region-specific insights into the relationship between occlusion and TMD, with the broader objective of enhancing awareness and supporting early identification efforts in clinical practice.
Materials and Methods
Study Design and Setting
This cross-sectional study was conducted at the Department of Orthodontics and Dentofacial Orthopaedics over a period of 1 year and 6 months. The study aimed to assess the prevalence of TMD among young adults and to examine the relationship between selected functional and static occlusal parameters in participants with signs and symptoms of TMD and non-TMD participants.
Participants
A total of 200 university students aged 18-28 years were selected using simple random sampling. Inclusion criteria were the presence of a full complement of permanent teeth (excluding third molars), the absence of intraoral causes of pain, and willingness to participate. Exclusion criteria included a history of systemic illness, trauma to the TMJ, the presence of psychiatric or neurological conditions, the presence of restorations, missing teeth, prostheses, or current undergoing fixed orthodontic treatment.
Sample Size Calculation
The required sample size was calculated using G*Power software (Version 3.1), assuming a 25% prevalence rate, with 5% margin of error, 95% confidence level, and 95% power. A minimum sample size of 197 was required, rounded off to 200 participants for convenience.
Screening and Grouping
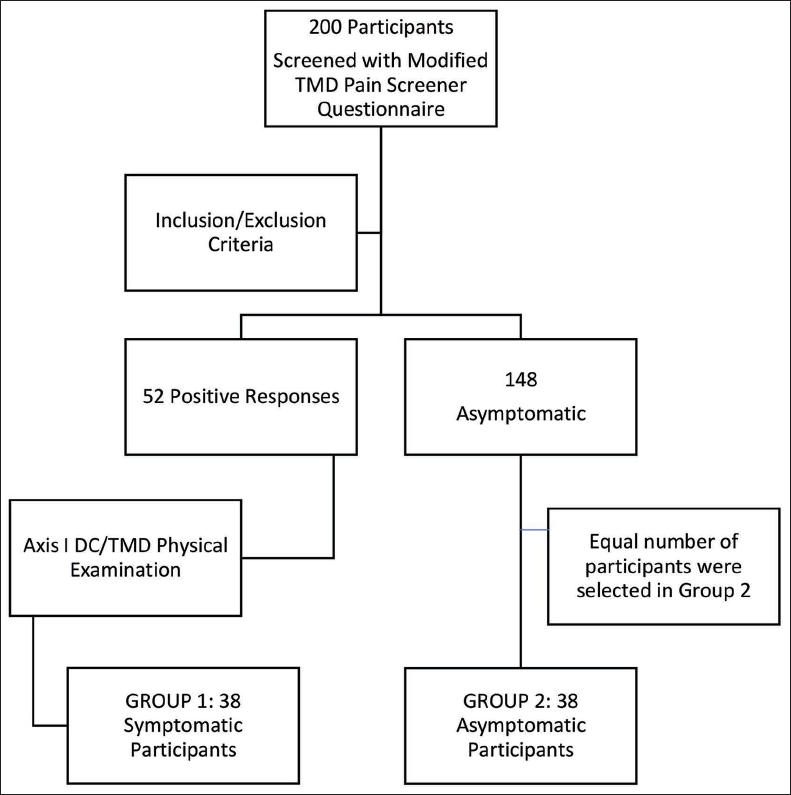
Participants were initially screened using a modified version of the TMD Pain Screener, adapted from the DC/TMD Axis I assessment. 1 While the original Pain Screener assesses pain experienced within the past 30 days, our version was extended to capture pain occurring over the previous 6 months. Based on their responses, 52 individuals were identified as positive for TMD-related pain. These participants then underwent a detailed clinical examination following the DC/TMD Axis I protocol, 1 which involved assessing pain during mandibular movements and palpating the TMJ and masticatory muscles to confirm the location and nature of the pain. Out of these, 38 participants were diagnosed with signs and symptoms of TMD. An equal number of asymptomatic participants (n = 38) were randomly selected to form the comparison group.
Group 1: Symptomatic participants (n = 38).
Group 2: Asymptomatic participants (n = 38).
The step-by-step procedure for participant selection and diagnosis is summarized in Flowchart 1.
Steps to Identify Participants with Temporomandibular Disorders (TMD) and Non-TMD.
Occlusal Parameter Evaluation
Functional Parameters
CR-MIP discrepancy: Discrepancy between jaw positioning in CR and MIP was observed using a Lucia jig (Figure 1) 10 for muscle relaxation. The Lucia jig was fabricated from thermoplastic beads. After approximately 5 min of use, this device eliminates the reflex arc responsible for the acquired mandible closure trajectory in MIP, determined by memory traces and the teeth. Subsequently, mandible manipulation (frontal technique) was used to identify the CR position until the first contact between opposing teeth (premature contact) occurs. At this time, the teeth in contact were marked with a pencil, registering the CR position. The maxillary tooth was used as a fixed reference point; subsequently, the subject was instructed to open and close the mouth in MIP. Thus, the mark present in the mandibular tooth enabled other demarcations in the maxillary arch in this new position. The distances between the maxillary markers were measured and reported as the discrepancy between CR and MIP in the anterior-posterior direction (Figure 2).
Lucia Jig.

Marking Shows that the Centric Relation-Maximum Intercuspation (CR-MIP) is Coinciding.

Excursive movements: Left and right lateral and protrusive excursions were recorded by measuring the change in position of the mandibular reference tooth relative to the maxillary counterpart (Figure 3).
(a) Left Lateral Excursive Movement. (b) Right Lateral Excursive Movement. (c) Protrusive Movement.

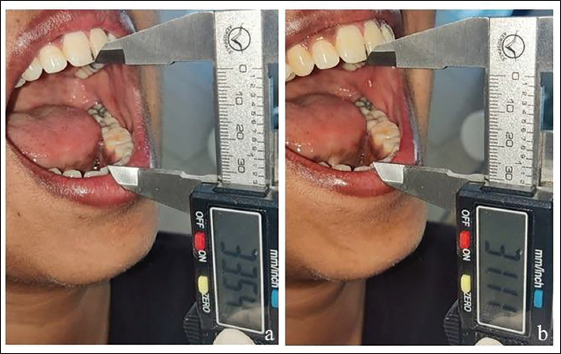
Maximum mouth opening: Both unassisted and assisted maximum mouth openings were measured using a digital caliper placed between incisal edges (Figure 4).
(a) Assisted Mouth Opening. (b) Unassisted Mouth Opening.
Static Parameters
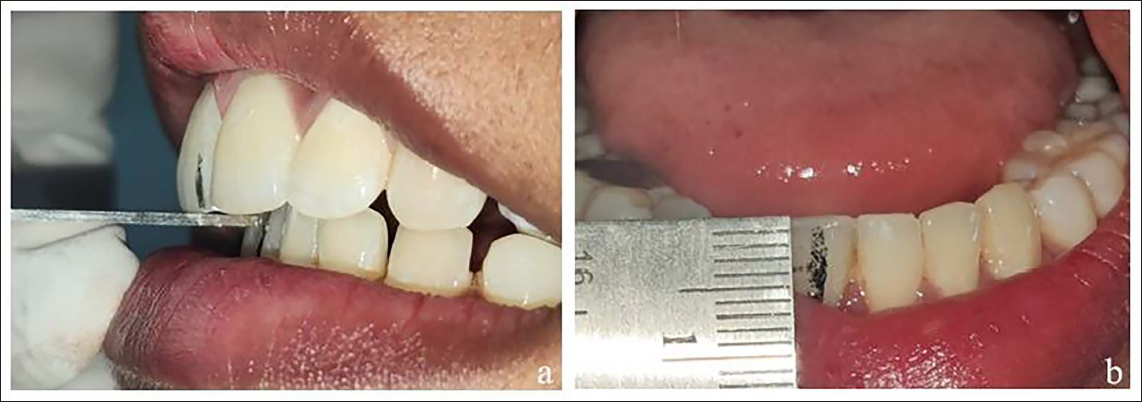
Overjet and overbite: Recorded in the MIP position (Figure 5).
(a) Overjet. (b) Overbite.
Midline deviation: Measured by noting the discrepancy between upper and lower dental midlines.
Molar relationship: Classified using Angle’s classification system. 15
Crossbite/open bite: Anterior and posterior crossbites, as well as open bites, were recorded as present or absent.
Data Analysis
All data were compiled and statistically analyzed using Statistical Package for the Social Sciences (SPSS) Version 25. Descriptive statistics were used to summarize findings, and one-way analysis of variance (ANOVA) was applied to assess group differences. A P value < .05 was considered statistically significant.
Results
Diagnostic Parameters
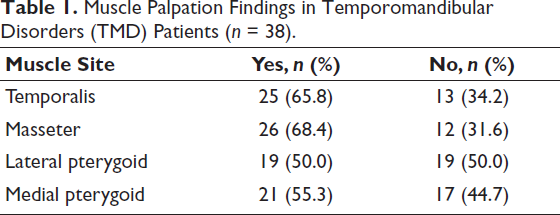
Muscle Palpation Findings (Table 1)
Palpation of the masticatory muscles revealed that the masseter (68.4%) and temporalis (65.8%) were the most frequently involved sites in TMD patients, indicating predominant myofascial involvement. Both the medial and lateral pterygoid muscles showed moderate involvement (55.3% and 50.0%, respectively), suggesting that deeper muscle groups are also commonly affected, although to a lesser extent than the superficial masseter and temporalis.
Muscle Palpation Findings in Temporomandibular Disorders (TMD) Patients (n = 38).
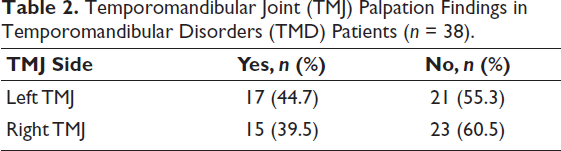
TMJ Palpation Findings (Table 2)
Examination of the TMJ revealed tenderness in 44.7% of the left joints and 39.5% of the right joints among TMD patients. Although the majority of joints were asymptomatic, the slightly higher prevalence on the left side may reflect unilateral functional stresses or asymmetrical loading patterns in these individuals.
Temporomandibular Joint (TMJ) Palpation Findings in Temporomandibular Disorders (TMD) Patients (n = 38).
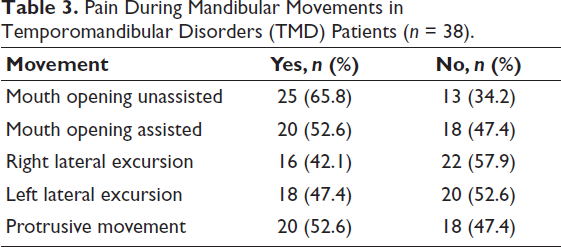
Pain During Mandibular Movements (Table 3)
Assessment of pain during mandibular movements showed that unassisted mouth opening was the most painful activity, with 65.8% of TMD patients reporting discomfort. Assisted opening and protrusive movements each produced pain in 52.6% of patients, while lateral excursions were less painful (47.4% on the left side, 42.1% on the right side). These findings underscore that both mouth opening and protrusive functions are significantly compromised in TMD.
Pain During Mandibular Movements in Temporomandibular Disorders (TMD) Patients (n = 38).
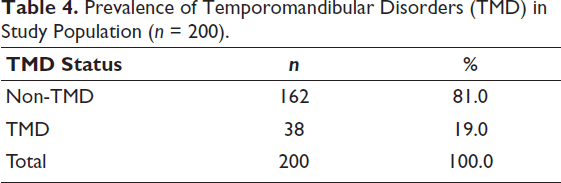
Prevalence of TMD
Among 200 young adult participants, 38 (19.0%) were diagnosed with TMD, leaving 162 (81.0%) participants as asymptomatic (Table 4). This prevalence aligns with published ranges for similar populations.16–18
Prevalence of Temporomandibular Disorders (TMD) in Study Population (n = 200).
Association of Occlusal Parameters in TMD and Non-TMD Groups
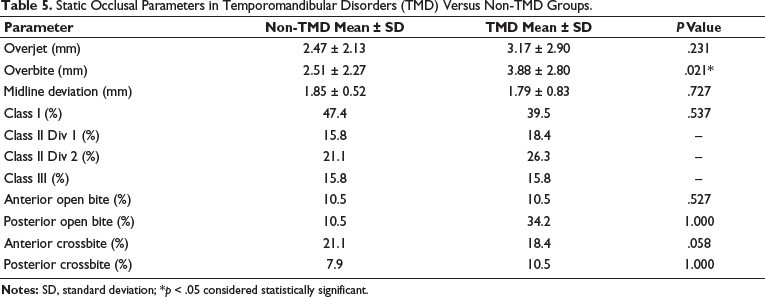
Association of Static Occlusal Parameters in TMD and Non-TMD Groups (Table 5)
Static occlusal characteristics were compared between TMD and non-TMD groups across multiple parameters. Overbite was the only parameter that showed a statistically significant difference, with a deeper mean overbite observed in the TMD group (3.88 ± 2.80 mm) compared to the non-TMD group (2.51 ± 2.27 mm; P = .021), suggesting a possible association with TMD. Overjet was slightly higher in the TMD group (3.17 ± 2.90 mm) than in the non-TMD group (2.47 ± 2.13 mm), but this difference was not statistically significant (P = .231). Midline deviation also did not differ significantly between the two groups (1.79 ± 0.83 mm in TMD vs. 1.85 ± 0.51 mm in non-TMD; P = .727). Analysis of molar relationships revealed no significant differences in the distribution of Class I, Class II Division 1 and 2, or Class III relationships between TMD and non-TMD groups (P = .537), with Class I being slightly more prevalent in the non-TMD group (47.4%) compared to the TMD group (39.5%). Anterior open bite was equally prevalent in both groups (10.5%), showing no significant association (P = .527). Posterior open bite was more frequent in the TMD group (34.2%) than in the non-TMD group (10.5%), though this difference was not statistically significant (P = 1.000). Similarly, anterior crossbite was present in 18.4% of TMD and 21.1% of non-TMD participants, with the difference approaching but not reaching significance (P = .058). Posterior crossbite was found in 10.5% of the TMD group and 7.9% of the non-TMD group (P = 1.000), indicating no meaningful association. Overall, except for the significantly increased overbite in TMD patients, all other static occlusal parameters, including overjet, midline deviation, molar classification, and the presence of open bites and crossbites, showed no statistically significant differences between groups, underscoring the limited diagnostic utility of static occlusion alone in identifying TMD.
Static Occlusal Parameters in Temporomandibular Disorders (TMD) Versus Non-TMD Groups.
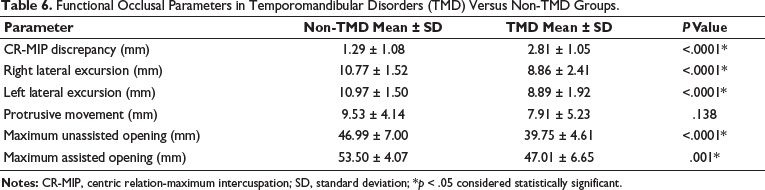
Association of Functional Occlusal Parameters in TMD and Non-TMD Groups (Table 6)
Functional occlusal assessments revealed significant differences between TMD and non-TMD groups, underscoring a strong association between dynamic mandibular function and the presence of TMD. The mean discrepancy between CR and MIP position was substantially greater in the TMD group (2.81 ± 1.05 mm) compared to the non-TMD group (1.29 ± 1.08 mm), with this difference being highly statistically significant (P < .0001). Right lateral excursive movements were notably reduced in TMD patients (8.86 ± 2.41 mm) relative to non-TMD individuals (10.77 ± 1.52 mm; P < .0001), as were left lateral excursions (8.89 ± 1.92 mm in TMD vs. 10.97 ± 1.50 mm in non-TMD; P < .0001), indicating restricted lateral mobility. Similarly, maximum unassisted mouth opening was significantly lower in the TMD group (39.75 ± 4.61 mm) compared to the non-TMD group (46.99 ± 7.00 mm; P < .0001), as was assisted mouth opening (47.01 ± 6.65 mm in TMD vs. 53.50 ± 4.07 mm in non-TMD; P = .001), suggesting a consistent limitation in jaw opening among TMD patients. In contrast, protrusive movement showed no statistically significant difference between the groups (7.91 ± 5.23 mm in TMD vs. 9.53 ± 4.14 mm in non-TMD; P = .138). Collectively, these findings highlight that functional deviations, particularly in jaw positioning, excursive movements, and mouth opening, are more closely associated with TMD symptomatology than static occlusal parameters.
Functional Occlusal Parameters in Temporomandibular Disorders (TMD) Versus Non-TMD Groups.
Discussion
TMD are among the most prevalent musculoskeletal conditions involving the craniofacial region, with multifactorial origins that continue to generate scholarly debate. In this study, a TMD prevalence of 19% was observed, aligning with earlier epidemiological data suggesting rates between 15% and 25% among young adults.19, 20 The findings resonate with more recent reviews, including those by Valesan et al. 20 and De Oliveira et al., 21 which confirm similar prevalence trends globally while noting variability based on DC and population demographics.
Clinical findings such as masseter and temporalis tenderness, joint sounds, and reduced mandibular movement were prevalent in TMD subjects, corroborating earlier work by Okeson, 9 Michelotti et al., 8 and Manfredini et al. 4 Functional parameters, particularly mouth opening (both assisted and unassisted) and reduced lateral excursive movements, have proved to be statistically significant, highlighting their potential clinical value in the diagnosis of TMD. Limited movement has been attributed to myofascial contracture, capsular tightness, or even anterior disc displacement without reduction.22, 23
Notably, CR-MIP discrepancies were more frequent among TMD patients. This finding supports Cordray’s findings, 24 which linked condylar displacement with increased neuromuscular strain, and Manfredini et al.’s pain-adaptation model. 25 In contrast, protrusive movements did not vary significantly between TMD and non-TMD subjects, which was a similar result observed by Farella et al., 26 likely due to the limited joint loading involved in protrusion.
Static occlusal parameters, though less frequently implicated, showed some notable associations. Deep overbite was significantly correlated with TMD in this cohort, and previous literature suggested that this may be due to posteriorly directed condylar forces and altered incisal guidance. 27 However, overjet and midline deviation did not exhibit statistically significant associations, in line with Pullinger and Seligman 12 and Gidarakou et al., 28 who have long advocated that the adaptive capacity of the masticatory system mitigates the impact of minor occlusal deviations. Similarly, molar classification based on Angle’s criteria, long viewed with skepticism, did not appear predictive of TMD, reflecting the positions of Mohlin et al. 29 and Türp and Schindler, 30 who dismissed simplistic associations between molar class and temporomandibular pathology.
Certain occlusal characteristics continue to draw clinical interest due to their potential role in TMD. Although a posterior crossbite did not achieve statistical significance in our findings, previous studies have linked it to TMD development. Both posterior crossbite and edge-to-edge bite, which were more prevalent in the TMD group, have been associated with asymmetric mandibular loading and insufficient anterior guidance in earlier research.31–33 The study also revealed a higher prevalence of excessive overjet and overbite (>5 mm) among TMD patients, conditions previously linked to occlusal instability and muscle hyperactivity.34, 35 The role of balancing-side interferences, found in 78% of TMD patients, is further corroborated by D’Attilio et al., 36 who documented altered muscle recruitment patterns in their presence.
However, an overwhelming body of evidence challenges the deterministic view of occlusion as a primary etiological factor in TMD. A series of systematic reviews and expert consensus reports by Manfredini et al., 4 de Leeuw and Klasser, 3 and Slade et al.⁵ argued for a biopsychosocial model wherein occlusion is merely one of many risk modifiers. In fact, many individuals with pronounced occlusal discrepancies remain asymptomatic, pointing to neuromuscular adaptation, cortical plasticity, and individual pain thresholds as protective factors. The current data also reflected this complexity, as several control subjects exhibited crossbites or midline deviations without any TMD signs. Bruxism, present in 68% of TMD subjects, likely plead a more central role in the development of muscular TMD, aligning with the updated international consensus on bruxism classification. 14
The association between orthodontic parameters and TMD has long been a subject of scholarly inquiry, with contemporary evidence suggesting that occlusal factors may act as contributing or perpetuating elements rather than primary etiological agents by Manfredini et al. 37 and Gesch et al. 38 Although occlusal discrepancies alone are not sufficient to cause TMD, they may interact with biopsychosocial variables to influence disease onset, severity, or chronicity, as per reports by Schiffman et al. 1 and Slade et al. 39 This study holds important clinical relevance by focusing on occlusal parameters as potential risk indicators for TMD, thereby aiding clinicians in developing more targeted and individualized diagnostic and therapeutic strategies.
To the best of the authors’ knowledge, no prior epidemiological or clinical research has examined the association between TMD prevalence and occlusal traits in the studied population. A limited number of studies from the region have addressed general TMD prevalence, like Kanjani et al. 40 and Soni et al., 41 or radiographic condylar positions in relation to Angle’s classification by Joshi et al., 42 but none have systematically explored the association of occlusal parameters in TMD and non-TMD groups. Considering the region’s distinct demographic and environmental factors, this study fills a critical gap in the regional literature and provides contextually relevant data that may inform preventive and early intervention strategies in clinical practice.
Furthermore, the findings underscore the necessity of incorporating comprehensive occlusal and functional assessments into routine dental evaluations. As highlighted by Proffit et al., 43 individualized treatment planning remains crucial, and decisions should not be driven solely by presumed TMD prophylaxis. Such integration may facilitate the early identification of at-risk individuals and support the implementation of conservative management strategies, thereby reducing the long-term burden of TMD on both patients and the healthcare system. 9
Limitations
Cross-sectional design of the study prevents establishing causality between occlusal factors and TMD, for which longitudinal research is needed. The sample, limited to university students aged 18-28 years from one region, restricts generalizability. While DC/TMD Axis I criteria were used, psychosocial factors from Axis II were not assessed, potentially missing important contributors. Subjective factors like bruxism and stress were not quantified. Finally, clinical occlusal assessments may be biased due to a lack of examiner reliability checks or blinding.
Conclusion
This study confirms a 19% prevalence of TMD among young adults and highlights the clinical significance of functional occlusal parameters. CR-MIP discrepancies, excursive interferences, and excessive overbite were significantly more prevalent in the TMD group. Static parameters such as Angle’s molar classification, overjet, and midline were not associated with TMD, but a higher frequency of multiple occlusal discrepancies in affected individuals suggested a potential cumulative burden on the masticatory system. These findings support the multifactorial nature of TMD, where occlusion may function as a contributing rather than a causal factor, emphasizing the need for comprehensive, individualized clinical assessment. Further interdisciplinary and longitudinal research is recommended to clarify these associations and inform evidence-based orthodontic and rehabilitative approaches.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was obtained from the Institutional Ethics Committee of the University (Ref: IEC/P-244/2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was collected from all participants.