
Abstract
Objective
To estimate the change in intraoral volume following orthodontic extraction correction in bidentoalveolar protrusion cases and to establish whether there is a significant change in intraoral volume associated with the above treatment.
Materials and Methods
This study was conducted on 15 patients with bidentoalveolar protrusion. Data were collected using cone beam computed tomography before and after orthodontic extraction correction. Pretreatment and post-treatment intraoral volume were determined for each patient from multiplanar reconstructions using Planmeca Romexis viewer software.
Results
The mean pretreatment and post-treatment intraoral volume was 43.055 ± 2.55205 cm3 and 38.4958 ± 2.42266 cm3, respectively. The mean change in intraoral volume was 4.5592 ± 0.72272 cm3.
Conclusion
There was a significant reduction in intraoral volume after orthodontic retraction in bidentoalveolar protrusion cases.
Introduction
Bimaxillary protrusion is one of the most prevalent dentofacial deformities in the Asian population. It is a common dentofacial deformity that leads to unacceptable facial aesthetics. It is characterized by proclined and protrusive upper and lower incisors, procumbent lips, lip incompetence, convex profile, and hyperactive mentalis. 1 The etiology is multifactorial and consists of a genetic component as well as environmental factors, such as mouth breathing, tongue and lip habits, and tongue volume (TV). 2
Orthodontic treatment alone or combined with orthognathic surgery are the treatments of choice. Orthodontic treatment often involves extraction of the four first premolars with subsequent retraction of the incisors. Orthodontic as well as surgical retraction of anterior teeth for the correction of bidentoalveolar protrusion would produce a change in intraoral volume. It is hoped that the intraoral structures will adapt to this volume change during the active phase of treatment or at least later in the retention phase.
Oral cavity dimensions, and particularly the dimensions of the dental arches, are subjected to environmental as well as genetic influences. The extent to which tongue and lip pressures influence tooth position remains controversial. The recent research and clinical findings have led to a resurrected interest in form–function relationship emphasizing the importance of function in deciding the form. An electronic search pertaining to the topic showed that no study has been reported on the intraoral volume change following orthodontic retraction of anterior teeth in bidentoalveolar protrusion cases.
The Aims and the Objectives of the Study
To estimate intraoral volume before and after orthodontic retraction following extraction of four premolar teeth in patients with bidentoalveolar protrusion using cone beam computed tomography (CBCT).
To establish whether there is a significant change in intraoral volume associated with the above treatment.
Materials and Methods
A new method of measuring intraoral volume from CBCT has been devised, and its accuracy was found to be satisfactory based on intraobserver and interobserver reliability. CBCT was performed using Planmeca Promax 3D Plus with exposure parameters: 90 kVp, 8 mA, scan time (0.04 s), and field of view (80 × 80 mm).
Inclusion Criteria
Age: 18-25 years.
Bidentoalveolar protrusion cases requiring extraction of four premolar teeth and treated with MBT appliance.
Normal body mass index (18.5-24.5).
Exclusion Criteria
Crowding of teeth greater than 3 mm.
Congenitally missing teeth other than third molar.
Patient with abnormal tongue size.
Patient with history of trauma-induced fracture of jaw bones.
Patient with anteroposterior jaw discrepancies.
Patient with history of chronic mouth breathing.
Craniofacial abnormality including cleft lip.
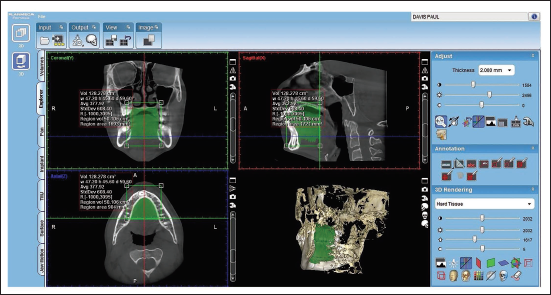
Volume was assessed from the coronal sections of the image obtained with the help of free-region volume tool in the software. An individual slice of 2 mm thickness was selected.
For volume assessment, the boundaries of the oral cavity were marked as follows.
The contour of the palatal vault was taken as the superior border (roof of the mouth). The palatal and lingual aspect of maxillary and mandibular teeth was taken as the anterior and lateral borders. Distal aspect of upper and lower second molars was taken as the posterior border of the oral cavity. The floor of the mouth was taken as the inferior border.
The genial tubercles on the lingual surface of mandibular symphysis give origin to the genioglossus muscle and hence can be considered the boundary for the floor of the mouth anteriorly. Similarly, the mylohyoid ridges, which give origin to the mylohyoid muscles bilaterally, can be considered the boundary for the floor of the mouth laterally. The mylohyoid ridges do not reach the genial tubercles anteriorly. Therefore, identifying a boundary for the floor of the mouth between the anterior end of the mylohyoid line and the genial tubercle needs some improvisation. The method used for this is as follows.
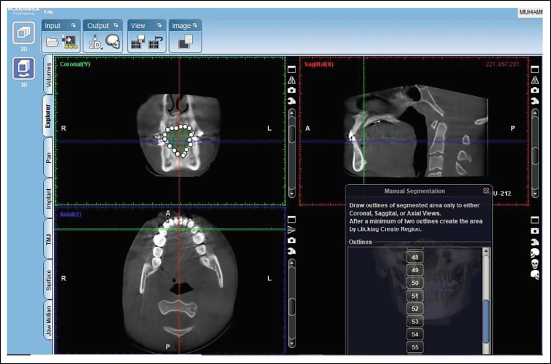
Outlines were traced manually in each section in each slice. The number of coronal sections (2 mm slice) between the genial tubercle and the anterior end of the mylohyoid line was estimated. Half the number of coronal sections was considered belonging to the genial segment, and half the number of coronal sections was considered belonging to the mylohyoid segment.
After reconstructing the 3D image, the volume was determined in individual sections by Planmeca Romexis viewer software, which was added upon to create the final regional volume. Each volume measurement was done by the same observer on three separate days, and the mean value was taken as the final volume.
Intraobserver and interobserver variability of making these above measurements was estimated, and inter-rater reliability was checked using SPSS version 16 software. Since the single measure intraclass correlation was 0.658, it shows that there was a substantial agreement between two observers, and the estimate was significant.
Methods of Data Collection
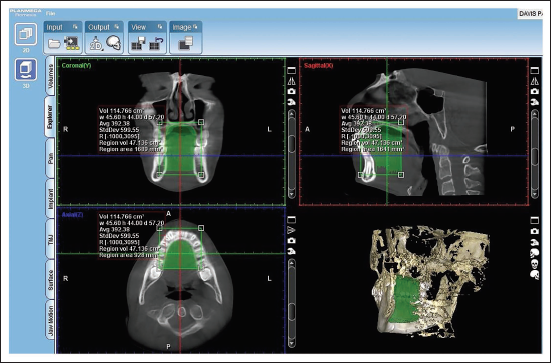
This study was conducted on 15 patients with bidentoalveolar protrusion. Data were collected using CBCT before (Figure 1) and after (Figure 2) orthodontic treatment, and intraoral volume assessment was carried out using Planmeca Romexis viewer software (Figures 3 and 4).
Pretreatment Intraoral Volume Assessment of a Patient.
Post-treatment Intraoral Volume Assessment of a Patient.
Romexis Viewer.

Segmentation of the Oral Cavity using the Reference Points.
Statistical Analysis
The data obtained by making these measurements were statistically analyzed using SPSS V.16 software (SPSS Inc., Chicago, Illinois, USA). The descriptive statistics for the mean difference and standard deviations were calculated. Student paired t-test was used to compare the pretreatment and post-treatment volume of the same patient. The level of significance was set at 0.05, at a 95% confidence interval. After the analysis, the data were sorted into various tables based on the objectives of the study.
Results
Fifteen patients who fit into the inclusion criteria were chosen for this study. Pretreatment and post-treatment intraoral volume was measured using CBCT for all the patients. The change in intraoral volume was estimated. Paired Student t-test was used to compare the pretreatment and post-treatment intraoral volume. The results of the study were tabulated and analyzed as discussed below:
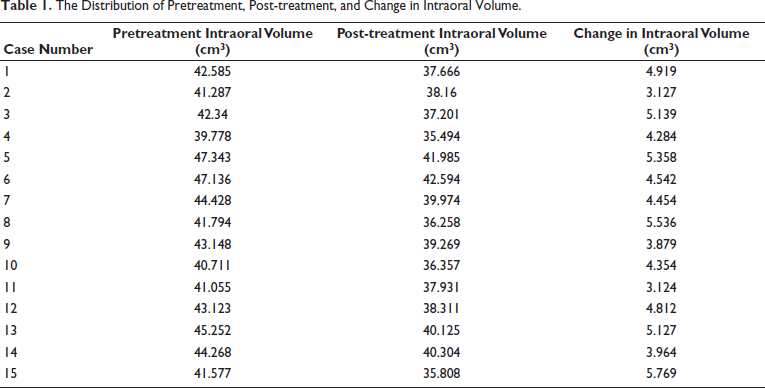
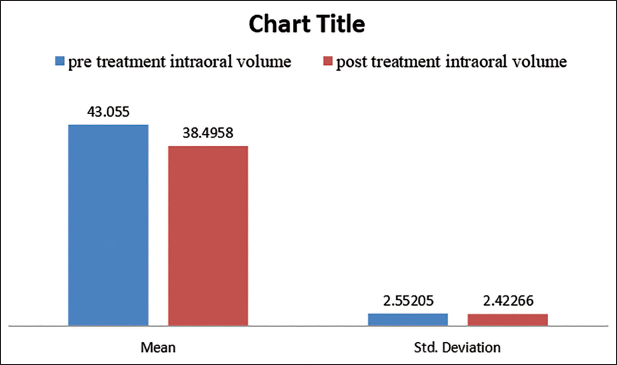
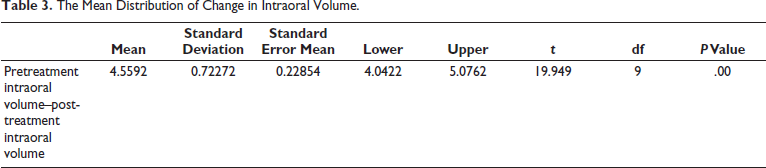
The distribution of pretreatment, post-treatment, and change in intraoral volume is given in Table 1. The mean distribution of pretreatment and post-treatment intraoral volume is shown in Table 2 and Figure 5. The mean pretreatment intraoral volume was 43.055 ± 2.55205 cm3 (Table 2). The mean post-treatment intraoral volume was 38.4958 ± 2.42266 cm3 (Table 2). The average change in intraoral volume was 4.5592 ± 0.72272 cm3 (Table 3). The results have shown that there was a statistically significant reduction in intraoral volume after orthodontic extraction correction (p value = .00).
The Distribution of Pretreatment, Post-treatment, and Change in Intraoral Volume.
The Mean Distribution of Pretreatment and Post-treatment Intraoral Volume.

Mean Pretreatment and Post-treatment Intraoral Volume.
The Mean Distribution of Change in Intraoral Volume.
Discussion
In bimaxillary dentoalveolar protrusion, incisors may appear well-aligned, but this is at the expense of lip protrusion. Incisor crowding and protrusion share a common etiology, which is tooth material arch length discrepancy. It can also adversely affect the harmonious lip function. 3 Retraction of the anterior teeth or expansion of the dental arches may result in volumetric changes in the oral cavity. Changes in oral cavity morphology can be seen in patients with facial deformities and constricted dental arch forms. 4 If there is a change in the oral environment, tongue position, or function, or both, will adapt to the size of the mandibular arch containing it.
Ding et al. 5 in 2018 evaluated TV and oral cavity capacity (OCC) using CBCT. They have calculated the OCC as OCC = TV + OCPV and the TV/OCC ratio. The mean TV was 47.07 ± 7.08 cm3. The mean oral cavity proper volume (OCPV) and OCC were 4.40 ± 2.78 cm3 and 51.47 ± 6.46 cm3, respectively. There was a significant correlation between TV and OCC.
In our study, the mean pretreatment intraoral volume was 43.055 ± 2.55205 cm3, which is less than the OCC (51.47 ± 6.46 cm3) measured by Ding et al. In their study, they considered patients with a mean age of 30.1 ± 2.3 years, which is more than our study group’s age, which is between 18 years and 25 years. The population taken by both studies are also different. They studied TV and oral cavity proper volume separately, but our study focused on intraoral volume, which includes the TV also. In their study, the mean TV was 47.07 ± 7.08 cm3, which is larger than the TV reported by Uysal et al. 6 (31.02 ± 9.75 cm3 for men and 28.13 ± 8.54 cm3 for women). Humbert et al. 7 reported a TV of 63.3 ± 8.2 cm3 measured on magnetic resonance imaging (MRI), which was larger than this study. Iida-Kondo et al. 8 reported a TV/OCC ratio of 86.98%, which is similar to this study.
Teramoto et al. 4 in 2020 evaluated the morphological and volumetric changes of the tongue and oral cavity before and after orthognathic surgery for patients with mandibular prognathism. This study concluded that the patients with mandibular prognathism showed a decrease in both OCC and TV following orthognathic surgery (BSSO setback), and the TV/OCC ratio remained unchanged before and after surgery.
Our study showed a reduction in intraoral volume of 4.5592 ± 0.72272 cm3 after orthodontic retraction, which was less compared to the results of the study of Teramoto et al. 4 after BSSO setback, which is about 6.44 ± 0.71 cm3. The smaller reduction in intraoral volume in our study could be because of anchorage loss or due to the selection of different landmarks for the inferior border. But in the previous study, they have taken all limits relative to occlusal plane, while in our study, we evaluated total space according to the contour of palatal vault and lower border as the floor of the mouth without considering the occlusal reference plane.
Rajkumar et al. 9 in 2021 published an article on “Evaluation of volume change in oral cavity proper before and after mandibular advancement.” In this study, they have taken a posterior border that extends to the oropharynx. Our study is limited to considering intraoral volume up to the distal aspect of the second molar. They have considered inferior border at the level of lingual frenulum, with the palatal plane as reference, which is different from our study.
They used the term “oral cavity volume,” which is a combination of oral cavity proper volume and TV. Oral cavity volume before and after BSSO advancement was 37.3 ± 7.7 cm3 and 49.8 ± 9.7 cm3, respectively, with an increase in oral cavity volume of 12.7 ± 5.1 cm3, which is more than the reduction in intraoral volume after BSSO setback, which is 6.44 ± 0.71 cm3 in a study by Teramoto et al. 4
In our study, we have taken the plane connecting the genial tubercle and mylohyoid muscle as the lower border. Lauder et al. 10 in 1991 reported difficulty in defining the inferior and lateral borders of the tongue on MRI. Loubele et al. 11 in 2007 also established that it is difficult to identify soft tissue borders on CBCT images because of the lack of contrast between the various soft tissue structures.
Various studies and clinical observations have conclusively proven the association between form and function. In our study, there is a significant reduction in intraoral volume after orthodontic retraction. If orthodontic treatment results in a significant reduction in intraoral volume and satisfactory adaptation fails to occur, the increased resting pressure from tongue could lead to orthodontic relapse.
Various studies have evaluated TV using CT, CBCT, MRI, and ultrasound.1–4, 12–16 Two studies evaluated OCC.4, 5 Two studies evaluated oral cavity proper volume.9, 17 In these four above-mentioned studies, they calculated TV separately. But our study estimated intraoral volume, which includes the TV, which is not evaluated separately.
Teramoto et al. 4 reported that there is a significant reduction in TV and OCC after BSSO setback. Rajkumar et al. 9 found that there is a significant increase in TV and OCPV after BSSO advancement. Our study concluded a significant reduction in intraoral volume following orthodontic retraction, which is less than that of surgical retraction (BSSO setback).
It is also possible that more relevant observations would have emerged from this study if the sample size was higher. The number of subjects in our study was limited and, therefore, future studies with more number of subjects are warranted.
Conclusion
The intraoral volume was estimated before and after orthodontic treatment with extraction for the correction of bidentoalveolar protrusion using CBCT images in 15 patients, and we evaluated the change in intraoral volume. From the results obtained from our study population, the following conclusions were drawn:
The results concluded that there was a significant reduction in intraoral volume after orthodontic retraction with extraction of all first premolars in bidentoalveolar protrusion cases. If orthodontic treatment results in a significant reduction in intraoral volume and if satisfactory adaptation fails to occur, the increased resting pressure from the tongue could lead to orthodontic relapse.
Limitatons of the Study
A more detailed study with a greater number of cases is required to assess the reduction in intraoral volume and TV following orthodontic retraction in bimaxillary dentoalveolar protrusion cases. It is also pertinent to evaluate the long-term effects of this reduction in intraoral volume on morphological adaptations in tongue posture and volume.
Footnotes
Acknowledgments
We acknowledge the support received from the Department of Oral Medicine and Radiology throughout this study in data acquisition and three-dimensional analysis.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was undertaken after the ethical clearance from the institutional ethics committee of the Postgraduate Institute of Medical Education and Research. The study protocol was approved by the Institutional Ethical Committee.
Informed Consent
All participants fulfilling the inclusion and exclusion criteria were informed about the study being conducted, and informed consent was obtained from all the participants before the commencement of the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.