
Abstract
Objectives
The study aimed to assess and compare the clinical outcomes of low-level laser therapy (LLLT) and subgingival ozone irrigation on gingival inflammation in patients undergoing fixed appliance therapy and to relate the clinical outcomes with lactate dehydrogenase (LDH) activity in gingival crevicular fluid (GCF).
Materials and Methods
15–25 year-old 30 healthy patients undergoing orthodontic treatment were selected in this prospective, cross-sectional study. In each subject, the upper right and left quadrants of the mouth were randomly designated as the control side and the interventional side, respectively. Clinical parameters (gingival index, plaque index, gingival bleeding index) and LDH enzyme activity were recorded at baseline (0th day) on both sides. The interventional side was irradiated with a soft tissue 980 nm diode laser (Zolar Photon Plus) with a power density of 100 mW cm–2 and an energy density of 18 J cm–2, and the control side was irrigated subgingivally with 0.01 mg/l ozonated water using the Kent Ozone Dental Jet TY-820. All the clinical parameters, except LDH, were reassessed on the 7th, 14th and 28th day, whereas LDH levels in GCF were reevaluated on the 28th day.
Results
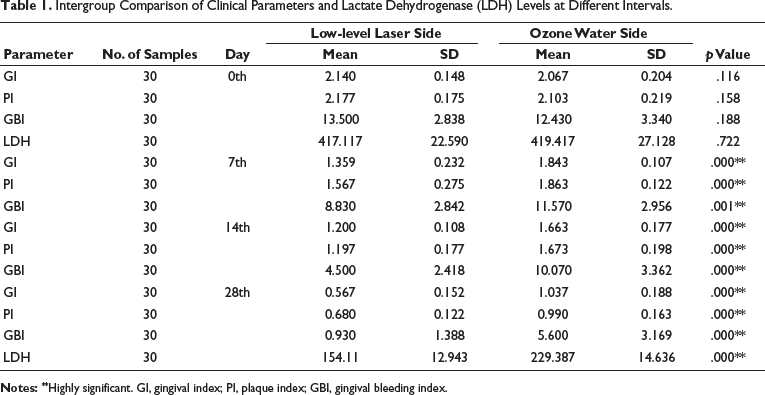
Both groups showed a significant reduction (p < .05) in gingival parameters and LDH activity after the study period. A greater decrease of clinical parameters and LDH activity (417.117 mU ± 22.59 to 154.11 mU ± 12.943) was seen on the LLLT side than on the ozone irrigation side (419.417 mU ± 27.128 to 229.387 mU ± 14.636). Also, a significant correlation existed among the clinical parameters assessed and the LDH activity in GCF after the treatment period.
Conclusions
LLLT and ozone irrigation were both effective in controlling gingival inflammation among which LLLT was superior.
Clinical Relevance
Fixed mechanotherapy makes oral hygiene difficult, necessitating the need for adjunctive methods. From this study, it was proved that ozone and laser therapy were effective in controlling gingival inflammation in orthodontic patients, thus enabling their use in the monthly visits.
Keywords
Introduction
Orthodontic treatment is aimed at improving the function and aesthetics of the mouth and the face using appliances, which may be fixed or removable. 1 Fixed orthodontic appliances can complicate brushing, making it harder to remove plaque thoroughly and increasing the risk of gingivitis. 2 Forces applied to these teeth can lead to increased periodontal damage and hinder the regeneration of periodontal ligament tissues. Additionally, the presence of periodontal inflammation makes these tissues more vulnerable to bacterial infection.3, 4
In the early 1900s, to treat periodontal inflammation, sodium bicarbonate was used. 5 In 1913, a decrease in plaque formation was noticed with hydrogen peroxide. 6 Deep pocket irrigation of oral tissues in patients with advanced periodontitis using Viadent oral rinse with a Propulse irrigating device proved to be effective. 7
An alternative approach is by changing the subgingival environment. Previous research has shown that chlorhexidine gluconate mouth rinse will effectively prevent the development of gingivitis during treatment. While chlorhexidine is not toxic, it has a disagreeable taste, affects taste perception and also causes brown staining on the teeth that is challenging to remove. Additionally, chlorhexidine promotes the formation of supragingival calculus, leading to calcified and stained deposits that stubbornly attach to the tooth or restoration surface and are difficult to clean.8, 9
In search of other alternatives to chlorhexidine, Ramzy et al., in their study on aggressive periodontitis, concluded that oral hygiene improved significantly after ozone irrigation. 10 In 2010, Kshitish and Lakshman found that the use of ozonated water led to a significant reduction in gingival inflammation in patients with chronic periodontitis compared to those using chlorhexidine solution. 11 Previous studies conducted by Dhingra and Vandana, 12 Sandra et al., 13 and Nooney et al. 14 had also proven that using subgingival irrigation with ozone water in orthodontic patients efficiently reduced the onset of gingival inflammation.
The laser is a single wavelength (single color) of light traveling through a collimated tube, delivering a concentrated source of energy. 15 Currently, the two most popular types of lasers used in dentistry are the diode and erbium lasers. 16 At the cellular level, light modulates cell biochemical reactions, stimulating mitochondrial activity and resulting in biomodulation of inflammatory processes by reducing prostaglandin E2 (PGE2) release. So, lasers are recommended for reducing gingival inflammation.17, 18 A study by Pejcic et al. demonstrated that low-level laser irradiation (semiconductor, 670 nm) can serve as an effective physical adjunct to traditional periodontal therapy, resulting in improved and more durable therapeutic outcomes.19, 20
Lactate dehydrogenase (LDH) is an enzyme present only in the cytoplasm of cells and is released upon cell death. Research has indicated that LDH activity in gingival crevicular fluid (GCF) rises during orthodontic treatment because of plaque-retentive appliances, with notably higher levels observed at dental sites subjected to compressive stress.13, 14 Hence, LDH in GCF can be used as an effective indicator in evaluating the inflammatory activity during orthodontic treatment.
While ozone irrigation and low-level laser therapy (LLLT) are effective alternatives to chlorhexidine gluconate oral rinse, no studies have yet compared the effectiveness of ozone and LLLT in reducing gingival inflammation.
The aim of this study was to compare the clinical effects of LLLT and subgingival ozone irrigation in managing gingival inflammation in patients undergoing fixed mechanotherapy and to correlate these clinical outcomes with LDH levels in GCF.
Materials and Methods
This single-center, single-blinded prospective study involved individuals receiving fixed mechanotherapy at the Orthodontics Department, CKS Theja Institute of Dental Sciences and Research in Tirupathi, Andhra Pradesh, India. All study procedures received approval from the Institutional Ethical Committee and were conducted in accordance with institutional and/or national research ethics standards, as well as the 1964 Helsinki Declaration and its revisions through 2008, or equivalent ethical guidelines.
Study Sample
The sample size was determined using a two-sample comparison of means test, with a power of 0.90 and a significance level of 0.05. Mean values and standard deviations were derived from a similar study by Cosala et al. 9 To identify a significant difference between the test and control groups, at least 28 patients (14 per group) were required. Consequently, 30 orthodontic patients aged 15-25 years were enrolled in the study and randomly assigned to two treatment groups by the conclusion of the screening process. All patients should have at least 24 teeth, excluding 3rd molars and should be at least 4–8 months into active fixed orthodontic appliance therapy. The selected participants had no systemic conditions and were not taking any medications that could impact overall gingival health. They did not have severe periodontitis and rampant caries or used any removable prostheses or appliances.
Method
The total time period for the study was 28 days. The data were collected at the baseline (0th day), the 7th day, the 14th day and the 28th day. A randomized split-mouth design has been implemented in the maxillary arch, with ozonated water on one side and low-level laser radiation on the other side as control and experimental sides, respectively.
Clinical Procedure
Clinical parameters—plaque index (PI), gingival index (GI) and gingival bleeding index (GBI) were recorded at the baseline, the 7th day, the 14th day and the 28th day. All the parameters were recorded by an experienced periodontist who was blinded to the treatment. The patients were asked to sit comfortably on the dental chair in an upright position, and the examination was carried out after proper illumination. Gingival and periodontal status were examined clinically using a sterile mouth mirror and William’s graduated periodontal probe. On the 0th day and the 28th day, GCF samples were collected using pipettes from both the interventional and control sides, prior to and following the application of LLLT and ozone water irrigation. To avoid the risk of contamination, upper teeth were taken for sampling.
Patient’s Instructions
After the ozone irrigation and LLLT, the patients were informed about routine oral hygiene habits, which include brushing for 2-3 minutes at least 2 times a day with a Colgate Super Flexi medium hard bristled brush using the modified Bass technique and fluoridated toothpaste (1,000 ppm fluoride, Colgate toothpaste) along with regular mouth rinsing after every meal. The patients were reviewed every 7th, 14th, and 28th days for recording the parameters.
Ozone Irrigation
Subgingival irrigation of one maxillary quadrant was carried out using 0.01 mg l–1 ozonated water with a modified needle (22-gauge blunt needle), which is connected to an irrigation device, “Kent Ozone Dental Jet TY-820” (Pure Water House, Bengaluru, India). The machine featured adjustable settings for speed and pressure (ranging from 350 to 500 kPa). It was calibrated to deliver a single pulsating stream of ozonated water through a modified needle, with an ozone output of 0.082 mg/h, a noise level of <70 dB, and a water flow rate of ≥450 ml. Irrigation was performed for 3 minutes per session on the 0th and 7th days.
Laser Irradiation
The other half of the mouth was treated with a laser beam positioned perpendicular to the gingival surface and 2 mm away from it. For anti-inflammatory effects, as recommended by the manufacturer, the laser used a power density of 100 mW/cm2 and an energy density of 18 J/cm2, with a 3-minute exposure per session in continuous mode. The low-level laser was applied on the 0th day and again on the 7th day.
GCF Sampling Procedure
Microcapillary pipettes (1-3 µl), which were calibrated from Sigma Aldrich Chemical Company, USA, were utilized to collect GCF. Patients were made to sit upright, and the supragingival plaque was removed. Care was taken not to touch the marginal gingiva in order to avoid contamination and blockade of the pipette while collecting GCF. A standardized volume of 2 µl unstimulated GCF was collected by placing the tip of the pipette extracrevicularly near the test site. Low volume samples (<2 µl) and samples contaminated with blood and saliva were excluded. All the pipettes collected were refrigerated at –20°C for biochemical analysis.
LDH Activity Determination
All the pipettes were put in a spectrophotometric apparatus (Cyber UV-1, Cyberlab, USA), which implements high-precision/resolution with a high-precision sine driver monochromator and a stable voltage signal process by adopting a noise reduction circuit. To the pipettes for various enzyme activity determination, a reagent of 50 µl (Infinite LDH reagent, ACCUREX, FDA-approved) is added. It is a two-liquid reagent system from which the working solution is prepared in the ratio of 4R1:1R2. LDH enzyme activity was estimated in 2.5 minutes at 37°C, at 340 nm using this apparatus, and the total volume of GCF was expressed in microliter. The LDH activity was calculated as total LDH unit activity (milliunit per sample (mU per sample)) by using the formula: GCF volume (µl) + LDH volume activity (IU l–1) × 10 6 .
Statistical Analysis
The results were subjected to statistical analysis. An independent t-test was employed to compare initial data between the interventional and control sides at various time points. A Pearson correlation test was used to examine the relationship between gingival parameters and LDH activity, while an analysis of variance (ANOVA) test assessed significant differences in gingival parameters across different time intervals. Post-hoc tests were conducted following ANOVA to determine the significance of differences at each time point. A p value of ≤.05 was considered statistically significant for all evaluated parameters.
Results
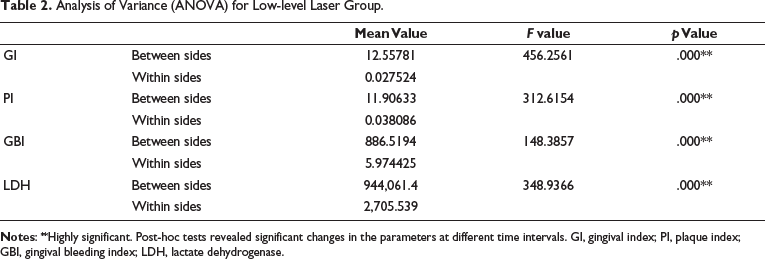
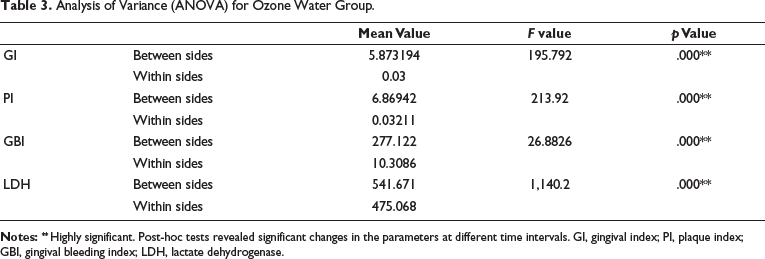
The results for the data collected at the baseline, the 7th day, the 14th day and the 28th day were reported in Tables 1–3. For all the parameters analyzed, a significant difference was observed both with ozone irrigation and LLLT. Also, LDH enzyme activity was significantly reduced in both groups from the 0th day to the 28th day. Post-hoc tests at different time intervals revealed statistical significance for the parameters.
Intergroup Comparison of Clinical Parameters and Lactate Dehydrogenase (LDH) Levels at Different Intervals.
Analysis of Variance (ANOVA) for Low-level Laser Group.
Analysis of Variance (ANOVA) for Ozone Water Group.
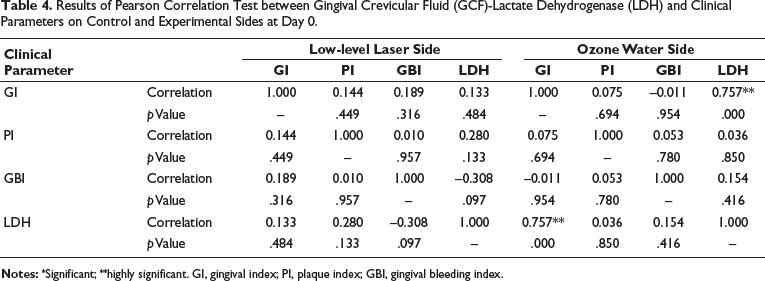
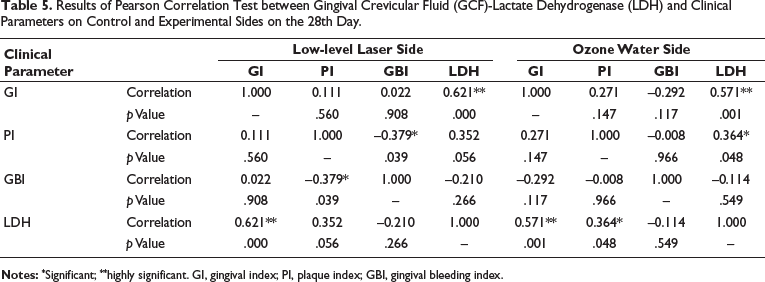
However, LLLT depicted a greater reduction in inflammatory action when compared to ozone irrigation. Tables 4 and 5 show a significant positive correlation between clinical parameters and LDH values among both groups, indicating a significant reduction in the inflammatory activity from the 0th day to the 28th day.
Results of Pearson Correlation Test between Gingival Crevicular Fluid (GCF)-Lactate Dehydrogenase (LDH) and Clinical Parameters on Control and Experimental Sides at Day 0.
Results of Pearson Correlation Test between Gingival Crevicular Fluid (GCF)-Lactate Dehydrogenase (LDH) and Clinical Parameters on Control and Experimental Sides on the 28th Day.
Discussion
The present study was about the effects of LLLT and ozone water irrigation on gingival inflammation. The patients selected for the study were undergoing fixed orthodontic therapy and expressed clinical symptoms of gingival inflammation by evaluating clinical parameters and their correlation with LDH inflammatory marker.
The results proclaimed that the evaluated parameters like GI, PI and GBI were reduced on the application of LLLT and subgingival ozone water irrigation from the 0th day to the 28th day.
Our results were consistent with those of Sandra et al., who assessed the clinical effects of ozone water irrigation on gingival inflammation in orthodontic patients. Their study also found a significant reduction in the evaluated parameters. 13 Similar findings were also reported by Jose et al.’s study, where repeated subgingival ozone water irrigation proved a consistent improvement in gingival condition in patients with fixed orthodontic therapy. 21
When studies were conducted to assess the efficacy of ozone irrigation in chronic periodontitis patients by Ramzy et al., 10 Kshitish and Laxman, 11 and Seydanur Dengizek et al., 22 they observed significant improvement in clinical parameters. Our observations were in accordance with Ren et al.’s study, who found a significant decrease in gingival parameters after LLLT in orthodontic patients. 23 Pejcic et al., Dukic et al., Zare et al., and Qadri et al., in their studies, evaluated the efficacy of conservative treatment with LLLT and found consistent improvement in gingival conditions after LLLT in chronic periodontitis patients.20, 24–26
The present study clearly demonstrates a significant change in the mean concentrations of LDH in GCF from the 0th day to the 28th day. This could be interpreted that the values were higher initially at day “0” when compared to the values obtained at the end of the study period, that is, on day “28.” This change was observed on both the experimental and control sides, but a greater difference was noted on the experimental side, where LLLT was applied, compared to the control side, where subgingival irrigation was performed with 0.01 mg/l ozonated water.
Our findings align with those of Dhingra and Vandana, who observed a significant change in gingival parameters and LDH enzyme activity in GCF following irrigation with ozone water in 15 patients undergoing fixed orthodontic treatment. 12 Identical findings were reported by Nooney et al., who proved a noticeable improvement in gingival condition. The clinical effects were also correlated with the LDH levels in GCF after irrigation with ozone water in orthodontic patients. 14
Similar to the present study, Ren et al. also reported a marked improvement in the gingival parameters after LLLT in patients undergoing orthodontic therapy. Along with a reduction in GCF levels, they also observed a decrease in interleukin-1β (IL-1β), PGE2, and substance P levels. 23
Gingival parameters and the average concentrations of LDH in GCF significantly decreased on the side treated with LLLT compared to the control side, which received ozonated water. The 28-day duration of our study aligns with the monthly orthodontic treatment appointments, suggesting that LLLT could be recommended for managing gingival inflammation in orthodontic patients.
The study lasted for 28 days, which may not be adequate to assess the long-term effects of a single application of LLLT on managing gingival inflammation in patients undergoing orthodontic treatment, which typically spans 18–24 months. Additionally, other factors influencing gingival health in orthodontic patients, such as ligation methods and bracket types, were not addressed in our study.
In the future, specific laser technologies are likely to play a significant role in modern orthodontic practice, potentially serving as adjuncts or alternatives for traditional methods of managing gingival inflammation. Hence, there may be a need for additional prospective clinical trials to assess the effectiveness of LLLT in managing gingival inflammation, considering various factors such as laser frequency and duration.
Conclusions
The present study was aimed at evaluating the effects of LLLT and ozone irrigation on the gingival parameters and LDH enzyme activity in patients undergoing orthodontic therapy. The following conclusions were drawn:
Both methods effectively controlled gingival inflammation, but LLLT had a greater effect in reducing the gingival inflammation when compared to that of subgingival ozone irrigation.
A significant positive correlation existed between gingival parameters and LDH enzyme activity among both groups, indicating a marked decrease in the inflammatory activity from the 0th day to the 28th day.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
All procedures performed in the study were approved by the Institutional Ethical Committee which is in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Reference no. CKS/ORTHO-THES/2012/6.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Prior to inclusion, informed consent was obtained from all individual participants included in the study.