
Abstract
Aim
The aim of the study was to develop new cephalometric angles TWM (T-Tuberculum sella, W-wing point, M-maxillary point) and TWG (T-Tuberculum sella, W-wing point, G point-center of mandibular symphysis) and to assess and evaluate the newly developed angles in determining the maxillary and mandibular sagittal position, respectively.
Materials and Methods
Ninety pretreatment lateral cephalograms from the records of Department of Orthodontics and Dentofacial Orthopaedics were traced and divided equally into three groups as class I, class II, and class III based on cephalometric values of ANB angle and WITS appraisal. Further for each radiograph, angles such as SNA, TWM, SNB, and TWG were measured and recorded. The TWM angle (Maxilla) was formed using the points T-Tuberculum sella, W-wing point, M-maxillary point, and the TWG angle (mandible) was formed using the points T-Tuberculum sella, W-wing point, G point-center of mandibular symphysis.
Results
The mean values of TWM and TWG angles for the class I group were 120.1°± 3.6° and 101.4 ± 3.7°, respectively. The one-way analysis of variance (ANOVA) was used followed by Tukey post hoc testing to determine whether there was a statistically significant difference between the mean values of the three groups. A p value ≤ .05 was considered to be statistically significant. Pearson correlation test revealed a strong correlation between SNA and TWM angles and similarly between SNB and TWG angles.
Conclusion
The two new angles, TWM for maxilla and TWG for mandible established, can be used as an alternative for assessing the sagittal position of the jaw bases and will give a clearer picture, as stable and reproducible landmarks are used.
Introduction
The discovery of cephalometrics in 1931 has proved to be an important clinical tool for the assessment of jaw relationship in all three planes, that is, sagittal, transverse, and vertical. An accurate anteroposterior assessment of jaw relationships is vital in orthodontic diagnosis and treatment planning. There have been numerous angular and linear measurements that have been proposed to assess the sagittal relationship of the maxilla and mandible. Any cephalometric analysis based on either angular or linear measurements has obvious shortcomings, which have been discussed in detail by Moyers et al. 1
McNamara’s main goal in his analysis was to relate the teeth, jaws, and cranial bases to each other. 2 The reference plane used was nasion perpendicular. The most popular parameter for assessing the sagittal position of maxilla and mandible remains the SNA and SNB angles, respectively, introduced by Cecil C. Steiner 3 where Sella–nasion plane was used as the reference plane for angular measurements. However, several authors4–6 have shown that the position of nasion is not fixed during growth (nasion grows by 1 mm per year), and any displacement of nasion will directly affect the SNA and SNB angles. Moreover, it is known that point A is not very clearly visible in many radiographs and the position of point A and point B gets affected with tooth movements and bone remodeling. 7
Arat et al. 8 in their study have stated that the anterior and posterior segments of the cranial base grow at the same rate as the craniofacial skeleton; thus, the development of these segments continues for many years. However, the middle cranial base completes its development earlier, due to its function of protecting the brain and other vital organs. 9 Thus, the stability of the middle cranial base after the age of 8 makes it an excellent baseline for the study. It has long been known that the tuberculum Sella (T) and Wing point (W), located in the middle cranial base, are highly stable.8, 9
Points M (midpoint of premaxilla) and G (midpoint of symphysis) are used to represent the maxilla and mandible respectively and are considered as stable points, as they do not get influenced by tooth movement unlike points A and B.10, 11
Therefore, the purpose of this study was to develop two new cephalometric angles, TWM (T-Tuberculum sella, W-wing point, M-maxillary point) and TWG (T-Tuberculum sella, W-wing point, G point-center of mandibular symphysis) to evaluate maxillary and mandibular sagittal position, respectively.
TWM and TWG Angles
The TWM angle used to assess the sagittal position of maxilla is formed by using the following points (Figure 1):
T Point (Tuberculum Sella):The mean intersection point of the lower contours of the anterior clinoid processes and the contour of the anterior wall of the Sella. W Point (Wing Point):The intersection of the contour of the ala major with the jugum sphenoidale. M Point:Midpoint of premaxilla-center of the largest circle that is tangent to the anterior, posterior, and superior surfaces of the premaxilla.
TWM Angle.
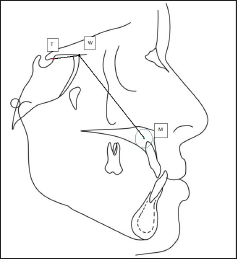
Maxillary point (M), 10 representing the midpoint of the premaxilla in the midsagittal plane, was located on the tracings according to the superior, anterior, and palatal outlines of the premaxilla, and the midpoint was identified with concentric circles to find the largest circle that best fits the premaxilla or the outline of the premaxilla. The center of this circle was defined as the midpoint of the premaxilla.
The TWG angle used to assess the sagittal position of the mandible is formed by using the following points (Figure 2):
T Point (Tuberculum Sella):The mean intersection point of the lower contours of the anterior clinoid processes and the contour of the anterior wall of the Sella. W Point (Wing Point):The intersection of the contour of the ala major with the jugum sphenoidale. G Point:Center of the largest circle that is tangent to the internal anterior, posterior, and superior surfaces of the mandibular symphysis.
TWG Angle.
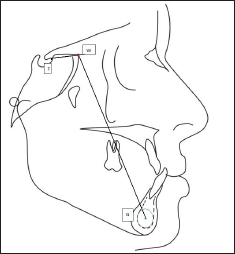
Point G 11 was determined by the center of the largest best-fit circle tangent to the internal anterior, inferior, and posterior surfaces of the mandibular symphysis.
Materials and Methods
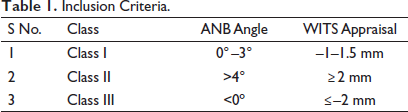
The study was conducted to develop two new cephalometric angles, TWM and TWG, for which a total of 120 pretreatment lateral cephalograms from the records of the Department of Orthodontics and Dentofacial Orthopaedics were traced; 90 met the inclusion criteria based on cephalometric values of ANB angle and WITS appraisal as shown in the Table 1. The study was approved by the Scientific Ethical Committee of the institution and necessary ethical clearance was obtained prior to commencement.
Inclusion Criteria.
Assuming a pooled standard deviation of 13 units, the study would require a sample size of 27 for each group (i.e., a total sample size of 81 with equal group sizes) to achieve a power of 80% and a level of significance of 5%. Keeping an attrition rate of 10%, three samples were added to each group making the study population to be 90 (30 in each group).
From the selected radiographs, 30 were assigned to each group.
Out of the 30 radiographs which met the criteria for the class II group, subdivisions were done based on class II skeletal pattern primarily due to maxillary prognathism (II A) and mandibular retrognathism (II B) according to the values of SNA and SNB. A total of 12 and 18 patients were assigned to the subgroups IIA and IIB, respectively.
Out of the 30 radiographs which met the criteria for the class III group, subdivisions were done based on class III skeletal pattern primarily due to maxillary retrognathism (IIIA) and mandibular prognathism (IIIB) according to the values of SNA and SNB. A total of 11 and 19 patients were assigned to the subgroups III A and III B, respectively.
Radiographs that showed excessive vertical growth and increased lower facial height were discarded to eliminate the effect of these factors on sagittal position.
Further for each radiograph, angles such as SNA, TWM, SNB, and TWG were measured and recorded.
Statistical Analysis
Data collected was entered into Microsoft Excel and was visually screened for any missing data and for the validity of distribution assumptions. Data was analyzed using SPSS Version 20 (IBM Corporation, SPSS Inc., Chicago, Illinois, USA). Data was then summarized by finding means and standard deviations. Mean and standard deviations of TWM and TWG angles were calculated for all three groups. The one-way analysis of variance (ANOVA) was used followed by Tukey post hoc testing to determine whether there was a statistically significant difference between the mean values of the three groups. A p value ≤ .05 was considered to be statistically significant. The Pearson correlation test was done to check the correlation between SNA and TWM angles and also for SNB and TWG angles for all the groups.
Results
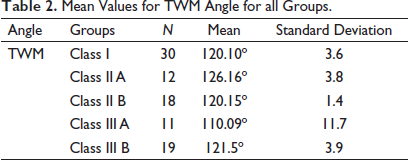
The mean value of TWM and TWG angles for class I, class IIA, class II B, class III A, and class III B are listed in Tables 2 and 3.
Mean Values for TWM Angle for all Groups.
Mean Values for TWG Angle for all Groups.
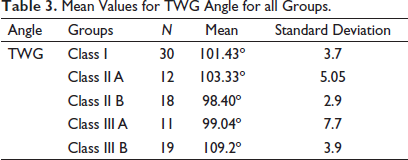
The mean values of TWM and TWG angles for the class I group were 120.1° ± 3.6° and 101.4° ± 3.7°, respectively.
The mean value of TWM for class IIA (maxillary prognathism) group was higher than the mean value for class I group, while the mean value of TWM for class IIIA (maxillary retrognathism) group was less as compared to the mean value of class I group.
The mean value of TWG for class IIB (mandibular retrognathism) group was less as compared to the mean value for class I group, while the mean value of TWG for class IIIB (mandibular prognathism) group was higher than the mean value of class I group.
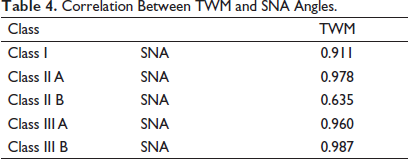
The Pearson correlation test was done to check the correlation of SNA and TWM angles. The test showed that the two angles have a strong correlation in all three groups. The correlation was significant at 0.01 level and the correlation coefficient was 0.911 for the class I group, 0.978 for the class IIA, 0.635 for class IIB, 0.960 for class IIIA, and 0.987 for class IIIB group (Table 4).
Correlation Between TWM and SNA Angles.
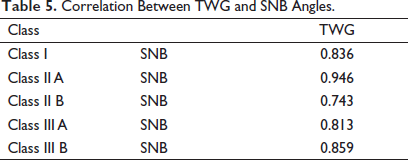
Similarly, the Pearson correlation test was done to check the correlation between SNB and TWG angles. The test showed that they have a strong correlation in all three groups. The correlation was significant at 0.01 and the correlation coefficient was 0.836 for class I group, 0.946 for class IIA, 0.743 for class IIB, 0.813 for class IIIA, and 0.859 for class IIIB group (Table 5).
Correlation Between TWG and SNB Angles.
Receiver operating characteristics curves showed that a TWM angle less than 116° has 96% sensitivity and 90% specificity for detecting retrognathic maxillary base. A TWM angle greater than 122° has 95% sensitivity and 98% specificity for detecting prognathic maxillary base. Receiver operating characteristics curves showed that a TWG angle less than 95° has 90% sensitivity and 85% specificity for detecting retrognathic mandibular base. A TWG angle greater than 105° has 92% sensitivity and 93% specificity for detecting prognathic mandibular base.
Discussion
Assessment of the sagittal jaw relationship is the most crucial step in orthodontic diagnosis and treatment planning. This assessment is made through cephalometric analysis, and for the same, several linear and angular measurements have been proposed over the years. Various studies have shown that linear measurements can get affected by the inclination of reference lines.12, 13 The most widely used parameters for assessing the sagittal position of the maxilla and mandible are the SNA and SNB angles, respectively. However, these angles have several drawbacks, that is, they can get influenced by various factors such as the length of the cranial base, the position of nasion (which is not stable and highly variable during growth8, 13, 14, 16–20), and position of point A and point B (which gets influenced by tooth movements14, 15). Moreover, point A is not clearly identifiable in many radiographs.12, 13
The middle cranial base completes its development earlier due to its function of protecting the brain and other vital organs.16, 17 Thus, the stability of the middle cranial base after the age of 8 makes it an excellent baseline for the study of facial growth.14–18, 20, 23 It has long been known that the tuberculum sella point (T) and wing (W) point, located in the middle cranial base, are highly stable. Information obtained from implant studies as well as from studies on human autopsy material20, 24–27 have confirmed the above findings.
Arat et al. 8 in their longitudinal study concluded that points T and W with 100% and 83% stability, respectively, were the most stable points in the cranial base, followed by nasion point with only 16% stability and basion with 0% stability considered as the least stable cranial landmark. Several authors have found similar results and showed that points T and W are highly reliable and have moderate to high reproducibility. 17
The authors also reported that the posterior longitudinal cranial base (T-Ba) shows a substantial increase during the growth period. 8 Sella turcica (S point), being an important parameter for most of the cephalometric analysis, is a point in the posterior cranial base; thus, it is vulnerable to growth changes, which can invariably affect various cephalometric readings. 8 Given the above facts, the present study was designed and utilized the two most stable landmarks points T and W in the middle cranial base to assess the sagittal position of maxilla and mandible. Although it can be argued that unlike N and S points, W point is slightly more difficult to identify due to the multitude of structures superimposing in the area; however, W point can be located easily with thorough knowledge of the structures present in the middle cranial base. Moreover, the numerous advantages of the W point outweigh any difficulties in locating the same.
Furthermore, points G and M, originally introduced by Nanda and Merrill and later used by Braun and co-workers,10, 11 are being constructed at the center of the largest circle placed tangent to the anterior, superior (represented by nasal floor), and palatal surfaces of the premaxilla and the internal anterior, inferior, and posterior surfaces at the mandibular symphysis, respectively. These points are not affected by local remodeling secondary to dental movements, unlike points A and B. The concept of the centroid point was introduced into orthodontics by Johnson. 21 The centroid or center of an area represents the mean point within a shape, about which it varies and is subject to least variation relative to non-mean anatomical points and therefore provides more stable and reproducible reference points. 22
Keeping these points in mind, the present study has introduced two new cephalometric angles angle TWM and TWG to assess the sagittal position of maxilla and mandible, respectively. The results showed that the mean values of TWM and TWG angles for the class I group were 120.1° ± 3.6° and 101.4º ± 3.7°, respectively.
Values greater than 120.1°± 3.6° for TWM angle suggest maxillary prognathism, while a value lesser than the mean value indicates maxillary retrognathism.
Similarly, values greater than 101.4º ± 3.7° for TWG angle suggest mandibular prognathism, while a value lesser than the mean value indicates mandibular retrognathism.
The second objective of the study was to assess the correlation between SNA and TWM angles and even for SNB and TWG angles using the Pearson correlation test. The test showed that these angles have a strong correlation for all three groups.
Hence, the results showed that TWM and TWG angles can be considered as a reliable method to assess the sagittal position of jaws and to determine the cause of sagittal discrepancy and treat accordingly.
Various new angles such as the W angle, Beta angle, YEN angle, Pi angle, etc., have been developed over the years, which help in the assessment of the sagittal discrepancy but do not determine which jaw is at fault. The recently introduced beta angle has certain demerits, that is, it depends on points A and B which get affected by alveolar remodeling; the condylion point (center of condyle) is difficult to locate and has limited reproducibility on closed mouth lateral head cephalograms. 28
YEN angle and W angle have utilized points M and G as geometric centers of maxilla and mandible, respectively, to eliminate the problems associated with points A and B, but these angles depend on sella point, which is a point in the posterior cranial base and is vulnerable to growth changes. 8
The limitation of the Pi angle is that it uses the true horizontal plane passing through nasion and it is evident from the literature that during growth, nasion point moves upward and forward. This movement can lead to changes in the angular measurements, and hence, this angle cannot be used with reliability in growing individuals. 29
The TWM and TWG angles not only help in identifying the type of malocclusion but also help in delineating which jaw is at fault and needs correction. These angles can be used in various longitudinal studies to assess the amount of jaw growth for the purpose of comparison and to generate norms. As these new angles depend on stable cranial base points and geometric points which are not subjected to alveolar remodeling, it becomes an excellent baseline for growth studies.
The two newly developed cephalometric measures, angle TWM and angle TWG, thus augment the diagnostic ability of the clinician and enable better treatment planning, as these angles can individually assess the sagittal position of maxilla and mandible. These angles can be used by any clinician to diagnose sagittal discrepancy, as they use stable, clearly visible, and highly reproducible landmarks with equal reliability by beginner and experienced.
However, the study can be repeated with different populations to generate mean values for different populations.
Conclusion
(1) Two new angles TWM for maxilla and TWG for mandible were established to assess the sagittal position of the maxilla and the mandible.
(2) The mean values of TWM and TWG angle for the class I group were 120.1° ± 3.6° and 101.4 ± 3.7°, respectively.
(3) The Pearson correlation test revealed that there was a strong correlation between SNA and TWM angle and similarly a strong correlation between SNB and TWG angle.
Thus, to conclude, these angles can be used as an alternative for assessing the sagittal position of the jaw bases and will give a clearer picture as stable and clearly visible landmarks are used.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and /or publication of this article.
Ethical Approval and Informed Consent
Necessary ethical clearances and informed consent was received and obtained, respectively, before initiating the study from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.