
Abstract
Facemask has been widely used in the successful correction of Class III malocclusion. A vast majority of the literature noted forward and a counter-clockwise rotation of the maxilla with facemask therapy. Although the counter-clockwise rotation is beneficial in the treatment of hypodivergent Class III patients, it is not advisable in high-angle Class III patients with anterior open bite. In order to minimize this undesirable side effect, the direction of protraction force at an angle of 30° downward from the plane of occlusion has been recommended. By directing the protraction force from a point 5 mm above the palatal plane and 15 mm above the occlusal plane minimized the counter-clockwise rotation of the maxilla. These attempts showed that the counter-clockwise rotation of the maxilla during protraction was unavoidable but can be reduced significantly.
Hence, the angulation of the extraoral elastics applied to the facemask for maxillary protraction is extremely important to reduce the counter-clockwise rotation of the maxilla.
This clinical pearl demonstrates an accurate and easy method to measure the angulation of the elastics applied to the facemask to reduce the above-mentioned side effect.
Introduction
Maxillary protraction is a well-accepted treatment technique for growing patients presenting with skeletal Class III due to maxillary deficiency. 1 The fundamental concept of maxillary protraction is by applying tensile force on the circummaxillary sutures and thereby stimulating bone apposition in the suture areas. 2 The facemask is a routinely used appliance to treat early maxillary deficiency. The variation in the direction, duration, and magnitude of force may result in different displacements of the nasomaxillary complex, which can lead to undesired effects such as the rotation of the maxilla in a counter-clockwise direction. 3
In order to minimize this unwanted side effect, the protraction force at an angle of 30° downward from the plane of occlusion has been recommended.3–5 Even so, the actual line of force is likely to be below the center of resistance (Cres) of maxilla, so a little downward movement of the posterior maxilla and opening of the bite anteriorly can be anticipated. 6 Hence it is very important to reduce this side effect, especially in patients with leptoprosopic facial form and anterior open bite.
This clinical innovation ensures the accuracy of line of force for facemask therapy to reduce the above-mentioned side effects.
Steps in Fabrication
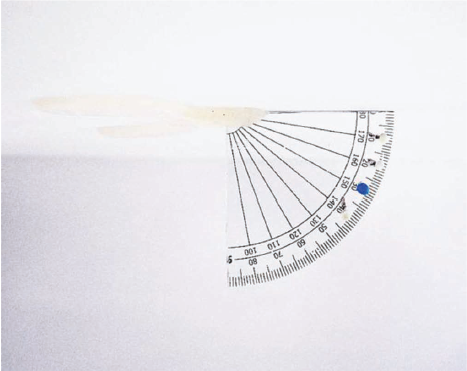
Cut the protractor exactly at the middle.
Attach the protractor to an acrylic bite plane.
Make small holes at the end of each 10-degree mark.
Fix small stainless steel wire hooks with composite button at each 10-degree mark to orient the extraoral elastics.
The 30° which is most commonly used angulation for facemask therapy is marked with blue colored composite resin (Figure 1).
Protramax Appliance.
Procedure
Guide the patient to bite on the bite plane so that zero degree coincides with the occlusal plane.
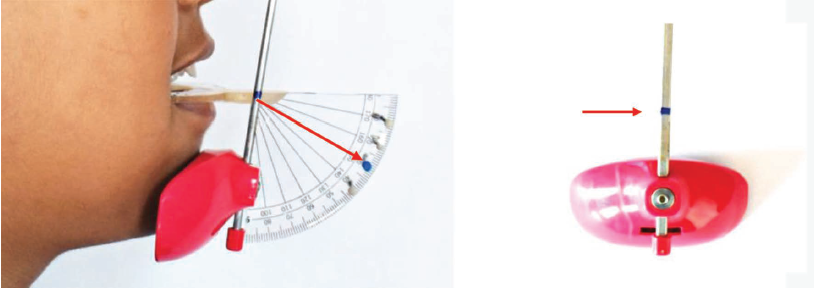
Orient the Petit’s facemask on the patients face to place a mark on the vertical rod of the facemask denoting the required angulation (Figure 2a,b).
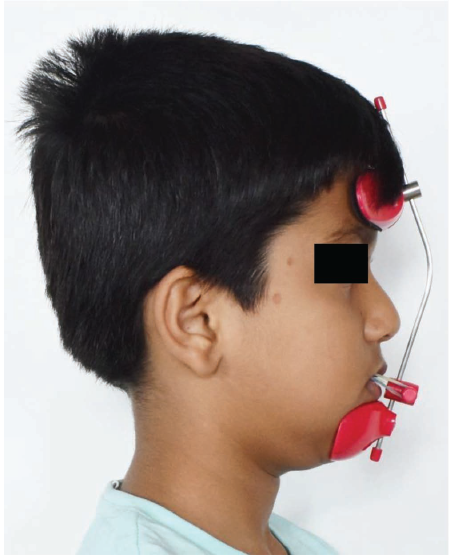
Place the horizontal arm of the facemask at the mark on the vertical rod and fix it with Allen wrench. This denotes the required angulation.
Engage the elastics from the hook of the bonded RME to the horizontal arm of the facemask (Figure 3).
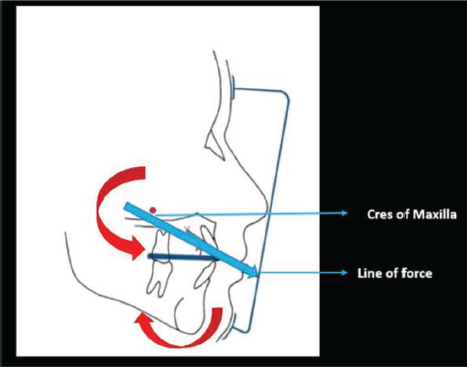
Orienting the elastics 30° to the plane of occlusion, the line of force passes closer and just below the center of resistance of maxilla. This reduces the counter-clockwise rotation of the maxilla and the resultant increase in lower anterior facial height (Figure 4).
Marking at 30° on the Vertical Rod of Petit’s Facemask.
Orienting the Horizontal Arm at 30° on the Vertical Rod. Engaging the Extraoral Elastics.
Biomechanics of Facemask Therapy with the Line of Force Passing Closer and Just Below the Cres of Maxilla.
Case Illustration
Case 1
Diagnosis and Etiology.
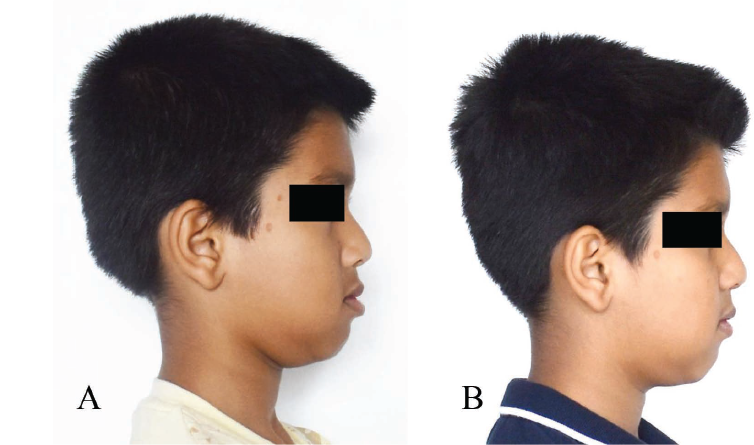
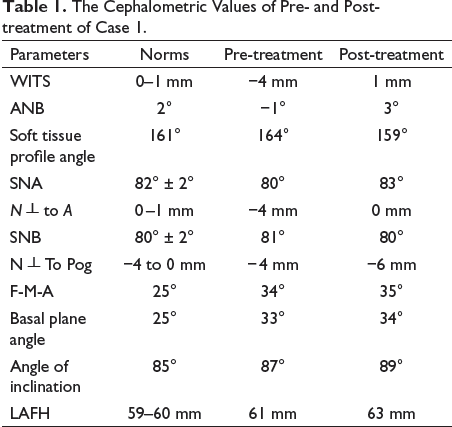
A 10-year-old male patient came to the Department of Orthodontics and Dentofacial Orthopedics presenting with a chief complaint of forwardly placed lower jaw. On extraoral examination, the patient demonstrated a leptoprosopic facial form, concave soft-tissue profile, maxillary retrognathism, mandibular prognathism with a vertical growth pattern (Figure 5a). The skeletal maturation stage of the patient was CS2, and MP3-F. Cephalometric analysis demonstrated a skeletal Class III relation with an ANB angle of −1°, WITS appraisal of −4 mm and N┴ to A of −4 mm suggestive of backwardly positioned maxilla. The patient demonstrated a vertical growth pattern with FMA of 34° and basal plane angle of 33° (Table 1).
(a) Pre-treatment Extraoral Photographs. (b) Post-facemask Therapy Extraoral Photographs.
(a) Pre-facemask Therapy Intraoral Photographs of Case 1. (b) Post-facemask Therapy Intraoral Photographs of Case 1.

The Cephalometric Values of Pre- and Posttreatment of Case 1.
Treatment Objectives.
The treatment objectives were to obtain a straight profile, advance the maxilla, achieve Class I skeletal profile, control of vertical proportions, correct bilateral posterior crossbite, establish Class I molar and canine relationship, normal overjet, overbite, improve facial profile and smile esthetics.
Treatment Plan.
The chosen treatment option for the patient was growth modification line of treatment with Facemask therapy. Followed by non-extraction treatment using MBT Versatile Plus appliance with 0.022″ slot.
Treatment Progress and Results.
The first step was insertion of bonded hyrax appliance with a hook soldered to the RME framework. Alt-RAMEC a protocol which involves alternate rapid maxillary expansion and constriction was followed for 7 weeks. After 2 weeks of Alt-RAMEC, Petit facemask was delivered to the patient. The extraoral elastic angulation was oriented with the aid of Protramax to pass the line of force closer to the Cres of maxilla. On completion of facemask therapy, pre and post functional cephalograms were traced and analyzed which demonstrated clinically insignificant counter-clockwise rotation of maxilla and good control of lower anterior facial height. The post functional cephalometric analysis showed an increase in ANB angle by 4°, WIT’s appraisal increased by 5 mm, soft tissue profile angle reduced by 5°, N perp to A increased by 4 mm, angle of inclination increased by 2° (Table 1).
Overall, the treatment outcome resulted in improvement of facial profile (Figure 5b).
Discussion
Facemask appliance is commonly used in Class III patients with maxillary under-development. The degree and direction of force application to maxillary dental arch are important factors in the treatment of such cases. This is especially important in Class III open bite subjects where the vertical dimensions are increased. Counter-clockwise rotation of the maxilla should be avoided as it can result in further increase in the vertical dimension. 7
Before deciding the direction of force application, locating the Cres of the maxilla is of utmost importance. The Cres of the nasomaxillary complex could be located at the posterosuperior ridge of the pterygomaxillary fissure registered on a median plane. 8
A force vector applied through the Cres region induces pure translation of the maxilla. 9 Hence, the line of force application must be closer to the Cres of the maxilla to minimize the undesired side effects. Though there are various studies describing the direction of force application, 10 there are no devices for measuring the exact direction of elastic force application during facemask therapy.
Hence, in this clinical innovation named Protramax device we have mainly focused on measuring the accuracy of extraoral elastic angulation during facemask therapy. The Protramax device was used in a patient with Class III skeletal profile associated with vertical growth pattern who was treated with facemask appliance as described above. The post facemask cephalometric values demonstrated significant correct of skeletal Class III with overall good control of vertical proportions. The appreciable advantages of Protramax include accurate measurement of elastic angulation that assists in orienting the line of force closer to the Cres of the maxilla. Also importantly, this device can be utilized as a simple and efficient chair side technique. The results that were achieved in this case report motivated us to plan a prospective cephalometric comparative study with and without the use of Protramax during Facemask therapy.
Being simple and economical to fabricate, we consider orthodontists can adopt this novel Protramax device during facemask therapy in their routine practice.
Conclusion
Protramax can be used as an effective aid for ensuring the accuracy of line of force to reduce the counter-clockwise rotation of maxilla during facemask therapy.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.