
Abstract
Aim
To analyze the pulpal stress in varied orthodontic tooth movements at ideal force levels and different bone levels, and compare any differences in pulpal stress values between anterior and posterior teeth.
Materials and Methods
Four Finite Element Method models of incisor and molar teeth were simulated with normal bone height and 50% bone height. Each of these models was loaded with five different types of orthodontic tooth movements—Tipping, Translation, Intrusion, Extrusion, and Rotation. The ideal force levels simulated for each type of tooth movement were: Intrusion-20 g, Extrusion-60 g, Tipping-60 g, Translation-120 g, Rotation-60 g. The pulpal stress was evaluated at three levels—pulp chamber, pulp canal, and below root apex, so that we get three values of pulpal stress for anterior and posterior teeth, for each type of tooth movement and its corresponding force level.
Results
The results showed that in both incisor and molar models with normal bone height as well as 50% bone height, rotation gave the highest pulpal stress while translation gave the least. In both incisor and molar models with normal bone height as well as 50% bone height, pulpal stress was found out to be highest in the root apex region of the tooth. The stress values for incisor and molar models with 50% bone height were found to be almost double that of the models with normal bone height. The pulpal stress for incisor teeth was found to be greater than the molar teeth for all types of tooth movement.
Conclusion
The present findings indicate that the stress manifested below the root apex is highest. Rotational movements induce the highest stress and translational forces develop the lowest stress related to the physiologic capillary blood pressure. Furthermore, in situations with reduced periodontium, lower forces are needed to reach the maximum tolerable stress compared with teeth with intact periodontium.
Introduction
Orthodontic tooth movement is majorly based on the principle of application of force to a tooth for a suitable period of time, which may vary from months up to several years. This evokes a pronounced biological reaction in the periodontal ligament (PDL) and pulp. The dental pulp is one of the constituents of the periodontium and is affected by the way the periodontal complex dissipates the loads during mastication. 1 The periodontal disease determines loss of attachment and bone resorption and reduces the ability of the periodontal complex to efficiently support the functional loadings. 1 The preservation of the periodontium at various levels of periodontal resorption is majorly dependent on the knowledge of stress distribution within dental pulp.
Orthodontic forces are known to produce a series of changes in dental pulp after tooth movement. These changes might be regressive leading to disturbance of pulpal blood flow and eventually the loss of pulp vitality. 2 It was proposed by Hamersky et al. that teeth may lose its vitality due to excessive and prolonged orthodontic forces. 3 Some studies have reported an increased number of irreversible inflammatory reactions of the pulp when teeth are periodontally compromised.4, 5 Orthodontic force type, duration, and amount can also result in disturbances in blood flow.4, 6 Proffit et al. 7 reported that light continuous forces have little or no effect on dental pulp. But in the literature, the reaction of dental pulp to orthodontic forces has been reported to vary from mild hyperemia to complete necrosis.8, 9 Increased levels of inflammatory mediators have been identified in pulp of teeth exposed to orthodontic forces. Therefore, from a clinical perspective, it is hypothesized and unanimously accepted that the magnitude of pulp inflammation or injury is directly proportional to that of the applied force. It is therefore tempting to speculate how the amount of pulpal inflammation or injury directly relates to the degree of applied orthodontic force.
Stresses generated within the dental pulp by an orthodontic force is an important factor that needs to be evaluated. There is scarcity of data about prevalence of long-term pulpal damage due to orthodontic treatment, and figures vary widely, ranging from 2% to 17% for root canal obliteration and from 1% to 14% for pulpal necrosis in adolescents treated orthodontically. 6 For avoiding irreversible changes in the dental pulp, it becomes important to correlate orthodontic forces with factors such as the grade of bone loss and the type of tooth (anterior or posterior).
In the past decade, the application of a well proven technique—the Finite Element Method (FEM)—has revolutionized the dental biomechanical research. With FEM, it is possible to anticipate the tissue responses to orthodontic mechanics applied. Its principle is based on the division of a complex structure into smaller sections called elements. Physical properties, such as the modulus of elasticity and Poisson’s ratio, are applied to these elements to indicate the object response against an external stimulus such as an orthodontic force. FEM is currently considered an ideal method for modeling of tooth supporting tissues, thus enabling us to inquire about how the loads are distributed and absorbed by the tissues and evaluating the produced stress as well. 7
The percentage of adult patients seeking orthodontic treatment has significantly increased in recent decades. Such patients often require multidisciplinary treatment, particularly when they are periodontally compromised. A prime challenge with advanced periodontal bone loss is accomplishing controlled tooth movement without causing complications because of an increased crown-to-root ratio. Excessive orthodontic force with advanced periodontal bone loss might traumatize the periodontium and pulp.
Therefore, the aim of this study was to evaluate, using a three-dimensional (3D) FEM analysis, the behavior of pulp following application of ideal orthodontic forces on anterior and posterior teeth, by varying bone level for different types of tooth movements.
Materials and Methods
Materials
2D CAD in Auto CAD 2017
3D modeling in Solid works 2018
Meshing in Hypermesh 2019
Finite Element Analysis (FEA) analysis in MSC Nastran 2018
Methods
The definition and the creation of the 3D model of the tooth consisted of the editing and constructing the tooth (enamel, dentin, pulp, cementum) and the accompanying structures (periodontal ligament, surrounding cortical, and cancellous bone), according to morphological and anatomical data. The PDL was stretched between surrounding bone and the tooth root, and its thickness being 0.16–0.24 mm. The cortical bone layer had an average length and thickness of 2 mm, and the residual bone was trabecular bone. The FEA was performed with the use of a software program coded with a FEM algorithm. Boundary conditions, material properties (Elastic constants, Young’s modulus, and Poisson’s ratio), and loading protocols were assigned to each finite element, defining how the model would deform under the applied loads. The FEM models were loaded up with 4-node tetrahedrons, and each of these models had 5,043,500–6,056,688 tetrahedral elements and 1,001,567–1,045,683 nodes.
A total of four models were simulated:
1st model: Central incisor with normal bone height 2nd model: Central incisor with bone height reduced to half 3rd model: 1st molar with normal bone height 4th model: 1st molar with bone height reduced to half
Also, five different types of orthodontic tooth movements were simulated in all the FEM models: Intrusion Extrusion Tipping Translation Rotation
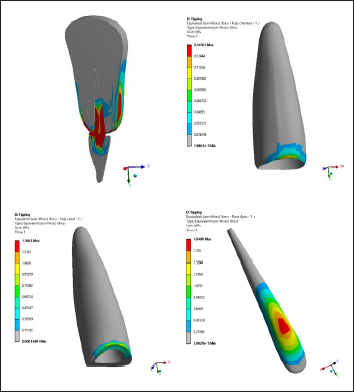
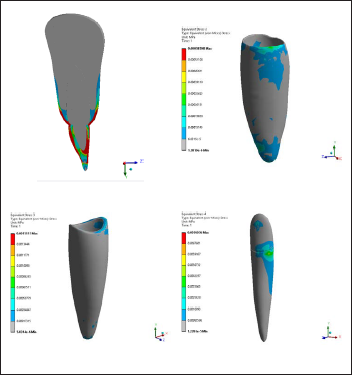
The ideal force levels were simulated for each type of tooth movement: Intrusion-20 g, Extrusion-60 g, Tipping-60 g, Translation-120 g, Rotation-60 g. 8 The pulpal stress was evaluated at three levels—pulp chamber, pulp canal, and below root apex, so that we get three values of pulpal stress for anterior and posterior teeth, for each type of tooth movement and its corresponding force level. The mechanical behavior of the structures were reflected by the stress magnitudes and also numerically represented as a color-coded projection on the FEM model.
Results
Incisor Model
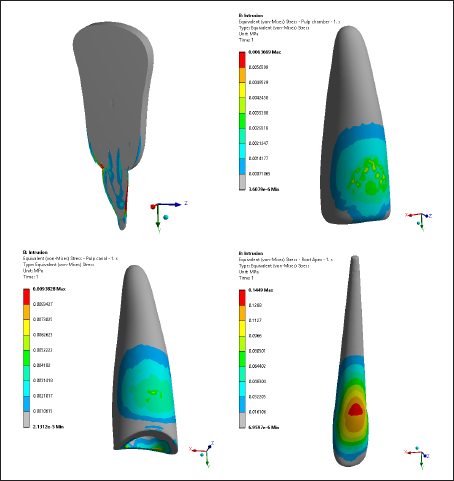
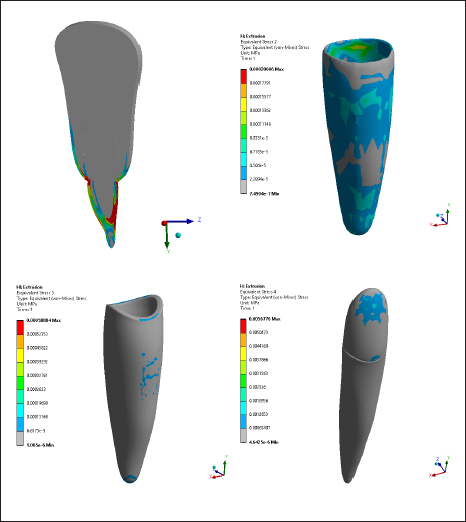
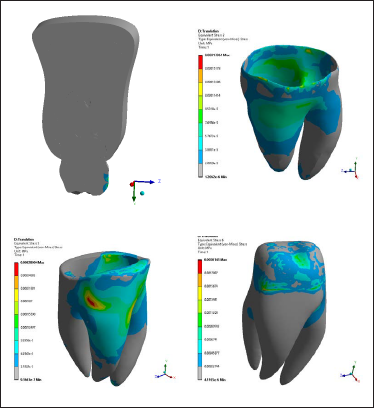
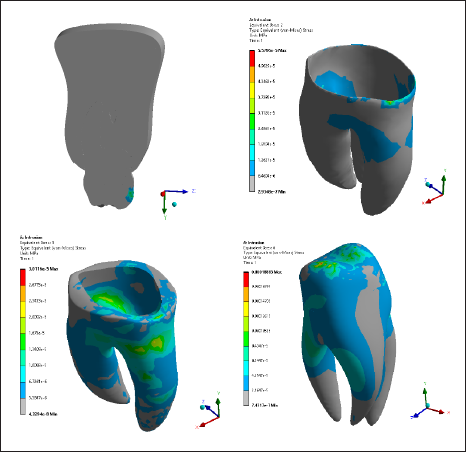
As can be observed from Tables 1 and 2, and Figures 1 to 5, the stress values for incisor model with 50% bone height were found to be almost double that of incisor model with normal bone height. In incisor models with normal bone height as well as 50% bone height, rotation gave the highest von Mises stresses and translation gave the least stress to the pulp. In both the models, pulpal stress was found out to be highest in the root apex region of the tooth.
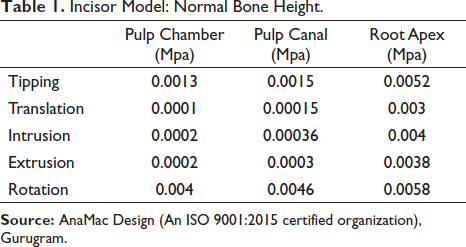
Incisor Model: Normal Bone Height.
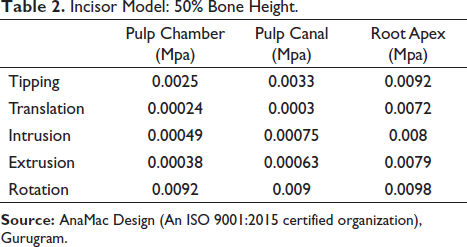
Incisor Model: 50% Bone Height.
Molar Model
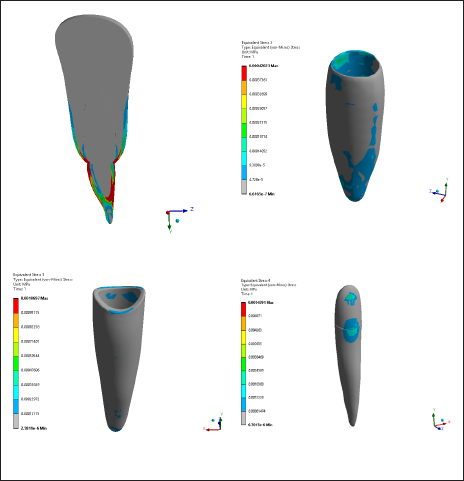
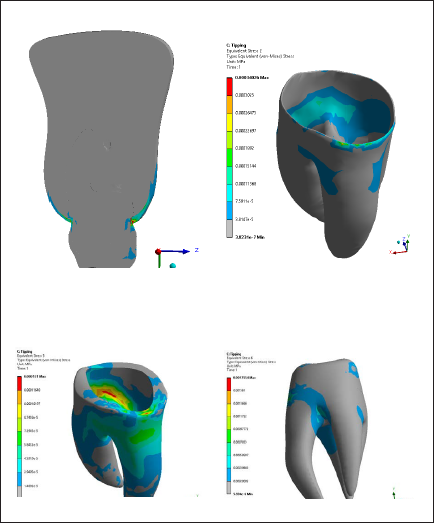
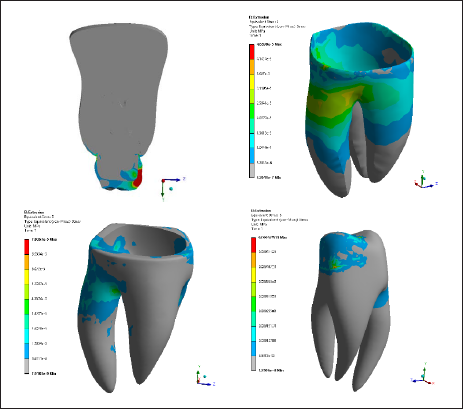
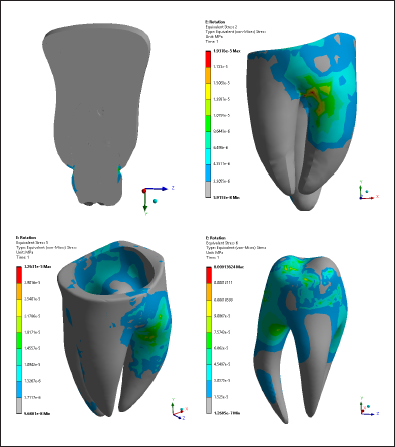
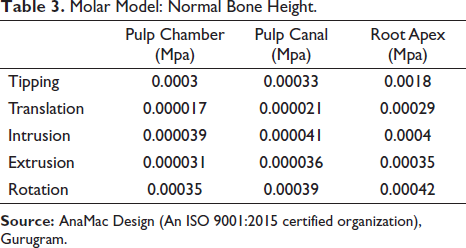
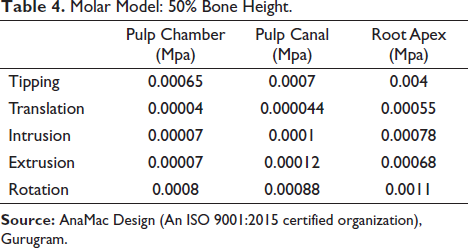
As can be seen from Tables 3 and 4, and Figures 6 to 10 the stress values for molar model with 50% bone height was found to be almost double that of molar model with normal bone height. In molar models with normal bone height as well as 50% bone height, rotation gave the highest von Mises stresses and translation gave the least stress to the pulp. In both the models, the pulpal stress was found out to be highest in the root apex region of the tooth. When stress values for incisor and molar teeth were compared, incisor teeth showed higher pulpal stress than molars.
Molar Model: Normal Bone Height.
Molar Model: 50% Bone Height.
Discussion
Profitt has explained that the orthodontic force applications may produce periodontal inflammatory reactions but should not show effects beyond mild inflammation of human dental pulp. Barwick and Ramsay 10 found no pulpal blood flow reduction with laser Doppler flowmetry during and after brief intrusive force application. On the other hand, Butcher and Taylor 11 demonstrated that the application of retraction forces caused pulp necrosis in monkey teeth.
There are few data in the literature regarding the values of maximum stress load which can be borne by dental pulp during orthodontic treatment. Tanaka et al. 12 showed that the dental pulp can withstand forces up to 2.94 MPa without signs of pulp damage. A systematic review by Von Bohl et al. 13 showed that there is no conclusive evidence for a direct relation between level of orthodontic force and pulpal reaction in human teeth. Since there is still debate about the optimal level of orthodontic forces that human teeth can withstand without causing pulpal inflammation or necrosis, we were interested to investigate the relationship between orthodontic force and its effects on the dental pulp.
Some previous studies14–17 evaluated the influence of orthodontic forces on dental pulp which showed that the magnitude of force applied to teeth dramatically varied between the studies (0.5–44 N). In the present study, we used Profitt’s 8 recommended optimum forces for orthodontic tooth movement that is, for tipping 60 g, translation 120 g, intrusion 20 g, extrusion, and rotation 60 g.
In this study, results showed that the stress at the root apex was shown to be higher than at the pulp chamber and pulp canal for each of the five types of orthodontic forces. This could be due to the fact that the neurovascular bundle of the tooth passes through the apical foramen in the root apex. This result is supported by a study done by Moga et al., 2 where they found that stress manifested at root apex was higher than apical third of root.
For the incisor and molar at 50% bone loss, rotational movements showed highest stress at root apex—0.0098 MPa and 0.0011 MPa, respectively. The higher stress value for incisor model could be due to the fact that incisor has lower surface area than the molar. For the incisor and molar at no bone loss, translational movements showed lowest stress—0.0001 MPa and 0.000017 MPa, respectively. This result is in confirmation with the outcomes shown by Moga et al., 2 where the stress was found to be 0.0009 MPa for translational movements at no bone loss.
For the highest evaluated translational force (120 g), the incisor exhibited stress at root apex ranging from 0.003 MPa (no bone loss) to 0.0072 (50% bone loss), and molar showed stress at root apex ranging from 0.00029 MPa (no bone loss) to 0.00055 MPa (50% bone loss). The results in the present study confirm those acquired by Jeon et al., 18 in which they assessed using translational forces the apical stress in the PDL of a maxillary 1st molar, and reported stress levels of 0.000445 MPa (3 mm bone loss), 0.000403 MPa (6 mm bone loss), and 0.000371 MPa (no bone loss).
As expected, lower stress levels for incisor (extrusion 0.0038 MPa, intrusion 0.004 MPa, tipping 0.0052 Mpa, and rotation 0.0058 MPa), and molar (extrusion 0.00035 MPa, intrusion 0.0004 MPa, tipping 0.0018 Mpa, and rotation 0.00042 MPa) were found in this study with intact periodontium, which is in confirmation with study done by Vikram et al. 19 This might be due to the fact that with a healthy periodontium the stress manifested in the tooth would be less than when the tooth is periodontally compromised. Excessive orthodontic force with advanced periodontal bone loss may traumatize the periodontium, and increased apical pressure because of reduced bony support may contribute to apical root resorption. Contrary to these, increased values of stress were obtained by Geramy (force 1 N, stress for intrusion 0.115–0.185 MPa, stress for tipping 0.026–0.722 MPa), 20 Hemanth et al. 15 (force 0.2–1 N, stress for intrusion 0.01337–0.02006 MPa, stress for tipping 0.0144–0.01646 MPa)16, 17 and Kumar et al. (force 1 N, stress for intrusion 0.074–0.315 MPa, stress for tipping 0.08–0.66 MPa) 21 for maxillary central incisors with no to 8 mm bone loss. Differences in all these stress values might be because of diverse tooth anatomies with varying PDL surfaces for model assumptions.
In the present study, the highest stress at root (0.0098 MPa caused by rotation) for incisor with decreased periodontium (50% bone loss) was higher than the physiologic values for capillary blood pressure (0.0020–0.0047 MPa) 16 and lower than PDL’s tolerable stress (0.015–0.026 MPa). 22
For incisor with intact periodontium, only rotational and tipping tooth movements resulted in a higher root apex stress than the physiologic values for capillary blood pressure. For molar with normal periodontium, the root apex stress acquired was lower than the physiologic values for capillary blood pressure for all types of tooth movements. It is confirmed by these results that the orthodontic forces applied (in the range indicated by Proffit 8 —20 g, 60 g, 120 g) are completely tolerable physiologically and do not affect pulp vitality or the PBF, except for tipping and rotational movements on incisors.
No study yet has evaluated and compared pulpal stress in anterior and posterior teeth when orthodontic load is applied to the teeth. The results in our study indicate increased pulpal stress in incisors than molars for all types of tooth movements, which might be explained by incisor being a single-rooted tooth with a conical apex having a smaller root surface area than the molar.
In the present study, it was noted that with 50% bone loss, the stress values were notably greater due to the combination of loss of bone and PDL and the anatomy of apical region. These results showed that when the stress at root apex is doubled, bone loss became directly proportional to the reduction in force levels for each of the types of orthodontic tooth movements. Clinically, these results show that when the periodontium is reduced, lower forces are required to reach the maximum stress that is tolerable in comparison with teeth with intact periodontium. Alveolar bone height loss causes an increase in von Mises stress values at all levels. 18 Similarly, Ghuloom et al. 23 (2017) reported a correlation among the root apex stress, bone loss, and reduction in force levels for the translational movement. The translational movement of a maxillary 1st molar for three levels of bone loss (2.5, 5, and 6.5 mm) were investigated in this study by Ghuloom, which showed that decreased force levels were required to develop stress levels similar to those obtained in areas without bone loss (80% of the initial force of 300 g for 2.5 mm bone loss, 60% for 5 mm bone loss, and 35% for 6.5 mm bone loss). In another study done by Juan Cobo et al., 24 they found that after applying the labiolingual force in the canine, a progressive increase of the stress in the labial and lingual zones of the tooth, periodontal membrane and alveolar bone was observed when the alveolar bone was reducing. They explained that when a bone height reduction is simulated in the model, greater increase of tension in the periodontal membrane is produced when the bone loss ranges from 6 to 8 mm. The implications of a reduction in alveolar bone have been assessed from the point of view of change in the center of resistance. 20 Although 0.017 mm/year of bone resorption can be considered quite normal (Corn & Mark, 1989), increased resorption can be detected in the patients referred for orthodontic treatment.
It seems suitable to assume that increased orthodontic forces with advanced bone loss have a greater effect on the neurovascular bundle at the root apex and PBF. This relevantly emphasizes the importance of applying lower forces (Proffit recommended up to 1.2 N) 8 in appropriate activation intervals in adult patients. Nevertheless, more statistics on the tolerable stress at root apex and orthodontic loads without affecting the pulpal blood flow in cases with reduced PDL and bone is needed.
Conclusion
There are a series of changes in dental pulp after orthodontic forces are applied. FEA constitutes a non-invasive, precise method providing both quantitative as well as detailed data regarding the physiological responses occurring in periodontal ligament, alveolar bone, and dental pulp. It was concluded from this study that:
Rotation type of tooth movement produced the greatest stress in the pulpal tissue whereas translation produced the lowest pulpal stress, be it incisors or molars. Maximum amount of pulpal stress was concentrated at the root apex, for any type of tooth movement. As bone level decreased the pulpal stress values increased almost linearly. Anterior teeth showed more pulpal stress than posterior teeth, be it normal bone height or 50% bone height.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Required ethical clearances have been obtained from the institution IEC/ORTHO/13/19 before initiating the study. No informed consent was necessary for this study because no patient data or information was used to create FEM models.