
Abstract
Objectives
The study aimed to develop a regional version of the Malocclusion Impact Questionnaire (MIQ-Malayalam) for the Malayalam-speaking Indian population.
Methods
The English version of MIQ was translated into Malayalam through a rigorous translation process, followed by cross-cultural adaptation. Young people aged below 18 years who were just about to start orthodontic treatment were invited to complete the Malayalam version of MIQ along with the available native version of the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ). The MIQ-Malayalam was readministered after 14 days to assess test-retest reliability. Treatment need was assessed normatively using the Dental Health Component of the Index of Orthodontic Treatment Need (IOTN-DHC) and subjectively using Aesthetic Component of the Index of Orthodontic Treatment Need (IOTN-AC).
Results
A total of 210 subjects completed the questionnaires (males = 47.2%; females = 52.8%; age = 12-17 years, mean = 15 years and 3 months; standard deviation = 1.9) and 50 completed repeat questionnaires. Internal consistency and test-retest reliability were high (Cronbach’s alpha = 0.952; Intra-class Correlation Coefficient = 0.93). Exploratory factor analysis derived 4 factors with exclusion of 1 item. There were significant differences (P < .05) in MIQ scores between IOTN-DHC subgroups, ensuring discriminant validity. There was a high correlation between total MIQ and total PIDAQ scores (rho = 0.884), while low between total MIQ and IOTN-AC scores (rho = 0.203).
Conclusion
The Malayalam version of MIQ was found to be valid and reliable and can serve as a useful condition-specific measure of oral health-related quality of life.
Introduction
A pleasing face and an attractive smile are important in today’s modern society as they attract a great deal of attention during social interactions. 1 An individual’s oral health can have a significant effect on their life through oral symptoms, lack of function, as well as worsening emotional and social well-being. This has led to the concept of oral health-related quality of life (OHRQoL), the meaning and the significance of which is still debated. 2 It has been shown that malocclusion, the third most prevalent oral condition, can have a major impact on OHRQoL. 3
Orthodontic treatment, traditionally, was aimed at improving the dentofacial aesthetics and function based on normative measures with little or no attention paid to the patient’s well-being. 4 But, it is often the psychosocial factors that influence a patient’s perceived need for orthodontic treatment. 5 This can be assessed only with the help of psychometric scales. In recent years, the use of such patient-reported measures to assess the psychosocial implications of malocclusion has grown in importance. The Malocclusion Impact Questionnaire (MIQ) is one such condition-specific measure, which estimates the impacts of malocclusion on the OHRQoL of individuals.6, 7
Patel et al 6 conducted the initial qualitative steps for the development of MIQ and derived 3 themes. This was based on how the arrangement and appearance of teeth affect the individuals’ day-to-day life. The items identified through qualitative analysis were tested by Benson et al 7 and the questionnaire was found to be valid and reliable.
The original English version of MIQ, when tested in the UK 7 , New Zealand 8 , and Nigerian 9 populations, was found to exhibit good validity and reliability. Subsequently, the MIQ was translated into and validated in Chinese, 10 Moroccan Arabic, 11 and Spanish. 12 However, an Indian version of MIQ has not yet been developed. Hence, this study aimed to translate and cross-culturally adapt the MIQ for the Malayalam-speaking Indian population.
Methods
A cross-sectional cross-cultural adaptation of MIQ into Malayalam language was undertaken. The study was conducted in the Department of Orthodontics & Dentofacial Orthopedics, Government Dental College, Kottayam, after the study protocol was approved by the Institutional Review Board (IEC/M/14/2017/DCK).
Individuals under 18 years reporting for orthodontic treatment were included after obtaining their assent and signed informed consent from their parents. Those under treatment or with a prior history of orthodontic treatment, as well as those with structural or cognitive disabilities, were excluded.
The study was aimed at deriving a regional version of MIQ for the Indian population. The process included linguistic and psychometric validations of the translated scale. The former involved translating the original MIQ into Malayalam, a pilot-testing of the translated version among 30 subjects which was followed by back-translation, finally yielding the translated questionnaire. The validity and reliability of the translated scale was ensured by psychometric validation.
Condition-Specific Scale
The MIQ comprises 17 items and 2 global questions. The item responses are based on a 3-point severity scale (0 = “don’t” or “doesn’t,” 1 = “a bit,” 2 = “very or a lot”). The total score can range from 0 to 34, obtained by summing up the individual item scores. The responses for global questions are based on a 5-point severity scale (0 = “not at all,” 1 = “a little bit,” 2 = “a bit more,” 3 = “a lot,” and 4 = “very much”); the scores of which are presented separately.
Translation and Cross-Cultural Adaptation of MIQ
The cross-cultural adaptation followed the guidelines of Wild et al. 13 The translation process included the following steps: a team of 4 bilingual translators, who were proficient in both the languages, independently translated the original English version of MIQ into Malayalam, the regional language. A panel of experts which included an orthodontist, an English-teaching college professor, and a public health dentist with expertise in OHRQoL measure analyzed the translations and ensured conceptual equivalence between the translated and original versions. The initial draft was thus synthesized based on their recommendations. This was subjected to pilot-testing in a sample of 30 individuals, who reported for orthodontic treatment. At the end of the session, feedback was obtained from each of them separately regarding the clarity in language, vernacular expressions, and need for modifications in order to ensure face validity. Amendments were made in the draft questionnaire based on their suggestions, after discussion with the expert panel.
Another team of 3 translators, who were unaware of the original version of MIQ, back-translated the draft version into English. The original English and the back-translated versions were compared, inconsistencies corrected, and the final draft was derived.
Scale Validation
The sample size for scale validation was based on the rule of thumb, that is, total number of items in the scale multiplied by 10, hence 19 × 10 = 190. 14 Considering 10% missing data due to unfilled questionnaires, the final sample size was fixed at 210. Subjects who fulfilled the inclusion criteria and provided consent were administered with the hard copies of the translated MIQ along with the available regional version of the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ), which was validated before. 15 Subsequently, the malocclusion status was assessed normatively using the Dental Health Component of the Index of Orthodontic Treatment Need (IOTN-DHC). In addition, the patient-reported aesthetic component of the IOTN was recorded. The socio-demographic information of the participants was also gathered. The subjects involved in pilot-testing were not included for the scale validation.
On day 14, they were recalled for case discussion and treatment planning, when the first 50 participants were readministered with MIQ for test-retest reliability assessment. The mean time taken for completing the questionnaire was also noted.
The total MIQ scores were compared with self-rated IOTN-AC scores and total PIDAQ scores to determine convergent and concurrent validities respectively, while with IOTN-DHC scores to assess discriminant validity of the translated questionnaire.
Statistical Analysis
The data were entered into SPSS software (version 16.0) by the principal investigator and was cross-checked by one of the coinvestigators (EP). Cronbach’s alpha coefficient and Intra-class Correlation Coefficient (ICC) were applied to test internal consistency and test-retest reliability, respectively.
The Kaiser-Meyer-Olkin (KMO) test and Bartlett’s test of sphericity were performed to ensure adequacy of samples and its suitability for factor analysis, respectively. Exploratory factor analysis (EFA) using principal component analysis (PCA) with Varimax rotation and Kaiser normalization was carried out to assess the psychometric properties. 16 One-way analysis of variance (ANOVA) with post hoc Tukey test and correlation coefficients were used for scale validation. The level of significance was set at 5% (P < .05).
Results
Subject Characteristics
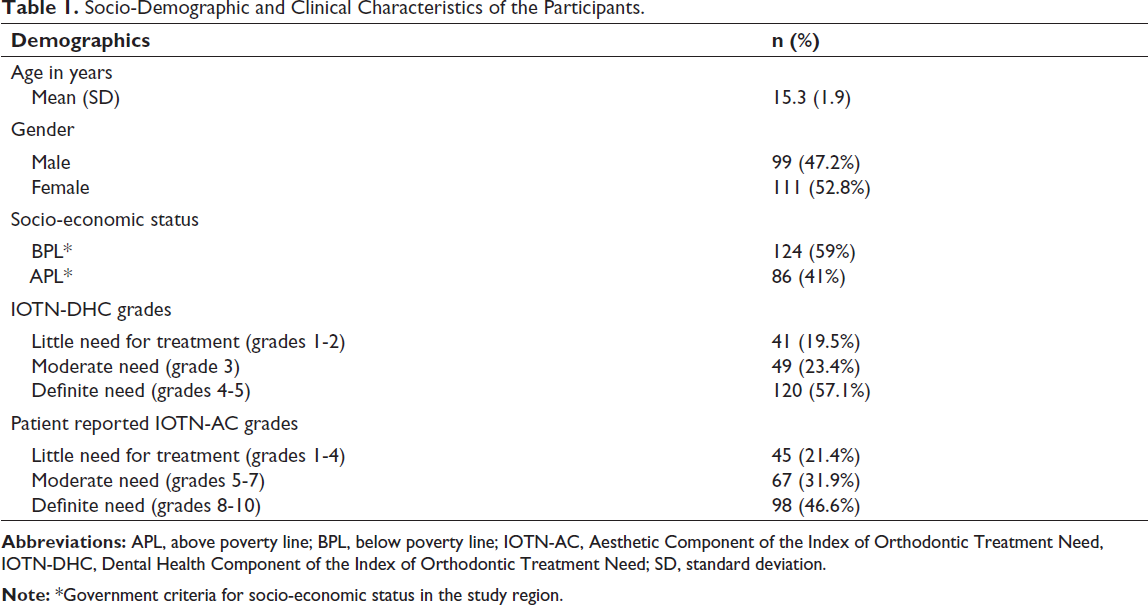
The MIQ-Malayalam was completed by 210 subjects (males = 47.2%; females = 52.8%) aged between 12 and 18 years (mean = 15 years 3 months; standard deviation [SD] = 1.9). There were no missing data. The average response time was found to be 11.5 min (SD = 1.4) per subject. The majority of participants belonged to the definite need category of IOTN-DHC (grades 4 and 5; 57%). Table 1 provides the socio-demographic characteristics of the subjects.
Socio-Demographic and Clinical Characteristics of the Participants.
Scale Validation
The Cronbach alpha yielded a reliability coefficient of 0.952, showing strong internal consistency of MIQ-Malayalam. The Cronbach alpha remained above 0.9 for each item, indicating the internal consistency was not affected adversely by any item (Table 2). Test-retest reliability correlation was 0.930 (95% confidence interval: 0.866-0.972).
Item-Wise Factor Loading After Exploratory Factor Analysis and Varimax Rotation With Kaiser Normalization, Amount, and Percentages of Explained Variance, and Cronbach’s Alpha If Item Deleted.
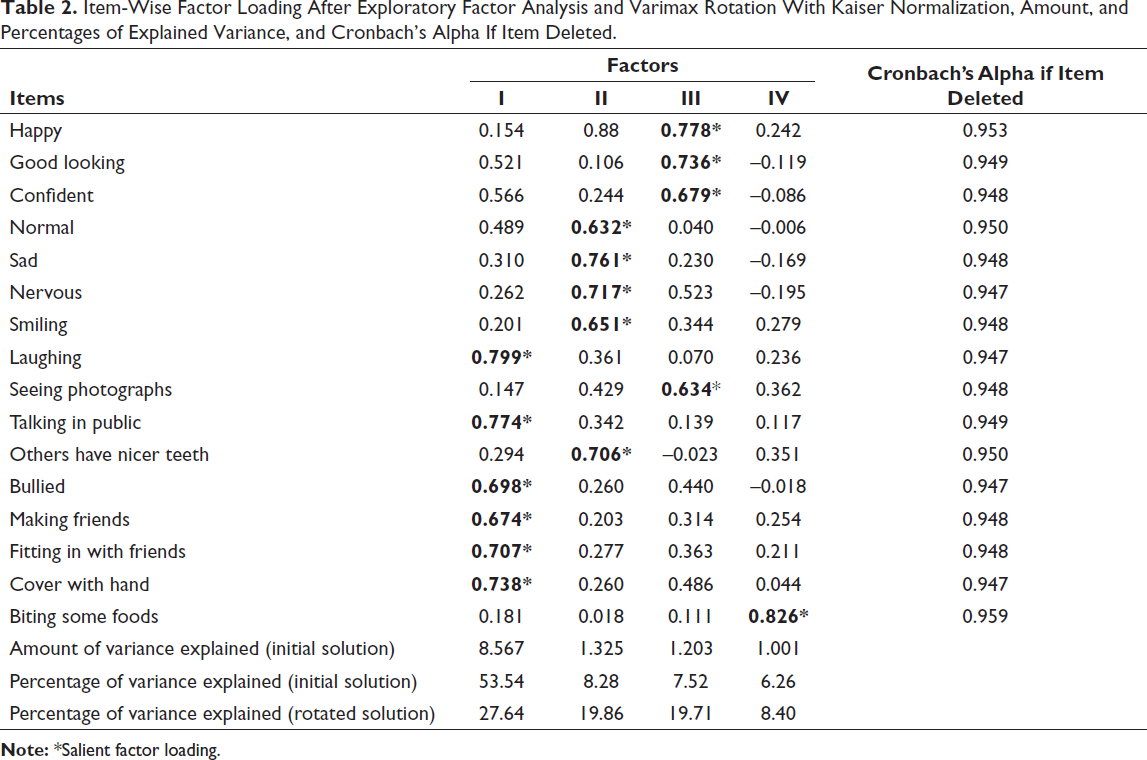
The sample size adequacy was confirmed by the KMO measure (0.76; P < .001). The Bartlett’s test of sphericity was significant (P < .001) showing the data was factorizable. EFA extracted 4 factors, each with an eigenvalue greater than 1.0 (Table 2). However, the initial factor loading with 17 items showed certain inconsistencies; hence, several rounds of factor rotation by excluding the cross-loaded items were performed. The most acceptable loading with the highest total variance (75.59%) was obtained when item 7 (Shy) was excluded (Table 2). Thus, the final version of the MIQ-Malayalam had 16 items.
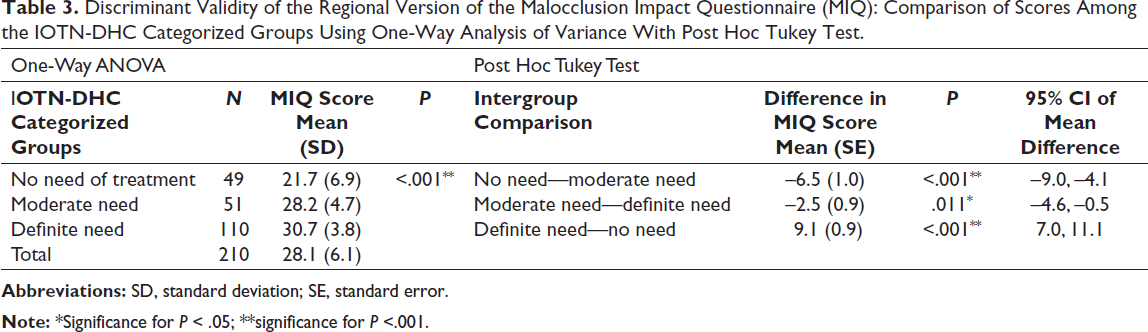
One-way ANOVA with post hoc Tukey test confirmed the discriminant validity of the translated scale with a statistically significant difference (P < .05) in the MIQ scores between the IOTN-DHC subgroups (Table 3).
Discriminant Validity of the Regional Version of the Malocclusion Impact Questionnaire (MIQ): Comparison of Scores Among the IOTN-DHC Categorized Groups Using One-Way Analysis of Variance With Post Hoc Tukey Test.
There was a high correlation (rho = 0.884) between the total MIQ scores and the total PIDAQ scores confirming convergent and concurrent validities (Table 4). The correlation between the total MIQ scores and self-rated IOTN-AC scores was lower (rho = 0.203) but significant (P < .05) (Table 4).
Convergent and Concurrent Validities of the Regional Version of the Malocclusion Impact Questionnaire (MIQ): Correlation of the Total MIQ Scores With IOTN-AC and PIDAQ Total Scores, Respectively.

Discussion
Several condition-specific17-19 questionnaires have been developed, validated, and used to study the OHRQoL associated with malocclusion and orthodontic treatment. MIQ is a recent addition, applicable to children between 10 and 16 years. For obvious reasons, the scales developed for one population and culture when used in another need translation, validation, and cross-cultural adaptation. Hence, the initial step was to translate the scale into Malayalam and cross-culturally adapt to the study population. Malayalam, the official language of the study region and one of the scheduled languages of India, is spoken by over 34 million people worldwide.
Certain items (confident, nervous, shy) in the initial draft questionnaire were difficult to comprehend by the study population. Therefore, subtle alterations were made, which were piloted for face validation and subjected to content validation by subject experts.
Conceptual equivalence between the 2 versions was ensured by the experts’ panel. The pilot test confirmed that the mode of questionnaire administration and response format were admissible, thereby confirming operational equivalence.
Cronbach alpha greater than 0.7 is considered acceptable for psychometric scales, while that above 0.8 is good and 0.9 is excellent. 20 ICC of 0.7 or more represents high reliability. 20 The MIQ-Malayalam showed excellent internal consistency (Cronbach alpha = 0.952), which was higher than the Chinese MIQ (0.929), 10 New Zealand version (0.924), 8 Moroccan Arabic (0.917), 11 and Spanish (0.85). 12 With an ICC of 0.93, it also showed high reliability, which again was more than the Chinese (0.893) 10 and Spanish MIQ (0.91). 12
EFA using PCA is a method widely adopted to ensure statistical construct validation of a scale, especially when the number of factors and the items under each factor are unclear. 16 The objective is to derive a scale with minimum items explaining the maximum possible variance of the construct. Varimax rotation is usually performed against Promax to reduce the items for the above objective. 16
The KMO value was more than 0.6 and the Barlett’s test of sphericity was significant, indicating the samples were adequate and factorizable. 21 Four factors were extracted based on the eigenvalue (>1). The loading cut-off for each item was set at 0.6. Several items demonstrated cross-loading to begin with. Hence, multiple rounds of factor rotation were performed, ensuring the Cronbach alpha of the scale was maintained each time. Finally, item 7 (Shy) was eliminated as it consistently exhibited cross-loading. Cultural differences of the participants might explain this. Another reason could be the unidirectional nature of the response options of MIQ as opposed to bipolar Likert scales, which are more commonly used. 22 The “alpha if item deleted” remained above 9 for item 7; however, elimination of the same did not affect the internal consistency reliability. Such reduction in items has been reported previously in the translational validation of PIDAQ. 23
The first factor contained items 9, 11, 13-16, which explained 53.54% of the variance. Factor 2 included items 4-6, 8, and 12, which explained 8.28% of the variance. Factor 3 contained items 1-3 and 10, explaining 7.52% of the variance. Finally, the fourth factor contained a single item (item 17) explaining 6.26% of the variance. The total variance in the MIQ-Malayalam (75.59%) was much higher than that in the Chinese version (65.95%), which also used EFA. 10
While 4 factors were extracted, as opposed to 3 in the Chinese MIQ, 10 no precise division of the domains was possible, except for factor 1 which could be differentiated as a “social impact” domain. This confirmed the unidirectional nature of MIQ.4, 5 Item 17 was functional in nature and it loaded distinctly during each rotation. Nevertheless, it was inappropriate to separate it as a “functional” domain with just 1 item, as a minimum of 2 are suggested. 24 The usual domains identified in condition-specific scales include psychological, social, aesthetic, functional, and so on.17, 19 Klages 17 introduced the dental self-confidence domain in PIDAQ. Such discrete domains were not possible in MIQ. Hence, a domain-wise impact assessment could not be performed.
One-way ANOVA results showed the MIQ-Malayalam was able to differentiate subjects with different treatment needs, graded using IOTN-DHC, with the results being statistically significant (P < .05). Thus, the scale demonstrated good discriminant validity.
The correlation between total MIQ scores and self-rated IOTN-AC was lower. Several reasons could be attributed for this. First, IOTN-AC is not representative of certain malocclusion traits such as bimaxillary protrusion (BMP), anterior cross-bites, and open-bites. On the other hand, BMP is highly prevalent in the study region with considerable number of participants belonging to that category. 25 With the photographs depicting only the frontal view, most BMP patients ended up grading themselves between 1 and 4, which indicates no treatment need. A previous study assessing the reliability of self-rated IOTN-AC also found a weak correlation of the same with the subjects’ expressed demand for orthodontic treatment. 26 Second, it is known that some people are concerned about quite minor problems and nearly 20% samples in this study had milder malocclusions.
Thus, the current version of MIQ with 16 items and 2 global questions proved to be reliable and valid for the Malayalam-speaking population across the globe. The global questions on QoL with bipolar options remain a strong component of the questionnaire. This obviates the need for the simultaneous use of another scale along with MIQ to assess concurrent validity in future studies, reducing the burden on patients.
Conclusion
The English version of MIQ was cross-culturally adapted for the Malayalam-speaking Indian population and the translated questionnaire demonstrated good psychometric properties. MIQ proved to be a simple condition-specific scale to assess the OHRQoL associated with malocclusion among younger adolescents.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical clearance was received from the Institutional Review Board (IEC/M/14/2017/DCK).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.