
Abstract
Context:
The objective of this systematic review is to analyze the pattern of masticatory muscle and its effects on craniofacial structures.
Method:
Electronic search was conducted for relevant studies in last 20 years (from January 1, 2002 to December 31, 2021) on the following databases: PubMed, Google scholar, Web of Science, Cochrane Library, and Wiley Library database. Hand searching of selected orthodontic journals was also undertaken. The selected studies were assessed for the risk of bias in Cochrane collaboration risk of bias tool. The “traffic plot” and “weighted plot” risk of bias distribution are designed in the RoB 2 tool. Two authors extracted the data which was then analyzed by another reviewer to obtain the final data.
Results:
Six studies fulfilled inclusion criteria. The risk of bias was high for all the studies. The sample size of the studies, methodologies used, muscles under study, parameters of muscles, and statistical analysis performed were extracted. The methodologies and results of the studies were found to be heterogenous.
Conclusions:
It is found that the vertical craniofacial dimensions can be better appreciated by masseter than by medial pterygoid. The volume of masseter is superior predictor than its cross-sectional area. The volume of the medial pterygoid affects the ramus of the mandible and the length and width of the lateral pterygoid are significantly correlated with transverse skeletal dimensions.
Introduction
The growth and development of the craniofacial structure depends upon functional need. Other than environmental factors, the craniofacial region’s soft tissue and muscles play a pivotal role in defining its morphology. According to Wolff’s law, the internal structure and shape of the bone are related to its function, which is indirectly affected by muscle function. According to Melvin Moss’s functional matrix theory, 1 the periosteal matrix (muscles and teeth) acts on the skeletal structures directly attached to it, resulting in basal bone remodeling and changes in its morphology. Solow 2 stated that the vertical dimensions of the craniofacial skeleton vary considerably among individuals. Those with long and short face morphologies showed the most extreme growth patterns in the vertical dimension, 3 as vertical craniofacial development is controlled by the elevator muscles.
Of all the facial muscles, masticatory muscles are pivotal in determining craniofacial morphology. The masticatory muscles are grouped into elevators (masseter, temporalis, and medial pterygoids) and depressors (lateral pterygoid). The elevator muscles influence the transverse and vertical dimensions of the face.
Length, cross-sectional area, orientation of muscle fibrils, volume, muscle thickness, width, function, and bite force4-9 are a few of the parameters that define the morphology of a muscle and helps to assess its functional needs. The shape and orientation of the masseter and medial pterygoid are important in the morphogenesis of the maxilla and mandible. Satiroglu et al 9 showed that masseter muscle thickness was significantly correlated to vertical face pattern and body mass index; individuals with a thick masseter muscle have a short face pattern. Muscle angulation also determines muscle performance. 10
Koolstra et al 11 stated that a masticatory muscle’s maximum bite force directly depends on its cross-section. The cross-sectional area of jaw muscles can vary across skeletal types I, II, and III. 12 Weijs and Hillen 12 stated that the cross-sectional areas of the temporalis and masseter muscles are directly proportional to the facial width, and those of the masseter and medial pterygoid are directly proportional to the mandibular length. According to Sassouni and Nanda, 13 the facial proportion and the orientation of the muscles are related—the masseter of skeletal deep-bite individuals is more vertical and that of open-bite individuals is more oblique. 13 Gionhaku and Lowe 14 showed that a masseter with more volume shows significant development of anterior facial height and a narrow mandibular angle. According to Azaroual et al, 15 the length and width of the lateral pterygoid are significantly correlated with transverse skeletal dimensions but not with any vertical skeletal dimensions. Although the above studies have confirmed the influence of the muscle and its effects on craniofacial morphology, it is imperative to know the concise relation between its form and function.
There are various techniques for evaluating and defining the muscular pattern, such as computed tomography (CT), ultrasonography (USG), magnetic resonance imaging (MRI), and so on. Ingervall 16 and Lowe 17 depend on electromyography (EMG) and bite force measurements in their studies. Weijs and Hillen 12 said that the mid-belly cross-section of muscles taken through CT is very similar to the anatomical cross-section. Hannam and wood21 (1989) used MRI instead of CT to take images of jaw muscles. Although there are many methodologies to evaluate a muscle, MRI is more advantageous than CT as it is a noninvasive technique that takes frontal, horizontal, sagittal, and even reconstructed angulated images; produces soft-tissue images of good quality; reduces X-ray exposure; and minimizes patient compliance.
This research asks the question, “What are the contributions of masticatory muscle pattern on craniofacial morphology?”
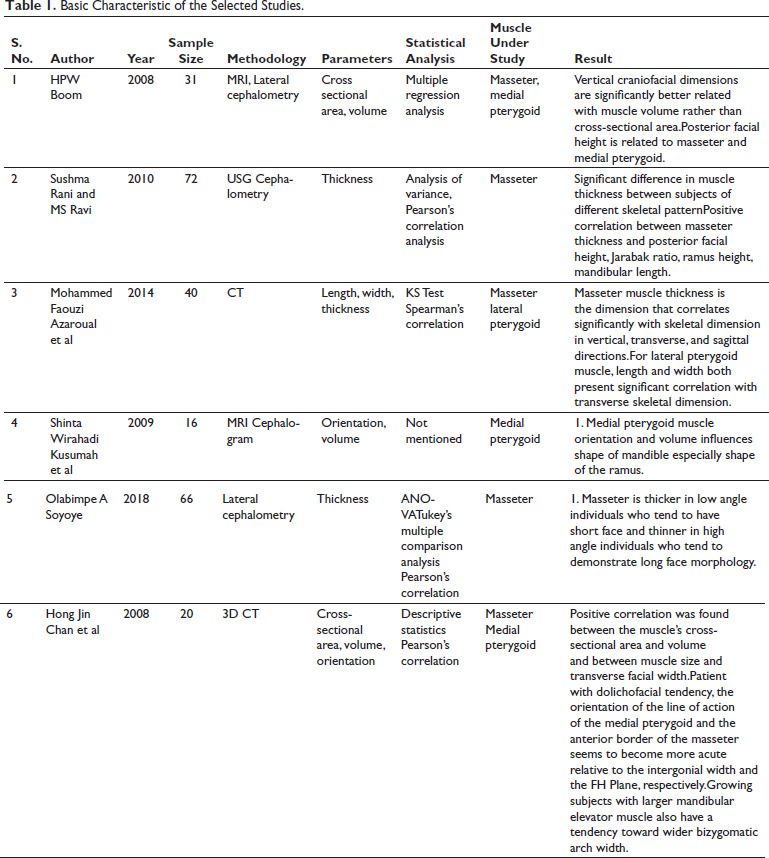
The focus of this study is to systematically review the available literature of the last 20 years to assess the contribution of masticatory muscle patterns to craniofacial structures. The characteristics of the selected studies are mentioned in Table 1.
Basic Characteristic of the Selected Studies.
Objective
This study aims to illuminate the contribution of masticatory muscle patterns to craniofacial morphology.
Materials and Methods
Protocol and Registration
The systematic review was performed following the preferred reporting items for systematic review guidelines. The main research question was framed based on population/participants, intervention, comparators/control, and outcomes (PICO). The protocol was registered with the number CRD42021283661 in the PROSPERO database (
Search Strategy
This systematic review was performed under the statement of preferred reporting items for systematic reviews (PRISMA). The comprehensive electronic database search was conducted with limited publications (from 2002/1/1 to 2021/12/31).
The literature was sought and collected through PubMed, Google Scholar, the Cochrane Library, Web of Science, and Wiley Library (Table 2). Only English language literature was selected. The record of references in the selected articles were searched by hand.
List of Search Engines and Their Results.
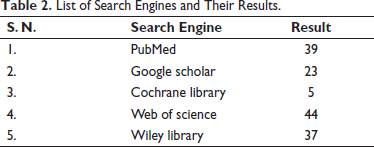
The following search terms were used for all search engines (Table 2):
(masticatory muscles) OR (muscles of mastication) OR (lateral pterygoid) OR (medial pterygoid) OR (masseter) AND (morphology) OR (craniofacial morphology) OR (facial morphology) AND (cephalometry) OR (cephalogram) AND (imaging) AND (MRI) AND (cephalograms) AND (MRI) OR (MRI)
The period for the search was set as January 1, 2002-December 31, 2021.
All search strategies showed similar sets of medical subject headings (MeSH) terms and texts. The shortlisted studies for full-text reading were selected and retrieved carefully based on inclusion and exclusion criteria.
Any difference in opinion was resolved after discussion. If necessary, a third-party author was consulted.
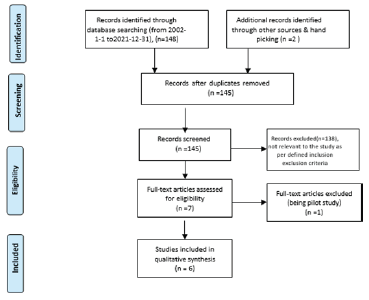
The PRISMA flow diagram has been shown in Figure 1.
Selection Criteria
The selection criteria were based on PICOS (population, intervention, comparison, outcomes, study design).
Focus of Research
Based on the PICOS criteria, our research focused on systematically reviewing the effect of masticatory muscle patterns on the craniofacial surface structure.
Inclusion Criteria
Inclusion criteria involve prospective and cross-sectional studies evaluating the effects of masticatory muscle patterns on craniofacial morphology.
POPULATION: Subjects undergoing routine dental examination prior to orthodontic treatment.
INTERVENTION: MRI/CT/USG/lateral cephalograms or combination in the selected samples.
COMPARISON: Comparison between muscle parameters of masticatory muscles and their effect on skeletal morphology in the population under study.
OUTCOME:
Parameters (cross-section, length, and angulation) of muscles that are more influential in framing craniofacial morphology. Determine the muscles of mastication that affect the skeletal architecture to a greater extent.
STUDY DESIGN: Prospective and cross-sectional studies that did not show any randomized control trials (RCTs) in the selected period of study.
Exclusion Criteria
Study type—Animal studies, case report, case series, pilot study.
Subjects—patients undergoing orthodontic treatment or orthognathic surgery.
Data Extraction
The data extraction was performed by two reviewers (AA and AN) independently to record general information such as author, year of publication, sample size, methodology, parameters, statistical analysis, muscle under study, and outcome of every individual study. The two recordings were further analyzed by a separate observer (MD) and final data was prepared.
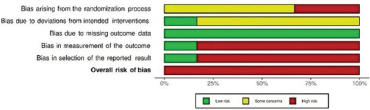
Risk of Bias or Quality Assessment of Selected Studies
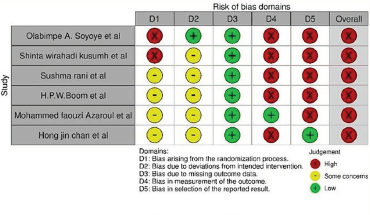
Observers AA and AN performed an independent quality assessment of the included studies by using the Cochrane collaboration risk-of-bias tool Risk-of-Bias Visualization (ROBVIS; RoB2) (
Five domains of bias were assessed: (a) bias arising from randomization process, (b) bias due to deviation from intended intervention, (c) bias due to missing outcome data, (d) bias in the measurement of the outcome, and (e) bias in the selection of the reported result.
The studies were categorized as follows: (a) high risk, (b) some concern, and (c) low-risk categories (Figures 2 and 3).
Results
Study Selection and Criteria
A total of 148 articles were identified after the electronic search (PubMed, Cochrane Library, Google Scholar, Wiley Library, and Web of Science) and 2 more were handpicked. After identical articles were removed, 145 were shortlisted for phase 1 screening (title and abstract reading), and seven were selected for phase 2 screening (full-text reading). Finally, 6 articles were chosen for qualitative review. One article was excluded from the study as illustrated in Table 3. All six articles were original studies; their basic characteristics and outcomes are tabulated separately in Table 1.
List of Excluded Studies and Their Reasons.
Synthesis of Results
Meta-analysis was not conducted due to the heterogeneity of the devices, techniques, additional results measured in each study, and the statistical method used.
Summary of Evidence
The selected articles were assessed and evaluated to analyze the contribution of masticatory muscle patterns to craniofacial morphology. In all these articles, year of study, sample size, methodology, parameters of muscles, different statistical analysis used, muscle under study, and its effect on craniofacial structures were assessed and evaluated. In all these studies, the methodological heterogeneity was noted, as authors have used different methods and parameters to assess the masticatory muscle pattern and its effect on associated skeletal structures.
In their prospective study, Boom et al 3 investigated whether jaw muscle volume or muscle cross-section area is strongly related to vertical craniofacial dimensions. The sample size was 31 (9 males and 22 females), with a mean age of 24.3 ± 9 (standard deviation [SD]) years and varied vertical dimensions. All subjects had a complete or nearly complete dentition and no functional disorder of the temporomandibular joint. Lateral cephalometric radiographs were available for each subject and were digitized using the software package view box (dHal software, KIFISSIA, Greece). The variables, that is, anterior total facial height [from nasion to menton], anterior lower face height [anterior nasal spine to menton], the ratio of (anterior lower facial height/anterior total facial height) × 100, posterior total face height [sella to gonion], posterior lower face height [articulare to gonion], the ratio of (posterior total face height/posterior lower face height) × 100, spina plane [ANS to PNS/mandibular plane angle (Go to Me)], and gonial angle [angle between Ar, Go, and Me] were measured to assess the vertical craniofacial dimension.
A series of axial MRI scans taken with a 1.0 T system (Siemens) was used for the imaging of 2 muscles, the masseter and medial pterygoid. The subjects were scanned in a supine position with the Frankfort horizontal plane perpendicular to the scan table. They were instructed to hold their teeth together but avoid clenching. The outcome of this study showed that the vertical craniofacial dimensions were significantly better related to muscle volume than the cross-sectional area and the posterior facial height was related to the masseter and medial pterygoid. In this study’s allocation sequence, no information was provided about sequence concealment or baseline differences between intervention groups. This suggests a problem with the randomization process during the selection of samples. There is a high risk of bias in the study as the participants were aware of interventions, and the outcome was influenced by the knowledge of interventions received. Moreover, there was clear evidence that a domain was not measured in multiple eligible ways; rather, data for only one or a subset of measures was fully reported without justification.
Sushma Rani and MS Ravi 23 studied 72 individuals between the ages of 18 and 25 divided into groups 1, 2A, and 2B according to their skeletal relationships as studied by lateral cephalometric parameters. Each group consists of 24 individuals with a 1:1 male-female ratio. Measurements on the lateral cephalogram were obtained under standardized conditions using the Planmeca PM 2002 cc proline machine. Angular and linear measurements were taken up to an accuracy of 0.5 degrees and 1 mm, respectively. In USG, all scans were taken using the LOGIQ 400 PRO SERIES scanner using a multi-frequency 7.5 to 11.0 MHZ broadband transducer. Bilateral imaging and measurements were carried out with the subjects in a supine position under 2 different conditions: (a) when teeth occluded gently, with the muscle in a relaxed position and (b) through maximum clenching with the masseter muscle contracted.
Group 1’s results showed a significant positive correlation between masseter muscle thickness (in the relaxed and contracted condition) and posterior total facial height (P = .001, .005), height of ramus (P < .0005), and mandibular length (P < .001, .021). There was a significant negative correlation between muscle thickness in the contracted state and mandibular plane angle (P = .090, .007). Group 2A showed a significant positive correlation between muscle thickness (in the relaxed and contracted condition) and posterior total face height (P < .0005), Jarabak ratio (P < .0005), ramus height (P < .0005), maxillary length (P = .004, .005), and mandibular length (P = .001). Significant negative correlations were noted between muscle thickness and mandibular plane angle (P = .001, <.0005), lower gonial angle (P < .0005), and PP-MP angle (P < .0005). Group 2B showed a significant positive correlation between muscle thickness (in the relaxed and contracted state) and ramus height (P = .001, <.0005). A significant negative correlation was noted between muscle thickness (in the relaxed and contracted state) and mandibular plane angle (P = .007, .001) as well as PP-MP angle (P = .013, .004). In this study’s allocation sequence, no information was given about sequence concealment and baseline difference between intervention groups. This suggests a problem with the randomization process. The study is at high risk as the participants were aware of the interventions, and the outcome was influenced by the knowledge of interventions received. Moreover, there is clear evidence that a domain was not measured in multiple eligible ways; rather, data for only one or a subset of measures was fully reported without justification. This puts the study at an overall high risk of bias.
Azaroual et al 15 conducted a study of 19 women and 21 men aged 20 to 45 with a mean age of 40.9 ± 12.8 (SD). A Siemen 32 row 64 slice spiral CT scan device was used for spiral acquisition of data around the facial bones with the mouth closed. The study was conducted in the parenchymal window for muscle measurements, in the axial and coronal planes. Bone measurements were taken after 3D reconstruction in Volume Rendering Technique mode. The results showed that, for the masseter muscle, thickness correlates significantly with skeletal dimension in vertical, transverse, and sagittal directions. For the lateral pterygoid muscle, length and width both present significant correlations with transverse skeletal dimensions. Analysis of these results shows that the dimensional characteristics of the masticatory muscles vary according to the vertical and transverse skeletal typology of the subjects concerned. In this study’s allocation sequence, no information was provided about sequence concealment and baseline difference between intervention groups. This suggests a problem with the randomization process. No information was provided about whether the participants were aware of the trial, and people delivering the interventions were aware of the participants assigned. There is clear evidence that a domain was not measured in multiple eligible ways. Therefore, the study has an overall high risk of bias.
In Chan et al’s 24 study, 20 children of mean age 11.9 ± 1.6 (SD) years underwent cranial CT examination. These patients were still growing and had no obvious facial asymmetry or malformation. 3D CT images were reconstructed for the evaluation of the cross-sectional size, volume, and spatial orientation of the masseter, medial pterygoid, and lateral pterygoid muscles. The vertical and transverse craniofacial forms of these muscle factors were assessed. The result showed a positive correlation between the muscle cross-sectional area and volume and between muscle size and transverse facial width (r = 0.84-0.89; P < .05). In this study’s allocation sequence, no information was given about sequence concealment and baseline difference between intervention groups. This suggests a problem with the randomization process. The participants and people delivering the interventions were aware of the participants assigned. Further, there is clear evidence that a domain was not measured in multiple eligible ways; rather, data for only one or a subset of measures was fully reported without justification. This puts the study at an overall high risk of bias.
Soyoye et al 18 conducted a study of 66 patients (21 males and 45 females) aged 12 to 30 years who presented for orthodontic appliance therapy. The inclusion criteria were no history of orthodontic treatment or orthognathic surgery. Participants with marked jaw asymmetry or craniofacial disorder were excluded. Standardized lateral skull cephalometric radiographs were taken for all participants using tech machine PaX-i. The masseter muscle thickness was measured using a real-time MINDRAY DC-7 ultrasound machine with a 7.5 MHz linear probe. The result showed a progressive reduction in muscle thickness, during relaxation and contraction, from low through normal to high angle cases. The high-angle cases demonstrated the least muscle thickness. In this study’s allocation sequence, no information was given about sequence concealment and baseline difference between intervention groups. This suggests a problem with the randomization process. No information was given about whether the participants were aware of the trial; people delivering the interventions were aware of the participants assigned. Domain 4 reveals a high risk because study participants were aware of the interventions and the outcome was influenced by the knowledge of interventions received. There was also clear evidence that a domain was not measured in multiple eligible ways; rather, data for only 1 or a subset of measures was fully reported without justification. So, the overall risk of bias is high.
For their study, Kusumah et al 25 selected 16 patients (5 males and 11 females), aged 13.5 to 27.5 years, with various craniofacial patterns and who were about to start orthodontic treatment. Lateral cephalometric radiographs and MRI were obtained and their image was uploaded to the computer in a digitizer. An area of the medial pterygoid muscle was selected by binarization from an MRI. The midsagittal plane MRI with a complete superimposed sagittal image of the medial pterygoid muscle was superimposed on the cephalogram using anatomical structures situated in the midsagittal plane of the head and shapes that could be identified from both radiograph and MRI images. The result showed various shapes of the medial pterygoid muscles. The inclination axis of the muscle was correlated with various cephalometric variables including SNB (r = 0.658), facial angle (r = 0.601), ramus inclination (r = 0.676), and Ba-Po% (r = 0.585). The muscle’s volume was also correlated with cephalometric variables such as ramus inclination (r = 0.453), Ba-Nmm (r = 0.676), Ba-Po% (depth) (r = 0.447), Ar-Go% (depth) (r = 0.444), and Ar-Go% (actual length) (r = 0.532). In this study’s allocation sequence, no information was given about sequence concealment and baseline difference between intervention groups, which suggests a problem with the randomization process. Domain 4 revealed a high risk because study participants were aware of the interventions, and the outcome was influenced by the knowledge of interventions received. There is also clear evidence that a domain was not measured in multiple eligible ways; rather, data for only 1 or a subset of measures was fully reported without justification. This put the study at an overall high risk of bias.
To summarize all 6 articles under study, as per Boom et al, 3 we find that vertical craniofacial dimensions (posterior facial height) are significantly better related with muscle volume (masseter and medial pterygoid) rather than cross-sectional area. Similarly, Sushma Rani and MS Ravi 23 found a positive correlation between posterior facial height (along with Jarabak ratio, ramus height, and mandibular length) and masseter thickness. Azaroual et al 15 showed a significant correlation between masseter muscle thickness and skeletal dimension not only in the vertical but also in the transverse and sagittal directions. The length and width of the lateral pterygoid muscle both present a significant correlation with the transverse skeletal dimension, similar to Chan et al’s 24 study. Growing subjects with a larger mandibular elevator muscle also had a tendency toward a wider bizygomatic arch width. According to Kusumah et al, 25 medial pterygoid muscle orientation and volume influences the shape of the mandible, especially that of the ramus. In Soyoye’s study, 18 the masseter plays an important role in defining facial pattern (short or long face).
Discussion
Balancing force distribution between oral and perioral structures is important for the harmonious development of dentition and orofacial structures. It is a proven fact that changes in craniofacial muscular activities that control a particular function may influence the developing underlying structures. 1 Studies have revealed a distinct relationship between muscular morphology—length, cross-sectional area, and orientation—and the structural pattern of craniofacial morphology,15, 18 which illustrates the craniofacial pattern variations in a population. It has been seen that muscles have an influential effect on the vertical,15, 19 transverse,7, 12, 20-22 and sagittal dimensions 10 of facial morphology.
The length of the masseter is positively correlated to lower facial height (anterior nasal spine to menton), ramus inclination, length of the mandible, ramal length, and upper and lower facial height. This is contradictory to Azaroual et al’s findings 15 where the relationship between masseter length and lower facial height is statistically insignificant. Based on statistically significant parameters, the cross-section of muscle has an influence on facial height (nasion to menton). This is contrary to Van Spronsen et al’s 20 findings that the masseter cross-sectional area is not significantly correlated with adult vertical craniofacial dimensions. The length of the masseter muscle is significantly negatively correlated with the mandibular plane angle, which is in accordance with Gionhaku and Lowe’s study 14 as well as with Satiroglu et al, 9 who found a negative correlation between masseter thickness and divergence.
The angulation of the muscle showed a significant correlation with the SNB and mandibular plane angle on the right side and with SNA and SNB on the left. Based on the number of significant parameters, the left side seems to have more influence than the right. The difference between the influential effect of both sides of the masseter muscle could be due to the difference in individuals’ bite forces and chewing patterns. This is in accordance with the study done by Hsu et al, 10 where angulation of masseter muscle was compared with the medial pterygoid muscle. The study concluded that the masseter is oriented more vertically than the medial pterygoid. The angulation of the medial pterygoid muscle has no significant correlation when compared bilaterally for the parameters; however, angulation of the medial pterygoid on the left side was negatively correlated to ramus inclination, ramal height, and thickness of the condylar head. In contrast, Kusumah et al’s 25 study showed a positive association with the shape of the ramus.
There are various diagnostic methods available to access the muscle parameters, such as CT, MRI, USG, EMG, and so on. MRI has been used as the most common tool for deciphering muscle patterns due to its obvious advantages of clear soft-tissue image, zero radiation, and so on.
At the time of registration with PROSPERO, this systematic review was the first to specifically examine the contribution of masticatory muscle patterns to craniofacial phylogeny.
For this systematic review, 148 articles were selected through the use of MeSH terms, and a few articles were handpicked. After using regressive scrutinization through inclusion and exclusion criteria, 6 articles from literature spanning the last 20 years were considered for this systematic review.
This systematic review was performed to acquaint clinicians with the authenticity of past research on the effects of muscle patterns on orofacial growth in order to formulate an efficient treatment plan. During the data search, there was no RCT available with respect to muscle parameters. Further, there is scope for future research to assess the effect of changes in muscle patterns pre and post orthognathic surgery, to reduce the chances of the tendency of relapse.
Limitations
Although randomization is the gold standard for the research, we cannot include RCT as muscle patterns cannot be randomized.
Bite forces cannot be calibrated during the intervention.
Because of heterogeneity in the study, meta-analysis of the studies is not possible.
Standardized intervention protocols cannot be followed as different interventions are performed by different researchers.
Conclusion
The effect of masticatory muscle patterns on craniofacial morphology has been well documented in the literature.
Vertical craniofacial dimensions are influenced more by the masseter muscle than the medial pterygoid.
Masseter muscle volume is considered a statistically significant parameter affecting craniofacial morphology in comparison to the muscle’s cross-section area.
The masseter muscle is thicker in short-faced individuals than in long-faced individuals.
In skeletal open-bite patients, the masseter is more horizontally placed relative to the SN, FH plane, and palatal plane.
The volume of the masseter determines the development of the anterior facial height and angle of the mandible.
The volume of the medial pterygoid affects the ramus of the mandible.
The length and width of the lateral pterygoid are significantly correlated with transverse skeletal dimensions but not with any vertical dimensions.
This systematic review revealed that the masseter muscle is the most extensively researched among all masticatory muscles.
In the last 20 years, little information has been made available about the medial pterygoid and almost none about the various parameters of the lateral pterygoid muscle and temporalis and their effects on the skeletal system.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.