
Abstract
Aim:
The aim of the study was to compare and evaluate the microleakage under the Adhesive Precoated Plus (APCP), APC Flash-Free (APCF), and conventional stainless steel (SLS) brackets on the occlusal and gingival sides of the bracket base.
Materials and Methods:
66 extracted premolar teeth were collected and divided equally into 3 groups. Bonding was done with APCP, APCF, and conventional SLS brackets using Transbond XT. After bonding, the samples were stored in a distilled water and thermocycled for 3000 cycles, followed by immersion in a 2% methylene blue for 24 h. After cleaning, the teeth were mounted in acrylic and sectioned longitudinally at about the center of the bracket in a buccolingual direction. Microleakage was recorded using a stereomicroscope.
Results:
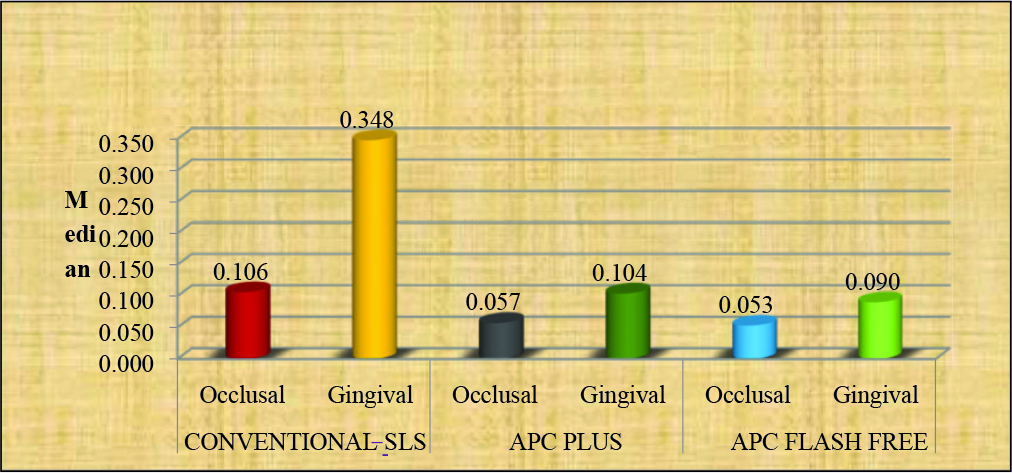
Kruskal–Wallis H test showed a significant difference (P < .005) in the microleakage scores between the 3 groups. Mann–Whitney U test showed a significant difference between group 1 to group 2 and group 1 to group 3 (P < .005) and an insignificant difference between group 2 and group 3 on the occlusal side (P = .116) and on the gingival side (P = .063).
Conclusion:
Conventional SLS bracket group exhibited greater microleakage scores at both occlusal and gingival sides, when compared with APCP and APCF groups.
Introduction
The introduction of the direct bonding technique in orthodontics by Buonocore 1 in 1955 revolutionized orthodontic therapy. Bracket bonding with light-cured composite has become increasingly popular in orthodontics because of longer material working time and flexibility in initiating the polymerization process, which means “on-demand polymerization.” 2 In 1992, a new-generation bracket system called adhesive precoated (APC) brackets were introduced. Each bracket is individually packaged, and the bracket bases are prepasted with the optimal amount of adhesives.3, 4 According to Cooper et al, 5 APC offers some advantages over the conventional system, such as consistent quality and quantity of adhesive, easy debonding, reduced adhesive wastage, improved asepsis, and better inventory control. The Adhesive Precoated Plus (APCP) system has provided better tolerance to humidity and has a fluoride-releasing effect. The adhesive's color change property helps the practitioner clean up the flash by providing a visual marker of adhesive placement. Conventionally, the flash needs to be removed before polymerizing the adhesive to avoid gingival irritation and plaque accumulation. 6
Studies aimed to reduce the excessive flash adhesive led to the development of different systems. The APC Flash-Free adhesive coated (APCF) appliance system developed by 3M Unitek (Monrovia, California, USA) uses individually packaged brackets with a low viscosity resin, applied to a nonwoven polypropylene mesh, which eliminates the need for flash removal and creates a seal to reduce microleakage. 7 Microleakage is an essential drawback of orthodontic adhesives because of photopolymerization shrinkage of the adhesive during curing. The shrinkage creates a gap between adhesive and enamel surface, allowing the infiltration of bacteria, fluids, and ions from the oral cavity. In addition to polymerization shrinkage, thermal stresses to the adhesive in the oral cavity would cause the adhesive joint's fatigue, causing microleakage. Microleakage can lead to white spot lesions under and surrounding the brackets and reduce the bond strength at the enamel-adhesive-bracket interface.8, 9
Previous studies10, 11 have shown increased microleakage at the enamel-adhesive interface rather than at the bracket-adhesive interface. Arhun et al 9 showed increased microleakage with metal brackets compared to ceramic brackets and on the brackets gingival side compared to the occlusal side. Kim et al 7 compared microleakage under APCP and APCF ceramic brackets and reported no significant difference between the systems in the extent of microleakage.
However, comparative studies reflecting the extent of microleakage under conventional metal brackets, APCP metal brackets, and APCF metal brackets are scanty. Hence, the present study has been taken up to assess the microleakage under APCF metal orthodontic brackets from gingival and occlusal surfaces at the enamel–composite interface and compare that with conventional metal brackets bonded with conventional composite adhesive and with APCP metal brackets.
Materials and Methodology
66 freshly extracted premolar teeth were collected. The sample size was determined using G*power version 3.1.9.2 (SPSS VERSION 14(SPSS Inc., Chicago, Illinois, USA)) with a confidence interval of 95%, power of 80%, α = 0.05, and effect size of 0.40. The sample included in this study was teeth with intact buccal enamel, teeth that were not subject to any pretreatment chemical agents (such as hydrogen peroxide), teeth having no cracks, no caries, and no previous orthodontic bonding. Teeth were stored in 0.1% thymol to inhibit bacterial growth. All samples were cleaned and polished with pumice and rubber prophylactic cups for 10 s and consequently etched with 37% phosphoric acid (D-tech dental technologies, Wagoli, Pune, India) for 15 s and then rinsed with water and air-dried to see the white frosty appearance of etched enamel. Teeth were divided into 3 groups: group 1 bonded with conventional metal brackets with conventional composite, group 2 with APCP metal brackets, and group 3 with APCF metal brackets. Each group consisted of 22 samples.
Group 1: Prepared samples from group 1 (22 premolars) were taken, and a thin layer of Transbond XT primer was applied onto the enamel surfaces, and a gentle burst of air was applied to uniformly spread the primer. The Transbond XT (3M Unitek. Monrovia, California, USA) adhesive composite was placed on the conventional stainless steel (SLS) bracket (3M Unitek) bonding surface, and then it was placed in the middle of the crown on the labial surface. The gentle force was applied to squeeze out the excess resin, which was removed using an explorer without disturbing the bracket.
Group 2: Prepared samples from group 2 (22 premolars) were taken, and a thin layer of Transbond XT primer was applied to the enamel surfaces, and a gentle burst of air was applied to uniformly spread the primer. APCP adhesive system brackets were placed on the middle of the crown on the labial surface. The gentle force was applied to squeeze out the excess resin, which was removed using an explorer without disturbing the bracket.
Group 3: Prepared samples from group 3 (22 premolars) were taken, and a thin layer of Transbond XT primer was applied to the enamel surfaces, and a gentle burst of air was applied to uniformly spread the primer. APCF adhesive system brackets were placed in the middle of the crown on the labial surface. All the adhesives were cured with light emitting diode (LED) with a wavelength between 450 nm and 470 nm and at an intensity of 1100 mW/cm 2 for a total of 20 s (10 s each on the mesial and distal sides).
To ensure complete polymerization of the bonding materials, all the teeth were stored in distilled water bath at 37°C for 24 h. All teeth were thermocycled for 3000 cycles between 5°C and 50°C. During the thermocycling procedure, all the teeth were exposed to 8°C for 30 s, followed by normal room temperature for 30 s and later to 45°C for 30 s. After the thermocycling procedure, roots of all teeth were sectioned 5 mm from the cervical margins, and exposed root canals were blocked with sticky wax. All teeth surface except 1 mm around bracket bases were coated with 3 different color varnishes to differentiate various groups (group 1 with red, group 2 with green, and group 3 with brown).
Microleakage Evaluation
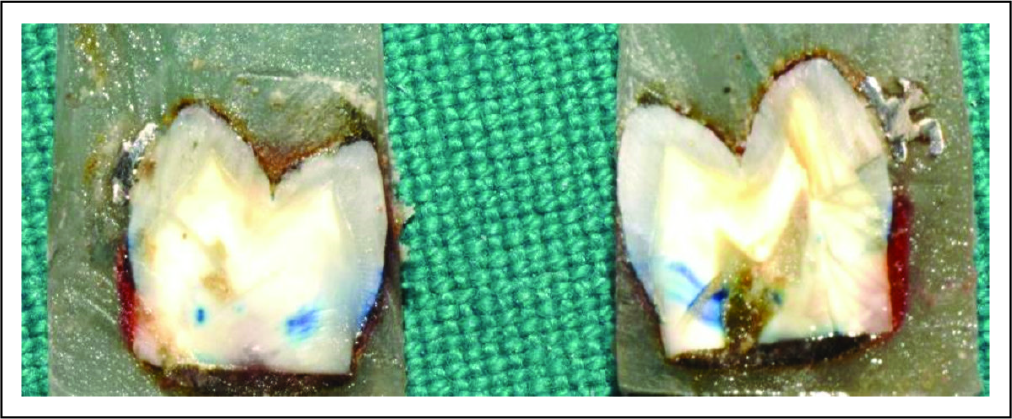
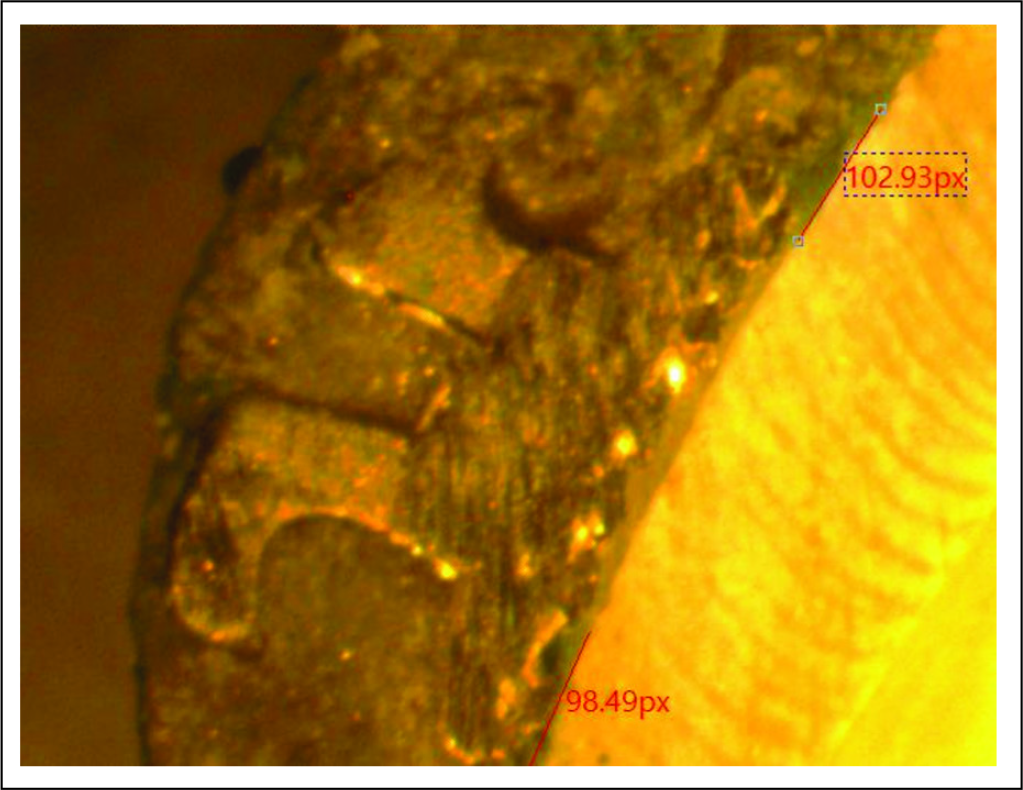
All the teeth were immersed in 2% methylene blue for 24 h. The teeth were then thoroughly cleaned and brushed around the brackets to remove any excess dye and stains. All the teeth were embedded in cold cure acrylic blocks taking care to keep the brackets' center in line with the long axis of the acrylic blocks. Teeth were sectioned longitudinally through the center of the bracket, using diamond cutting equipment, and cut surfaces were thoroughly polished (Figure 1). Microleakage was recorded using a stereomicroscope with MICAPS-microview software on the occlusal and gingival regions of the brackets at the tooth adhesive interface (Figure 2). Half of the samples were randomly selected and examined again by the same observer after 2 weeks to measure the intraobserver error of measurements.
Teeth Sectioned in a Buccolingulal Direction Through the Center of the Bracket.
Sample Showing Microleakage at the Occlusal and Gingival Border of the Bracket Base.
Statistical Analysis
Statistical analysis was performed using Kruskal–Wallis H tests to test the difference between the groups and Mann–Whitney U test to compare the differences between 2 independent groups. The level of statistical significance was set at P < .005. Intraobserver error was evaluated with the Kappa statistics.
Results
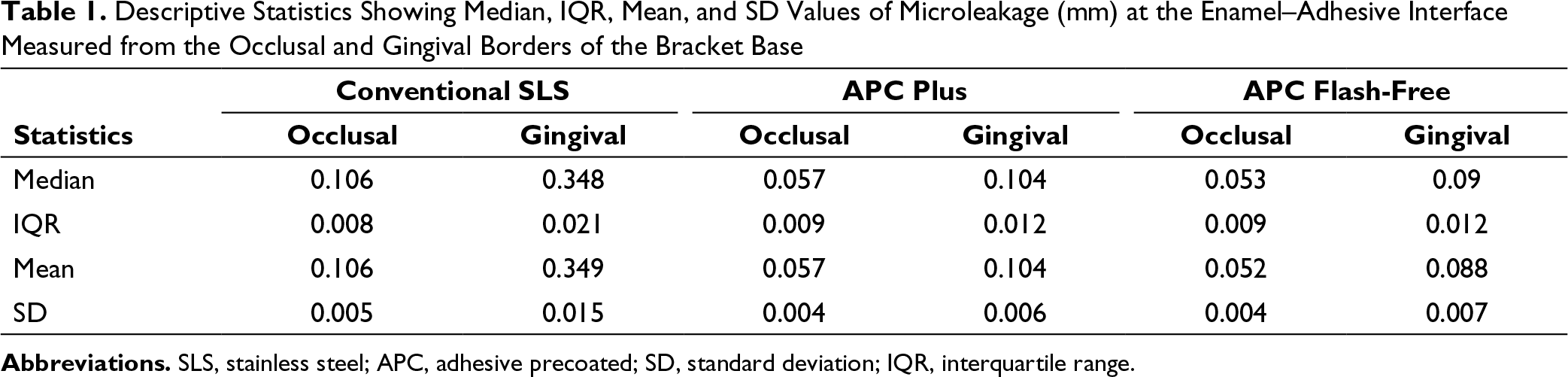
Descriptive Statistics Showing Median, IQR, Mean, and SD Values of Microleakage (mm) at the Enamel–Adhesive Interface Measured from the Occlusal and Gingival Borders of the Bracket Base
Inferential Statistics Showing Comparison of Microleakage Between Occlusal and Gingival Borders of the Bracket Base in 3 Different Experimental Groups
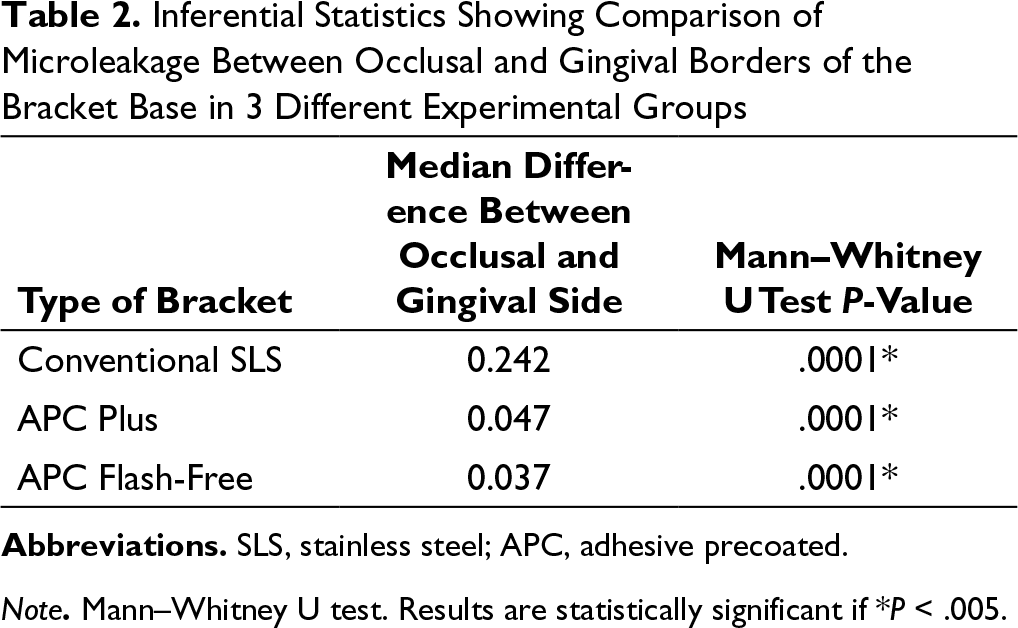
Note. Mann–Whitney U test. Results are statistically significant if *P < .005.
Depiction of Microleakage (mm) on Occlusal and Gingival Side of the Bracket in 3 Experimental Groups.
Comparison of Microleakage (mm) Among Conventional SLS, APC Plus, and APC Flash-Free in Occlusal and Gingival Borders of the Bracket Base Using Kruskal–Wallis H Test.
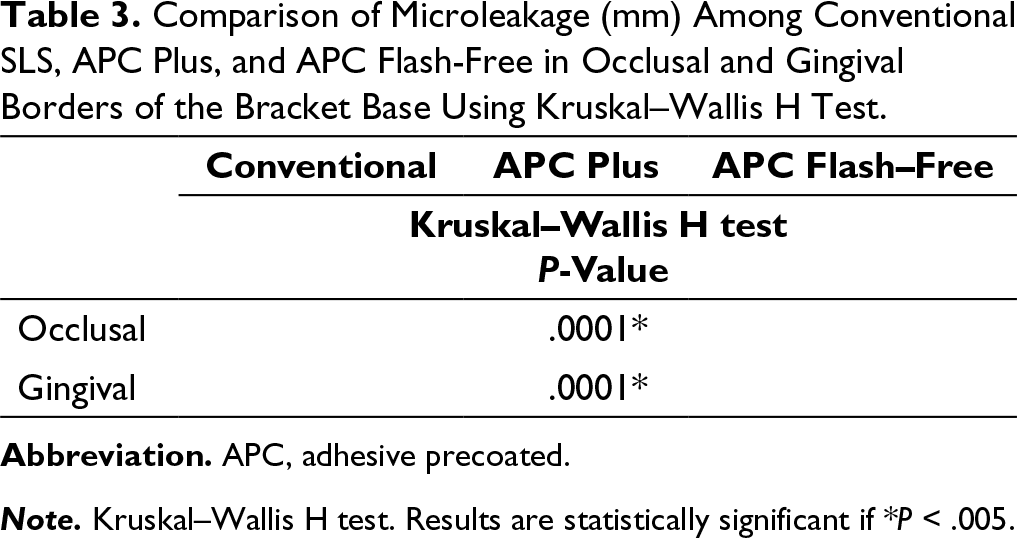
Note. Kruskal–Wallis H test. Results are statistically significant if *P < .005.
Intergroup Comparison of Microleakage (mm) Among Conventional SLS, APC Plus, and APC Flash-Free in Occlusal Side and Gingival Borders of the Bracket Base Using Mann–Whitney U Test.
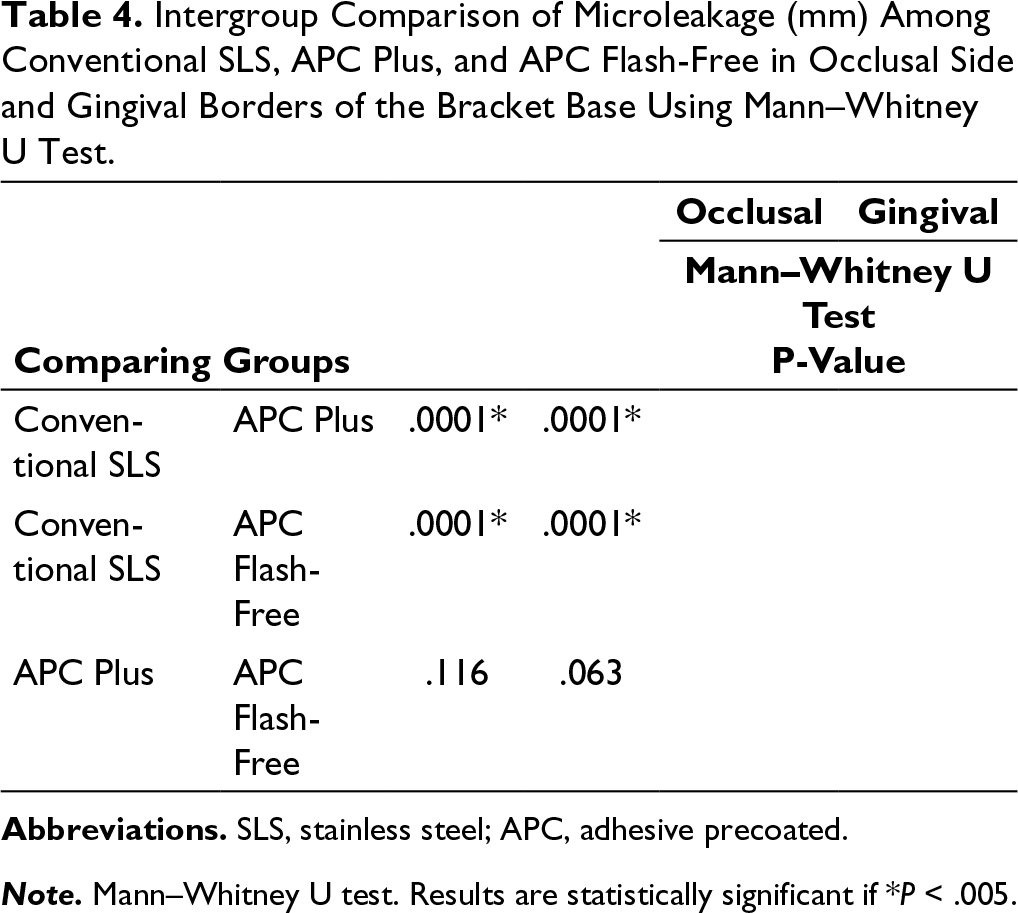
Note. Mann–Whitney U test. Results are statistically significant if *P < .005.
Discussion
Microleakage from an orthodontic point of view is the seeping and leaking of fluids and bacteria between the enamel–adhesive or adhesive–bracket interface. Polymerization shrinkage of the adhesive and differences in the rates of thermal expansion and contraction between the adhesive, bracket, and the enamel during exposure to hot and cold foods can cause gaps between the adhesive and enamel or between the adhesive and the bracket thus contributing to microleakage.
Microleakage presents the likelihood of formation of white spot lesions on the enamel at the adhesive–enamel interface and a reduction in the shear bond strength of the adhesive leading to bracket failure. It is reported that an average of 2 of the 3 teeth bonded with an orthodontic adhesive were affected by some form of enamel opacity after orthodontic treatment; the most common type identified as diffuse opacity. O'Reilly and Featherstone 12 and Øgaard 13 have shown that visible white lesions can develop within 4 weeks. Although microleakage-oriented caries is a well-documented entity in the restorative dentistry literature, the potential of caries adjacent to and beneath orthodontic brackets as a result of microleakage remains an underestimated threat to the permanent tooth, especially concerning long-term fixed appliance therapy. Several techniques have been introduced to assess microleakage around dental restorations. Microleakage is determined by a variety of in vitro techniques such as air pressure, fluid filtration, dye penetration, and microcomputed tomography14-16 and the most commonly used evaluation method is that of dye penetration.14, 17, 18 Researchers use colored dye agents or chemical tracers, which can penetrate and stain. The specimens are then sectioned longitudinally through the research area and assessed with stereo optical microscopy or scanning electron microscopy. To evaluate the relevance of a leakage test, the effective size of oral bacteria must be considered. Because of the range of bacteria sizes, dyes such as methylene blue and fuchsine are realistic agents to identify the presence of a clinically relevant gap.19, 20 2% methylene blue dye penetration was chosen for this study for the assessment of microleakage at the enamel–adhesive interface on the occlusal and gingival sides of the bracket. Thermal cycles were used in this study to mimic thermal changes in the mouth for the production of thermal stress at the tooth–adhesive interface.
The procedure of bonding orthodontic brackets at the enamel surface with composite resin consists a series of preparatory steps. New orthodontic materials are getting evolved in an effort to reduce the procedure time without reducing the bond strength of the bracket. APC brackets, a new generation bracket system introduced in 1992, had bracket bases prepasted with the optimal amount of adhesives. The APCP system provided better tolerance to humidity, has a fluoride-releasing adhesive, and the color change property of the adhesive helps to practitioner clean up the flash by providing a visual marker of adhesive placement. Excess flash is removed before curing an orthodontic bracket to avoid gingival irritation and plaque accumulation. Efforts aimed at reducing the excessive flash led to the development of APCF bracket systems. When APCF brackets are pressed on the enamel surface, the adhesive resin spreads out and conforms to the surface and creates a channeling border at the edges of the brackets, thus creating a seal to reduce microleakage.
This study evaluated and compared the microleakage scores at the enamel–adhesive interface on the occlusal and gingival side in conventional SLS, APCP, and APCF brackets. The mean of the microleakage scores both at the gingival and occlusal sides of the bracket was significantly lesser in APCP and APCF compared to conventional metal brackets. However, although the scores were higher on the gingival and occlusal sides of the bracket in APCP over APCF, the difference was insignificant.
The mean microleakage scores with metal brackets in the current study were in the ranges reported by Ulker et al 21 and James et al, 22 but were lesser than the mean values reported in the study by Abdelnaby and Al-Wakeel, 8 In the present study LED light was used to bond the metal brackets, while James et al in their study used halogen light, argon laser, and plasma arc curing light. The results of the present study support the results of Ulker et al 21 who concluded that the type of light-curing unit has an insignificant influence on the microleakage scores. Microleakage scores were measured at the gingival and occlusal sides of the bracket in the present study, while James et al in their study measured at the bracket margins after debonding the bracket. Abdelnaby and Al-Wakeel 8 measured microleakage at the underneath the bracket base after debonding.
Significantly lesser microleakage scores with APCP and APCF brackets are consistent with studies that show that the filler content of the adhesive has an inverse relation to the polymerization shrinkage. Decreased filler content causes greater polymerization shrinkage. 23 Transbond XT has approximately 3% lesser filler content than the APCP, and this could have contributed to lesser microleakage with APCP brackets. The APCF system has a nonwoven mat at the bracket base, saturated with resin adhesive. When pressed on the enamel surface, the transparent resin forms a channeling border at the edges of the brackets, thus sealing the bracket on the margins. The superior performance of APCF brackets over APCP brackets is consistent with the findings of Foersch et al, 24 which reports dye penetration in 35% of interfaces with APCF brackets relative to 97.5% of interfaces in APCP brackets. The results of the present study are consistent with the findings of Lee and Kanavakis 4 that proved the APCF system showed increased shear bond strength compared with the APCP system and shear bond strength is an absolute indicator of gaps and microleakage in the adhesive. However, microleakage scores with APCP metal brackets in the present study were significantly lesser than the values reported by James et al 22 in those brackets cured by argon laser and halogen light but were comparable to the values obtained with plasma arc curing.
Mean microleakage scores in all the 3 systems of stainless-steel brackets were higher at both occlusal and gingival side of the bracket than the scores with conventional, APCP, and APCF ceramic bracket systems reported in the previous studies.7, 25 A possible explanation for this finding is the “incomplete polymerization” phenomenon. In restorative dentistry, researchers have documented several factors that affect the depth of photoactivated cures, including duration and intensity of light exposure, filler type and shade of adhesive resin, and the reflective characteristics of the adhesive resin bulk.26-28 As light passes through the bulk of the restorative resin material, its intensity decreases greatly, thus decreasing the potential for cure. This decrease results in a gradation of the cure such that it decreases from the top surface inwards. 29 In orthodontics, brackets may act as the bulk of restorative material. Because metal brackets do not conduct light, the underlying adhesive resin may remain incompletely polymerized. Several studies have shown that ceramic brackets produce significantly stronger bond strength compared with conventional metal brackets.30-32 Increased bond strength with ceramic brackets resulted in bond failure at the enamel surface rather than at the bracket–adhesive interface, resulting in more enamel fractures after debonding23,32-34.This increased strength and difficulty in debonding for ceramic brackets may be attributed to the close adhesion of the ceramic bracket to the adhesive in the absence of microleakage. Similarly, the weaker bond strength of metal brackets may be attributed to relatively more microleakage between the bracket and the adhesive.
In the present study, microleakage was significantly greater on the gingival side than on the occlusal side. In the present study, the curing device was used from both sides for equal time duration. However, the difference in the microleakage scores could be explained by the fact that a greater surface curvature anatomy at the gingival side may result in a thicker adhesive at the gingival margin. The results of the present study are consistent with the previous studies9, 13, 35 which report increased microleakage at the gingival margin than on the occlusal margin.
In restorative dentistry, the shrinkage of the resin caused by the rapid curing with high-intensity lights has been considered a disadvantage because of the large amount of resin placed in the cavity. Fast curing may generate excess shrinkage by permitting little opportunity for the flow of cured resin; also, it may result in gap formation along the resin–tooth interface, which most likely increases the potential for microleakage. However, from an orthodontic perspective, this condition is different. Adhesives at the edges of the bracket can absorb some shrinkage, 9 and this shrinkage can pull the bracket closer to the enamel by the bracket's free floating. In contrast to the thick composite resin put in the prepared cavity in restorative dentistry, polymerization shrinkage and the subsequent microleakage is less of a concern in orthodontic adhesives because only a thin layer is used.
In the present study, APCP and APCF groups were cured with the LED light-curing unit, etched with 37% phosphoric acid, and microleakage was observed at enamel–adhesive interface only. However, the compatibility of APCP, APCF bracket systems with various curing methods such as plasma arc, argon laser, and halogen light curing and with various methods of enamel surface preparation such as self-etching primers, Er:YAG laser, and Er, Cr:YAG laser could significantly influence the level of microleakage between enamel–adhesive–bracket interface.
Future studies are recommended to test in vivo properties of the APC and APCF systems as well as the compatibility of the above systems to various curing and enamel preparation methods at both enamel–adhesive and adhesive–bracket surfaces.
Conclusion
Microleakage was observed in all the investigated groups.
The conventional SLS bracket group exhibited higher microleakage scores compared with APCP and APCF bracket systems at both occlusal and gingival sides.
Gingival sides in all groups exhibited higher microleakage scores compared with those observed in occlusal sides for the enamel–adhesive interface.
APCP and APCF bracket systems do not have a significant difference in the microleakage levels at the enamel–adhesive interface.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.