
Abstract
Introduction:
Patients undergoing orthodontic therapy face greater difficulties in maintaining good oral hygiene. To improve mechanical plaque removal, a common strategy is to incorporate a chemotherapeutic agent. Thus, the effects of adding essential oil mouthwash to a standard oral hygiene regimen to maintain oral health were evaluated.
Material and Method:
Two groups were created with 25 patients each. Gingival index and orthodontic plaque index were calculated as initial reading. Gingival index and orthodontic plaque index were calculated again after 6 months.
Result:
In the control group, the mean score of gingival index and orthodontic plaque index were significantly increased from baseline reading (T1) to after 6 months reading (T2). In the experimental group, increase in the mean score of gingival index and orthodontic plaque index was not statistically significant.
Conclusion:
When an essential oil mouthwash is added to the daily oral hygiene regimen (conventional manual toothbrushing + brushing with monotufted brush), it maintained the gingival health and amount of plaque accumulation in orthodontic patients over a period of 6 months.
Introduction
A well accepted rationale for orthodontic treatment is to prolong the life of individual’s dentition. 1 Orthodontic treatment may provide patients with an improved esthetic facial appearance and a well-functioning occlusion. 2 Orthodontic treatment can be a caries-preventive measure in itself. 3
Health of periodontium should be maintained during active orthodontic treatment as the efficiency of orthodontic treatment depends upon the response of periodontal tissues to orthodontic intervention. 4 Patients undergoing orthodontic therapy face greater difficulties in maintaining good oral hygiene. Orthodontic bands, brackets, and archwires are barriers for brush bristles and floss, leading to greater accumulations of plaque which subsequently causes gingival inflammation, bleeding, and gingival enlargement. 5
During orthodontic treatment, when oral hygiene is poor, development of white spot lesions is almost inevitable. 6 Demineralization is more commonly seen on the buccal surfaces of orthodontically treated teeth than on untreated teeth as prolonged plaque retention around the brackets causes decrease in pH when certain bacteria interact with sugars,7, 8 and the presence of such white spot lesions may lead to patient dissatisfaction which necessitates cosmetic intervention. 9
Mechanical method which involves tooth brushing is the most widely used and accepted method of plaque control. 10 Interdental cleansers (dental floss, interdental brushes, toothpicks) and oral irrigation devices are also used, but much less commonly. Mechanical cleansing procedures are efficient; however, according to several studies, maintaining satisfactory standards of oral hygiene for a longer period of time with these methods is laborious. 11
Also mechanical tooth cleaning is a skill that many people are unable to perfect. 12 Many orthodontic patients, especially children and adolescents, find flossing a time-consuming and tedious procedure with orthodontic archwires in place. 13
Dong-Won Lee 14 has shown effectiveness of monotufted brushes over normal flat trimmed brushes. To improve mechanical plaque removal, a common strategy is to incorporate a chemotherapeutic agent, such as an antibacterial mouthrinse. 15 Chlorhexidine is the most effective agent for the chemical control of dental biofilm but it is not recommended for long-term use due to its numerous adverse effects. 16 Alternative chemical agents with no side effects such as antiseptics containing essential oils have been widely studied and have been found to exhibit satisfactory results in the control of dental biofilm. Mouthwashes containing four phenol-related essential oils (thymol, eucalyptol, menthol, and methyl salicylate) claim to penetrate the plaque biofilm and thus kill micro-organisms that cause gingivitis.17-19 Little is known about the effect of addition of an essential oil mouthwash to standard oral hygiene regimen in orthodontic patients. Therefore, purpose of this study is to determine whether the use of an essential oil mouthwash in addition to standard oral hygiene regimen (conventional toothbrushing + brushing with monotufted brush) has an added benefit for orthodontic patients in maintaining proper oral health.
Materials and Method
Ethical approval from relevant committee was obtained. Study included 50 patients who were undergoing orthodontic treatment at Department Of Orthodontics and Dentofacial Orthopaedics of our college. Sample size was selected based on the following formula where S is pooled standard deviation, M1 is experimental group and M2 is control group. Z1 is value associated with alpha which is 1.64 and Z2 is associated with beta which is 0.84.
Inclusion Criteria
Patients having Angle’s class I malocclusion with mild or no crowding.
Patients within first 6 months of treatment were selected in study with initial reading (T1) recorded on round NiTi wire and final reading (T2) recorded on a rectangular stainless steel wire.
In all 50 patients, banding were done on first permanent molars and bonding done on premolar, canine, and incisors with metal brackets of 3 M Gemini series having 0.022 slot.
Patients in which stainless steels ligation system was used.
Patients without a clinically significant medical or dental history.
Patients who agreed to participate signed a consent form before the study. Approval from the institutional ethical committee was obtained before the study began.
Study population had the mean age of 15 years (range = 12-28 years).
The patients were divided into two groups with 25 patients each. The control group included conventional manual toothbrushing with Oral-B toothbrush + brushing with monotufted brushhead + rinsing with placebo mouthwash.
The experimental group included conventional manual toothbrushing with Oral-B toothbrush + brushing with monotufted brushhead + rinsing with essential oil mouthwash (Listerine).
At the beginning of the study, each participant received an initial prophylaxis by same dental surgeon. At this time, baseline readings (T1) were recorded for the gingival index (GI) and orthodontic plaque index (OPI). The examiner who performed the measurements was blinded to the group assignments.
Both the groups had equal number of males and females distribution which was 14 females and 11 males. To minimize potential bias, group assignments were made by chits system. Chits were selected by a person otherwise not involved in the study.
Now subjects in the control group were instructed to perform conventional manual toothbrushing and use monotufted brushhead twice daily. In addition, they were asked to rinse vigorously for 30 seconds twice daily with 20 ml of placebo mouthwash. Placebo mouthwash were prepared by adding synthetic food color (Three Leaves, Garden House, Navi Mumbai, India) to distilled water.
Subjects in the experimental group were asked to rinse vigorously for 30 seconds twice daily with 20 ml of an essential oil mouthwash (Listerine) in addition to their basic oral hygiene regimen (conventional manual toothbrushing + brushing with monotufted brushhead).
All patients were advised Bass method for brushing. For monotufted brushhead, patients were instructed to use monotufted brush at interbracket area and between tooth and archwire with back and forth short stroke movement and light pressure. Every patient was asked to demonstrate the Bass method of brushing and monotufted brushhead as instructed on a typhodont on each visit.
All patients were provided with an Oral-B soft textured toothbrush (Rialto enterprises, Tamil Nadu, India), monotufted brushhead (TePe, Sweden), and Colgate toothpaste (Colgate-Palmolive, India). Placebo mouthwash and Listerine mouthwash (Johnson and Johnson, Bangalore, India) was provided in plane unlabeled plastic bottles of the same sizes and shapes. Subjects in both the groups were provided with a measuring beaker. All of the subjects were monitored for compliance by having them bring empty bottles from the previous visit.
GI and OPI were performed again at 6 months interval (T2) and no oral prophylaxis was performed during this time.
GI was scored according to Loe H. 20
Each of the four gingival areas of the tooth is given a score from 0 to 3, this is the GI for the area. Four areas of the tooth are scored which are added and divided by four to give the GI for the tooth. Finally, by adding the indices for the teeth and dividing by the total number of teeth examined, the GI for the individual is obtained.
Subjects with mild inflammation usually score from 0.1 to 1.0, those with moderate inflammation score from 1.1 to 2.0, and scores between 2.1 to 3.0 signify severe inflammation.
OPI was scored according to Heintze SD, Jost-Brinkmann PG, and Finke C. 21 Presence of plaque was assessed using a disclosing agent (Plaksee, 2% erythrosine solution; ICPA, Ankleshwar, India) in three sites of buccal surfaces of all teeth except first, second, and third molars. Erythrosine solution was applied to buccal tooth surface with cotton swab and the subjects rinsed thoroughly with water. Then the presence of dyed plaque is evaluated with the YES-NO system in 3 sites of the buccal surface of a tooth.
Each area has its own level of difficulty depending on the accessibility for cleaning. So points were given accordingly.
Cases with plaque mesial or distal to bracket = 3 points
Cervical to bracket = 2 points and
Coronal to bracket = 1 point.
Total score is computed using the following formula,
Sum of values from dyed areas

Condition of oral hygiene is evaluated according to the following scheme,
0%-30% = Good,
31%-50% = Fair,
51%-100% = Poor.
Statistical Analysis
Statistical analysis was performed by using a commercially available software program SPSS version 20.
To determine whether there is a difference in gingival health and in plaque accumulation in both the groups, the calculated mean at baseline observations were compared with the observations obtained after 6 months using paired t test at 24 degree of freedom and 95% confidence level separately for control group and experimental group.
To evaluate the effectiveness of an essential oil mouthwash in maintaining proper oral health in orthodontic patients, unpaired t test was applied at 48 degree of freedom and 95% confidence level separately for GI and OPI at the initial stage and readings obtained after 6 months. (Level of confidence was set at 95%, keeping α error at 5% and beta error at 20% which gives a power of 80% to the study).
Significance for statistical tests was predetermined atP ˂ .05. For all the tests, P value was considered for statistical significance.
Result
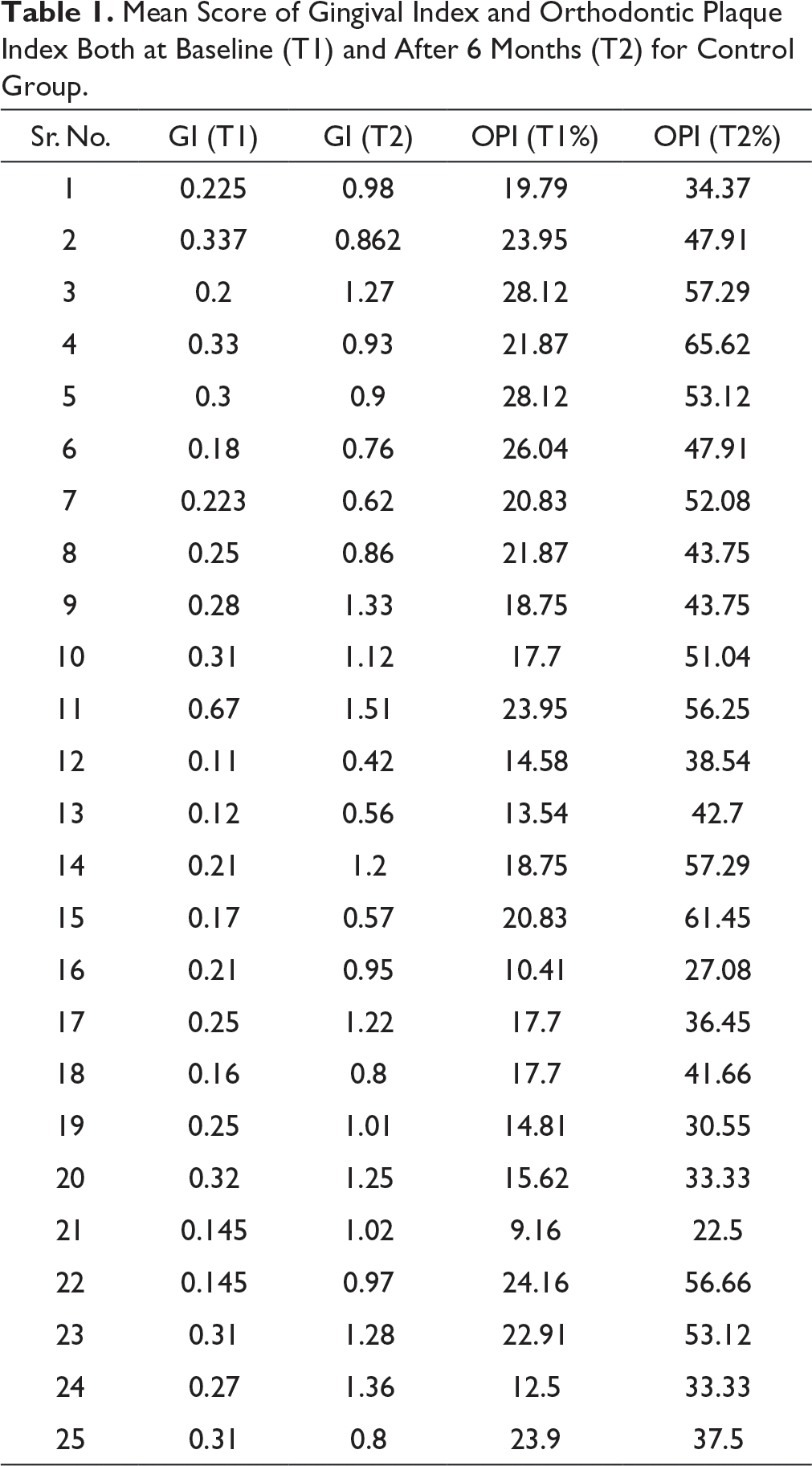
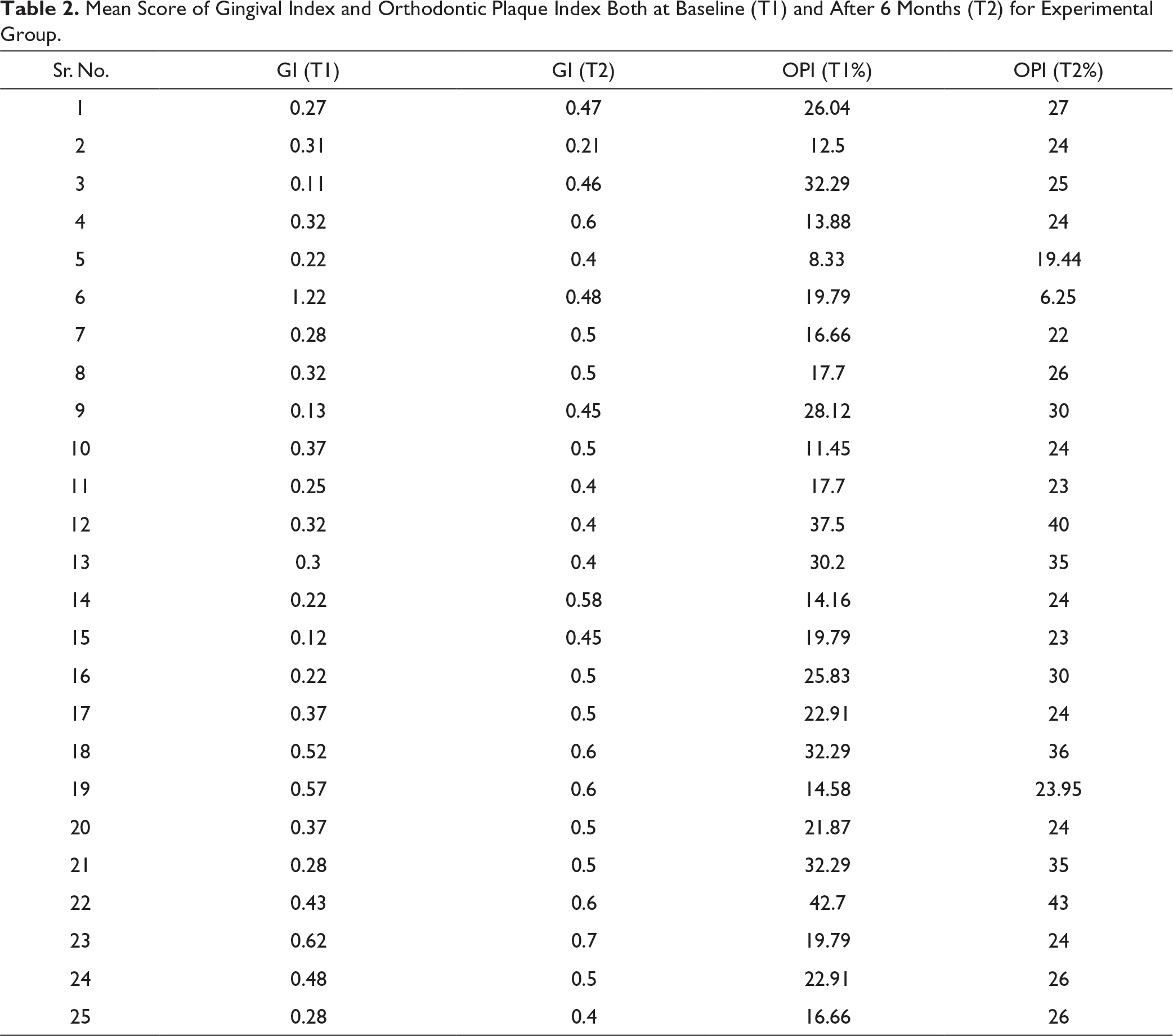
Values obtained for GI and OPI both at baseline (T1) and after 6 months (T2) for the control group and experimental group are shown in Tables 1 and 2, respectively.
Mean Score of Gingival Index and Orthodontic Plaque Index Both at Baseline (T1) and After 6 Months (T2) for Control Group.
Mean Score of Gingival Index and Orthodontic Plaque Index Both at Baseline (T1) and After 6 Months (T2) for Experimental Group.
In the control group, the mean score of GI at baseline was 0.2514 and after 6 months it was 0.9821. A paired t test was carried out to determine whether there is any difference in gingival health at T1 observations and at T2 (Table 3). Test statistic P value was .000 (P < .05), this showed that, there was significant increase in the mean score of GI from T1 to T2.
Comparison of Gingival Index Mean of the Control Group at Baseline (T1) and After 6 Months (T2) Using Paired t Test.

In the experimental group, the mean score of GI at T1 was 0.356 and at T2 was 0.4228 (Table 4). Test statistic P value was .160 (P > .05), this showed that the mean score of GI increased from T1 to T2 but it was not statistically significant.
Comparison of Gingival Index Mean of the Experimental Group at Baseline (T1) and After 6 Months (T2) Using Paired t Test.

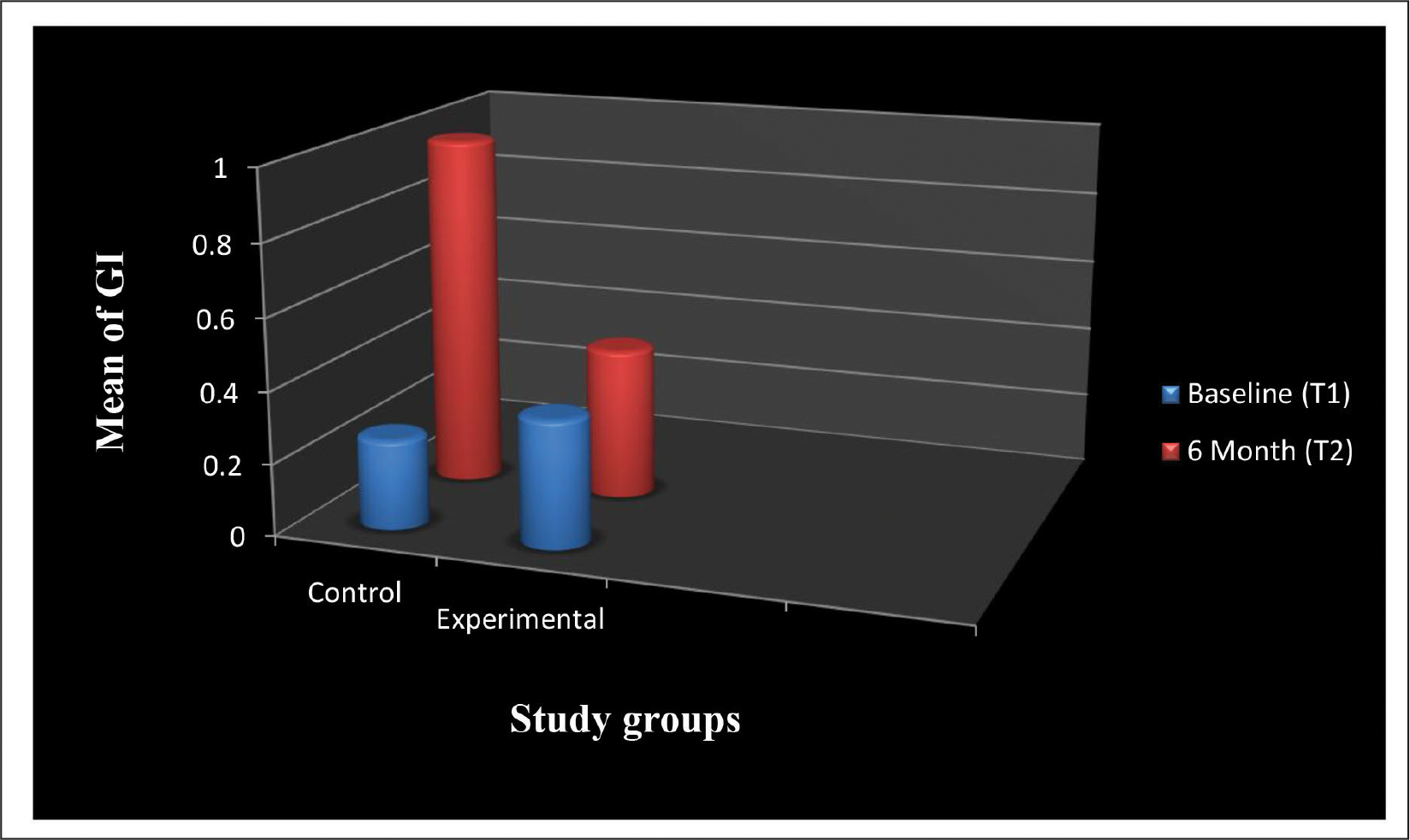
Figure 1 shows the treatment response for GI of both the control group and experimental group.
Treatment Response for Gingival Index (GI) of Both the Control Group and Experimental Group.
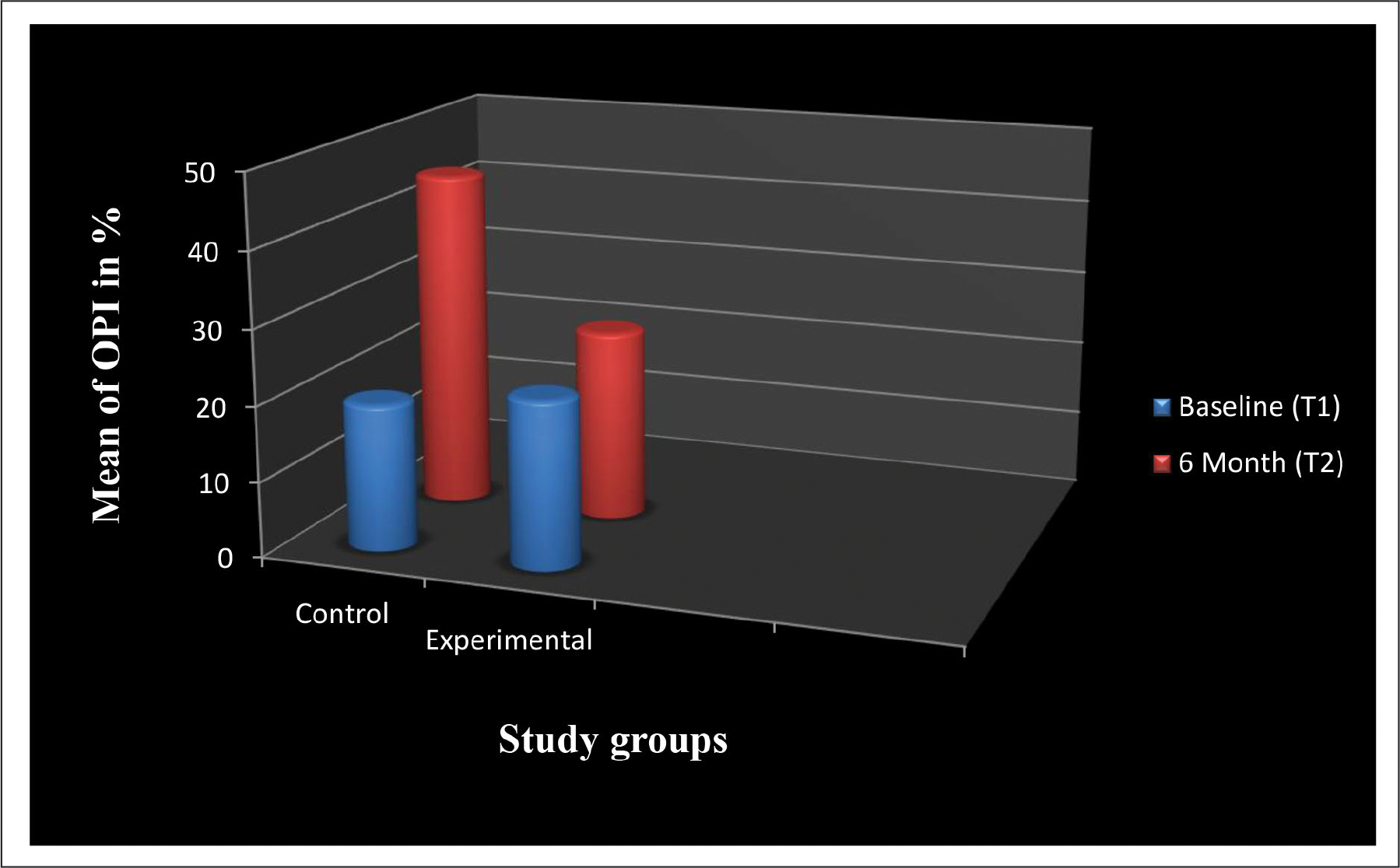
In the control group, the mean score of OPI at T1 was 19.5024 and at T2 was 45.01. A paired t test was carried out to determine whether there is any difference in plaque accumulation at baseline observations and after 6 months (Table 5). Test statistic P value was .000 (P < .05), this showed that there was a significant increase in the mean score of OPI from T1 to T2.
Comparison of Orthodontic Plaque Index mean of Control Group at Baseline (T1) and After 6 Months (T2) Using Paired t Test.

In the experimental group, the mean score of OPI at T1 was 22.3176 and at T2 was 25.5056 (Table 6). Test statistic P value was .089 (P > .05), this showed that the mean score of OPI increased from T1 to T2 but this increase was not statistically significant.
Comparison of Orthodontic Plaque Index Mean of Experimental Group at Baseline (T1) and After 6 Months (T2) Using Paired t Test.

Figure 2 shows the treatment response for OPI of both the control group and experimental group.
Treatment Response for Orthodontic Plaque Index (OPI) of Both the Control Group and Experimental Group.
From results, it can be seen that within group comparison shows statistically significant increase in the mean score of both the indices from T1 to T2 for the control group, and in the experimental group, there was an increase in the mean score of both the indices but this increase was not statistically significant.
Mean score for GI at T1 for the control group was 0.2514 and for the experimental group was 0.356. Results of unpaired t test (Table 7) showed that test statistic P value was .052 (P > .05), this showed that the mean score for GI of both the control and experimental group at baseline did not show any significant difference.
Comparison of Baseline Mean (T1) of Gingival Index (GI) Between the Control Group and an Experimental Group Using Unpaired t Test.

Mean score for GI after 6 months for the control group was 0.9821 and for the experimental group was 0.488. Test statistic P value (Table 8) was .000 (P ˂ .05), which showed mean score for GI of the control group was more than the experimental group at T2 and this difference was statistically significant.
Comparison of After 6 Months Mean (T2) of Gingival Index (GI) Between the Control Group and an Experimental Group Using Unpaired t Test.

Mean score for OPI at T1 for the control group was 11.5024 and for the experimental group was 22.3176. Test statistic P value (Table 9) was 0.170 (P > .05), which showed mean score for OPI of both the control and experimental group at T1 did not show significant difference.
Comparison of Baseline Mean (T1) of Orthodontic Plaque Index (OPI) Between the Control Group and an Experimental Group Using Unpaired t Test.

Mean score for OPI at T2 for the control group was 45.01 and for the experimental group was 26.5856. Test statistic P value (Table 10) was .000 (P ˂ .05), which showed the mean score for OPI of the control group was more than the experimental group at T2 and this difference was statistically significant.
Comparison of After 6 Months Mean (T2) of Orthodontic Plaque Index (OPI) Between the Control Group and an Experimental Group Using Unpaired t Test.

From the result, it can be seen that baseline measurements for both the parameters, GI and OPI were not significantly different for the control group and experimental group.
After 6 months, subjects in the experimental group had statistically significantly lower mean GI and OPI scores than subjects in the control group.
Discussion
In assessing the role of gender for compliance in maintaining oral hygiene in orthodontic patients, previous studies22, 23 demonstrated that females are generally better compliers than males. However, other studies24, 25 have shown that it has moderate or no effect on patient compliance. This study has equal distribution of males and females in each group thus eliminating any bias in results regarding compliance.
Study population had the mean age of 15 years; although some studies suggested that young patients were more compliant than older ones, others found no correlation with age.25, 26
As the placement of bands is associated with change in the bacterial composition of plaque,27, 28 criteria of banding on the permanent first molars and bonding on premolars, canines, and incisors were kept constant to eliminate discrepancy in the results. In this study, patients with Angles class I malocclusion with mild or no crowding were selected so the wire sequence was kept constant, that is, the first two months round NiTi, next two months rectangular NiTi, and last two months rectangular S.S., to eliminate discrepancy in results.
Each participant received an initial prophylaxis at the beginning; the purpose of this prophylaxis was to have almost the same baseline readings for both the groups. At this time, baseline readings were recorded for the OPI and GI. OPI is an internationally accepted scoring system. 21 OPI enables an estimation of the patient’s need for prophylaxis, so that appropriate preventive measures can be taken. 29
The same dental hygiene products are provided for both the control and experimental groups and patients were asked to use only these products.
Previously the roll method was the one method most often advocated for brushing in orthodontic patients. 30 However, on the basis of available evidence, it seems justifiable to recommend horizontal brushing with the Bass technique as the method of choice for patients wearing orthodontic appliances. 2 Many previous studies2, 31, 32 concluded that a single tufted interspace brush (monotufted brush) may be used as an adjunct to the ordinary toothbrush in patients wearing orthodontic appliances. In this study floss was not included as many orthodontic patients fail to floss as they find this procedure difficult, complicated, and long in presence of orthodontic archwires. 13
Results of this study showed that the mean scores for GI and OPI at the baseline of both the control and experimental group do not show any significant difference (P > .05), thus achieving the objective of initial prophylaxis.
Within group comparison shows a significant increase in the mean score of both the indices from the baseline to after 6 months for the control group, and in the experimental group, there was increase in the mean score of both the indices but this increase was not statistically significant.
After 6 months, subjects in the experimental group had statistically significant lower mean GI and mean OPI scores than subjects in the control group. This suggests that the oral hygiene status of the patients of the control group had worsened during the period of study. In contrast to this, the oral hygiene status was maintained in the patients of the experimental group.
Results of this study are in agreement with the study conducted by Tufekci E et al. 9 They concluded that the use of Listerine mouthrinse can reduce the amount of plaque and gingivitis in patients undergoing orthodontic treatment.
Also, a systematic review by JE Stoeken, S Paraskevas, and GA van der Weijden, 33 and Fahad Ali Alshehri 34 supports the benefit of adding an essential oil containing mouthwash Listerine to the daily oral regimen to maintain personal oral hygiene.
The lower mean scores in GI and OPI measurements in the experimental group after 6 months may also have been attributable to the mechanical effect of rinsing alone. However, results from the previous studies conducted in nonorthodontic subjects suggest that the reduction in GI and OPI scores in essential oil mouthwash groups is due to bactericidal efficacy rather than any mechanical effect 35 ; thus, results of these studies were in agreement with this studies.
The results of this study demonstrated that the use of an essential oil mouthwash (Listerine) containing eucalyptol 0.092%, menthol 0.042%, methyl salicylate 0.060%, and thymol 0.064% as active ingredients in the experimental group provided significant reductions in the amount of plaque and gingivitis present when compared with the control group. Also, use of Listerine in addition to the standard oral hygiene regimen (conventional manual toothbrushing + monotufted brush) was found to be beneficial for orthodontic patients in maintaining proper oral health.
Limitations of the Study
The techniques used in this study require superior manual dexterity which may be difficult for young patients to perform.
Our study results cannot be generalized as the sample size is small. So in the coming future RCT with larger sample size should be conducted.
Average orthodontic treatment is carried out for more than a year. However, the study evaluated the effect of essential oil mouthwash only for a period of 6 months.
Conclusion
When an essential oil mouthwash is added to the daily oral hygiene regimen (conventional manual toothbrushing + brushing with monotufted brush), it maintained the gingival health in orthodontic patients over a period of 6 months.
When an essential oil mouthwash is added to the daily oral hygiene regimen (conventional manual toothbrushing + brushing with monotufted brush), it maintained the amount of plaque accumulation in orthodontic patients over a period of 6 months.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances and informed consent was received and obtained respectively before initiating the study from all participants.