
Abstract
This case was submitted to the board under Category I for the Indian Board of Orthodontics examination. This communication describes the management of a female patient who presented with severe crowding in both upper and lower arches. Comprehensive fixed orthodontic mechanotherapy including extractions of all first premolars was carried out. Stable harmonious occlusion was achieved on long-term follow-up.
Introduction
A female patient aged 12 years reported with a chief complaint of irregularly placed upper and lower front teeth. On corroborating clinical findings and diagnostic records, it was observed that she was skeletally and dentally class I with severe crowding of 10 mm in the upper arch and 8 mm in the lower arch. She also had incompetent lips, non-consonant smile, and 12, 22 in crossbite. Comprehensive fixed orthodontic mechanotherapy including extractions of all first premolars was carried out. Active treatment over a period of 18 months resulted in a 100% improvement of the peer assessment rating index. Results were stable both esthetically and functionally over a follow-up of 2 years.
Diagnosis and Etiology
KD, a 12-year-old female reported to the dental center with the chief complaint of irregularly placed upper and lower front teeth. Her medical and dental history was nil relevant. On facial examination, the patient had acceptable facial symmetry with face proportional in horizontal thirds and vertical fifths. She had a convex profile and normal growth pattern. Her lips were incompetent. She had non-consonant smile and normal nasolabial angle. In TMJ (Temporomandibular Joint), there were no joint sounds on palpation and mouth opening was normal with no deviations.
On intraoral examination, her oral hygiene was good, 46 was carious, all third molars were unerupted, and lower second molars were partially erupted. Both of her arches were symmetrical; the upper arch was ovoid shaped, whereas the lower was U shaped. Crowding in the upper and lower arches was 10 mm and 8 mm, respectively. Incisor as well as molar relation was class I, whereas canine relation was class II bilaterally. Overjet and overbite were 1 mm and 0.5 mm, respectively. Both upper and lower midlines were centered. 12, 22 were in crossbite. Displacements up to 9 mm were present in the upper anterior segment, whereas the lower anterior segment demonstrated displacements up to 3 mm (Figures 1 and 2).
Pre-treatment Facial and Intraoral Photographs.

Initial Dental Casts.

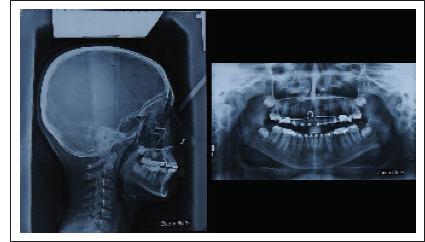
OPG (Orthopantomagram) revealed no obvious bony pathology, normal TMJ, all third molars in varying stages of development, and partially erupted mandibular second molars. None of the tooth had poor prognosis.
Lateral cephalogram revealed class I skeletal A to P relationship (ANB (Angle formed by the intersection of Nasion - Point A and Nasion - Point B)—2° and Wits appraisal—0 mm) and mild vertical growth pattern (SN-GoGn angle—36°, FMA (Angle formed between Palatal Plane and Mandibular Plane)—27°, and Bjork—400°). Upper and lower incisors were proclined (U1 to NA—29°/6 mm, L1 to NB—36°/7 mm, and IMPA—105°) resulting in reduced interincisal angle (113°). Overbite was reduced to 0.5 mm. Nasolabial angle (100°) was normal. In relation to the Ricketts E-Line, the lower lip was forwardly placed. The primary problem was tooth size–arch perimeter discrepancy (Figure 3).
Diagnostic Summary
KD, a 12-year-old female, presented with incompetent lips, non-consonant smile, convex profile, carious 46, crowding of 10 mm and 8 mm in the upper and lower arches, respectively, displacements in upper and lower anterior segments, 12, 22 in crossbite, class II canine relationship bilaterally, proclined upper and lower incisors, reduced overbite, and skeletal class I with vertical growth pattern.
Aims and Objectives of Treatment
In the present case, our main objectives were to (a) achieve lip competency, (b) improve smile esthetics, (c) restore 46, (d) correct axial inclination of upper and lower incisors, (e) level and align the arches, (f) maintain molar relationship, (g) correct canine relationship, (h) optimize overbite, and (i) retain corrected results.
Treatment Plan
A comprehensive analysis of the face, dental casts, and the cephalogram were the determining factors for conducting comprehensive fixed orthodontic mechanotherapy including extractions of all first premolars in this patient.
The long-term stability of treatment changes was dependent on effective decrowding, derotation, proper torquing, good interdigitation, and maintenance of general arch form. The skeletal basal relationship was favorable for harmonious growth of maxillomandibular complex. To maximize stability, a wrap-around retainer in the upper arch and a bonded retainer in the lower arch were considered appropriate.
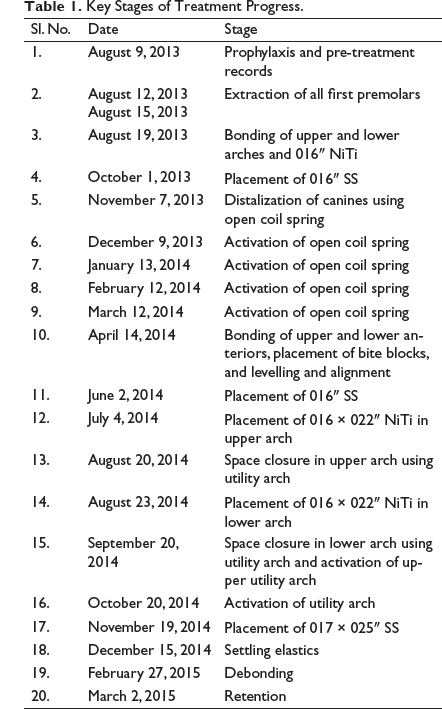
Treatment Progress
The initial treatment plan involved prophylaxis and restoration of 46. The upper and lower tooth axes were improved by a fixed pre-adjusted edgewise appliance with 0.018 × 0.028″ slot in Roth prescription brackets in both arches. Anchorage reinforcement was done by Nance button and bonding of second molars in upper and lingual arch in lower. Since patient had vertical growth pattern, bonding of second molars was done occlusally to avoid their extrusion. In both the arches, initial levelling and alignment was carried out by 0.016″ NiTi wire. Decrowding was done by open coil spring from canine to canine on 0.016″ stainless steel wire in both the arches (Figure 4). Residual space closure was done using intrusion retraction utility arch (Figure 5). Finally, the patient was put on settling elastics (Triangular elastics 3/16″, 3.5oz U3, U5s↓L5s). The treatment took approximately 18 months. Following debonding, the maxillary arch was given a removable wrap-around retainer, and the lower arch was given a bonded canine-to-canine lingual retainer. The patient was placed in a retention control program with periodic visits. Key stages of treatment progress are depicted vide Table 1.
Initial Lateral Cephalometric Radiograph and Panoramic Radiograph.
Decrowding of Upper and Lower Arches.

Closure of Residual Spaces by Intrusion Retraction Utility Arch.

Key Stages of Treatment Progress.
Treatment Results
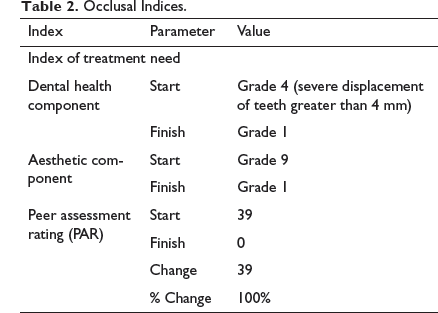
The posttreatment photographs and models confirmed good esthetic results and dental relationships. The dental and the facial midlines were coincident with each other. The posttreatment intraoral photographs showed good interdigitation of the lateral segments, overjet, and overbite of 2.5 mm. Following treatment, no premature occlusal contacts during mandibular movements were present. Class I incisor relationship and bilateral class I molar and canine relationship were achieved (Figures 6 and 7; Table 2). Complications encountered during the course of treatment were nil.
Posttreatment Facial and Intraoral Photographs.

Final Dental Casts.

Occlusal Indices.
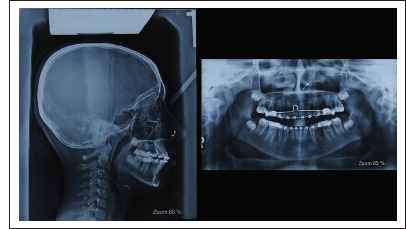
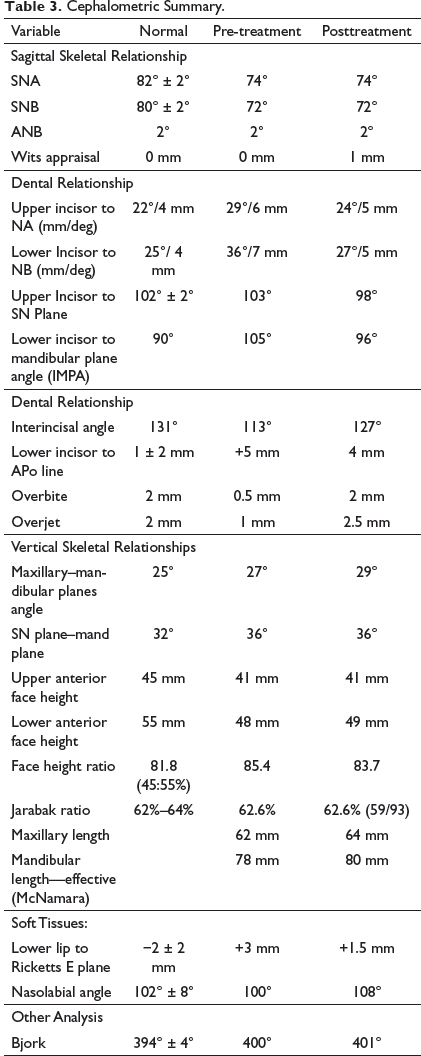
Posttreatment OPG revealed root parallelism, third molars in varying stages of eruption, no obvious bony pathology, and normal TMJ. Cephalometric tracings and superimpositions confirmed minimal anteroposterior (ANB—2° and Wits appraisal—1 mm) and vertical change (SN Plane–Mand plane angle—36° and Jarabak Ratio—62.6%). FMA increased by 2° when compared to pre-treatment measurements, which may be due to ongoing growth and vertical growth pattern. The inclination of upper and lower incisors improved with the treatment (U1-NA—24°/5 mm, L1-NB—27°/5 mm and IMPA—96°) which, in turn, resulted in the improvement of interincisal angle (127°). Overbite and overjet got optimized to 2 mm and 2.5 mm, respectively. The balance of soft tissues improved considerably. The relationship of the lower lip to Ricketts E-line improved to +1.5 mm (Figures 8 and 9). Cephalometric summary is depicted vide Table 3.
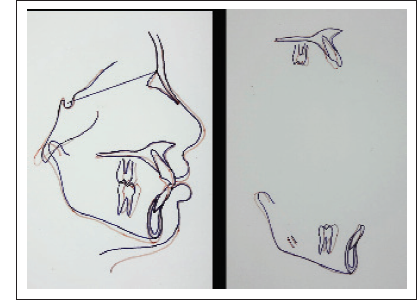
Final Lateral Cephalometric Radiograph, Panoramic Radiograph.
Superimposition.
Cephalometric Summary.
Critical Appraisal
KD was successfully treated over a period of 18 months. The patient’s chief complaint was adequately addressed, and objectives of the treatment were achieved. The patient was highly satisfied with the treatment outcome. Results were stable both esthetically and functionally over a follow-up of 2 years (Figure 10).
24 Months Follow-Up Facial and Intraoral Photographs.

Skeletal
There is minimal A to P change which is evident from maintenance of ANB angle at 2° and a slight change in Wits appraisal from 0 mm to 1 mm. All the parameters depicting vertical component of the skeletal relation showed no change except FMA, which increased by 2°. This slight vertical increase may be due to ongoing growth and vertical growth pattern.
Dental
Upper and lower incisors demonstrate marked improvement in inclination. Though there was good intercuspation in the buccal segment, the vertical settling of 24 should have been better. Marginal ridge relation of 34 to 36 and 44 to 46 should have been better. Radiographically, root parallelism was achieved but root uprighting was required in 32 and 42.
Soft Tissue
The patient had a well-balanced face post treatment with marked improvement in lip competency. Smile of the patient became consonant.
Iatrogenic
On clinical examination, there were no areas of decalcification on any tooth surface. Radiographically, there was no root resorption observed.
Statement of Informed Consent
Written informed consent was obtained from the subject for the use of photographs for publication.