
Abstract
Facial esthetic has always been a concern for humans for ages. The anteroposterior (AP) position of central incisors plays a key role in building facial esthetic in a smiling profile view. There have been various cephalometric, profilometric, and photographic methods used in the past to assess and predict the AP position of maxillary incisors in their optimal esthetic position. Our new device will help to predict, assess, and measure the optimal AP position of maxillary central incisors clinically using the glabella as a landmark.
Introduction
The anteroposterior (AP) position of the maxillary incisors has been observed to affect the soft tissue profile and can be manipulated by orthodontic and/or surgical treatment. Each AP millimetric change in the maxillary incisor position has a direct impact on oral and facial harmony and esthetic judgment in both frontal and profile views. 1
Ajmera et al 2 found that the forehead can be used as a useful landmark for assessing AP maxillary central incisor position with the help of a smiling profile photograph in the adult Maharashtra female population. According to Andrews, the maxillary incisor position is optimally positioned when the facial axis (FA) point—a clinical midpoint of the labial surface of maxillary central incisors—contacts the goal anterior-limit line (GALL), a parallel line to the frontal plane of the head passing through a line between the forehead’s anterior-limit line (FALL) and the glabellar vertical line (GVL) (Figure 1). 3
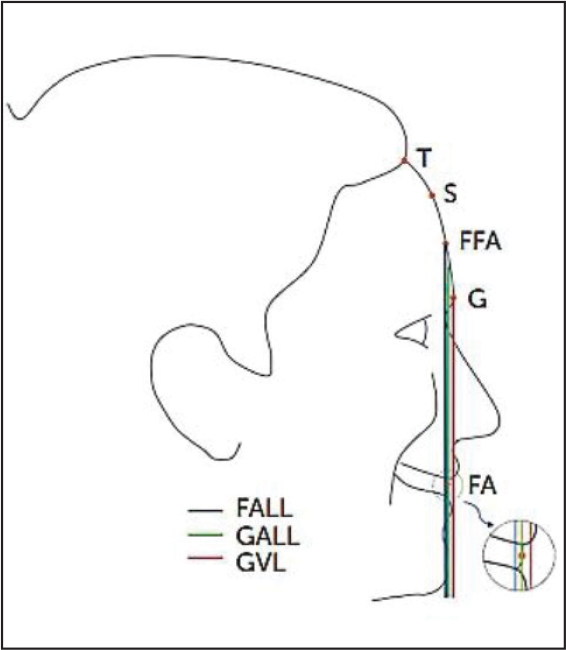
Source: Carruitero et al. 3
Recently, a study showed that the Glabella Vertical (GV) corresponded with GALL in most Caucasian patients. They found that in 95% of the population, GALL is within 1 mm of GV and 1.5 mm of GV in 99.7% of the population. They concluded GV as a new reliable frontal plane and boundary for the anterior maxillary incisor AP position. 1
The present article describes an innovative device, that is, P-device, which can assess and measure the central incisors’ position with respect to glabella in an AP dimension clinically.
Source:
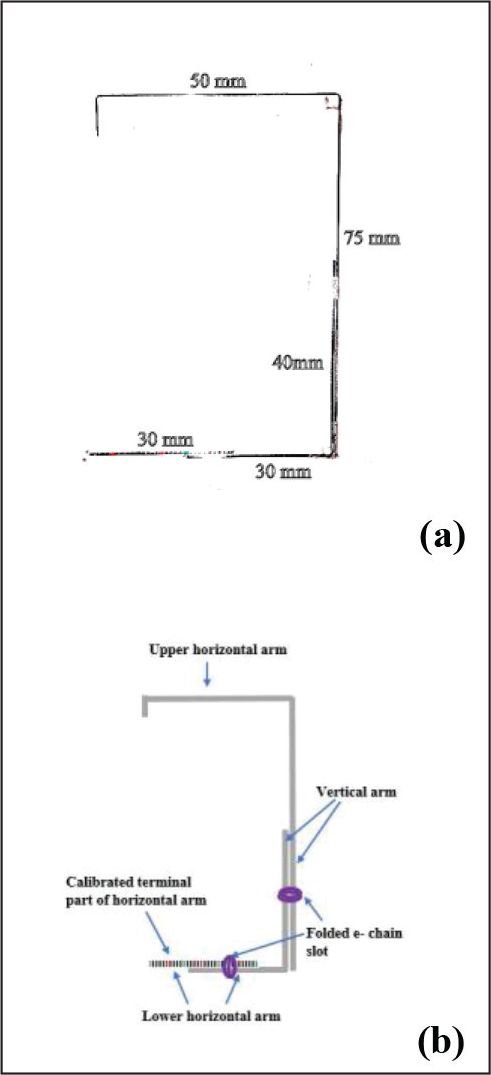
The device is made of spectacle and 0.019 × 0.025’ straight stainless-steel wire. It consists of 2 horizontal arms (ie, upper and lower) and 1 vertical arm made of 3 units of wire. The vertical arm is placed such that it is perpendicular to both the horizontal arms in 1 plane at its ends. The upper horizontal arm length is fixed and is 50 mm, while the lower horizontal arm and vertical arm length are adjustable. Adjustable arms are connected to folded e-chain slots such that they can be slid. The vertical arm can be adjusted 75–115 mm, and the lower horizontal arm can be adjusted 30–60 mm. Hence, it can measure the central incisor position up to 20 mm anterior and 10 mm posterior from its most esthetic position. Thirty millimeters of the incisal end of the lower horizontal arm are calibrated with every 1 mm marking using a fine tip permanent marker. The wire assembly is permanently glued at the center of the nose rest of the spectacle such that the upper horizontal arm is perpendicular to it.
Source:
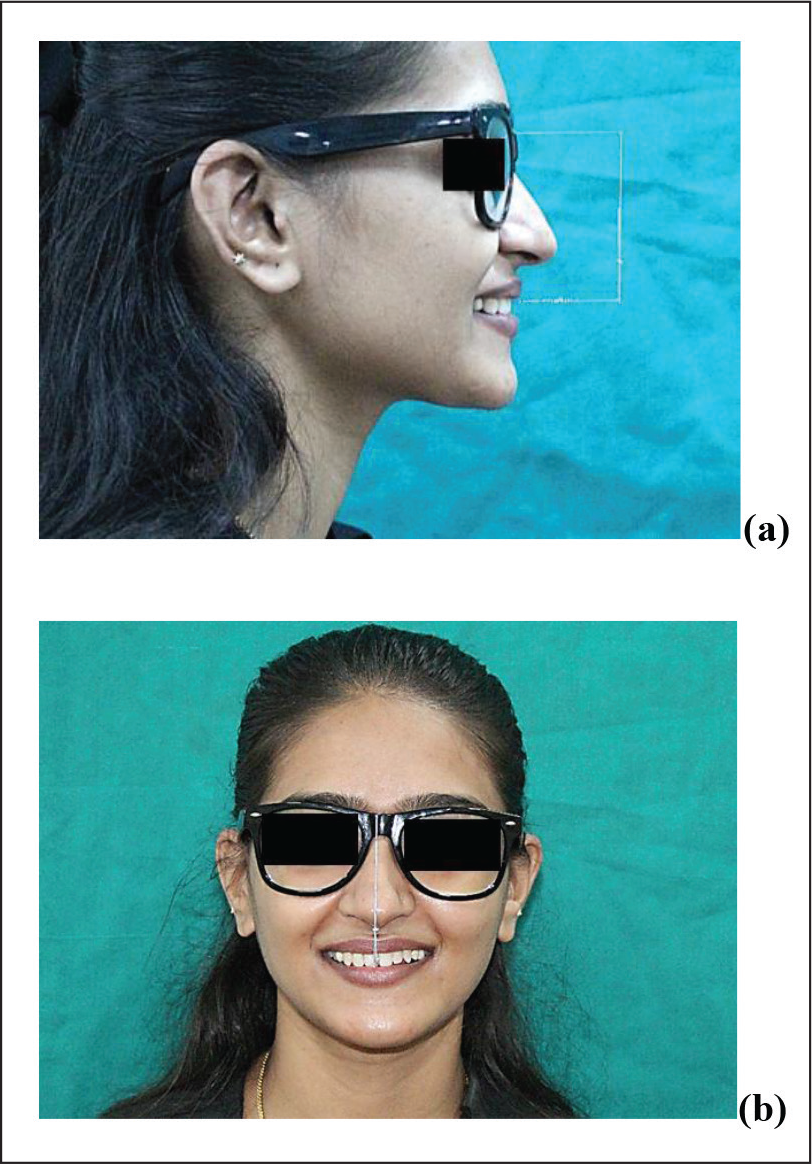
The patient is asked to wear the device, and the vertical arm is adjusted according to the vertical dimension of the patient’s face, such that the incisal end of the lower horizontal arm lies at the midpoint of the clinical crown of central incisors at the midline. Distance is measured with the horizontal calibrated arm of the device. The length of the lower horizontal arm is compared with the upper fixed horizontal arm. The difference in their lengths is the amount of forwarding or backward placement of incisors from their most esthetic position.
Advantages
It is cost-effective and easy to fabricate the device, and it can be used in all patients without any design modification. It is helpful in clinical examination of the position of incisors from its most esthetic position in the AP dimension.
Limitations
It cannot differentiate whether the position of the central incisor is due to skeletal or dental malocclusion.
It cannot be used in patients who are missing both central incisors and malformed central incisors.
Its accuracy is compromised in cases with restorations and/or veneers on central incisors.
It cannot be used in growing children in whom the AP growth of the maxilla has not been completed.
It cannot be used in patients who cannot wear spectacles due to the structural deformity of the ears or/and nose.
Conclusion
While using the P-device, the clinician should bear in mind that it is an adjunct to the photographic method, and that it is used to assess the optimal position of maxillary central incisors clinically. It can be incorporated in routine orthodontic record taking, diagnosis, and treatment planning.