
Abstract
Rectangular loops have been advocated for correcting severely malaligned teeth due to their simplicity and range of activation. This article describes a novel design of two rectangular loops used for correcting the bilaterally malaligned teeth without using the molars as anchor tooth. The present Rho loop offers an alternative for improving the position and angulation of severely malaligned bilateral teeth.
Introduction
Canines have the reputation of being the most notorious teeth of the oral cavity. As their eruption into the oral cavity is in the late mixed dentition period, in cases of tooth material arch length discrepancy, they are often left with no space within the arch, leading to their impactions or severe deviation from the normal eruption pattern or rotation along the axis leading to malalignment.
Movement of such severely rotated canines, most importantly, mandibular canines, requires several careful considerations like root proximity and positioning with the cortical bone, vertical and rotational control, and anchorage requirement, for the correction of these rotated canines in continuous mechanics is not advised due to large amount of indeterminate forces. Segmental mechanics provide a suitable alternative wherein the forces are determinate and rotated canines can be corrected.1, 2
This article describes a new loop design—Rho Loop—that leads to the correction of rotated and distally angulated canines simply and efficiently without generation of any unwanted reciprocal forces on the adjacent teeth.
Technique
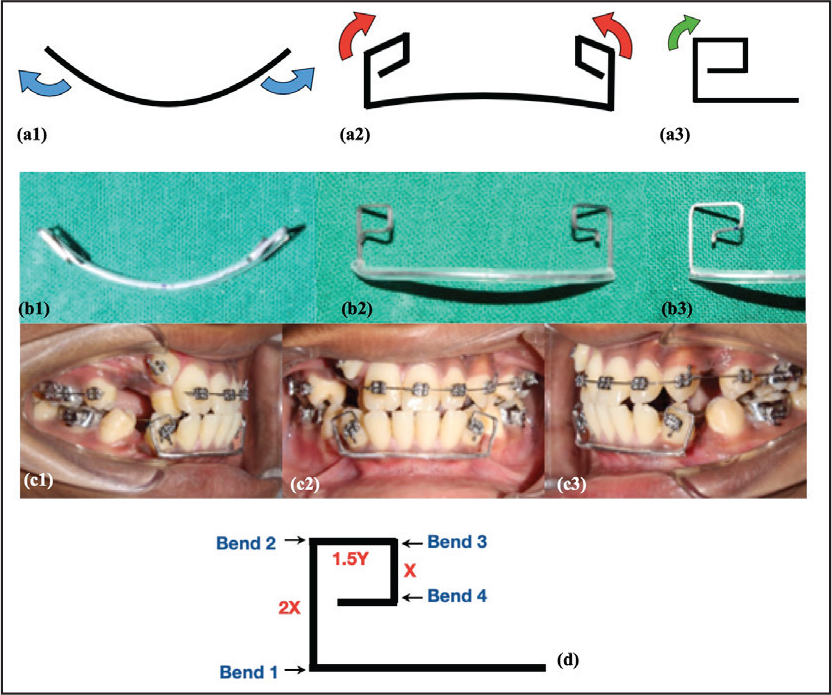
A segment of titanium molybdenum alloy or beta titanium (TMA) 0.017″ × 0.025″ or 0.019″ × 0.025″ depending upon the bracket slot is taken and formed into an arc in the region of mandibular canine, extending into the canine on the opposite side and bent occlusally (Bend 1) at the distal end of the canine bracket with the help of a light wire plier.
The distance between the bracket slot and the incisal edge of the teeth is measured (denoted as X) to determine the length of the vertical arm of the loop. Another bend is given at “2X” distance, in the same direction as Bend 1. At this point, the free end of the loop must be parallel to the occlusal plane.
The width of the preadjusted edgewise bracket is measured (denoted as Y) to determine the length of the horizontal segment. At 1.5 times the length of distance “Y,” a third bend (Bend 3) is given in the same direction as previous bends. This distance ensures that the vertical segment of the loop is clear of the distal surface of the canine bracket once it is engaged for the unrestricted action of the generated moments.
A fourth and final bend (Bend 4) is given in the same direction, as the previous bends at distance “X,” thus completing the Rho Loop (Figure 1[d]).
This distance “X” will ensure that the loop stays clear of the occlusal plane and does not project beyond it, thus avoiding chances of deformation and breakage due to occlusal forces during mastication.
Biomechanics and Function
The Rho loop is a self-activating loop and the amount of deflection of the malaligned teeth determines the amount of activation on full engagement. The moments for rotation correction are generated in the horizontal arms and uprighting are generated in the vertical arms of the loop, as shown in Figure 1(a). Thus, during the fabrication, the arch form of the patient is considered, and correspondingly, a matching arch form is made in the segment joining the two loops.
Since equal and opposite reactionary forces are generated on both sides of the arch, the technique involves no anchorage from the molar teeth, thus reducing the overall anchorage requirement.
The loop is recommended for rotation correction with simultaneous improvement in axial inclination of the bilaterally malpositioned teeth.
Due to limitations in the bond strength of the brackets, and to keep the forces within the physiological range, full activation for rotation and angulation correction is not recommended for severely malaligned teeth. Thus, in/out bends may be given in the horizontal segment of the Rho loop to decrease/increase the amount of activation.
However, possibility of gingival tissue irritation is present if the loop is abutting the marginal gingiva; hence, to prevent such incidents, a protective sleeve is recommended to be placed for the segment connecting the bilateral Rho loop and is not recommended in cases with high labial frenum. Furthermore, as the loop has little vertical control, it should be avoided in cases with vertical discrepancy in the two malpositioned teeth.
Clinical Procedure
Patient presenting with distally tipped and rotated bilateral mandibular canines was selected to be corrected by Rho loop, that is, modified segmental mechanics, prior to a complete bonded appliance therapy, since the canines require significant rotation correction and uprighting, as determined on an orthopantomograph and study models (Figure 2 and 3[a]). Additional cone beam computed tomography (CBCT) imaging was not done keeping as low as reasonably achievable (ALARA) principle as the amount of rotation could be assessed with the study model and photographs.
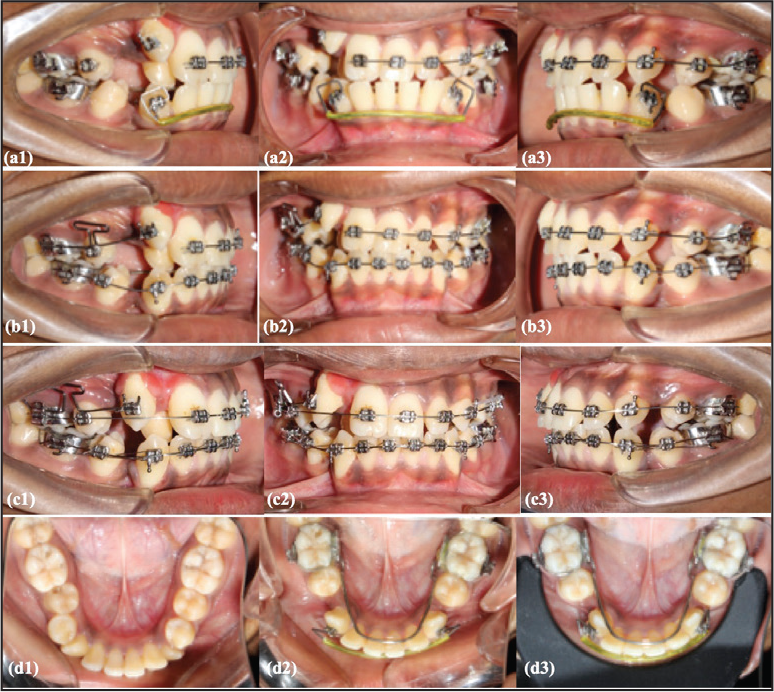
Rho loop was fabricated and placed in the patient after the first premolar extraction (Figure 1[c]). The patient was kept of recall visits and after 5 months, improvement in canines rotation and angulations were observed to be incorporated into the 0.016″ NiTi arch wire (Figures 3[b, c] and 4).
Discussion
In cases involving severely rotated teeth, segmental mechanics have been advocated to have better control over the positional correction of the teeth. Among the variety of loops, the most commonly employed loops are T-loop 3 , R-loop, 2 and box loop, 4 but one common aspect to all of the loops is the requirement of the anchorage preparation to transmit the reciprocal forces.
In this novel design, instead of the reactionary forces being transmitted to the molar tooth, these forces were balanced by connecting the other end of the loop with the canine on the opposite side of the arch showing the same degree of malalignment.
Schematic diagram of Rho loop in (al) Transverse view (a2) Frontal View (a3) Sagittal view. Representative sample in 0.017”x 0.025” TMA wire (b1) Transverse view (62) Frontal View (63) Sagittal view. Loop placed in the oral cavity (c1) Right Lateral view (c2) Frontal view (c3) Left Lateral view (d) Design description of the loop
Rho loop engaged in the mandibular arch after 3months (al) Right Lateral View (a2) Frontal View (a3) Left Lateral View, Continuous engagement of the lower arch possible after canine rotation correction after 5months (b1) Right Lateral View (62) Frontal View (63) Left Lateral View, case progression with straight wire appliance (cl) Right Lateral View (c2) Frontal View (c3) Left Lateral View, Progressive changes in the mandibular arch with the Rho loop (dl) Pretreatment (2) After 3 months (3) After 5 months
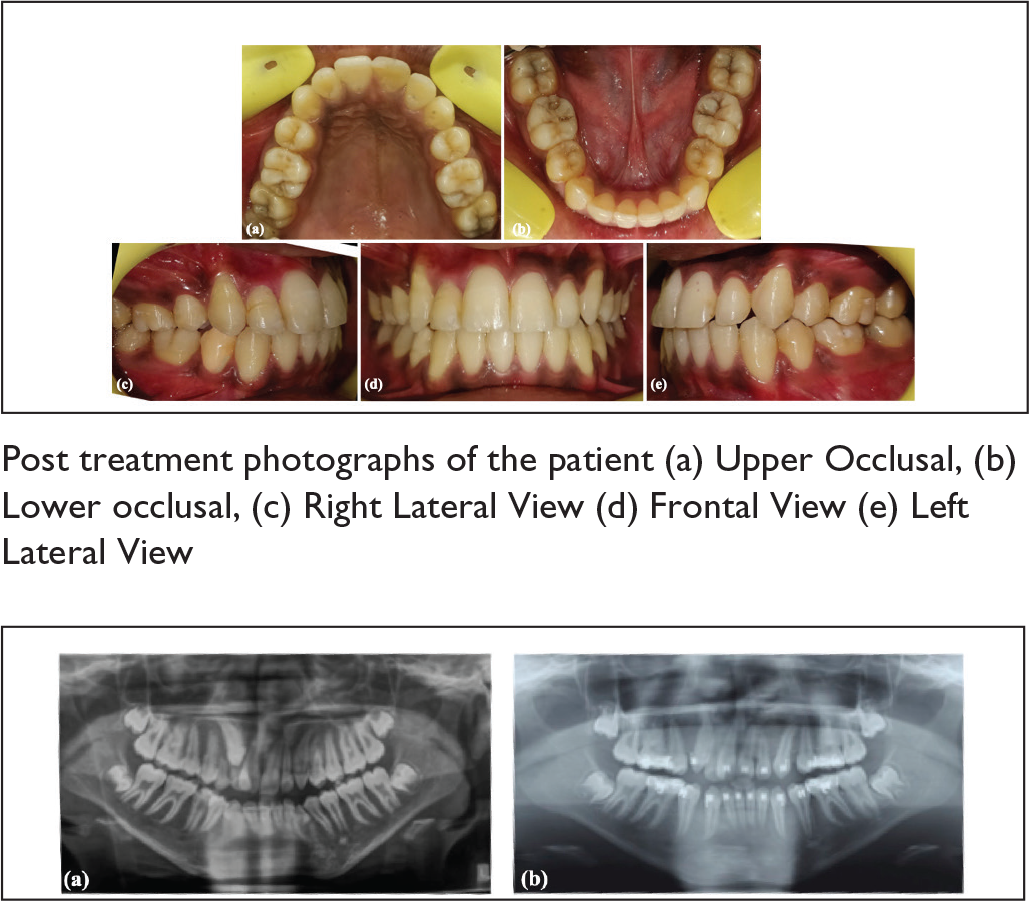
Progressive changes in the angulation of the mandibular canine on the OPG (a) Pretreatment and (b) After 6months
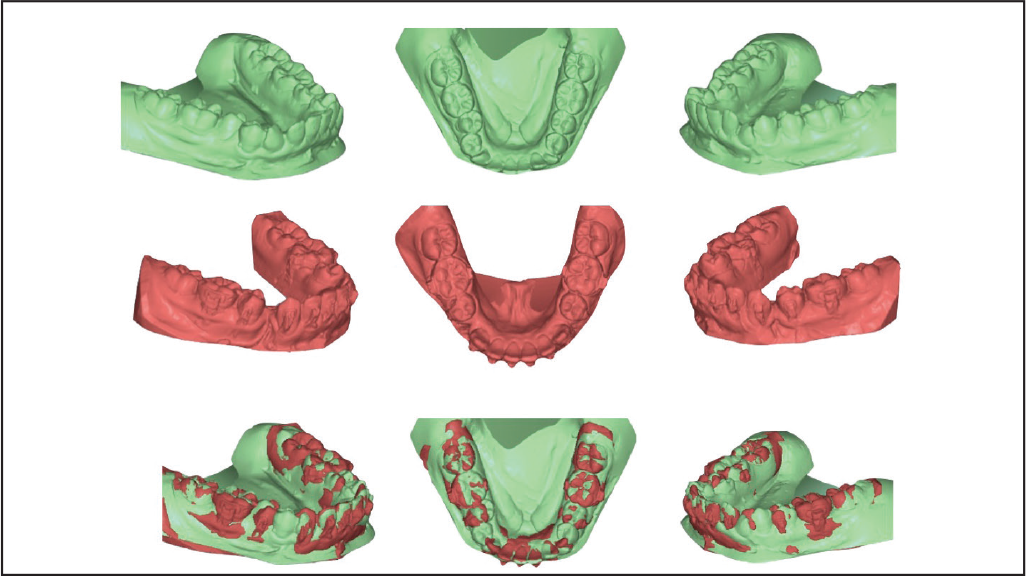
Pre-treatmment model of the patient (in green) (al) Right Lateral View (a2) Occlusal View (a3) Left Lateral View, Stage model of the patient after rotation correction of canines (5months) (in red) (b1) Right Lateral View (62) Occlusal View (b3) Left Lateral View, Superimposition of the changes in the mandibular arch (cl) Right Lateral View (c2) Occlusal View (c3) Left Lateral View
Conclusion
The quest for simple and efficient mechanics to correct bilaterally malaligned teeth led to the development of this loop. The reported “Rho loop” can be used to correct bilaterally malaligned teeth with simple segmental mechanics, which decreases the overall anchorage requirement during the fixed orthodontic therapy.
Statement of Informed Consent
Informed consent was not sought for the present study because no identifiable images were used