
Abstract
Introduction
As regards the prevention of spread of COVID-19, the first step taken by many countries, along the lines of the hierarchy of infection control, has been attempting elimination of the risk by very simply avoiding exposure. This has been instituted in the form of partial or complete lockdowns, including instructions to limit dental procedures to only those absolutely necessary, with almost no elective orthodontic treatment rendered in any form. 1 The only problem with this has been that when regular monitoring of orthodontic treatment cannot be done, there is every scope for a minor issue escalating into a dental emergency.2-6
With community transmission slowly ebbing in most parts of the world, decisions are being made to revert back to a pattern of normalcy while attempting to strike a balance between lives and livelihoods as the danger has not completely passed us yet. 7 This article strives to re-emphasize infection control protocol that can allow for safe practicing even under challenging circumstances to prevent recurrences or relapses of disease transmission.
Methods
Scientific databases, such as PubMed, Cochrane Library, and Google Scholar, were searched for relevant articles. Emphasis was placed on the following search terms: “Covid-19,” “SARS-CoV-2,” “Coronavirus,” “infection control,” “standard precautions,” “dentistry,” and “orthodontics.” In addition to this, updated information from various advisory sources, such as the World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), United States, European Centre for Disease Prevention and Control (ECDC), Chinese Center for Disease Control and Prevention (China CDC), Ministry of Family Health and Welfare (MOFHW), India, American Dental Association (ADA), Canadian Dental Association (CDA), National Health Service, England (NHS UK), National Health Service Scotland (NHS Scotland), and International Society for Infectious Diseases (ISID), United States, was also referenced.
The author and co-author scrutinized articles of relevance, along with their references, for further information, if any. The recommendations of advisory bodies were cross compared to allow a compilation.
Literature Overview
There has been a growing impetus in getting the dental community to adopt uniform standards of efficient infection control and prevention in the form of universal precautions ever since the AIDS pandemic created an awareness of blood-borne diseases, and soon after as standard precautions to include other bodily fluids under what is referred to as “Other Potentially Infectious Material” (OPIM).8-11 When a certain disease has a mode of transmission that requires additional care, transmission-based precautions are also instituted, as is the case with the current COVID-19 crisis. 12 Efficient infection control would not only safeguard health care professionals but also protect patients from nosocomial infections. 13
In spite of advisories and protocols, compliance has always been a bit poor, as most dental work seems to be essentially nonsurgical, with no visible blood.14-20 Dr. James Crawford, one of the founding officers of the Organization for Safety, Asepsis and Prevention, managed to dent this nonchalant attitude with his graphic video “If Saliva Were Red,” in which cross contamination of a mannequin, the dental unit and the dental operatory were depicted with the assumption that saliva was dyed red, allowing visualization of the cross contamination. On the one hand, it might seem best with regard to single-handed procedures for the operator to clean up after a procedure through multitasking, while, on the other hand, division and delegation of responsibilities to an assistant or an infection preventionist might seem to increase single-task efficiency.21, 22 Thus, there is normally a requirement for a dedicated infection preventionist who supervises the before, during and after protocols of procedural infection control. 23
The least effective modality of infection control is in the use of personal protective equipment (PPE), as failure can result either due to a breach in protocol, a laxity in the formulation of the policy of PPE usage, or a laxity in the actual utilization without sticking to proper protocol. Multilevel compliance is required for PPE to be effective, as personal protection has multiple aspects working together synergistically. 24 To this day, there is reluctance to use proper PPE even when available, and most often, errors in donning and doffing result in autoinoculation. 25
As dentistry is essentially a collection of elective procedures that usually aim to finally provide an aesthetic outcome, as orthodontics essentially does, most operatories are designed to be as aesthetically appearing as possible. 26 There has never been much thought put into stark operatories, much like operation theatres that are devoid of decoration, additional furniture and the items like toys for children or magazines for the adults.
The need to limit dental procedures has stemmed from the fact that COVID-19 has caught us unprepared. With respiratory health becoming the keyword of the day it has finally dawned upon us that our profession needs the same sort of high efficiency particulate filter protection as used by industrial workers in the form of N95 or N99 respirators. Advisories that initially tried to quell public panic and preserve vital supplies through stressing on no need for any form of masks were soon replaced with advisories that recommended some form of protection, much as how it had been during the SARS epidemic. 27 Most droplet models revolve around the Wells evaporation curve that predicts how far a droplet may travel before it either drops to the floor or evaporates and becomes a droplet nucleus. In certain circumstances, especially those involving aerosol procedures, the mode of spread seems to be opportunistic airborne.28-31 Slowly but surely, acceptance of this risk and proposed countermeasures have found their way into most post-lockdown advisories that still seem limited to very basic treatments as the bigger question remains unanswered: “If infections like Covid-19 could be opportunistic airborne and if dentistry had the risk of aerosols and confined spaces, shouldn’t there be a focus on not used droplet infection precautions but also airborne infection precautions as a standard part of all of our practices?”32-35
The problem with engineering controls is that most often they are better implemented at the time of inception, during the construction phase. Remodeling an existing setup, while not impossible, might seem tedious. The main motivational thought here should be that if these engineering controls are in place in all dental facilities, it might be possible to render a larger spectrum of treatment options in safety. Administrative controls essentially aim at ensuring that the workflow is much more effective from an infection control standpoint, with policies, protocols, checklists, and audits to keep a check and to ensure compliance.
Discussion
COVID-19 or SARS-CoV-2 is predominantly a droplet infection spread by the release of droplets through talking, sneezing, or coughing, and also by hand-to-nose, hand-to-mouth, or hand-to-eyes transmission after touching contaminated surfaces. 36 Certain situations that may induce aerosol generation may allow for an opportunistic aerosol mode of transmission. Saliva in itself is to be considered infectious. 37
Infection control guidelines are often listed in an order of priority, in which the first and foremost desirable option is always elimination of the problem. In the case of COVID-19, that would imply avoiding exposure. In situations where this may not be feasible, as when called upon to render professional services, the next two options of significance are engineering controls and administrative controls that include safe practices. Finally, PPE is used as the last resort, the final option of a barrier between the actual pathogen and the dental health care worker (the dentist, the assistant or even the laboratory technician). Apart from the standard protocol of infection prevention and control, it is necessary to emphasize transmission-based protocol as well, necessitating the use of tight-fitting eyewear and respiratory protection in the form of FFP2- or FFP3-type respirators.38-53
Engineering Controls
These involve modifications made to the equipment, ventilation or work processes which aim to eliminate, reduce, or contain the hazard.
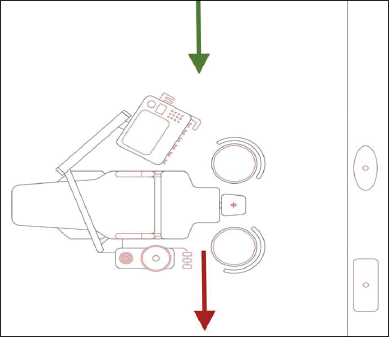
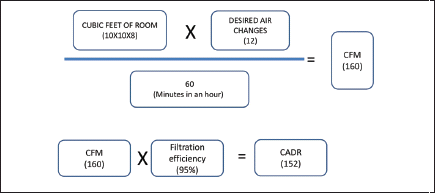
General Ventilation: With regard to respiratory health, this control aims at eliminating, reducing, or containing dust, fumes, and suspended infectious materials, like droplets or aerosol, by also including guidelines already existing for the airborne diseases like tuberculosis.54-62 The recommended ventilation is around 60l/s per patient if mechanical ventilation is considered and around 160 L/s if natural ventilation is harnessed, thus effecting a minimum of 12 air changes per hour (12 ACH).63-68 Advisories list the importance of isolating a suspected positive patient or performing aerosol-generating procedures in an airborne infection isolation room (AIIR).42, 64, 67, 69 AIIRs are temporary negative-pressure isolation (TNPI) rooms that have the heating, ventilation, and air conditioning (HVAC) system modified to allow for a differential between the supplied or incoming filtered air, which is filtered through either high-efficiency particulate air (HEPA) filters or ultra-low particulate air (ULPA) filters, and the exhaust of outgoing air that is sucked out through an exhaust mechanism either comprising simple wall or ceiling exhaust fans that have the exhaust air ducted to a remote location or by way of centrifugal or inline exhaust fans installed in the existing HVAC ducts.70–72 Germicidal ultraviolet (UV)-C lamps may be installed both in the incoming air portion and the outgoing air portion of the HVAC system.73-75 Some advisories list working in a well-ventilated area as an option wherein natural ventilation is harnessed, provided this can be unidirectional, with no buffeting that might create turbulence, and provided the location of the contaminated-air exhaust poses no risk.65, 67 As regards dental operatory, an ideal HVAC installation should allow for fresh filtered air to enter either from the side of the operator (the right side of the dental chair) towards the spittoon and out (the left side of the dental chair), as shown in Figure 1, or from the foot end of the patient at a lower level, finally exiting toward the head end by way of ceiling exhausts, especially if the HVAC option is to provide air that is cool, as in hotter climates. Here the assumption of two stacks of air, the cooler air towards the bottom of the room and the warmer air at a higher level, is made. For an operation theatre, the normal recommendation is for 12 ACH, under the assumption that the operation theatre is not going to be used for back-to-back procedures. In a dental operatory, if there are appointments that are being given once every half hour for minor procedures or a brief consultation, 12 air changes for every half hour can be tweaked through modifying the cubic-feet-per-minute (CFM) parameters of the HVAC exhaust, as detailed in Figure 2.63-68
Local exhaust ventilation: Unlike surgical suction cannulae or saliva ejectors that have lower flow rates so that delicate tissues are not damaged while aspirating fluids, high-volume evacuation (HVE) cannulae have a flow rate of approximately 300L/min. When used appropriately, HVE cannulae not only aspirate fluids but also serve the purpose of local evacuation ventilation through aspirating aerosol as well. Extraoral vacuum aspiration devices, which mimic industrial fume extractors, have been used in dentistry to eliminate or reduce mercury vapor fumes in the Safe Mercury Amalgam Removal Technique, smoke plumes in electrosurgery and laser surgery, and dust in air abrasion dental procedures.76-80 When used in conjunction with infective aerosol, there are two problems: one of infection control between patients and the other of moisture gathering at the receptacle and dripping. A simple workaround would be to use an autoclavable spittoon funnel or cup in conjunction with an extra HVE suction line. As the only two portions of a dental unit that accept infectious waste are the suction line and the spittoon, some dental manufacturers, like M/S Planmeca Oy, Finland, offer, by default, the provision to order a unit with or without a spittoon, as shown in Figure 3. Source: Procured directly from the manufacturer M/S Planmeca Oy, Finland. In recent COVID-19 advisories released, India, France, and Belgium stress on not using the spittoon at all.32, 81, 82 A spittoon funnel is used in units that do not have a spittoon, in that the patient holds it in their hand and spits into the funnel when required. Requesting the patient to hold it close to the face helps aspirate aerosol much like extraoral suction. Mobile high-efficiency-filter air cleaners are another form of local exhaust ventilation.
83
An Ideal Negative Pressure Scenario Creating Unidirectional Air Flow from the Operator Side Towards the Patient and Beyond the Spittoon thus Creating a Clean Zone Near the Operator.
Exhaust Fans are normally described by their airflow capacity in CFM or Cubic Feet per Minute. A standard room 10 feet long & 10 feet wide with a ceiling height of 8ft requires an exhaust fan with a minimum 160 CFM rating to achieve 12 ACH. Mobile High Efficiency Filter Air Cleaners are rated by their CADR or Clean Air Delivery Rate which is the CFM multiplied by filtration efficiency. The required CADR is the area of the room divided by 1.55 (100 sq.ft divided by 1.55 = CADR 64.5).

UVGI is used either as part of the HVAC system for continuous air purification within the ducts or for upper room irradiation and disinfection.84-88 UV-C germicidal lamps within the HVAC system may have the benefit of continuous exposure to and purification of air, as they are hidden from sight and are thus not a risk. 89
Administrative Controls and Safe Practices
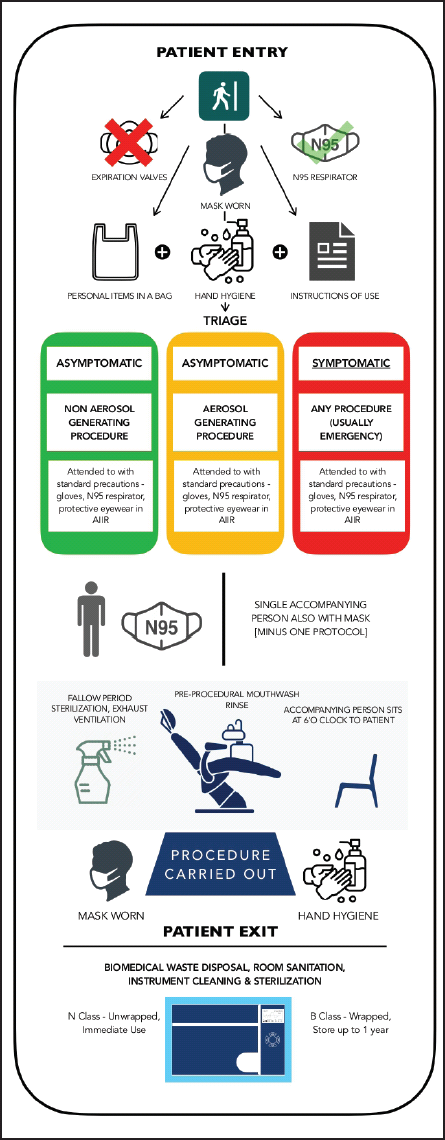
These are policies or protocols that change the work style through effecting changes in the timing or scheduling of work, standard working or operating protocol, safe practices, and hygiene protocol, including cleaning, disinfection, and sterilization as listed in Table 3 and summarized in Figure 6.
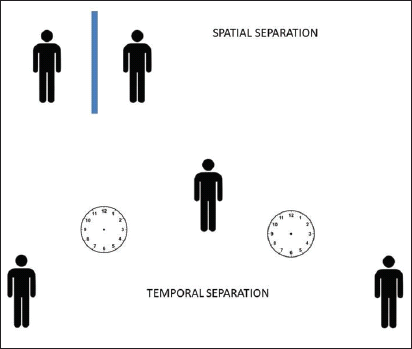
Social Distancing Options are Referred to as Spatial Separation or Temporal Separation Based on Barriers or Time of Entry.
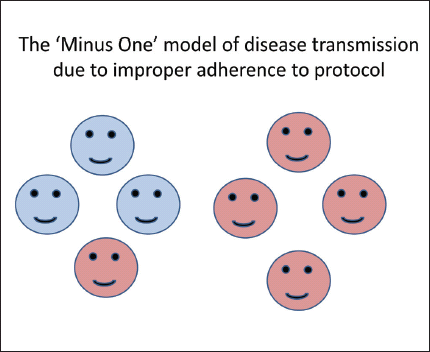
The ‘Minus One’ Model Proposed by The Authors Indicates the High Chance of Transmission Risk to Everyone in a Confined Space Even if One Person is not Shielded as in the Case of a Patient not Wearing a Mask During a Procedure Due to Errors in Donning or Doffing PPE.
Sequence of Patient Entry and Handling.
Suction lines can be disinfected between patients using biocides, as advised or recommended by most dental-unit manufacturers. Some of these biocides also have enzymatic constituents aimed at keeping the various parts of the suction system clean and running efficiently. Dental-unit waterlines are similarly to be flushed with a biocide between patients and at the beginning and end of each day. Some manufacturers offer an option of inbuilt catalytic converter purifiers that purify city water and produce hypochlorous acid and hypochlorite to directly disinfect the water and waterlines.
94
The authors propose a MINUS ONE MODEL as related to the number of people within the operatory at risk of infection . If all individuals within the operatory have donned appropriate PPE and the only individual who is allowed to remain within the operatory without any form of respiratory protection is the patient, the number of individuals at risk of contracting a respiratory illness on account of improperly used PPE is the total number of individuals minus one (Figure 5).
Results
The main focus of the research was to collect information relevant to resuming routine work. Preference was given to consolidated data that had already been thoroughly vetted, allowing a comparison of recommendations to be done. Proposals based on this data have been listed in Table 1, with Level 1 being safer and optimum or desirable and Level 2 being the minimum level of desirable safety.
A Summary of Safety Protocol Proposed in the Literature Reviewed Divided into Level 1 and Level 2 .

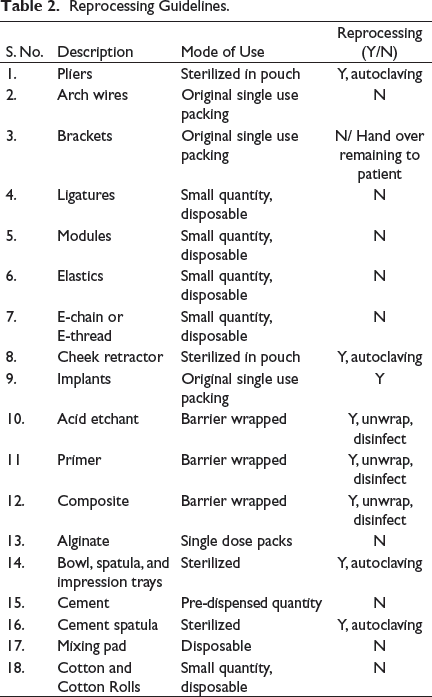
Reprocessing Guidelines.
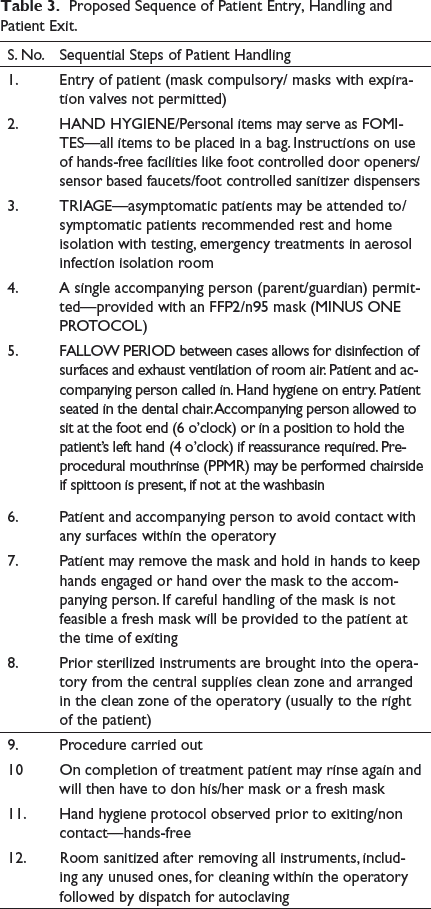
Proposed Sequence of Patient Entry, Handling and Patient Exit.
Conclusion
Infections are always going to be part of health care systems. However, if infection control is truly efficient, health care would always have the upper hand. With each challenge posed, a call arises for better measures to safeguard health care workers and patients alike, and the community on the whole. Advisories often stress on the bare-minimum level of precautions that must be followed, and thus judicious, scenario-based application of infection control protocol is always required.