
Abstract
Objective:
The objective of this systematic review was to assess the available evidence to evaluate the effectiveness of en-masse retraction design with mini-screw with respect to the retraction hook and mini-implant position and height.
Methods:
The following electronic databases were searched till July 31, 2020: Pro-Quest Dissertation Abstracts and Thesis database Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, Google Scholar, US National Library of Medicine, and National Research Register. En-masse retractions with anterior retraction hooks assisted by mini-implant three-dimensional finite element method (3D FEM) models were included in the study. The selected studies were assessed for the risk of bias using the Cochrane Collaboration risk of bias tool. The “traffic plot” and “weighted plot” risk of bias distribution were designed using the ROBVIS tool. The authors extracted and analyzed the data.
Results:
Twelve studies fulfilled the inclusion criteria. The risks of biases were low for 9 studies and high for 3 studies. Data on mini-implant, retraction hook, and the center of resistance/force vectors were extracted. The outcomes of the included studies were heterogeneous.
Conclusions:
According to the currently available literature review for successful bodily en-masse tooth movement, the force vector should pass through the center of resistance, which can be achieved by the clinical judgment of placing a mini-screw and an anterior retraction hook. The force from an implant placed at a higher level from the anterior retraction hook will cause intrusion; an implant placed at the medium level shows bodily movement; and an implant placed at a lower level shows tipping forces in consolidated arches.
Introduction
Anchorage is a crucial step in planning for orthodontic treatment. It can be provided by both intraoral and extraoral techniques and which can act as primary or reinforced anchorage. Newton’s third law states, for every action, there is an equal and opposite reaction, which is applicable in orthodontics. With recent advances in the specialty of orthodontics, it is established that skeletal anchorage provides absolute stability to the segments by providing resistance toward undesirable reactionary tooth movements. Bone screws, Y-shaped plates, and onplants 1 are used as means of achieving absolute anchorage. Intraoral anchorage using appliances such as transpalatal arch and nance holding arch does not require patient cooperation, whereas extraoral anchorage using appliances such as headgear demands patient’s cooperation for successful treatment outcome. The first successful orthodontic implant was placed by Creekmore and Eklund 2 in 1983, but it was Kanomi 3 in 1997 who described a mini-implant specifically designed for orthodontic use. In anterior en-masse retraction, anchorage planning is critical for successful orthodontic treatment. Conditions such as skeletal open bite 4 and skeletal class III malocclusion may require absolute anchorage. Planning anchorage, especially in extraction cases, is critical in determining both the treatment outcome and the selection of appropriate mechanisms 5 .
The photoelasticity method, the strain gauge method, laser holography, and the finite element method (FEM) are some of the advanced technologies used to analyze the biological and biomechanical properties of orthodontic tooth movement. FEM is a tool used to gauge stress and strain by simulating a biological entity to a computer-generated model 6 . FEM evaluates the stress distributions and three-dimensional (3D) displacements in different organic/inorganic models with irregular geometry and nonhomogeneous physical properties 7 . In 1943, R. Courant 8 first formulated mathematical techniques to analyze the biomechanical properties of the object. It was Weinstein 9 in 1976, who first applied FEM to dentistry to measure the various occlusion loads on implants. Since then, the FEM method has been used in the field of orthodontics to decipher the physiologic responses of dentoalveolar complex to orthodontic forces by exhibiting quantitative data.
Objectives
The aim of this study was therefore to compare and evaluate the effectiveness of en-masse retraction design with mini-screw with respect to the retraction hook and mini-implant position and height.
Material and Methods
Protocol and Registrations
The systematic review was performed in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analysis
10
guidelines and the main research question was formatted according to the patient, problem or population intervention comparison, control or comparator outcome (PICO). The protocol for a systematic review of mini-screw-enabled en-masse retraction was registered on the National Institute of Health Research Database (PROSPERO
Eligibility Criteria
The following selection criteria were applied for the review.
Information Sources, Search Strategy, and Study Selection
List of Search Engines and the Result Obtained Using MeSH Terms With Sample of PubMed Search Terms.
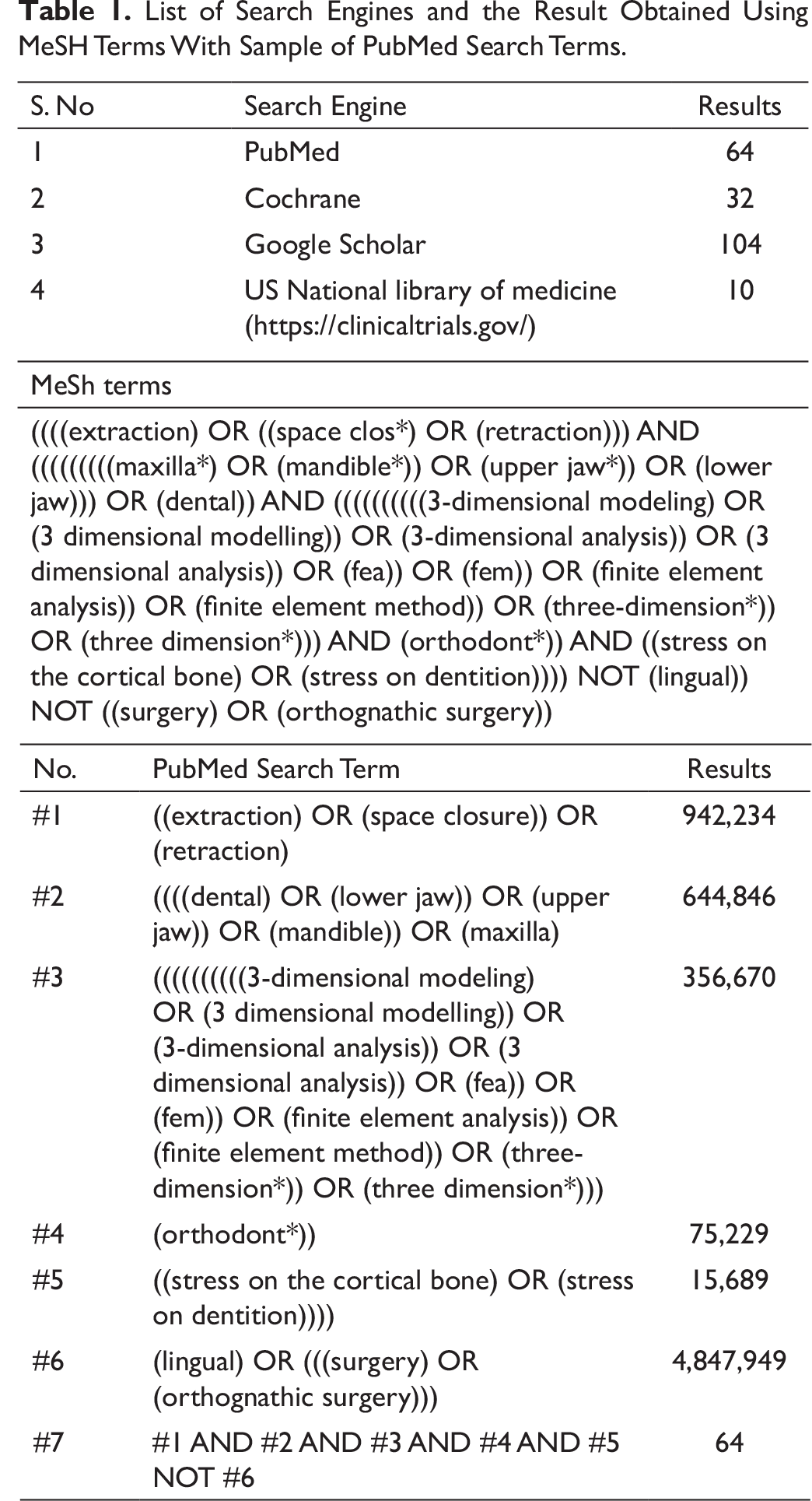
The study selection was done in 2 phases. In the first phase, the title and abstract were screened independently by 2 reviewers (AA, PS). The short-listed studies are selected for full-text reading. Strict inclusion criteria scrutinizing was done. Any disagreements between the 2 reviewers were sorted by a discussion with third and fourth reviewers.
Data Items and Collection
The data extraction was performed by 2 reviewers (AA, PS) independently to record the general information such as author, year of publication, and study setting, study method, FEM software used, a technique used (En-masse retraction method, friction mechanics), the primary outcome, that is, position of ARH and mini-screw and secondary outcome, that is, force vector considerations, and inference/recommendations.
Risk of Bias/Quality Assessment in Individual Studies
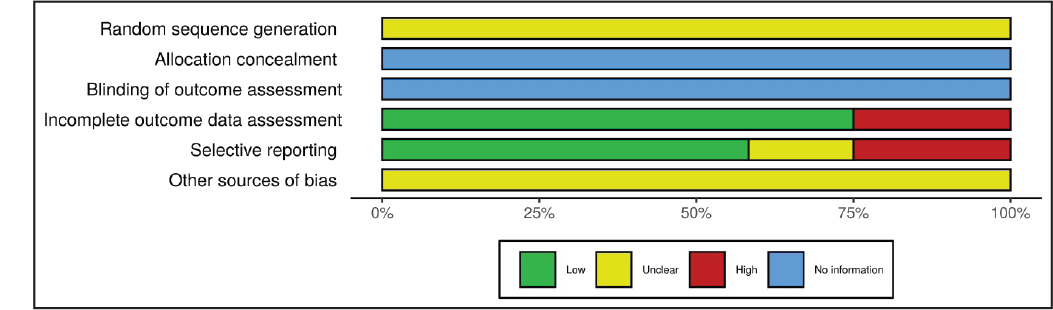
The quality of the selected studies was evaluated by a pair of observers (AA, PS) on ROBVIS 11 (Covidence) using the Cochrane Collaboration risk of bias tool, as described in the Cochrane Handbook for Systematic Reviews of Interventions 12 . A total of 6 domains of bias were assessed: (a) random sequence generation, (b) allocation concealment, (c) blinding of outcome assessment, (d) incomplete outcome data assessment, (e)selective reporting, and (f) another source of bias. The blinding of participants and operators was not included. The sequence generation was not explained, as the included studies did not report it. The use of sequence generation is questionable for in vitro studies or perhaps impossible, particularly for FEM study. Evaluation of allocation concealment of in vitro studies was not appropriate.
Results
Study Selection and Characteristics
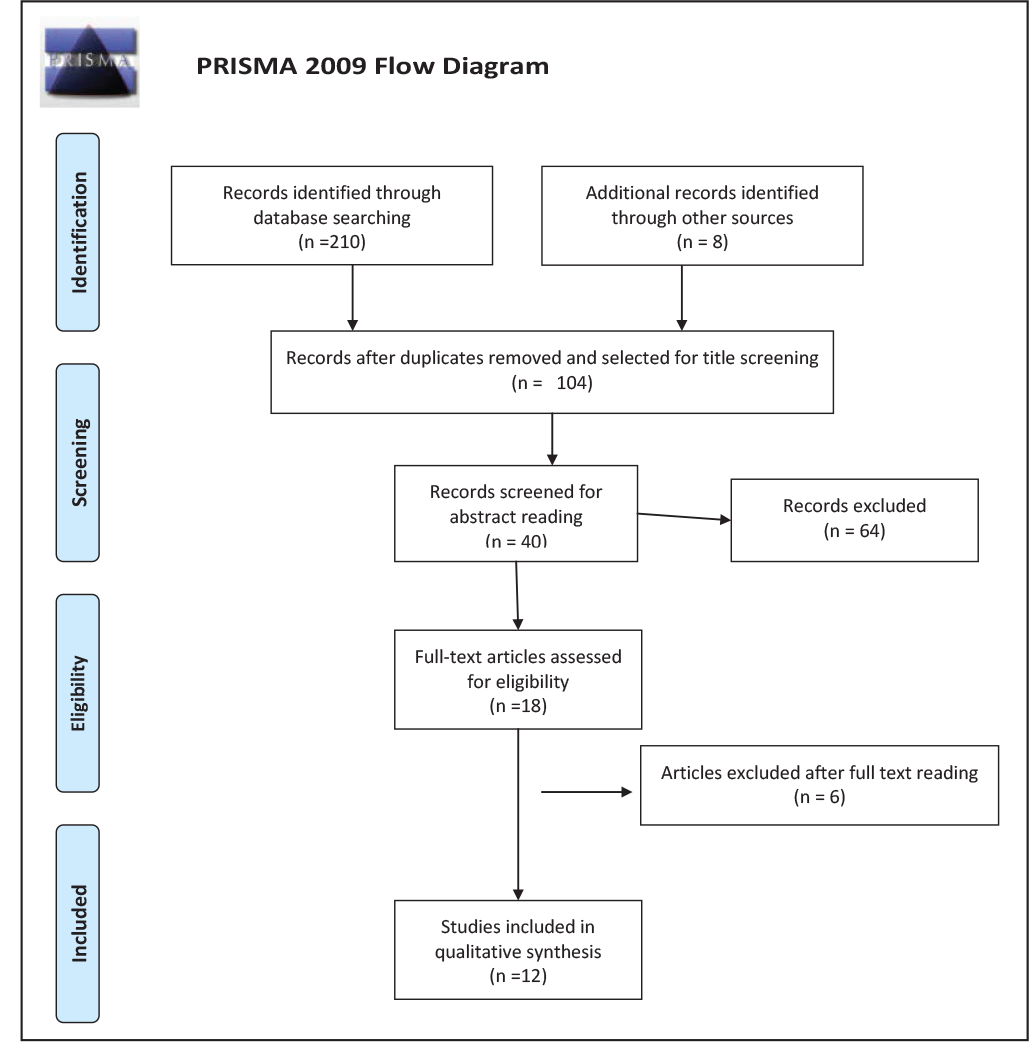
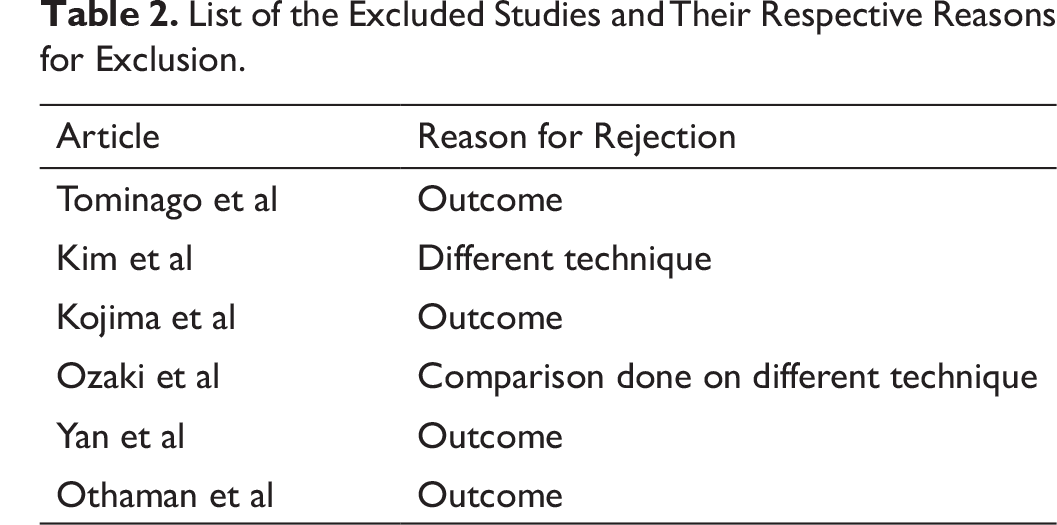
A total of 210 articles were identified after electronic search (PubMed, CENTRAL, Google Scholar, and US National Library of Medicine) and 8 articles were included by hand search. After removing the duplicates, 104 articles were short-listed, out of which 40 articles were included for abstract reading for Phase I screening. Totally, 18 articles selected for Phase II full-text reading (Figure 1). Finally, 12 articles were selected for qualitative review. Six articles were excluded, and the reasons for their exclusion are presented in Table 2. All the 12 articles were original research articles, and basic characteristics and inference were tabulated separately.
List of the Excluded Studies and Their Respective Reasons for Exclusion.
Risk of Bias Within Studies
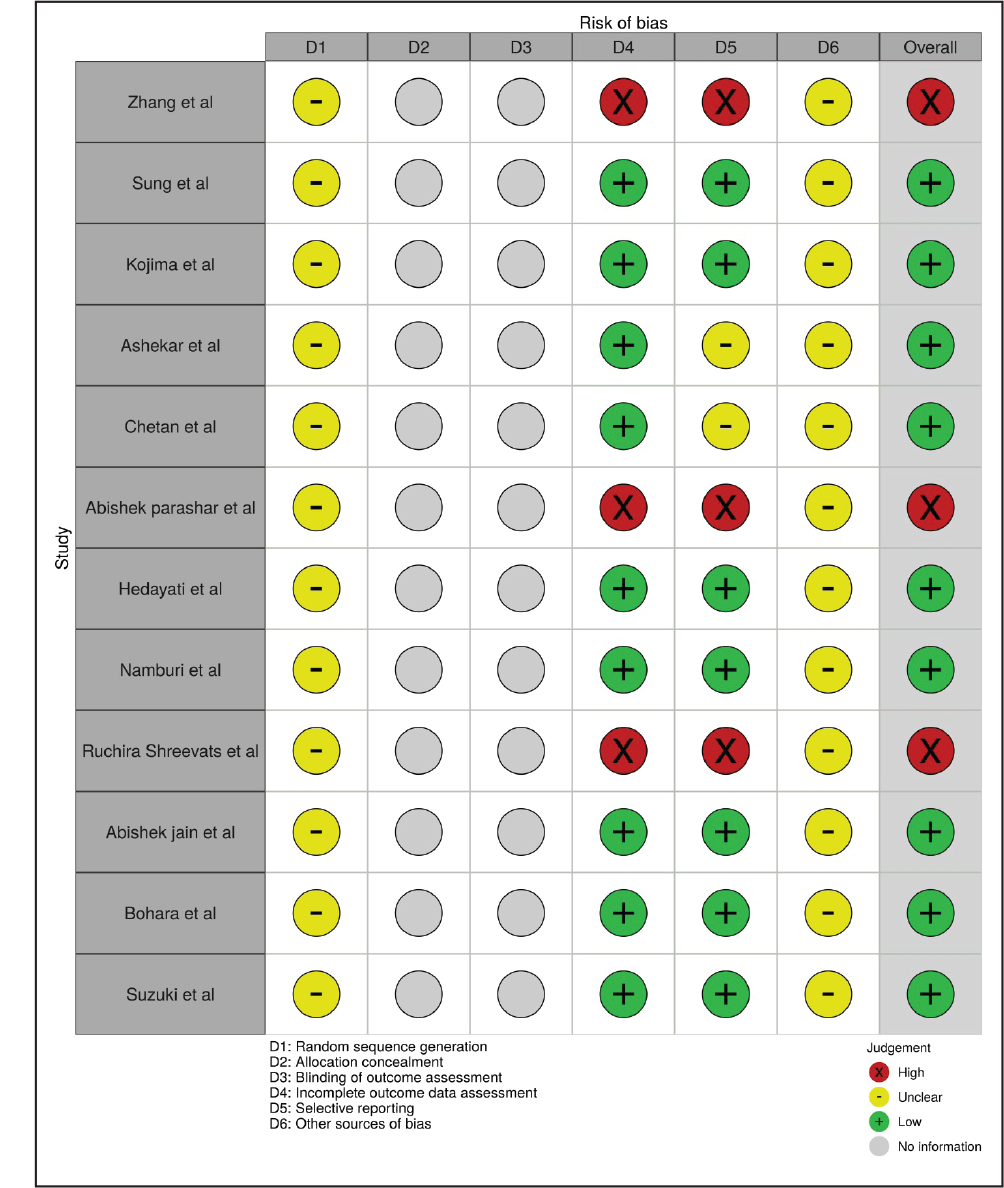
All the included studies were assessed for risk of bias through the Cochrane Collaboration risk of bias tool, as described in the Cochrane Handbook for Systematic Reviews of Interventions (Figures 2 and 3). The overall assessment of bias was done under high, low, unclear, and not applicable as per Cochrane Handbook for Systematic Review. Three articles were having a high risk of bias, whereas 9 articles were having a low risk of bias. Tests for the risk of bias across studies were not undertaken.
Synthesis of Results
Meta-analysis was not possible due to sizeable heterogeneity in various methodological, clinical, and statistical variations. Solid heterogeneity is present in the various methods of outcome measurement, the different landmarks used for positioning the mini-implant and ARH, and application of force via elastics versus coil. Hence, only a qualitative report was obtained.
Results of Individual Studies
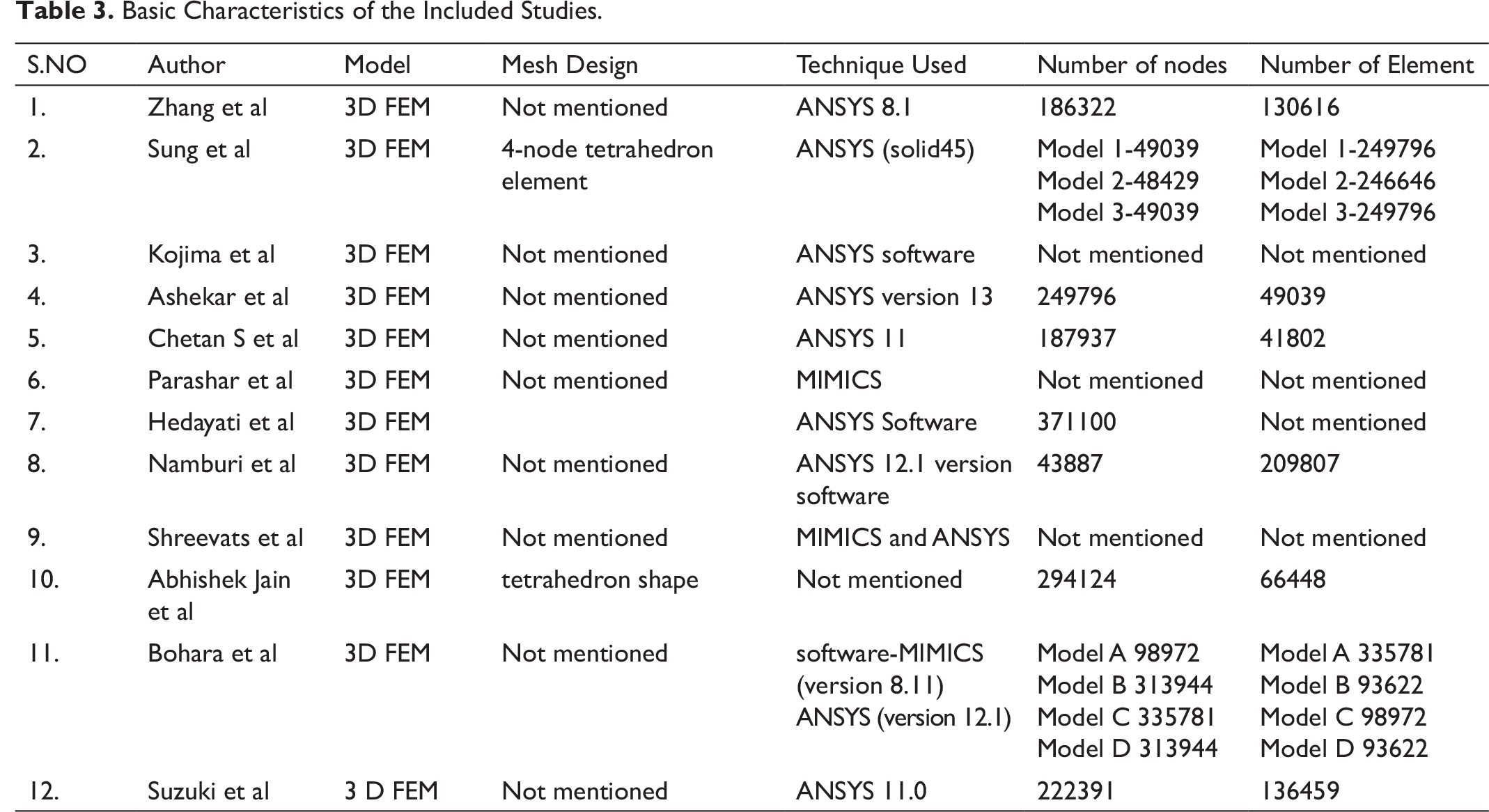
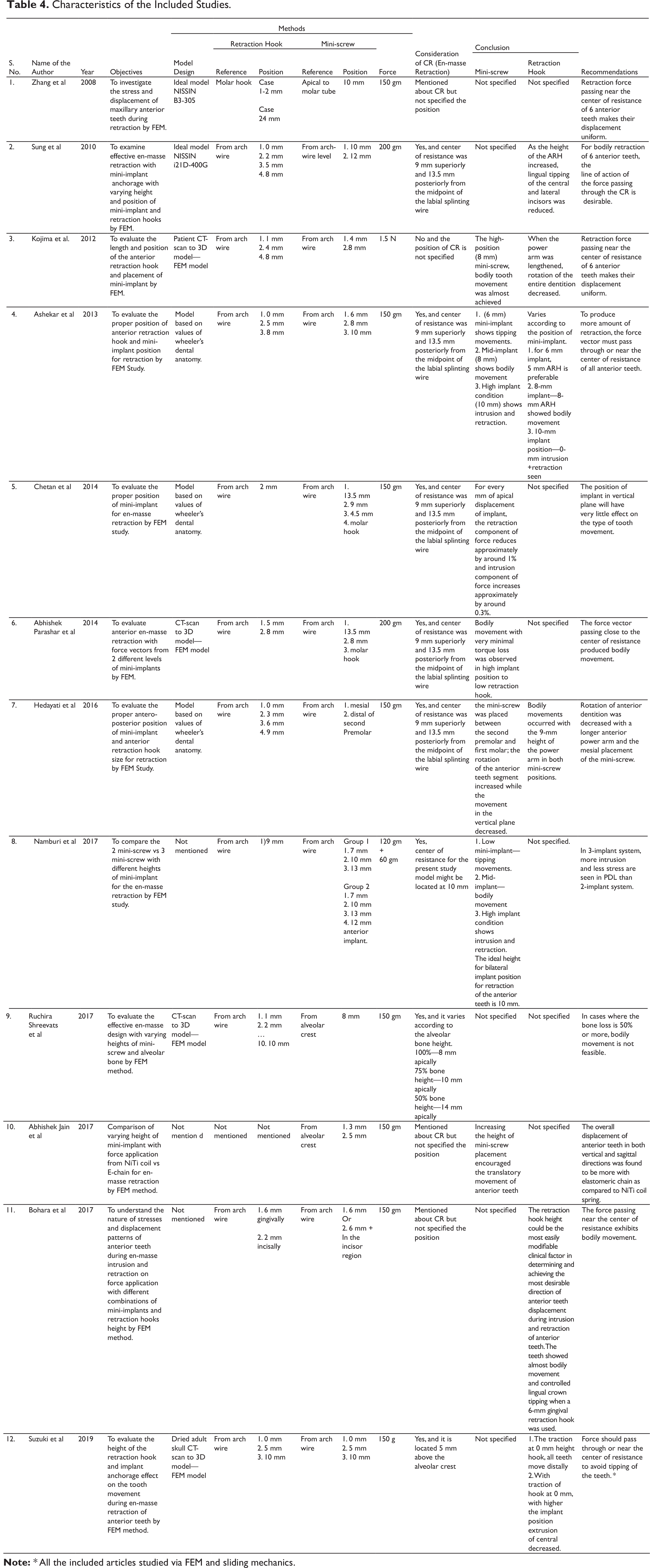
The summary of the included variables is outlined in Tables 3 and 4.
Position of Mini-screw
Basic Characteristics of the Included Studies.
Characteristics of the Included Studies.
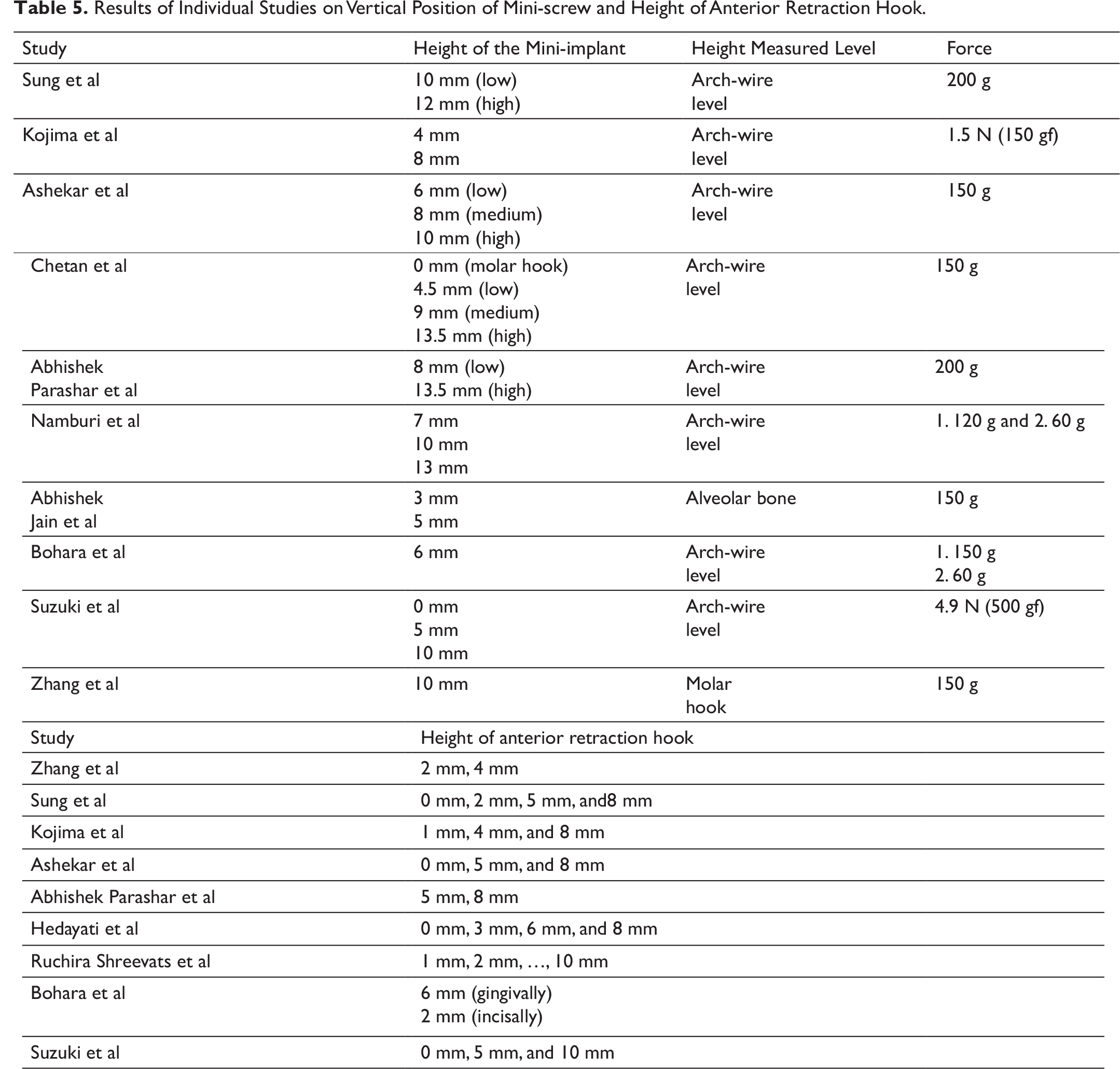
Results of Individual Studies on Vertical Position of Mini-screw and Height of Anterior Retraction Hook.
Position of Anterior Retraction Hooks
A total of 9 articles have considered the varying height of the ARH for en-masse retraction (Table 5). Hedayati et al 19 suggested that placing an ARH size of 9 mm exhibits bodily movement independent of mini-screw position, mesial or distal to premolar. The rotation of anterior dentition was also decreased with a longer anterior power arm. On the contrary, Zhang et al 13 found that when an ARH of 2 mm is used, the lateral incisor showed controlled lingual crown tipping; on the other hand, when an ARH of 4 mm is used, the central and canine teeth showed lingual crown tipping and laterals shows bodily retraction and intrusion.
Tooth Movement
Seven studies had discussed tipping, torque, and translation of incisor while retraction. Parashar et al 18 suggested positioning the mini-implant in a higher position (13.5 mm from the archwire plane) while retraction prevents torque loss and also positioning the mini-screws in a lower position (8 mm from the archwire plane) leads to maximum torque loss. Namburi et al 20 suggested placing mini-screw 10 mm from arch wire as a reference point. Chetan et al 17 suggested the more apical the placement of the mini-screw, the more is the intrusion achieved. Sung et al quoted increasing the length of ARH (<8 mm) reduces unwanted tipping of the central and lateral incisors. Shreevats 21 et al suggested that bodily movement during en-masse retraction is feasible only when 50% alveolar bone height is present in the anterior. In addition to the bilateral implants, an inter-radicular implant in the incisor region reduces the stresses in periodontal ligament (PDL) and achieves greater intrusion in comparison to the 2-implant system. Retraction with elastomeric chain produces lesser amount of von Mises stress on the bone as well as mini-implant and produces more displacement of anterior teeth in both vertical and sagittal directions as compared to that with nickel titanium wire (NiTi) coil spring.
Discussion
At the time of registration with PROSPERO, this systematic review was the first to specifically investigate the position of mini-screw, the height of ARH, and the CR of 6 anterior teeth for en-masse retraction. However, before writing this systematic review, several in-vitro FEM studies were published which have addressed various aspects of en-masse retraction as stated. Studies such as Zhang et al, 13 Sung et al, 14 Chetan et al, 17 Parashar et al, 18 Namburi et al, 20 Jain et al, 22 Shreevats et al, 21 and Suzuki et al 24 have not concluded either optimum position of mini-screw, size of ARH, reference plane to be considered, or the exact position of CR in their respective published articles. To elucidate the above aspects, it was imperative that a systematic review be conducted for discernment. A total of 218 articles were selected using medical subject headings (MeSH) terms, and few articles were handpicked. After regress scrutinization using inclusion and exclusion criteria, 12 articles were finally considered for a systematic review.
Summary of Evidence
The methodological heterogeneity was noted in all these studies. Parashar et al, Sreevats et al, and Bohara et al used MIMICS software for simulation. Zhang et al, 13 Sung et al, 14 Kojima et al, 15 Ashekar et al, 16 Chetan et al, 17 Hedayati et al, 19 Namburi et al, 20 Bohara et al, 23 and Suzuki et al 24 used ANSYS software for simulation, whereas Jain et al have not mentioned the software used for the study. Kojima et al, 15 Suzuki et al, 24 and Parashar et al 18 designed an FEM model based on the CT scan and converted it into a 3D model, while other studies such as Ashekar et al, 16 Chetan et al, 17 and Hedayati et al 19 designed a model based on Wheeler’s dental anatomy textbook. Jain et al 22 and Bohara et al 23 did not quote the model design.
Namburi et al 20 compared the stresses on the 2-implant systems with 3-implant systems for retraction. He stated that the stresses on the hard bone, PDL, and implant showed less stress in 3-implant systems. Zhang et al 13 found more displacement and stress in the cervix and root apex in teeth and also that lateral incisors experience more compressive stress on the labial and lingual surfaces with mini-screw assisted retraction. Jain et al 22 used NiTi coil spring and elastomeric chain on mini-screws for retraction force. They inferred a higher level of Von Mises stresses in bone while using the NiTi coil spring and mini-screw. Sung et al 14 found higher periodontal tensile stress (0.67 g mm−2) on the bucco-cervical third of canine when the force vector passed through CR during en-masse retraction. Bohara et al 23 stated that the nature of stresses changes from tensile to compressive from the cervical area to the apical area while retraction.
The method of retraction and force used for retraction varied in the studies. The force of 150 gm was used in studies conducted by Zhang et al, 13 Ashekar et al, 16 Chetan et al, 17 Hedayati et al, 19 Shreevats et al, 21 Jain et al, 22 Bohara et al, 23 and Suzuki et al. 24 Sung et al 14 and Parashar et al 18 used 200 gm of force and Namburi et al 20 used 120 g for retraction and 60 gm for the intrusion. Jain et al 22 showed the method of en-masse retraction using NiTi spring in comparison with the power chain. Other included studies did not mention the method of retraction.
The positioning of the ARH differed inciso-gingivally and mesiodistally in included studies. Bohara et al 23 compared the position of ARH incisally (inverted) and gingivally with respect to the arch wire. The positioning of ARH in between lateral incisors and canine was common, and this was specifically mentioned in the 12 studies. Zhang et al 13 considered a molar hook for deciding the dimensions of ARH, whereas an arch wire was reported as the reference plane in studies by Sung et al, 14 Kojima et al, 15 Ashekar et al, 16 Chetan et al, 17 Parashar et al, 18 Hedayati et al, 19 Namburi et al, 20 Shreevats et al, 21 and Suzuki et al. 24 Biomechanical effects of different positions of mini-screw were compared with the fixed dimension of ARH by Chetan et al 17 (2-mm ARH), Namburi et al 20 (9 mm), and Bohara et al 23 (6-mm ARH for gingival model and 2-mm ARH for incisal model), respectively, whereas other studies such as those by Zhang et al, 13 Sung et al, 14 Kojima et al, 15 Ashekar et al, 16 Parashar et al, 18 Hedayati et al, 19 and Suzuki et al 24 evaluated different dimensions of ARH with fixed position of mini-screw. Sung et al 14 and Hedayati et al 19 varied the ARH for four different heights. Kojima et al, 15 Ashekar et al, 16 and Suzuki et al, 24 varied the height of ARH thrice in their studies. Zhang et al 13 and Parashar et al 18 changed the height of the ARH twice in their studies. Shreevats et al 21 studied the effects by varying the height of ARH in increments of millimeter. Park et al 25 considered short ARH to increase the vertical component and decrease the horizontal component and vice versa.
In terms of mini-implant, the number of implants, height, and position were discussed. Namburi et al 20 and Bohara et al 23 compared 2-mini-implant models versus 3-mini-implant models for an anterior retraction and showed that the 3-implant system has better biomechanical advantages for better intrusion and retraction and minimum stress on the periodontium. Hedayati et al 19 studied the mesiodistal positioning of the mini-screws by comparing the bio-mechanical effects by placing one implant placed at the mesial and other at the distal of the second premolar. Shreevats et al 21 and Jain et al 22 considered the alveolar crest as a reference point for the mini-screw placement. Zhang et al 13 considered apical to Molar tubes. Park et al 25 took the bracket slot as a reference plane for placement of mini-screw. Studies such as Sung et al, 14 Kojima et al, 15 Ashekar et al, 16 Chetan et al, 17 Parashar et al, 18 Hedayati et al, 19 Namburi et al, 20 Bohara et al, 23 and Suzuki et al 24 had taken arch-wire level as reference. Zhang et al 13 and Shreevats et al 21 placed the mini-implant at a fixed height from the respective reference planes and varied the ARH height. Ashekar et al, 16 Chetan et al, 17 Namburi et al, 20 and Suzuki et al 24 used 3 different implant positions for comparison. Sung et al 14 (10 mm, 12 mm), Kojima et al 15 (4 mm, 8 mm), Parashar et al 18 (13.5 mm, 8 mm), and Jain et al 22 (3 mm, 5 mm) used 2 different implant positions.
The CR is critical for assessing the resultant direction of force for en-masse retraction when applied from mini-screw to ARH. The line of force vector passing through CR will bring about the bodily retraction. Melsen et al 26 considered CR at a point 9 mm superiorly and 13.5 mm posteriorly from the center of the arch wire. The same point is considered in studies by Sung et al, 14 Ashekar et al, 16 Chetan et al, 17 Parashar et al, 18 and Hedayati et al. 19 Namburi et al 20 estimated the location to be at 10 mm from the alveolar bone in between lateral and canine. Suzuki et al 24 considered CR to be at 5 mm above the alveolar crest apically above the central incisor. Zhang et al, 13 Kojima et al, 15 Bohara et al, 23 and Jain et al 22 have mentioned the importance of CR but not specified its location. Shreevats et al 21 discussed CR in relation to periodontally compromised patients. He stated that as the alveolar bone loss increased, the CR moved apically.
Upadhayay et al 27 suggested retraction force to be angulated when applied from mini-screw whereas in the conventional techniques force vector remains parallel to the occlusal plane. Antoszewska-Smith et al 28 stated retraction with mini-screw is more efficient with minimum undesirable effects. Koyama et al 29 and Rizk et al 30 laid stress on en-masse retraction using mini-screw, as it reduces the treatment time period and augments anchorage. Kim et al 31 corroborate the above results by retracting 6 anterior teeth using mini-screws without bonding posterior segments.
Limitations
The FEM model is an emerging diagnostic and investigating method in the engineering and biomedical fields, but the simulation and original result may vary due to clinical and biological factors such as bone level, bone density, age/gender of the patient, and periodontal integrity. The studies included in this systematic review were in English, although few studies in different languages were published but not included, suggesting incomplete data collection and probably publication bias. The 12 articles discussed in the systematic review used FEM as an investigating tool however, the results of these studies were not corroborated with clinical studies under the same orientation of mini-screw and ARH.
Conclusions
According to the currently available literature review for successful bodily en-masse tooth movement, the force vector should pass through CR, which can be achieved by the clinical judgment of placing a mini-screw in the right position and assessing the height of ARH.
The retraction force should pass through the CR, to achieve the bodily movement and controlled lingual crown tipping. The force from an implant placed at a higher level from the ARH will cause intrusion; an implant placed at a medium level shows bodily movement, and an implant placed at a lower level shows tipping forces in consolidated arches. The use of an extra implant in the incisor region improves intrusion and reduces stress in the periodontal ligament.