
Abstract
Introduction:
The objective of the study was to assess the rate of canine retraction and secondary outcomes associated with conventional fixed orthodontic treatment (CFO) and CFO with micro-osteoperforation (CFO + MOP), that is, anchorage loss, root resorption, vitality of tooth, pain and discomfort level during the procedure.
Methods:
A total of 16 patients with Class II Division 1 malocclusion who required upper first premolar extraction with lower non-extraction/single incisor extraction were divided into the test group (MOP) and positive control group (CFO + MOP) for a split-mouth study. Both maxillary canines were retracted with nickel–titanium (NiTi) closed coil springs. Patients were reviewed after 24 hours, 7 days, 28 days, and 4, 8, and 16 weeks to assess the rate of tooth movement, anchorage loss, root resorption, vitality of tooth, pain and discomfort level.
Results:
There was a statistically significant difference in the rate of tooth movement between the CFO and CFO + MOP groups after the first 4 weeks (P-value = .026), whereas no statistically significant difference was observed at 8, 12, and 16 weeks (P-value = .33, .99, and .08, respectively). In the CFO group, there was no statistically significant difference in tooth movement between different time intervals (P-value > .05). There was no significant difference in root resorption between the groups. The pain level was higher in the MOP group in the first 24 hours (P-value < .05) after the procedure. Later on, the difference in pain level between the groups was not significant (P-value > .05). The vitality of retracted canines in both groups was healthy.
Conclusion:
The study recommends that the CFO + MOP procedure has substantial potential to be used as an adjunct to the routine mechanotherapy for faster tooth movement, as it may reduce the treatment time by half in the first 4 weeks after the MOP procedure. There are no potential differences in anchorage loss, tipping, vitality, and apical and lateral root resorption between the CFO and CFO + MOP groups. This trial was registered at Clinical Trial Registry, India.
Keywords
Introduction
A common problem associated with adults during orthodontic treatment is the prolonged treatment time. 1 In recent times, significant changes have been witnessed in the mechanotherapy and appliance system.
The standard orthodontic treatment period is usually up to 20 to 24 months.2, 3 Various innovations have been made in recent years to create different approaches to reduce the treatment time without compromising the treatment result.1, 4, 5 They can be broadly classified into biological, device-assisted, and surgical approaches. Biological and device-assisted approaches have been experimented with using animals, and further studies are being done to achieve better results in humans.4, 5 Surgical approaches induce a localized inflammatory response, which encourages local recruitment and stimulation of osteoclasts that enhance remodeling.6, 7 They have shown better results with regard to decreased treatment time.8-12
Micro-osteoperforation (MOP) is considered the least invasive surgical technique to reduce the duration of conventional fixed orthodontic treatment (CFO). It involves multiple transmucosal perforations within the alveolar bone, placed close to the region of desired tooth movement, with a specific configuration depending on the tooth movement required.
Studies by Alikhani et al, 13 Khan et al, 14 and Feizbakhsha et al 15 were of the opinion that the rate of tooth movement associated with MOP increased by 2 to 3 times, and significant results were also noted 16 when MOP was compared with the conventional method. Contradictory to the above studies, the current article suggests a lack of conclusive evidence regarding the effectiveness of MOP in increasing the rate of tooth movement.17, 18 This may be due to the limited study duration or the impact of tipping as a part of the treatment.19-21 Hence, newer studies are required to understand the clinical effectiveness of MOP.22, 23
The present study investigated the effect of MOP during canine retraction with fixed orthodontic appliances. A randomized clinical control trial was performed, with a focus on canine retraction within the maxilla following the extraction of first premolar teeth, to assess the effect of MOP on the rate of tooth movement during canine retraction after 16 weeks, in comparison to that of the randomly allocated control group. The secondary outcomes expected were anchorage loss, root resorption, and canine tipping in both the MOP and control groups, which were evaluated before treatment, after 28 days, and after completion of canine retraction on both sides. The pain and discomfort level of the participants during the treatment period was also appraised as a secondary outcome.
Material and Methods
Trial Design
The study was a single-centered, split-mouth randomized control trial to investigate the effectiveness of (minimally invasive) MOP therapy on the rate and amount of orthodontic tooth movement and secondary outcomes.
Participants, Eligibility Criteria, and Settings
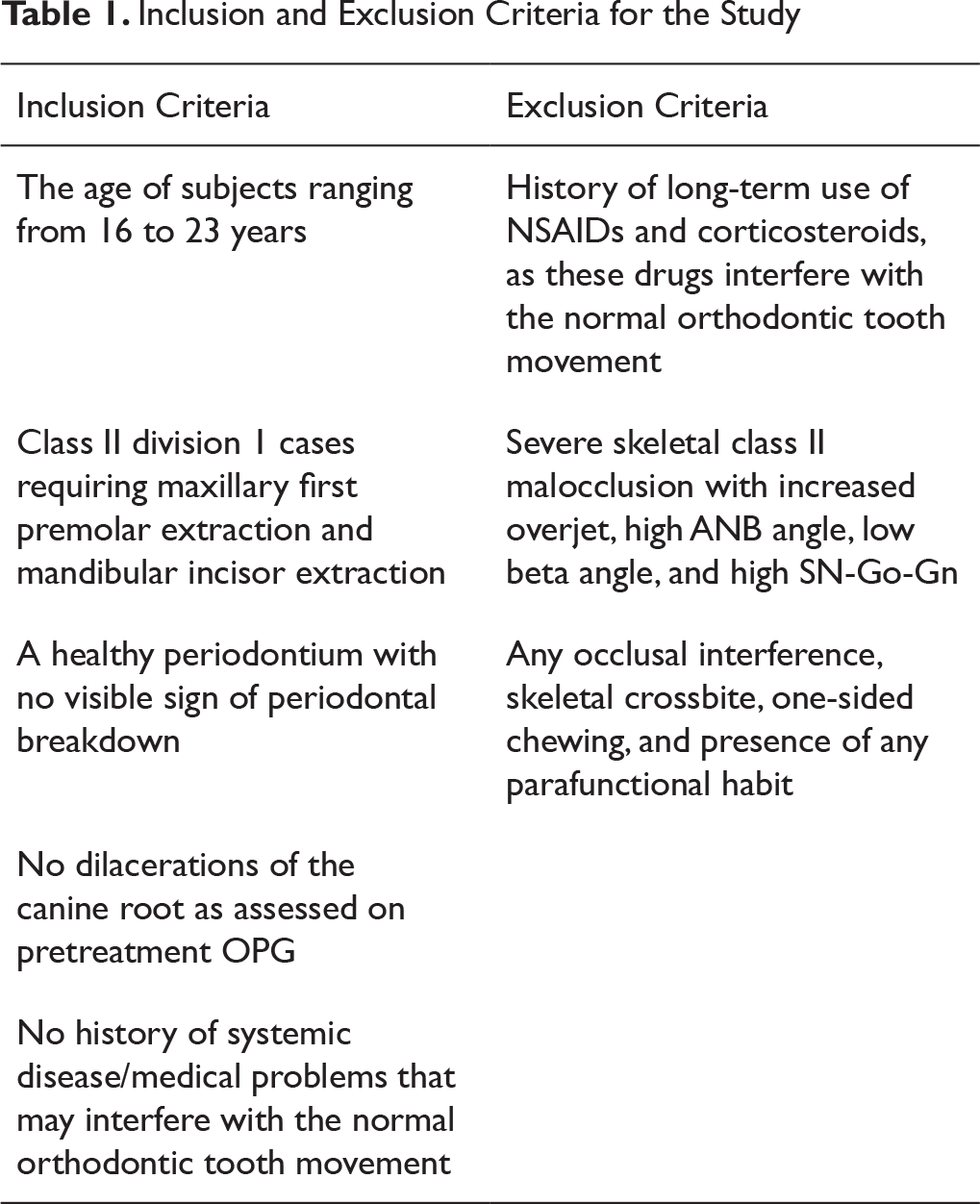
The sample comprised patients who were undergoing comprehensive fixed orthodontic treatment with premolar extraction. Subjects who fulfilled the inclusion criteria (Table 1) were randomly allocated to 1 of the 2 groups. The lottery method of the simple random sampling technique was followed after informed consent was obtained from all the study subjects.
On the one side was the test group (MOP), and on the other side was the positive control (CFO) group. A total of 16 subjects were included in the study, and overall 32 canine retractions were undertaken for assessment (16 for CFO + MOP and 16 for CFO).
Sample Size
A pilot study was done to determine the sample size of the 2 different groups of the study. The values obtained from each group were calculated and the effect size was obtained using G* power 3.1.9.2. Subsequently, we obtained a sample size of 13 per group. To avoid unexpected errors, outcomes and dropout, the size was rounded up to 16 per group.
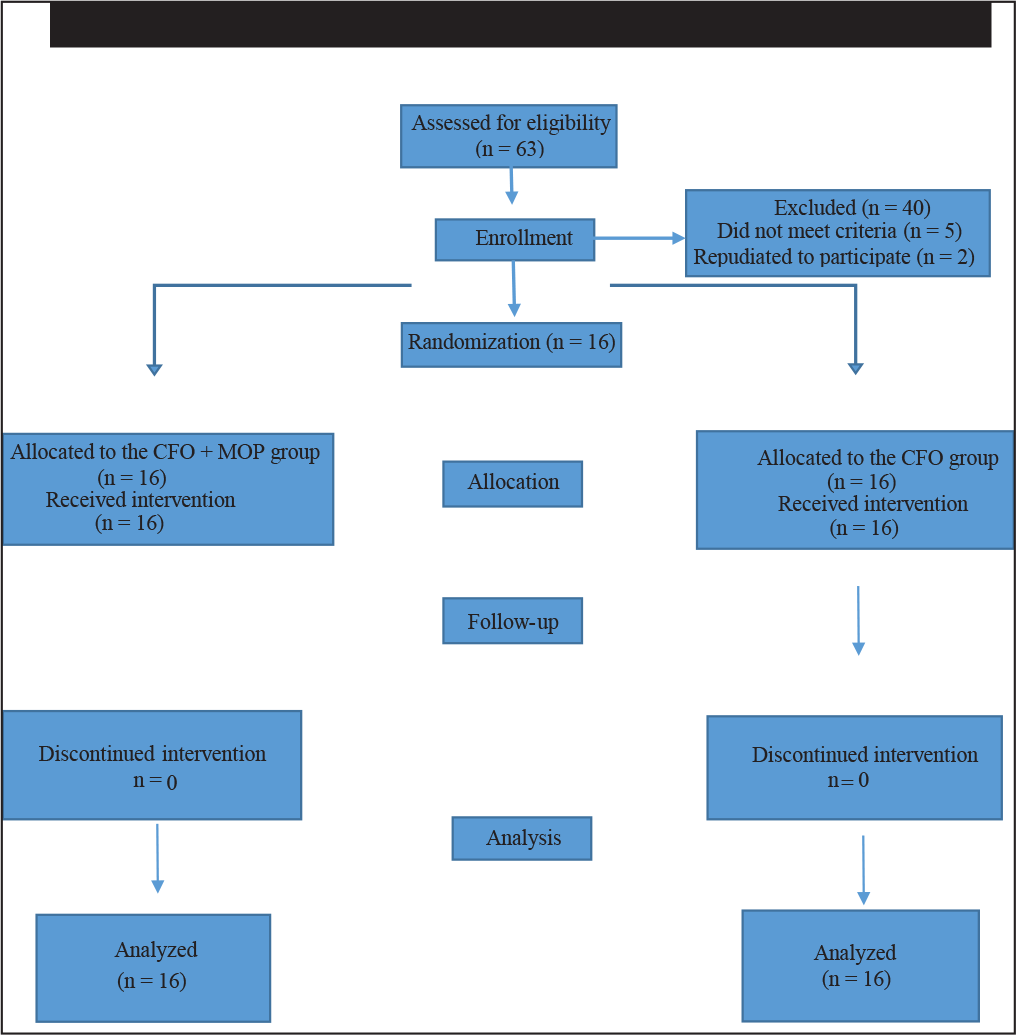
The samples were split into 2 groups in which interventions were carried out (Figure 1):
Group 1: Among the patients in this group, the conventional method of CFO was used for canine retraction (frictional mechanics).
Group 2: Among the patients in this group, canine retraction was done with CFO + MOP.
Inclusion and Exclusion Criteria for the Study
Interventions
Treatment was initiated using fixed preadjusted appliance (0.022-MBT prescription; 3M UnitekTM Gemini, Monrovia, CA). The standardized bonding system was enforced as per the manufacturer’s information (Figure 2A). A transpalatal arch was placed to prevent unwanted movement of posterior teeth, and second premolars were passively ligated to enhance anchorage during canine retraction. All extractions of maxillary first premolars had been performed 6 months earlier in the Oral and Maxillofacial Surgery Department by the same surgeon, to decrease the chances of unevenness. 24 After that, leveling and alignment were done, and the retraction of the canines was delayed until the wire sequence reached a wire size of 0.019 in × 0.025 in stainless steel. Checks for the presence of any occlusal hindrance were made at regular intervals, and if hindrance was present, the bite was raised with the use of Anabond Blu-Bite on the mandibular molars. 25
Before the procedure, the patients were asked to rinse their mouth with 15 mL of chlorhexidine oral solution for 30 s; the area was wiped with a wet gauge to remove excess saliva (Figure 2B). MOP was performed with the handheld orthodontic micro-implant appliance LH 1514-10 (Dentos AbsoAnchor® system) of the long-head (LH) type (with diameter 1.5 mm and length 10 mm) (Figure 2C).
(A) Leveling and Alignment; (B) Part Preparation for MOPs Distal to Canine; (C) Orthodontic Microimplant (Dentos AbsoAnchor®system); (D) MOPs Application; (E) Three MOPs Visible Distal to the Canine
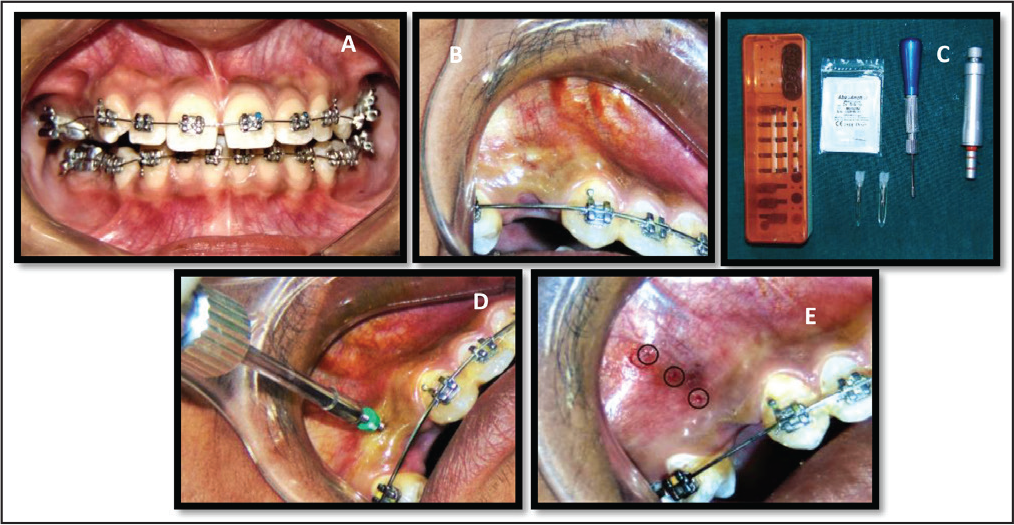
In the split-mouth design, on the test side (CFO + MOP), the procedure was programmed under local anesthesia (2% lidocaine, 1:100,000 epinephrine). Three small MOPs of 1.5 mm diameter and 3 to 5 mm depth, 5 mm away from the free gingival margin, were made on randomly selected experimental sites in the extraction space, and the depth confirmation was done by using a rubber stop (Figures 2D and 2E). No flap was raised, and no analgesics or antibiotics were prescribed, as all necessary sterilization protocols were followed during the procedure.
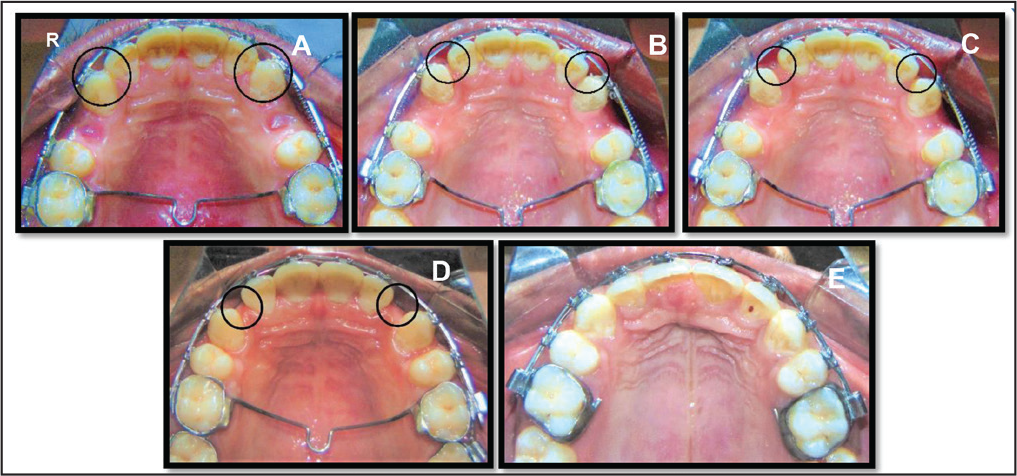
In the positive control side (CFO) and test side (CFO + MOP), canine retraction was initiated with nickel–titanium (NiTi) closed coil springs (3M Unitek; 9 mm) connected from the first molar to the hook of the canine bracket. A force of 150 g was delivered for the canine retraction and calibrated with a force gauge, that is, a dynamometer (Ortho Quest; Nexa Dental, La Vista, NE, USA). The patients were reviewed after 24 hours, 7 days, 28 days, and 4, 8, 12, and 16 weeks to assess their oral hygiene, rate of tooth movement, anchorage loss, root resorption, vitality of tooth, pain and discomfort level (Figures 3A-3E).
Records and Data Collection
Determination of Rate of Canine Retraction and Anchorage Loss
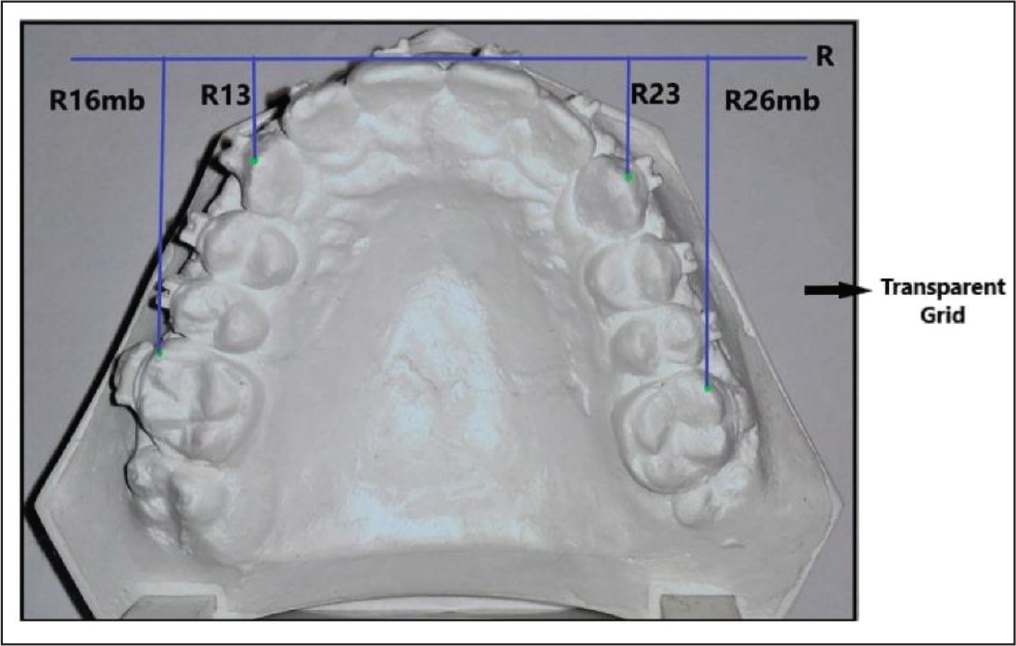
The magnitudes of canine movement and posterior anchorage loss were acquired using 2 predetermined reference points as described by Haas and Cisneros 26 and Hoggan and Sadowsky 27 (Figure 4). Reference points and lines were drawn for the measurements to be performed on the study casts. Reference plane ‘R’ was formed by plotting tangents to the interdental contact point of the upper central incisor, which is also perpendicular to the lower border of the transparent grid. The perpendicular distances from the cusp tip of the upper canine and the mesiobuccal cusp tip of the upper first molars to the reference line were measured (Figure 4). Further, with the help of a transparent grid, the amount of canine and molar movement in the model analysis was calculated.
Determination of Root Resorption (Apical and Lateral) in Canine
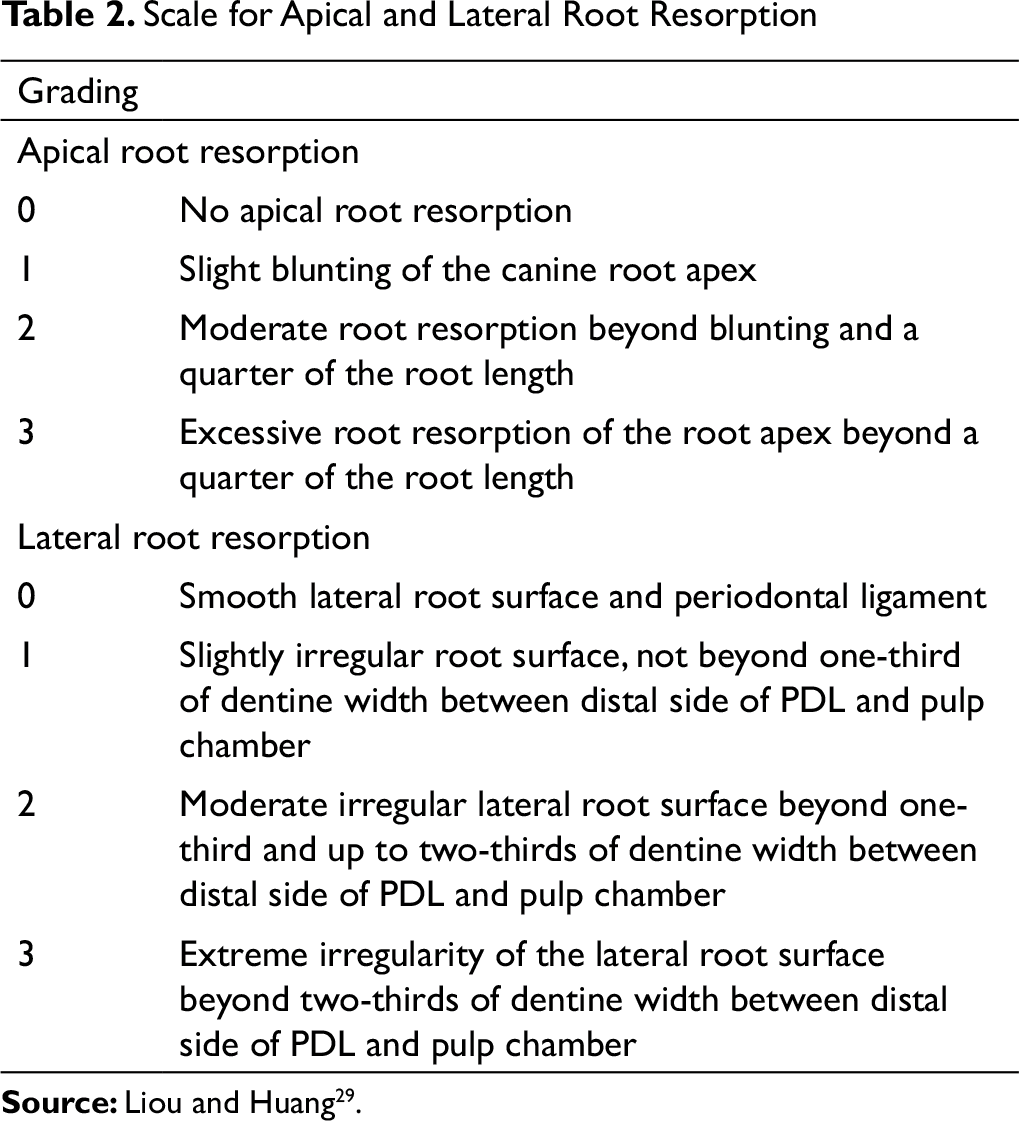
The magnitude of root resorption was evaluated with periapical radiographs conducted on all patients, before and just after 16 weeks of canine retraction in both groups, with a standardized periapical X-ray machine and developer (INTRASKAN DC: ISDC, Skanray Technologies Pvt. Ltd, Made In India, Periomat Plus: Automatic intraoral periapical (IOPA) X-Ray Developer). The long-cone paralleling technique was used to obtain all IOPAs with Octa X-ray film positioner extension cone paralleling (XCP), and standardization was maintained by using a similar guideline for each X-ray before and after 16 weeks of canine retraction, as suggested by White and Pharoah. 28 An experienced periodontist evaluated all the periapical radiographs, and the Mann–Whitney test was performed on the data obtained, through using a scale described by Liou and Huang 29 (Table 2). The present study incorporated a single standardized method for the evaluation of root resorption. 29 A periapical X-ray was done just before premolar extraction and after the completion of canine retraction in all the patients. The X-rays were projected on a screen and magnified by 10 times, and qualitative assessment was done.
Determination of Pain and Discomfort Level and Vitality Test
Scale for Apical and Lateral Root Resorption
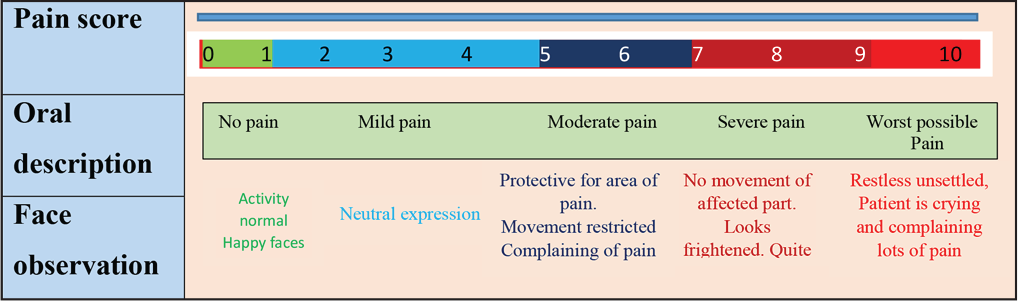
VAS Scale
An electric pulp vitality test (Waldent Electric Pulp Tester, India) was performed just before and after either procedure. A pulp tester probe was placed against the incisal/occlusal one-third of the tooth surface. Signs of pain, with an ascribed number on the scale, were registered with the gradual increase of current (mA) in each participant, at regular time intervals. Each tooth was tested twice and the arithmetic means calculated and indexed in the patients’ charts.
Statistical Analysis
Sixteen subjects who fulfilled the inclusion criteria were selected for the study. The sites were randomly allocated for CFO treatment with or without MOPs, to either the right or left side, with a 1:1 allocation ratio. All the data were entered in Excel sheets and were subjected to statistical analysis using SPSS software for Windows (ver. 26, SPSS, Chicago, IL). The rate of tooth movement and anchorage loss between sites were analyzed using unpaired t-tests. Tooth (canine) movement at the test sites at different time intervals was analyzed using repeated measures analysis of variance (ANOVA). The differences in pain and root resorption between the sites were analyzed using the Mann–Whitney U Test. The lateral and apical root resorption at the CFO and CFO + MOP sites was analyzed using the chi-squared test, and P < 0.05 was considered as statistically significant.
Results
Rate of Orthodontic Tooth Movement
Tooth Movement in the CFO and CFO + MOP Groups
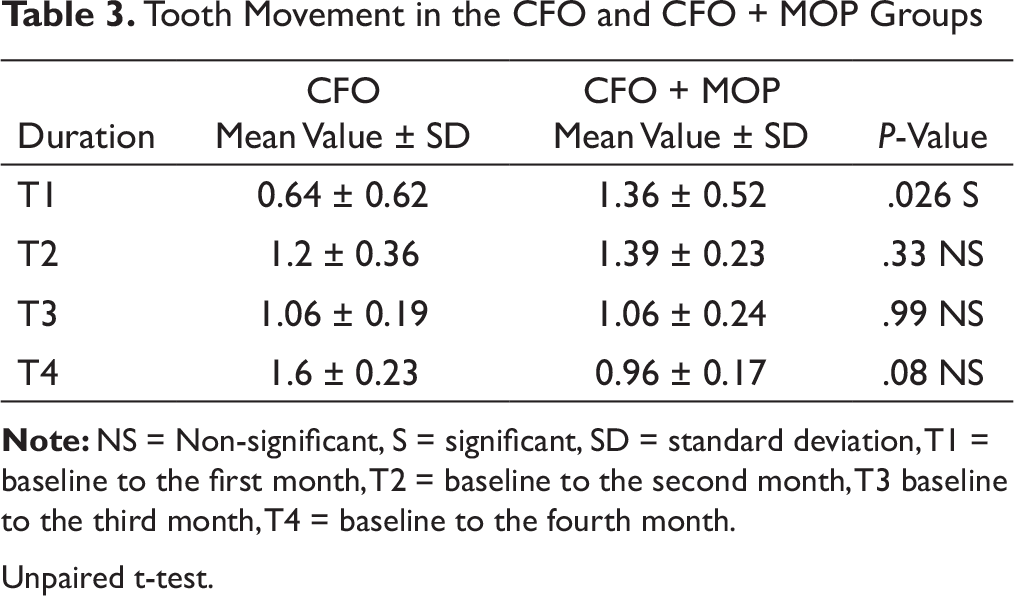
Unpaired t-test.
Comparison of Tooth Movement From the Baseline to 1, 2, 3, and 4 Months in the CFO Group, With Mean, Standard Deviation, P-value, and 95% Confidence Intervals
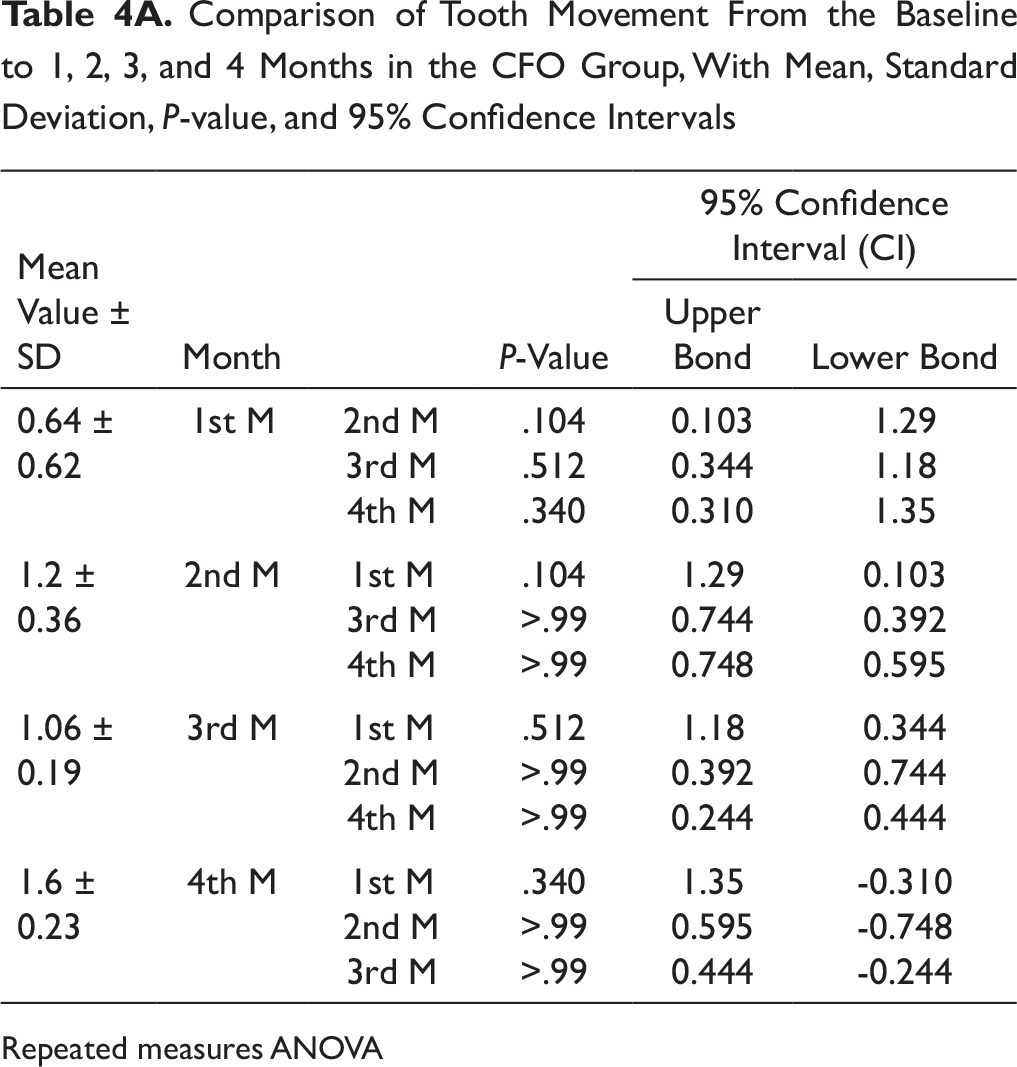
Repeated measures ANOVA
Comparison of Tooth Movement From the Baseline to 1, 2, 3, and 4 Months in the CFO + MOP Group, With Mean, Standard Deviation, P-value, and 95% Confidence Intervals
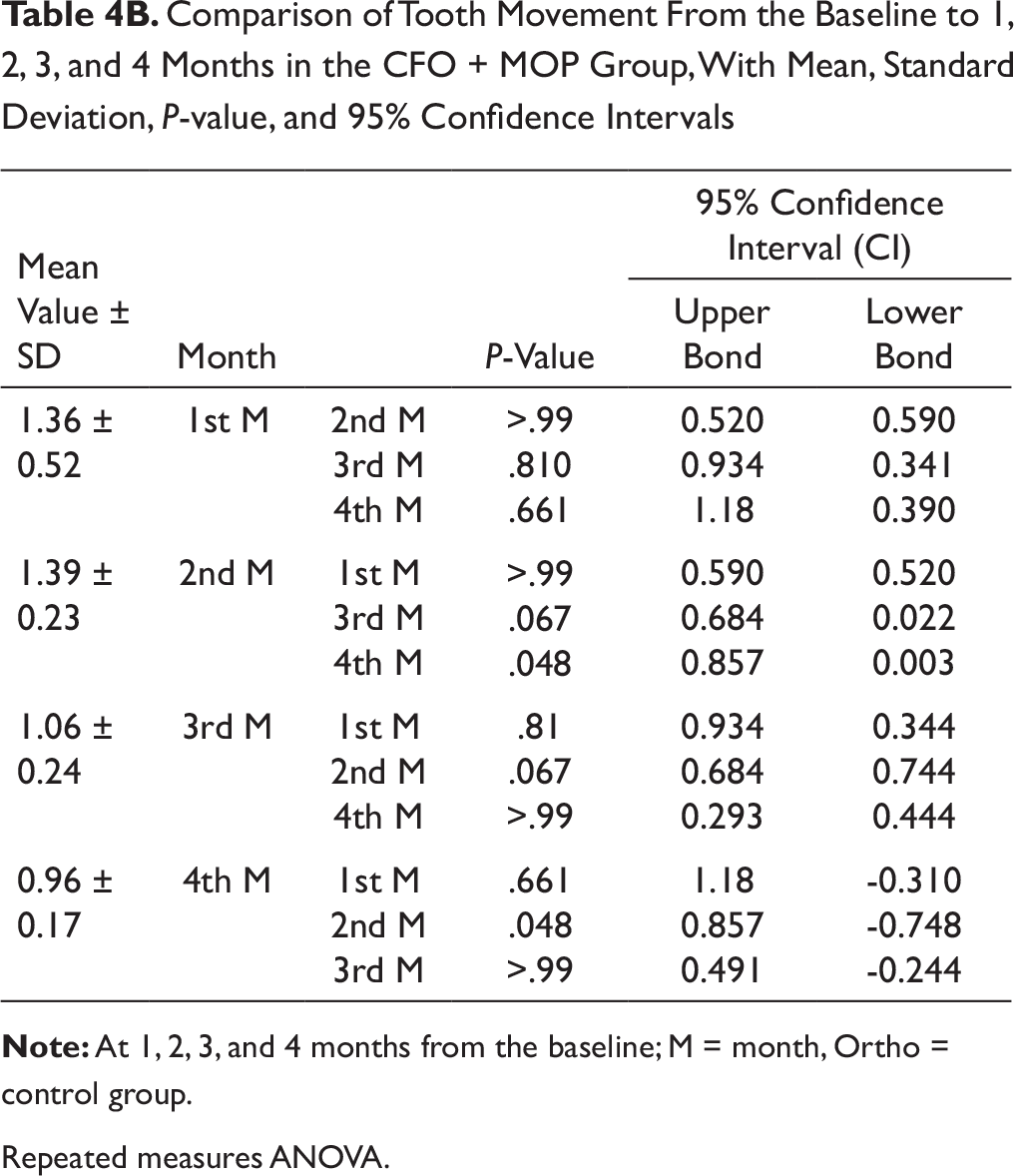
Repeated measures ANOVA.
Anchorage Loss
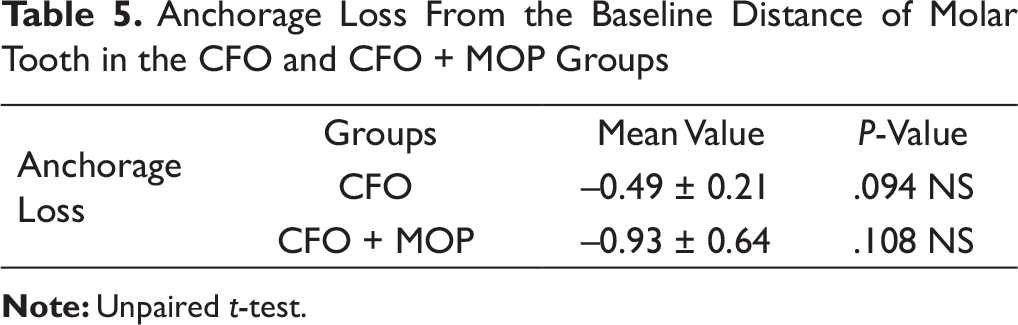
Based on the unpaired t-tests, there was no statistically significant difference in anchorage loss, rotation, and tipping between the two groups from the baseline up to 16 weeks (P-value = .094 and .108) (Table 5).
Root Resorption
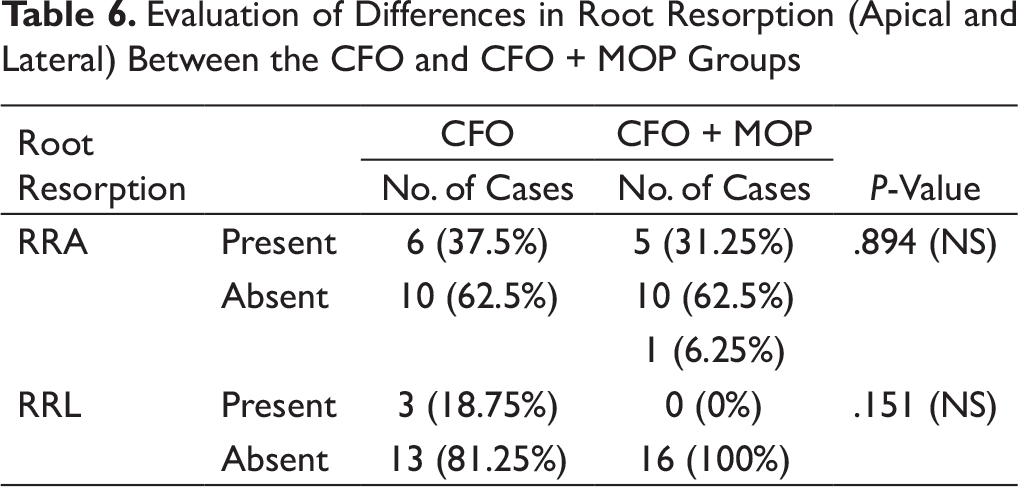
There was no significant difference in apical and lateral root resorption between the groups. Whereas none of the samples in the CFO + MOP group had lateral root resorption, in the CFO group, 18.75% had lateral root resorption, but the difference was statistically insignificant (Table 6).
Pain, Discomfort, and Vitality
Anchorage Loss From the Baseline Distance of Molar Tooth in the CFO and CFO + MOP Groups
Evaluation of Differences in Root Resorption (Apical and Lateral) Between the CFO and CFO + MOP Groups
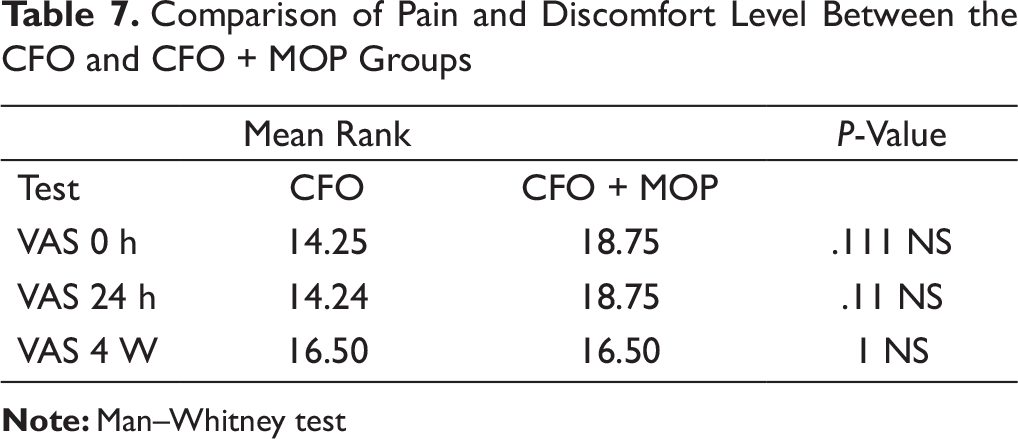
Comparison of Pain and Discomfort Level Between the CFO and CFO + MOP Groups
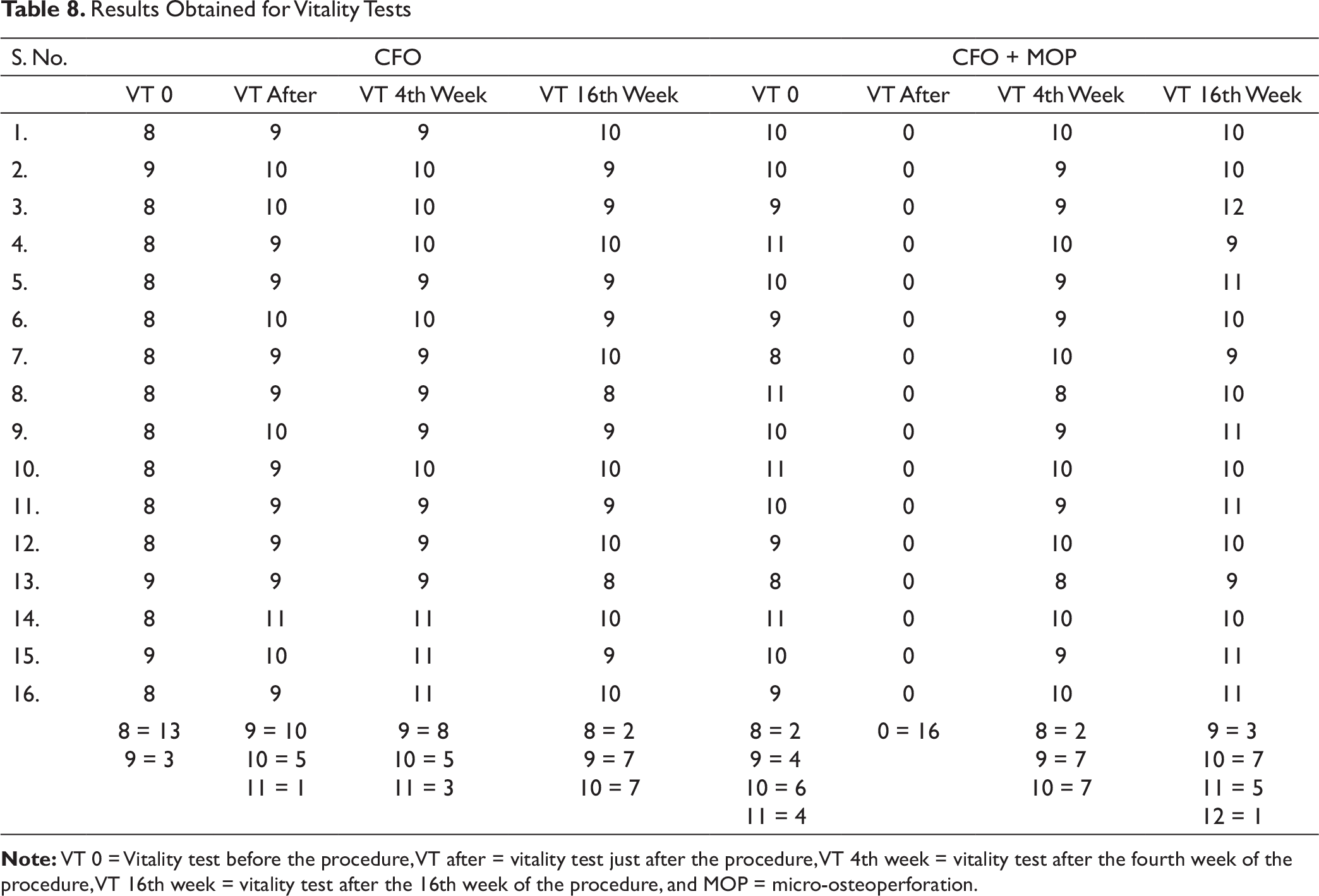
The vitality of the retracted canines was healthy in both groups according to the result obtained from the electric pulp vitality test that was performed just before and after the procedure (Table 8).
Discussion
A split-mouth randomized clinical trial was designed to predict the difference in the rate of movement of maxillary canines between the CFO and CFO + MOP groups. Sixteen subjects (32 canines) were randomly assigned to the two groups for intervention in either the left or right side in the extracted maxillary first premolar space, with an allocation ratio of 1:1.
Previous researches on the acceleration of canine retraction have shown that the changes in the canine retraction devices have been done along with fixed orthodontic components,30, 31 including conventional NiTi closed coil springs. Samuels et al 32 suggested that 150 g of force is sufficient for space closure for sliding mechanics. Dixon et al 33 observed that the rate of canine retraction with NiTi closed coil springs was 0.81 mm/month. Cacciafesta et al 34 reported a 1.1 mm/month canine movement. Nightingale and Jones et al 35 illustrated a canine movement of 0.21 mm/week using a power chain. Shanker et al 36 noted tooth movements of 2.14 mm, 1.99 mm, and 1.87 mm at 1, 2, and 3 months, respectively.
The present study investigated tooth movement over 16 weeks in both groups. The tooth movements noted in the CFO group at regular intervals were 0.64 ± 0.62 mm, 1.2 ± .36 mm, 1.06 ± 0.19 mm, and 1.6 ± 0.23 mm at 1, 2, 3, and 4 months, respectively. The rate of canine retraction was noted to be slow during the first month and higher in the following weeks. The results of the present study are similar to those of the studies quoted above.34-36 In the CFO + MOP group, the observed tooth movements were 1.36 ± 0.52 mm, 1.39 ± 0.23 mm, 1.06 ± 0.24 mm, and 0.96 ± 0.17 mm at 1, 2, 3, and 4 months, respectively. There was a statistically significant difference in the tooth movement during the first month between the CFO and CFO + MOP groups (P-value = .026). A change in the rate of tooth movement was also noted between the second and fourth months in the CFO + MOP group. This may have been because of the fact that canine retraction in the MOP side was completed earlier than that in the CFO side (Tables 4A and 4B).
Results Obtained for Vitality Tests
In the present study, the total magnitude of tooth movement was noted to be higher in the CFO + MOP group throughout the study period. An increase in the rate of tooth movement was seen in the first month, whereas the rate of tooth movement progressively slowed down to become similar to that of the CFO group across the remaining 3 months, since the expression of inflammatory markers decreased with time, similar to findings reported by Alikhani et al 13 in their study.
Most of the studies that used an absolute anchorage system by placing miniscrews to facilitate the canine retraction procedure, through using NiTi closed coil springs, reported no anchorage loss.13, 17, 18 In the present study, the posterior anchorage was augmented with a transpalatal arch in the maxilla during canine retraction, which was kept standard for all the cases. In previous studies by Bokas and Wood, 37 a transpalatal arch was used as an anchorage reinforcement unit, and anchorage loss was noted as 0.46 mm/month. In a recent study by Davis et al 38 without any anchorage reinforcement and using only the molars and premolars as anchor units, anchorage loss was noted to be 1.3 mm during canine retraction. In the present study, anchorage loss from the baseline was noted to be 0.49 ± 0.21 mm in the CFO group and 0.93 ± 0.64 mm in the CFO + MOP group. Though the difference between the groups was appreciable, it was not statistically significant (P-value = .094 and .108). The results of the present study are similar to those of the studies quoted above (Table 5).
Achieving the highest rate of tooth movement with minimal iatrogenic side effects is the common goal of orthodontists with a good understanding of “optimal” force magnitude.32, 33 A force of 150 g was employed in the present study, similar to the force applied by many other authors, ranging from 100 g to 200 g, for canine retraction.32, 36, 37 Boester and Johnston 39 found that a retraction force of 150 g resulted in the highest canine retraction rate. Ren et al 40 found no conclusive evidence regarding the optimal force level. Still, there is an unacceptable risk of orthodontics-induced inflammatory root resorption present with a long duration of treatment.
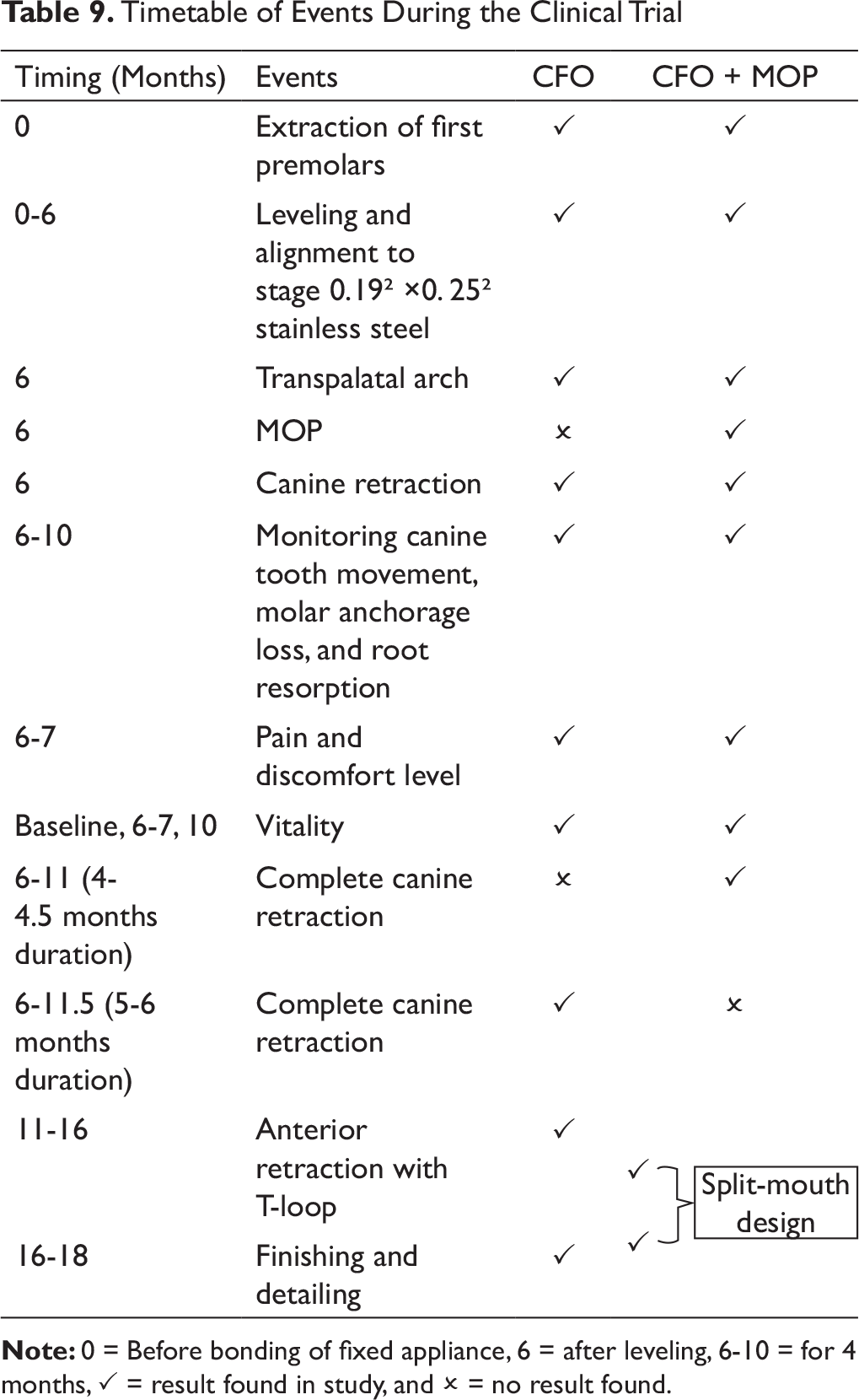
Timetable of Events During the Clinical Trial
Whereas in the present study, Grade 1 apical root resorption was noted in 37.5% cases in the conventional group and 31.25% cases with Grade 1, 6.25% case with grade 2 in CFO+MOPs group which was statistically not significant (P-value = .894). Lateral root resorption was not seen in CFO cases, whereas 18.75% of the cases in CFO + MOP showed Grade 1 lateral root resorption with a P-value of .151, which was statistically insignificant. This result is similar to that of the studies by Mani Alikhani et al 13 and Alkebsi et al. 18
Pain and inconvenience are typical antagonistic impacts related to orthodontic treatment. 44 Past examinations have demonstrated that 70% to 95% of orthodontic patients experience pain.5, 45, 46 This pain could be an explanation behind the attrition of subjects seeking orthodontic treatment; past investigations have demonstrated that 8% and even up to 30% of orthodontic patients discontinue treatment as a result of pain and discomfort. 44 According to our study findings, the pain level was higher in the CFO + MOP group in the first 24 hours (P-value = .111) after the procedure; however, it was not statistically significant. The pain level became the same across the CFO and CFO + MOP groups after 4 weeks (P-value = >.99).
The vitality47, 48 of the retracted canines in both groups was found to be clinically healthy according to the results obtained from the electric pulp vitality test that was performed just before and after the procedure.
Conclusion
From the present study, it can be concluded that the CFO + MOP procedure has substantial potential to be used as an adjunct to the routine mechanotherapy for faster tooth movement, as it may reduce the treatment time by half in the first 4 weeks after the MOP procedure. There are no potential differences in anchorage loss, tipping, vitality, and apical and lateral root resorption between the CFO and CFO + MOP groups.
Although MOP can reduce the duration of orthodontic treatment by accelerating canine retraction in extraction patients without undesirable side effects, there are some drawbacks associated with it, including the need for a specific surgical procedure, a little discomfort felt by the patient in the first 24 hours, supervised activation protocol, the need for individual devices and knowledge of MOP application and timing (Table 9). It is recommended that the various factors mentioned in this study and the level of inflammatory markers be taken into account and discussed in future studies.
Footnotes
Declaration of Conflicting Interests
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Necessary ethical clearances obtained from institution Dean/2018/EC/376; informed consent was taken before initiating study procedures from all participants.