
Abstract
Background and Objectives:
This study was conducted to assess the effect of light-curable fluoride varnish on enamel demineralization adjacent to orthodontic brackets using polarized light microscopy and to compare the depth of demineralization at different time periods.
Method:
In 15 patients, the first premolars were allocated into 2 groups. In the experimental group light-curable fluoride varnish was applied. At the end of each time period (60, 90, and 120 days), first premolar brackets were debonded and premolars were extracted. Buccolingual sections were evaluated under a polarized light microscope and depth of demineralization was assessed.
Results:
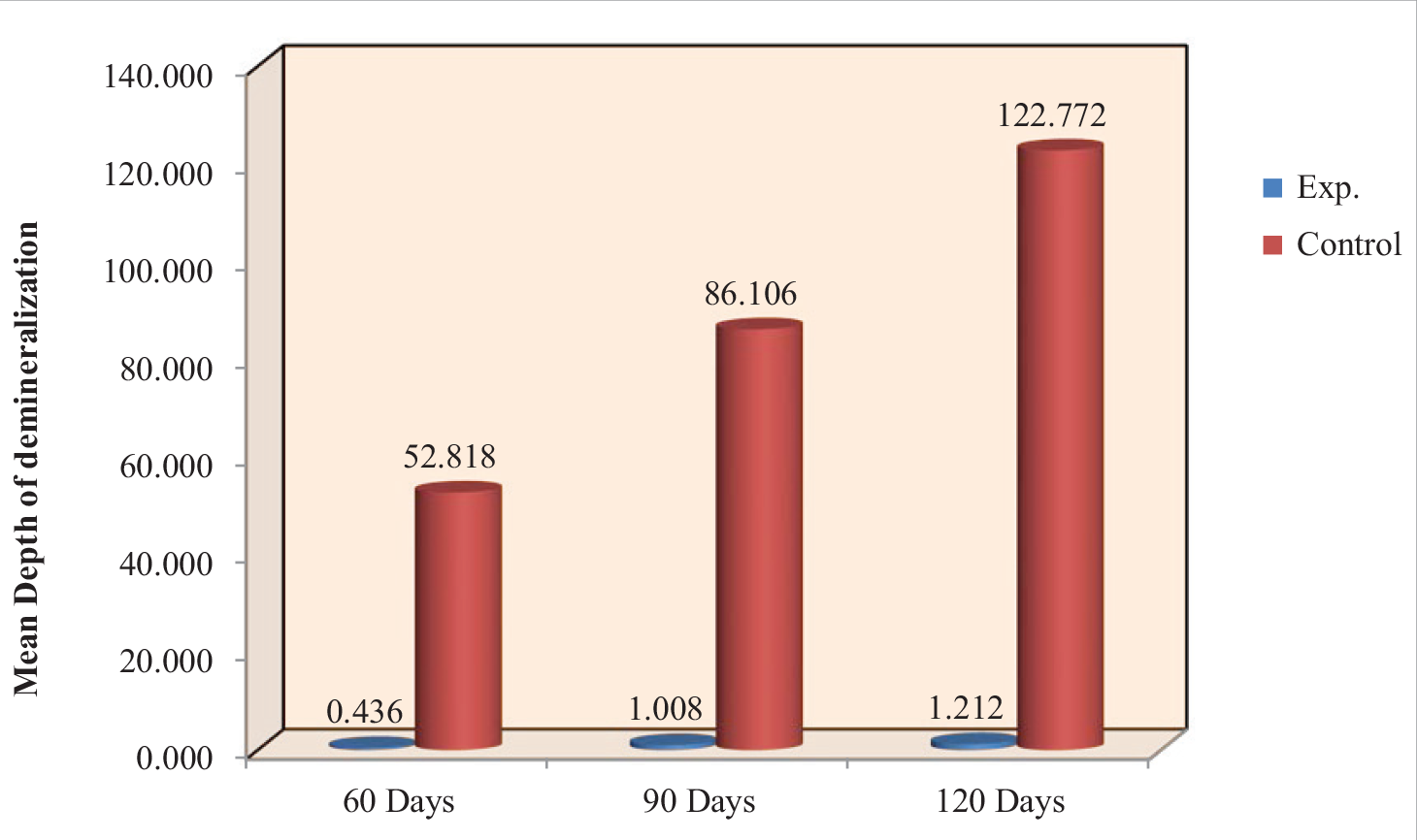
The depth of demineralization in the control group increased from 60 to 120 days, and the experimental group did not show any significant difference during the time period.
Conclusion:
Single application of light-curable fluoride varnish, Clinpro XT can be effective in reducing enamel demineralization during fixed orthodontic mechanotherapy, especially in noncompliant patients.
Introduction
In fixed orthodontic treatment, the chance of occurrence of white spots is comparatively more and is a matter of concern. There are mainly two contributing factors for enamel demineralization, which include the complex structure of orthodontic brackets and etching of enamel for bonding orthodontic brackets. A white spot lesion is defined as “subsurface enamel porosity from carious demineralization,” which presents itself as an opaque milky white surface. During fixed appliance orthodontic therapy, dental plaque accumulation is more, and the pH of plaque is less compared to non-orthodontic patients, and levels of acidogenic bacteria like Streptococcus mutans and Lactobacillus are also increased.
As the pH of plaque drops below the threshold of remineralization, the process of demineralization starts to occur. The lesion starts with dissolution of hydroxyapatite crystals from the enamel prisms that form the superficial surface of the enamel. At a certain point of time, the demineralization appears clinically as white spot lesions. The periphery of orthodontic brackets becomes a responsive site for plaque retention; hence, there is an increased risk for enamel demineralization. 1 The occurrence of white spot lesions in patients receiving fixed appliance treatment is up to 50% and can be seen 1 month post starting orthodontic therapy when no preventive fluoride programs are used.
Once the lesion is established, it may lead to various subsurface lesions, which are difficult to be controlled. The teeth which are commonly affected by white spot lesion include maxillary lateral incisors and mandibular canine, even though there is a generalized distribution of white spot lesion, and the distogingival part of the labial surface is more prone to demineralization. 2 There are many methods to prevent enamel decalcification, which include maintaining proper oral hygiene by following proper brushing techniques, modifying the diet by reducing carbohydrate intake, and applying prophy powder, prophy paste, fluoride paste. 3
Varnishes provide a high fluoride concentration to prevent demineralization. The adherence of varnish to teeth is more compared to topical fluorides, which show increased ability of enamel for fluoride uptake. 4 Compared to other sources of fluoride applications such as monofluoride phosphate dentifrices, acid phosphate fluoride gel, and fluoride rinse, fluoride varnish permits incorporation of more fluoride due to prolonged contact time with the tooth surfaces. Vivaldi-Rodrigues et al reported trimonthly application of fluoride varnish after orthodontic treatment reduced the white spot lesion incidence rate by around 44%. Teeth that had been previously subjected to fluoride varnish around composite resin-bonded orthodontic brackets showed 35% reduction in the depth of the demineralized lesion. 5
Certain kinds of light-curable fluoride varnish remain intact to the tooth surface for a longer duration compared to regular fluoride varnish and can resist tooth abrasion caused by brushing and wear for 6 months or more; moreover, it helps in remineralization. The purpose of this study is to find out the effectiveness of a single application of highly filled resin-modified glass ionomer-based light-cure fluoride varnish on enamel decalcification around orthodontic brackets by using polarized light microscopy.
Materials and Methods
Fifteen patients whose fixed orthodontic treatment involved all first premolar extraction were recruited for the study. The study was designed such that for each patient, the first premolars were allocated to either the control group or the experimental group. Total sample size is 15 patients (4 first premolars each patient)—control group 30 teeth and experimental group 30 teeth.
The experimental group was treated with light-curable fluoride varnish, Clinpro XT. (Figure 1). Non-randomized split-mouth design was used, in which diagonally opposite quadrant received the same treatment. Every alternate patient received the same application pattern in the respective quadrant.
Single blinding was done in this study. The patients were not aware of the intervention being done.
Light-Curable Fluoride Varnish, Clinpro XT
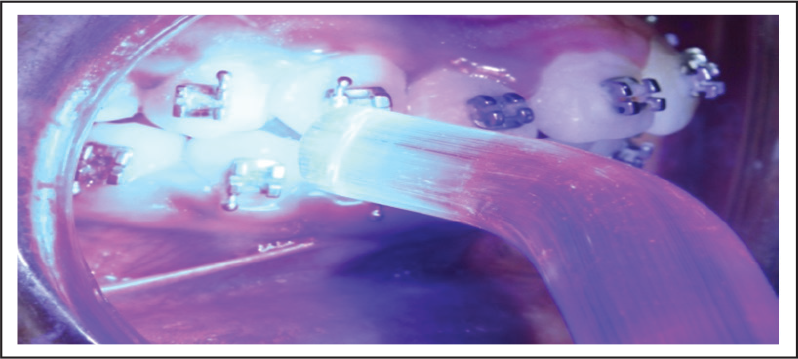
Light-Curable Fluoride Varnish, Clinpro XT Was Applied on the Buccal Surface and Light-Cured for 20 s
After cleaning the tooth with non-fluoridated pumice paste, enamel surfaces were etched with 37% phosphoric acid for 30 s, followed by rinsing and air drying. After this stage, Transbond XT primer was applied on the etched enamel surface. MBT 022 slot standard stainless steel brackets were bonded with Transbond XT adhesive resin.
Experimental group—light-curable fluoride varnish, Clinpro XT was applied on the buccal surface and cured for 20 s using a light cure unit (Figure 2).
All patients were instructed to maintain standard oral hygiene, and non-fluoridated toothpaste was advised until the end of each time period. After bonding, at the end of each time period (60, 90, and 120 days), the first premolar brackets were debonded, and premolars were extracted. A careful debonding procedure was used to prevent enamel microfractures around the bracket base. Extracted premolars in both experimental and control groups were stored in normal saline solution. Each tooth was then embedded in self-cure acrylic resin.
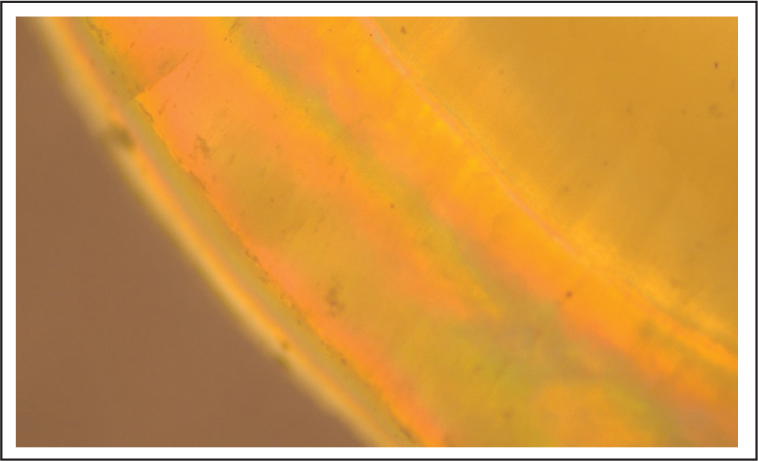
Buccolingual sections were made from the middle third of crown by using a rotating carborundum disc attached to a micromotor, with continuous drip of water. The thickness of each section was further reduced by hand grinding (Figure 3). Sections were evaluated under a polarized light microscope (Olympus CX41, Tokyo, Japan) (Figure 4). Microphotographs of the buccal surface were taken with the fixed magnification of 20 times (Figure 5). The depth of enamel demineralization was assessed using Image J software.
Statistical Analysis
Statistical Package for Social Sciences [SPSS] for Windows Version 22.0 (released 2013, IBM Corp., Armonk, NY) was used to perform statistical analyses.
Descriptive Statistics
Descriptive analysis of all the explanatory parameters was done using frequency and proportions for categorical variables, and using Mean and SD for continuous variables.
Inferential Statistics
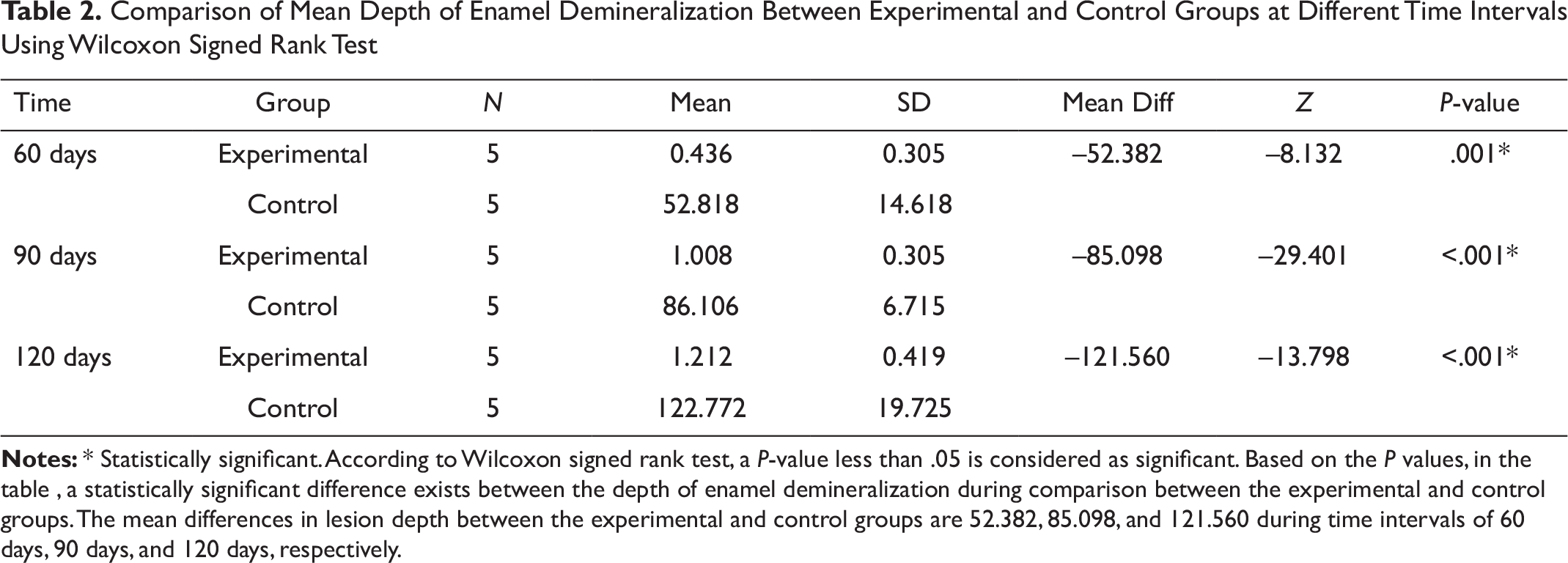
Wilcoxon signed rank test was used to compare the mean depth of demineralization between experimental and control groups at different time intervals.
The Thickness of Each Section Was Further Reduced by Hand Grinding

Polarized Light Microscope (OLYMPUS CX41, Tokyo, Japan)

Microphotograph of the Buccal Surface
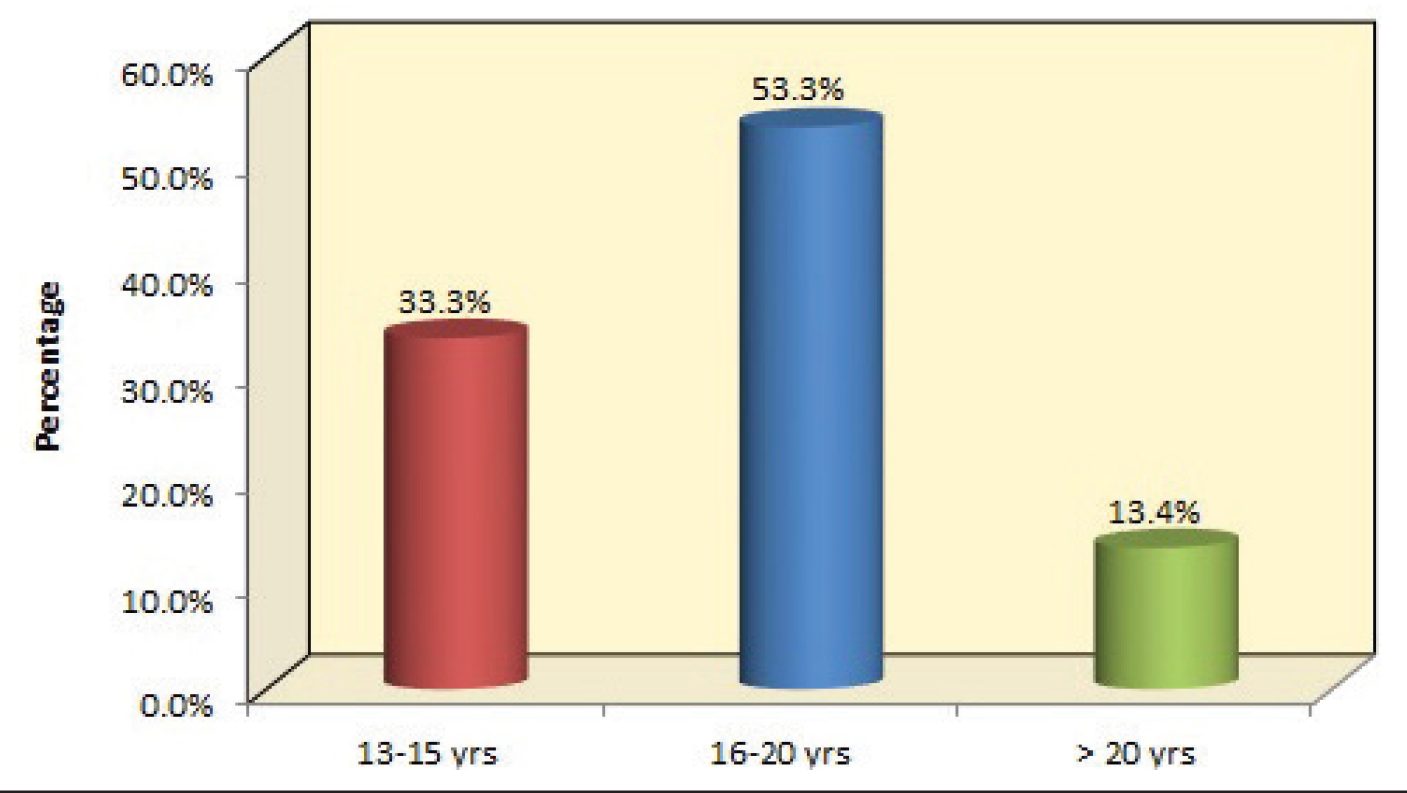
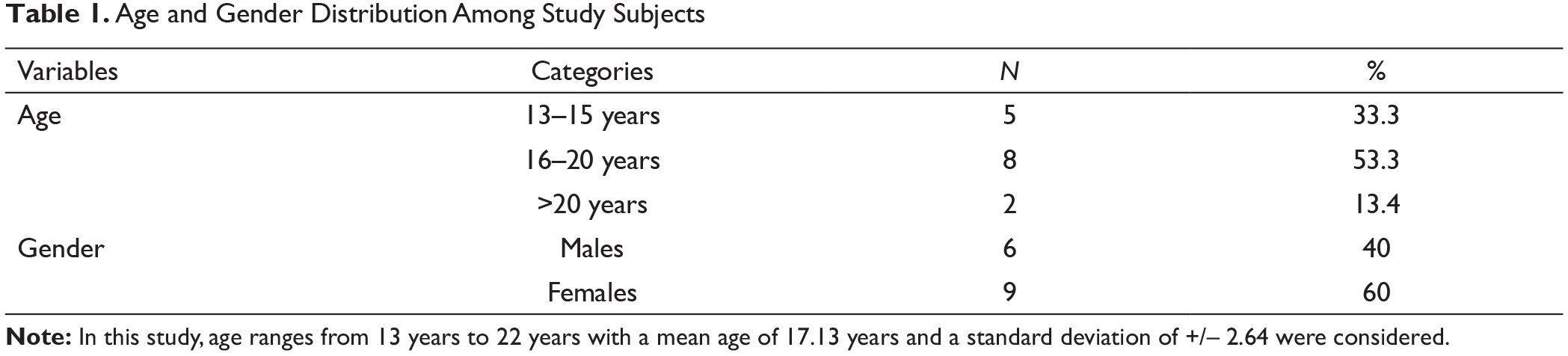
Age Distribution Among Study Subjects
Gender Distribution Among Study Subjects
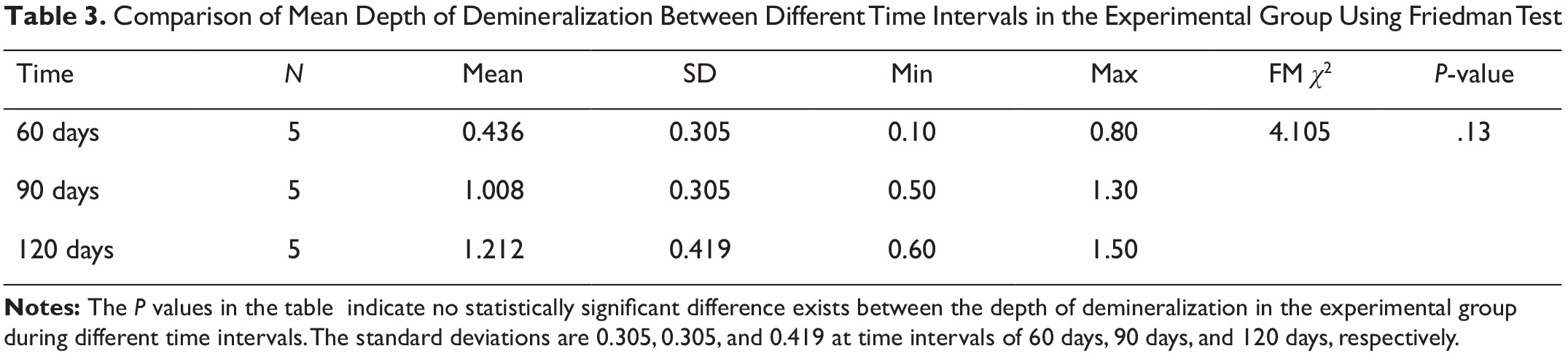
Friedman’s test, followed by Wilcoxon signed rank test as post hoc analysis, was used to compare the mean depth of demineralization between the experimental and control groups at different time intervals. The level of significance was set at P < .05.
Inclusion Criteria
A subject who consented to all first premolar extractions;
fully erupted premolars with intact buccal surface;
no evidence of demineralized lesions; and
no evidence of fluorosis.
Exclusion Criteria
Partially erupted premolars and
premolars with fluorosis and demineralization.
Results
This is an in vivo study to assess the effect of light-curable fluoride varnish on enamel demineralization around orthodontic brackets bonded to first premolars by using polarized light microscopy. Fifteen patients fulfilling the inclusion criteria were included in the study.
Totally, 60 teeth were divided equally (refer Figures 6, 7 and Table 1 for age and gender distribution) into experimental and control groups based on 3 time intervals (60, 90, and 120 days). The objective of the study is to compare the depth of demineralization of enamel in the experimental (group in which fluoride varnish is applied) and control groups.
Discussion
The appearance of white spot lesion after fixed mechanotherapy is esthetically discouraging as the goal of orthodontics specialty is to improve dental and facial esthetics. 6 Insertion of fixed appliances creates stagnation areas and, thus, alters the ecology, resulting in increased microbial content. 7 The principal agent to reduce demineralization is fluoride.
In this study, a light-curable fluoride varnish, CLINPRO XT is used for the clinical trial. Clinpro XT varnish is a site-specific, resin-modified light-cured glass ionomer durable cement coating that forms an immediate layer of protection to prevent enamel demineralization. The “XT” in Clinpro XT represents “extended varnish” having durability, with sustained release of fluoride. Clinpro XT releases more flouride compared to conventional fluorides, and they are more resistant to brushing strokes, approximately 5000 strokes. This resistance is due to the higher filler content of the resin-modified light-curable varnish. 1
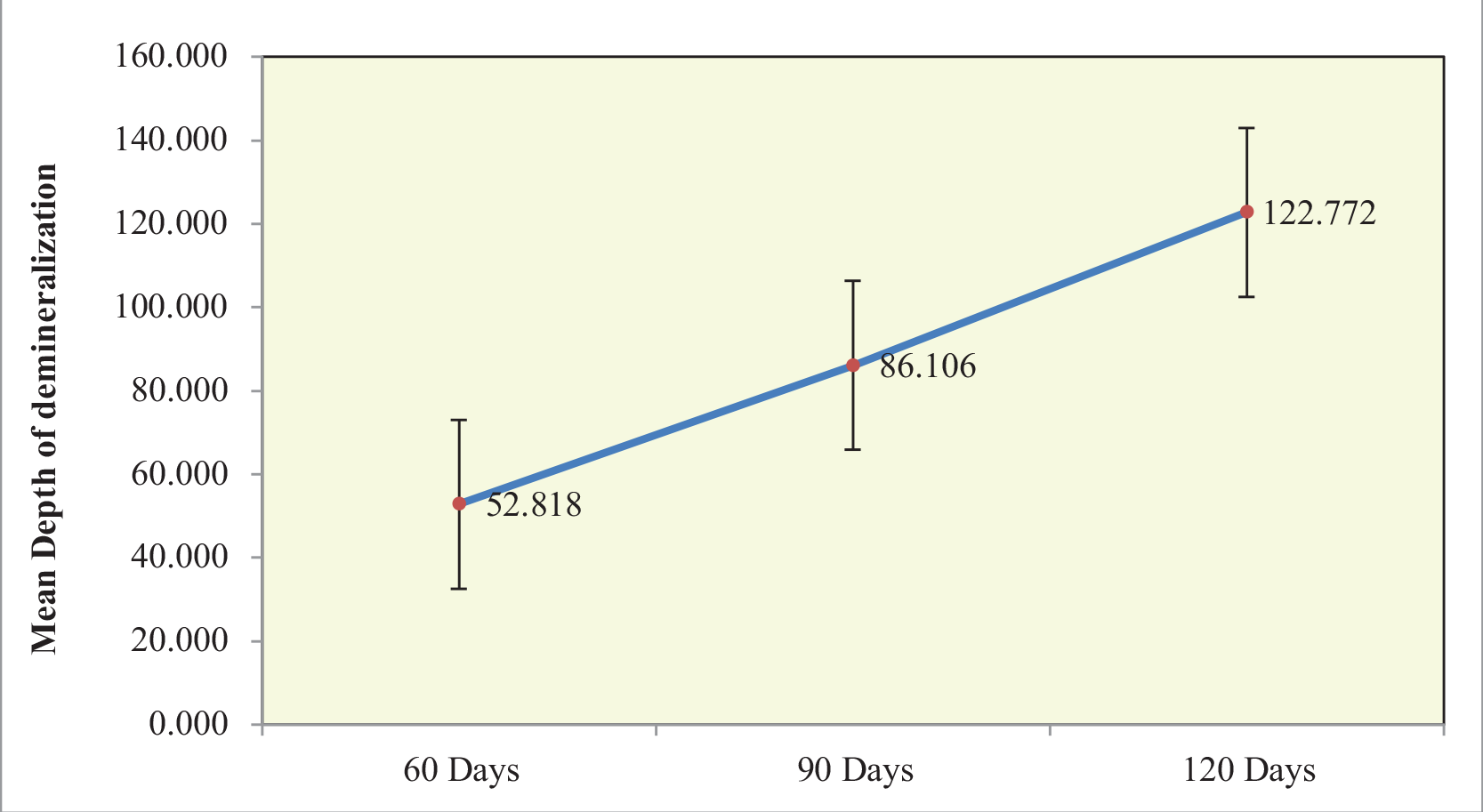
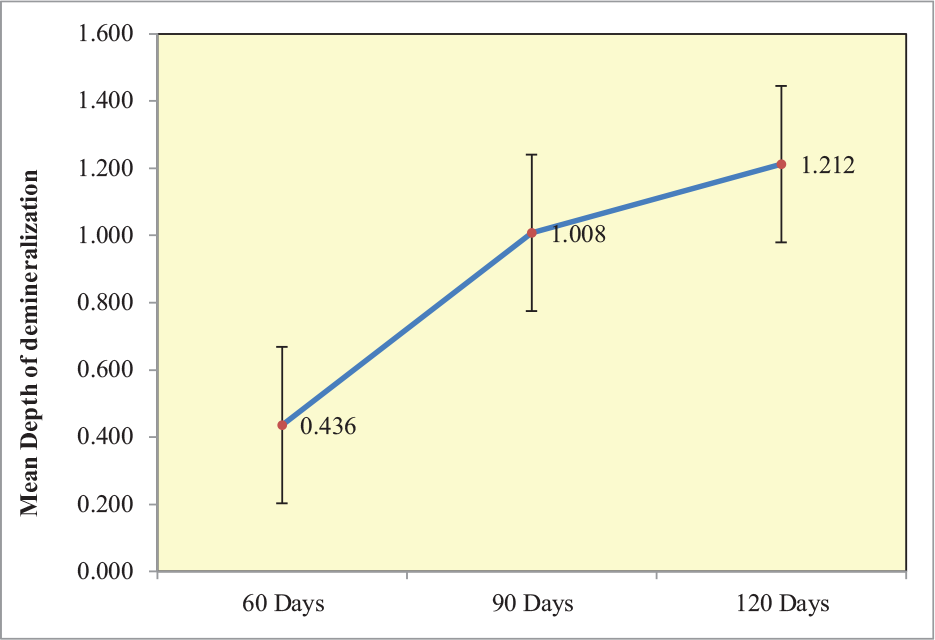
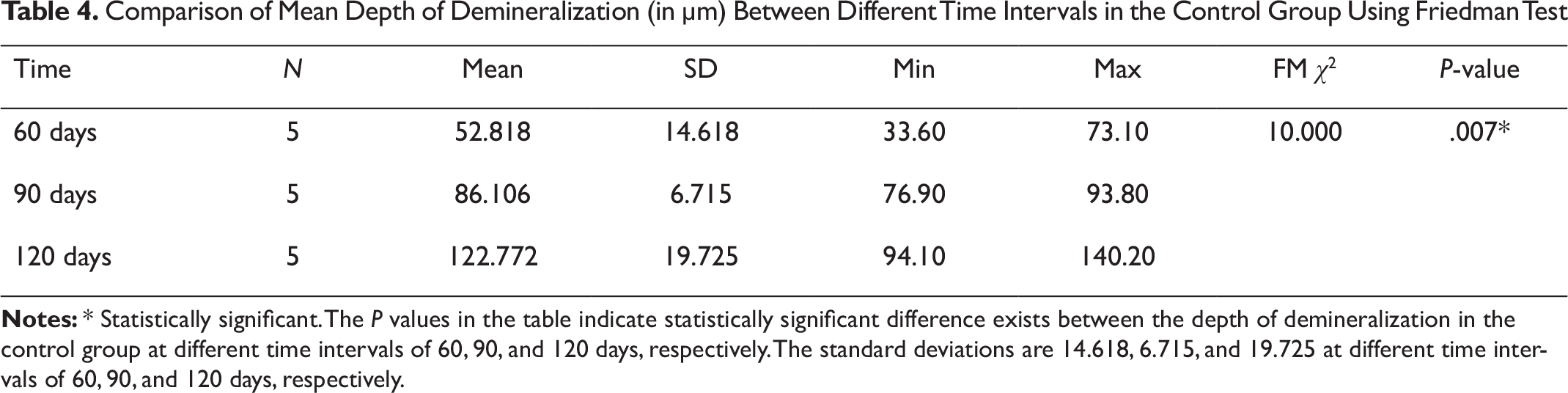
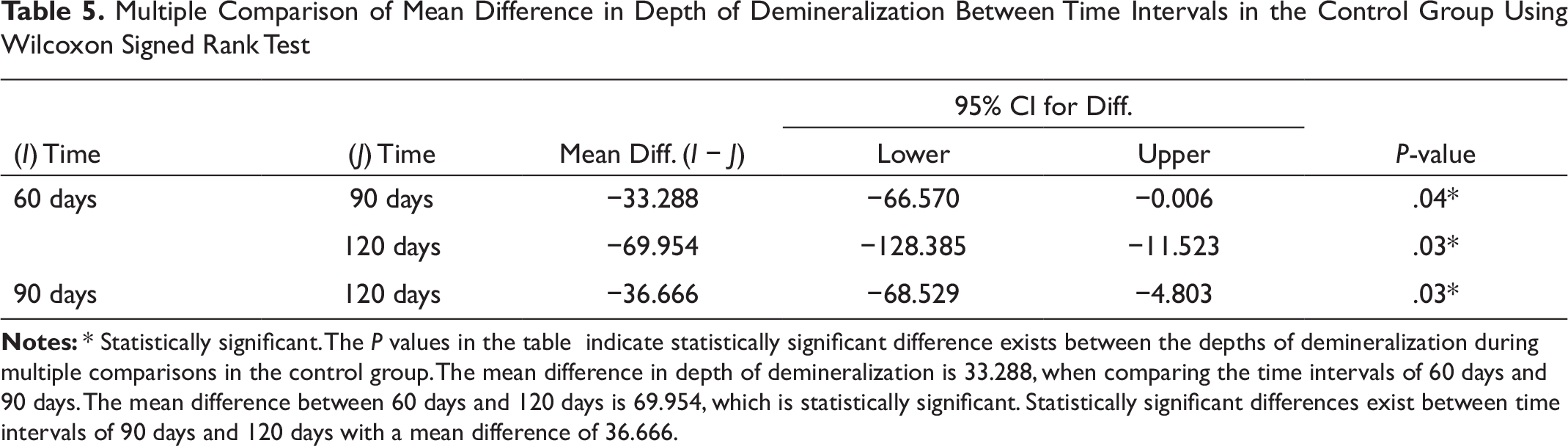
The effect of light-curable fluoride varnish on enamel demineralization was studied for a period of 4 months at time intervals of 60 days, 90 days, and 120 days without interfering with the regular treatment process. The depth of demineralization was assessed by using polarized light microscopy technique. In the control group, demineralization depth increased from 60 to 120 days; (Figure 9, Tables 4 and 5) however, symptoms of dentinal hypersensitivity were not reported during the study except for 2 patients in the 120-day group (Figure 9). In the experimental group, there is no statistically significant difference in lesion depth at different time intervals (Figure 10 & Table 3). There are only limited in vivo studies related to the use of light-curable fluoride varnish to assess the depth of demineralization for a period of 4 months. The closest in-vivo study was one by A. Mehta et al to evaluate the depth of demineralization, and they concluded that the mean lesion depth is 10.6 µm in the experimental group for a period of 90 days compared to 1.008 µm in the present study. 1
Effectiveness of Conventional Fluoride Varnish Application
Du et al evaluated the effectiveness of Duraphat fluoride varnish for a period of 3 and 6 months. The assessment was carried out using DIAGNOdent, and it was found that Duraphat fluoride varnish was effective in the reversal of white spot lesions. 8 In a recent split-mouth study by Perrini et al, when applied at time intervals of 3, 6, 9, and 12 months, Duraphat did not show a significant difference in enamel demineralization in control and experimental groups. 9 Repeated application of conventional fluoride varnish is recommended to prevent the occurrence of white spot lesions (WSL). Various regimens of application of fluoride varnish have been evaluated till date. Van Eck et al 10 suggested one application per year; Beltran et al 11 advocate semiannual application of fluoride varnish. In another study by Modeer et al, 12 it was found that 4 applications of Duraphat fluoride varnish per year can reduce proximal caries progression. Monthly application of fluoride varnish was suggested by Schmit et al. 13
Primarily, varnishes used in dentistry contain biocompatible solvents, such as water, ethanol, acetone, or esters. In these solvents, film formers based on high-molecular polymers (eg, polyamides, cellulose derivatives) or low-molecular resins (eg, colophony) are dissolved. Once applied to the tooth, the solvent starts to evaporate, meaning the film former and active ingredients are available in ever-increasing concentrations. The increasing concentration of the solid and dissolved components of the varnish during evaporation of the solvent leads to closer proximity of the film-forming molecules to each other. This induces an increase in Van der Waals forces and the purely mechanical interactions of the molecules among each other. These interactions eventually lead to the immobility of the molecules and, thus, the formation of a calcium fluoride layer on the tooth surface, which resists subsequent enamel demineralization.
Effectiveness of Light-Curable Fluoride Varnish
Liquid varnishes are based on established dental methacrylates (eg, HEMA, bis GMA). They are diluted to an easy-flowing consistency with solvents (eg, methyl methacrylates, dipentaerythrol pentaacrylates). The addition of blue light-sensitive photoinitiators enables the quick formation of a film when radical polymerization takes place after a dental curing light is illuminated. The most prevalent type of photoinitiators are carbonyl compounds such as diketones or other acrylic components.
A chain reaction in which the radicals formed by the photoinitiator react with the methacrylate monomers results in giving rise to a polymer network that envelops the active ingredients and, thus, permits their extended release. Clinpro XT, light-curable fluoride varnish, provides a rapid release of fluoride during initial few days and, thereafter, sustained release. The fluoroalumiosilicate glass particles present in the surface of varnish provide the immediate release of fluoride by certain surface reactions, while interior provides the reservoir for sustained release of fluoride. 14
Kumar Jena et al conducted a study using resin-modified glass ionomer cement varnish for a period of 6 months, and demineralization was assessed by DIAGNOdent. The results were promising as light-curable fluoride varnish was effective, but careful monitoring was essential for DIAGNOdent reading, as it is susceptible to various local environmental factors such as plaque, calculus, and stains. 15 The present study focused on histological sectioning and assessment of enamel demineralization using polarized light microscopy, and hence is more dependable than other studies.
Conclusion
Age and Gender Distribution Among Study Subjects
Comparison of Mean Depth of Enamel Demineralization Between Experimental and Control Groups at Different Time Intervals Using Wilcoxon Signed Rank Test
Comparison of Mean Depth of Demineralization Between Different Time Intervals in the Experimental Group Using Friedman Test
Comparison of Mean Depth of Demineralization (in µm) Between Different Time Intervals in the Control Group Using Friedman Test
Multiple Comparison of Mean Difference in Depth of Demineralization Between Time Intervals in the Control Group Using Wilcoxon Signed Rank Test
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.