
Abstract

Introduction
Performing a mock surgery on orthodontic models enables a surgeon to envision the blueprint for surgery and to fabricate an accurate dental template that facilitates precise and accurate surgical movements. 1
Hohl, 1 in 1978, postulated that in order to achieve accuracy in the maxillary position and its relationship to the optimal functional centric occlusion, a preoperative model surgery is essential. Model surgeries allow the planned osteotomies to be carried out on a 3D model and allow fabrication of splints, which are used to maintain the occlusal relationship and integrity of skeletal segments during surgical procedures. According to Bamber et al, 2 the Lockwood keyspacer system 3 and Eastman anatomically oriented technique are the 2 most widely used model surgery techniques. Jeon et al 4 stressed on the importance of the concept of 6 degrees of freedom, explaining that mechanical movement is possible only when translation for 1 point is determined three-dimensionally and described using yaw, roll, and pitch. Recently, virtual surgical planning (VSP) 5 has gained a foothold in orthognathic surgery rapidly, thus replacing the traditional model of surgery. It is of a more superior quality than plain radiographs but has inherent shortcomings, such as cost, inability of VSP to incorporate occlusal surfaces into the computed tomography (CT) images, and splint fabrication time lag from the completion of VSP to splint delivery.
In most of the model surgery techniques, the casts are sawed at the bases from the articulator. This procedure is time-consuming and laborious. The sawing of the plaster bases may not be accurate, which might lead to the development of malocclusion post surgically. The aim of this article is to introduce a simplified procedure by utilizing old radiographic films as a surgical cut template placed in between the mounted plaster.
Procedure
An orientation jaw relation is taken with the help of a face bow transfer and secured with dental plaster on a semi-adjustable articulator (Figure 1).
Beading and boxing with modeling wax, space is maintained between the wax boxing and the previously mounted maxillary cast in the case of a mandibular surgery (Figure 2).
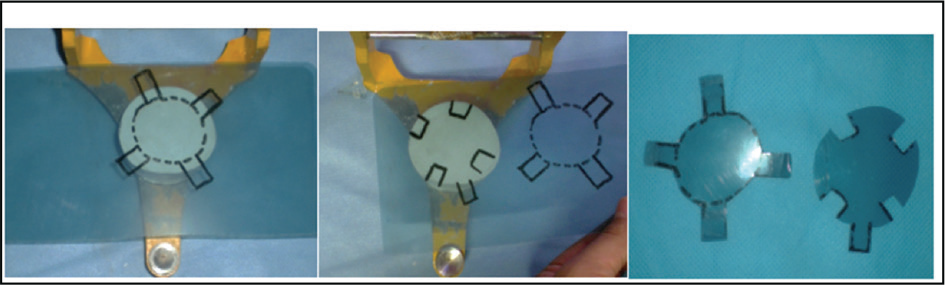
Dental plaster is poured in this undersized boxing and allowed to set, in order to create a dental plaster platform. A surgical cut template is made from old radiographic film with a specific design, which is cut and placed on the dental plaster platform, and the remaining mounting is completed (Figure 3A–C).
The final mounting has extensions of radiographic film surgical template indicating the area of cut (Figure 4A and B).
With the help of a plaster-cutting saw, the minimum attached area is effortlessly cut and separated (Figure 5).
A neat cut preserving the original orientation of the cast is accomplished, the desired amount of movement in millimeters is achieved, and splint fabrication is completed (Figure 6).
Mounting of Maxillary Cast

Undersized Boxing

Radiographic Film Surgical Template (2 Different Designs)
Mounting with Radiographic Film Extending Out for Both Maxillary and Mandibular Surgery

Easy Cut on Mounted Plaster with Plaster Knife
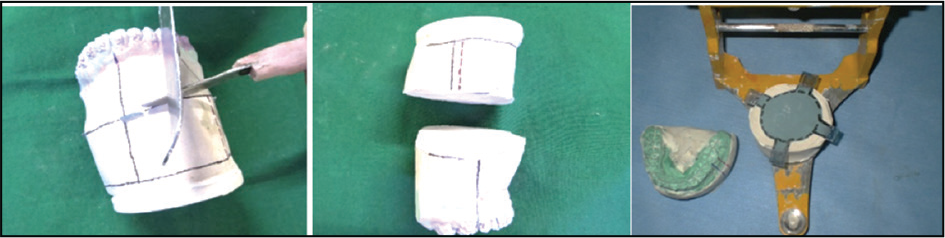
(A and B) Required Millimeter Advancement After Plaster Cut and Final Mounting for Splint Fabrication

Discussion
Mock surgery is one of the most important phases of treatment planning for surgical cases, as it provides a 3D view of the malocclusion in all spatial planes. 2 The mock surgery model has withstood the test of time and has been a traditional method of training the apprentice surgeon for orthognathic surgery. The ability to quantify information from the clinical and radiographic examination, perform a 3D analysis via model surgery, and subsequently manipulate the models into their new position essentially allows the clinician to have a firm understanding of the preexisting relationship and the expected movements. Ideally, the model surgery must not be erroneous in itself at any stage of the manipulation and must be easily performed and highly reproducible. It must be accepted by clinicians with ease, based on their background knowledge, and facilitate communication among clinical specialists in a cost-effective and less time-consuming manner. In the past, authors have employed old radiographic films as a partition prior to plaster model fabrication in order to ease the separation of parts of the model at the desired level, for example, the Kesling setup. Nagar et al. proposed a modification for simplifying model surgery for segmental maxillary surgery, which includes placing an x-ray film in the premolar region in a case treated using the Wassmund technique. A review of literature does not reveal any documented evidence of similar innovative use of radiographic film in order to simplify model surgery. The present article highlights this innovation as very convenient in making a precise and exact surgical cut on the mounted cast, thus eliminating any errors that might take place in the vertical or sagittal dimensions for accurate splint fabrication. This innovation also minimizes the time and effort required during the sawing of mounted casts.
Conclusion
This innovative technique of utilizing old radiographic films as a surgical cut template is a novel method that has a simple design, is easy to fabricate, is affordable, does not require any special instruments, and utilizes readily available, old, superfluous radiographic films, with the additional advantages of providing comfort to the clinician and preserving time.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.