
Abstract
Aim and Objectives:
Inappropriate authorship is a threat to the integrity of scientific publication. Although many journals have authorship guidelines, there may be a gap between knowledge of authorship criteria and practice. The purpose of this study was to assess and compare the knowledge, attitude, and practice of authorship guidelines among medical and dental professionals.
Material and Methods:
A web-based cross-sectional study was carried out using Google Survey after obtaining approval from our University Ethics Committee. The knowledge, attitude, and practice of dental and medical faculty towards authorship were assessed using a self-administered questionnaire. The corresponding authors of original articles published in 4 medical and 4 dental journals from 2014 to 2016 were sent an e-mail with a link to an electronic survey containing a questionnaire. Voluntariness, privacy, and confidentiality were ensured and mentioned in the participation information sheet (PIS). Submission of the survey was construed as informed consent. A total of 541 corresponding authors (medical [n = 275], and dental [n = 269]) were invited to the study, and 207 responded to the survey (medical [n = 104] and dental [n = 103]). Incomplete responses were eliminated (n = 5). The remaining responses (total [n = 202]; medical [n = 100], and dental [n = 102]) were analyzed.
Results:
The mean scores of knowledge, attitude, and practice of the participants regarding authorship were 6.9 ± 2.02 (scale of 11), 29.13 ± 3.66 (scale of 45) and 6.70 ± 0.08 (scale of 10), respectively. The knowledge of authorship guidelines among medical professionals was significantly higher than that among dental professionals. No statistically significant difference was observed in attitude and practice scores (P > .05). There was a weak correlation between knowledge with attitude, and practice. There was a weak correlation between the age, gender, number of publications, and different levels of hierarchy with knowledge, attitude, and practice.
Conclusions:
• Participants had moderate knowledge of, attitude towards, and practice of authorship guidelines.
• Researchers should undergo adequate training on authorship guidelines before initiation of a project.
Introduction
Inappropriate authorship is a threat to the integrity of scientific publication. In order to overcome this problem, many associations of editors have proposed guidelines for authorship.
The criteria for authorship, according to the International Committee of Medical Journal Editors (ICMJE),1 are (a) substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work; (b) involvement in drafting the work or revising it critically for important intellectual content; (c) final approval of the version to be published; and (d) agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Only when all 4 criteria are fulfilled can the author’s name appear in the byline of an article. Persons who fulfil only some criteria but not all should only be acknowledged. The World Association of Medical Editors (WAME) provides guidelines on different issues of authorship, such as criteria for authorship, number of authors, the order of authorship, and authorship disputes.2 The Committee on Publication Ethics (COPE) provides information on all aspects of publication ethics, including what constitutes authorship. It provides guidelines on “How to Handle Authorship Disputes: A Guide for New Researchers.”3 The Council of Science Editors (CSE) published a white paper on publication ethics, which also includes authorship and its responsibilities.4 The European Association of Science Editors (EASE), in collaboration with other organizations, endorses guidelines on authorship.5 Although authorship guidelines are established, there may be a gap between knowledge and practice of authorship.
Inappropriate Authorship
Two terms can be used to describe inappropriate forms of authorship: (a) a ghost author is one who has contributed significantly to a research project but is not listed as an author; and (b) a guest author is one who does not fulfil the ICMJE criteria but is listed as an author. These names may be added because of their reputation, or position of authority, and sometimes a name may be added based on the understanding that one would do the same for you regardless of your contribution. Guest and ghost author practices dilute the credibility and accountability associated with authorship.
Authorship in Student–Faculty Projects
A student–teacher relationship is delicate, built on trust, dependence, and respect, but many times, the student is vulnerable.6,7 Misuse of authority by a teacher and ignorance of a student about his or her rights can lead to inappropriate authorship. The order of authors while publishing a student’s dissertation can get complicated when the student does not show any inclination to write the manuscript and where the guide has to spend considerable time for preparing the manuscript. However, the student should be the first author for any publication based wholly on his or her dissertation.6,8,9 Although excluding a non-contributing head of department may be difficult, authorship should not be gifted.
Authorship Order
The order of authorship on the byline should be a joint decision of all the authors and should be discussed during the initial conceptualization of the project.10 The most accepted order of the authors should be based on the relative contribution.11,12 The alphabetical order may be used where all co-authors have contributed equally. The meaning of the order of authorship should not be assumed unless an assigning order has been described by the authors.2
Authorship Contributions
The corresponding author should provide a description of each author’s contribution, and ideally, the editors should publish this information.2,4,13,14 However, some journals publish this, and many times, it is only for the editors’ reassurance that the authors have fulfilled the criteria.
Role of the Corresponding Author
The corresponding author should take the responsibility to communicate with the journal throughout the publication process and to respond to the editorial and reader queries after publication.1 The corresponding author should be the guarantor for the integrity and accountability of the manuscript.
Acknowledgement Contributions
A contributor who fulfills 1 or more but not all the authorship criteria should only be listed in the acknowledgement section.1 Contributors who provided purely technical help, or who helped in the collection of data or literature survey, the writing assistant, the statistician, a head of department who provided general support, such as the acquisition of funding or supervision of the research, all should only be acknowledged.1,2,4,15
Publication Misconduct
Plagiarism is the practice of taking someone’s work, idea, results, text, or illustration and passing it off as one’s own work without acknowledging the source.16-18 Plagiarism could also be ‘content recycling’ (self-plagiarism), where authors fail to provide the source of their own published literature. Many journals now ask for a report of a plagiarism-detecting software as part of the submission procedure. Dividing studies into shorter-length articles is known as “salami slicing,” and it results in the proliferation of mediocre papers.16-18 The practices of salami slicing and plagiarism are also forms of publication misconduct.
Knowledge is a fact. Attitude is our belief and what we follow, or what we think to be the best. Practice is how closely we follow the knowledge in reality.
The present study is undertaken to assess and compare knowledge, attitude, and practice (KAP) of authorship guidelines among medical and dental professionals. The study also aims to assess the correlation between KAP among medical and dental professionals.
Material and Methods
A web-based cross-sectional study was conducted after approval from the Yenepoya University Ethics Committee (YUEC/2016/182).
The sample size was computed using priori power analysis after determining alpha (0.05) and beta (80%) errors based on time and availability of respondents’ list. The calculation showed a minimum of 100 patients in each group would be required at a significance level of 0.05, at 80% power, and with an effect size of 0.1. After analyzing responses from the survey for KAP of medical and dental professionals (mean and standard deviation [SD]), post hoc power calculation was carried out at a significance level of 0.05 and power at 80%. For knowledge, it was significant at an effect size of 0.3, and for attitude and practice it was not significant at an effect size of 0.4.
The methodology used in this study was adopted from previous literature.19,20 The journals selected for the study are specialty journals (in medicine and dentistry) from associations of the United States and India that profess to follow ICMJE guidelines for publication, as the associations are guardians of the profession and are expected to hold high scientific and ethical standards. The journals were American Journal of Medicine, American Journal of Ophthalmology, Journal of Periodontology, American Journal of Orthodontics and Dentofacial Orthopedics, Indian Journal of Medical Research, Indian Journal of Ophthalmology, Journal of Indian Society of Periodontology, and Journal of Indian Orthodontics Society. Journals provide communication details of only corresponding authors, and so only they were contacted.
Questions were formulated under the following sections: (a) authorship contribution; (b) authorship in student–faculty projects; (c) criteria for acknowledgement; (d) authorship order; (e) inappropriate authorship; (f) authorship misconduct; and (g) authorship accountability.
A questionnaire not based on previous studies was used. It was developed using 7 steps based on the guidelines for formulating a questionnaire.21 The questions developed were then subjected to preliminary pilot testing using 10 participants for reliability and validity. Reliability was established for internal consistency, and so were test–retest reliability and inter-rater reliability. Content and construct validity were determined and later modified for initial testing using 30 intended participants. The content validation of the questionnaire was carried out by 3 faculty members from Centre for Ethics.
The questionnaire consisted of 38 questions. Eight questions were on demographic data, 11 questions were on knowledge (best-response multiple-choice questions [MCQs]), 9 questions were to assess their attitude (Likert-format statements), and 10 questions were related to their practice (Yes/No or best-response MCQs). The Likert-format statements consisted of a 5-point scale (strongly agree, agree, uncertain, disagree, and strongly disagree).
For the 11 knowledge questions, scores 0 and 1 were considered for incorrect and correct responses, respectively. Therefore, the knowledge score range was 0 to 11. Nine questions on attitude were assessed on a 5-point Likert scale, with score 1 for strong disagreement and score 5 for strong agreement. The attitude score range was 0 to 45. Ten questions on practice were assessed by “Yes”/“No” or best-response questions, and a score of 1 was given for each correct response and 0 for each incorrect response. Therefore, the practice score range was 0 to 10.
Each section of the questionnaire was assessed at 3 levels: level 1—a score of less than 50% of the total achievable score was classified as poor; level 2—a score of 50% to 70% was classified as moderate; and level 3—a score over 70% was classified as good.22
The table of contents of each issue of all the 8 journals published during 2014 to 2016 was reviewed. The original articles to be included had to have 2 or more authors. Once the articles were identified and the e-mail addresses of the corresponding authors obtained, the latter were contacted through e-mail. The PIS contained details of this anonymous survey, with the assurance and commitment that all replies would be kept confidential. Submission of the survey was construed as informed consent to participate in the study, which was clearly mentioned in the PIS. If the corresponding author had more than 1 article, he or she would be taking only 1 survey. The survey was conducted between September 15, 2016 and October 8, 2017.
Corresponding authors (total [n = 541]; medical [n = 275], and dental [n = 269]) were contacted through e-mail. Two reminder e-mails were sent in 2-week intervals. A total of 207 corresponding authors responded to the survey (medical [n = 104]; dental [n = 103]). Incomplete responses were eliminated (total [n = 5]; medical [n = 4], and dental [n = 1]). The remaining responses (total [n = 202]; medical [n = 100; 36.36%], and dental [n = 102; 37.91%]) were analyzed.
Statistical Analysis
Statistical analyses were performed using the SPSS software (IBM SPSS Statistics for Windows, Version 23.0, Armonk, NY, USA). Descriptive statistics were used to summarize the most appropriate answer. The KAP scores were assessed for data distribution. As data followed normal distribution after normality tests (histogram, normality plots, Shapiro–Wilk, and Kolmogorov–Smirnov tests), a parametric test (Z test) was applied. Independent t test was used to assess the KAP scores among medical and dental professionals. Pearson correlation was used to assess the correlation between KAP. A P-value of less than .05 was considered statistically significant.
Results
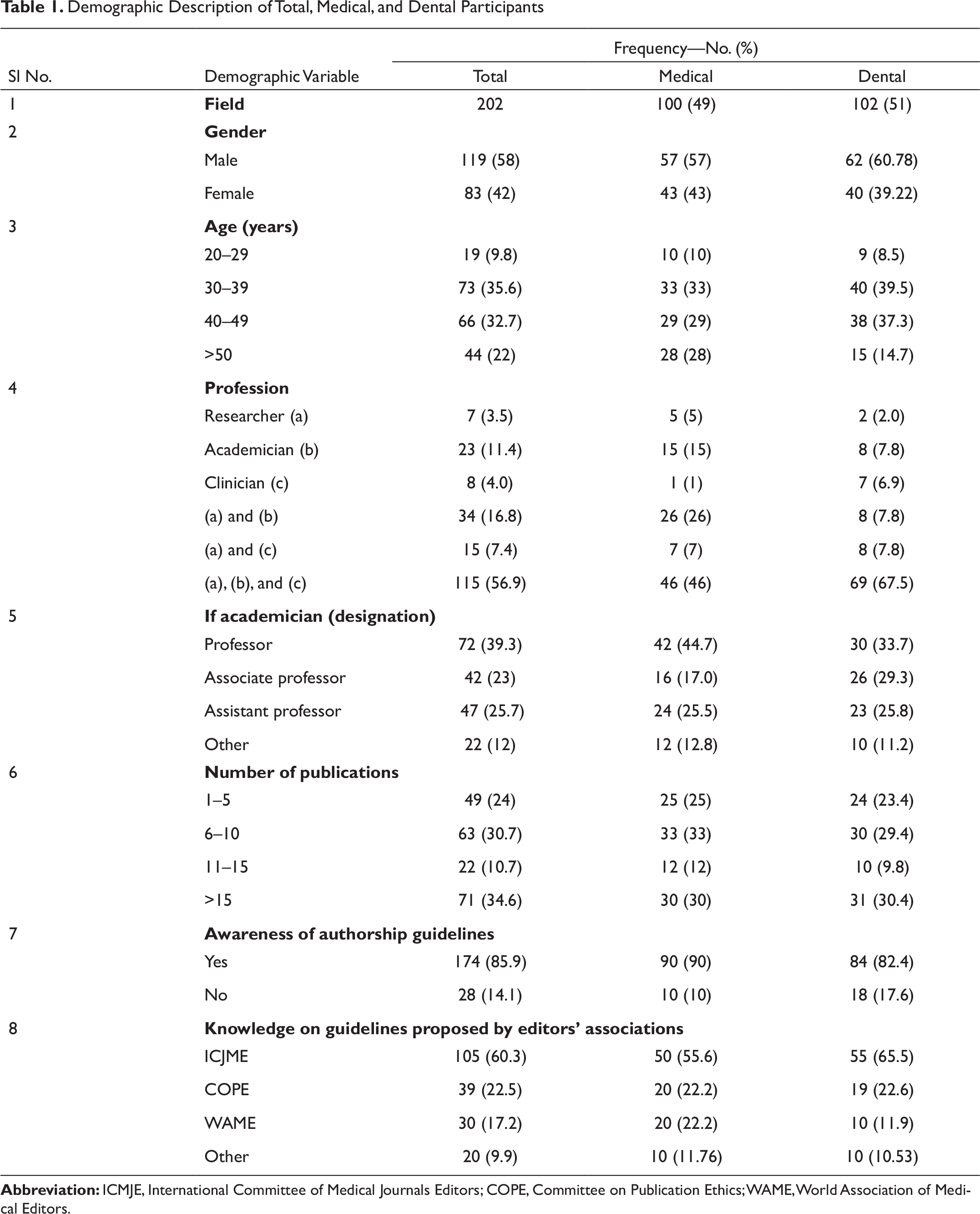
Demographic details showed that 202 respondents participated in the survey, out of which 100 were medical and 102 were dental professionals (Table 1). Of them, 70% had more than 5 publications, 174 were aware of ICMJE guidelines, and 105 followed ICMJE guidelines.
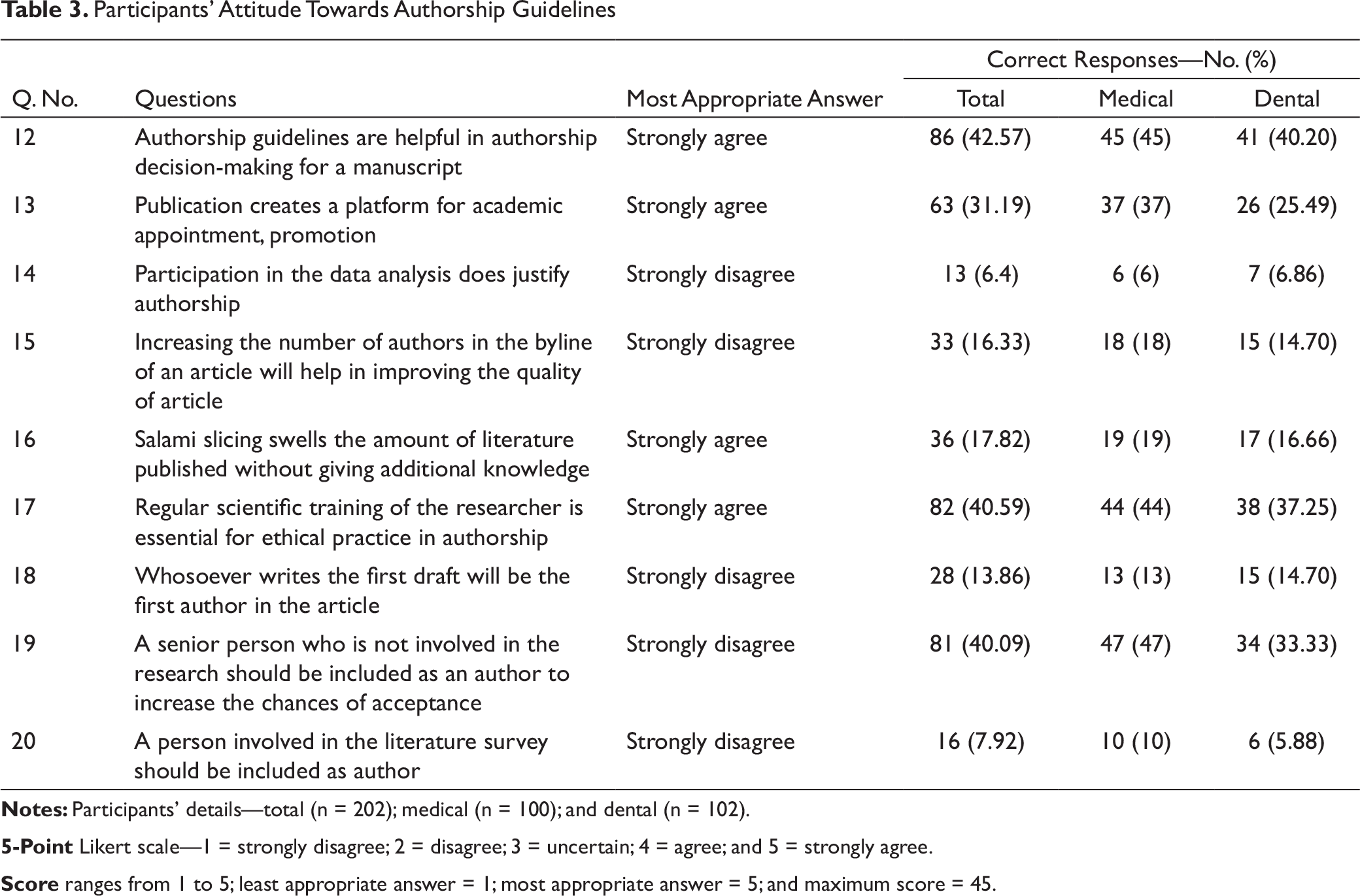
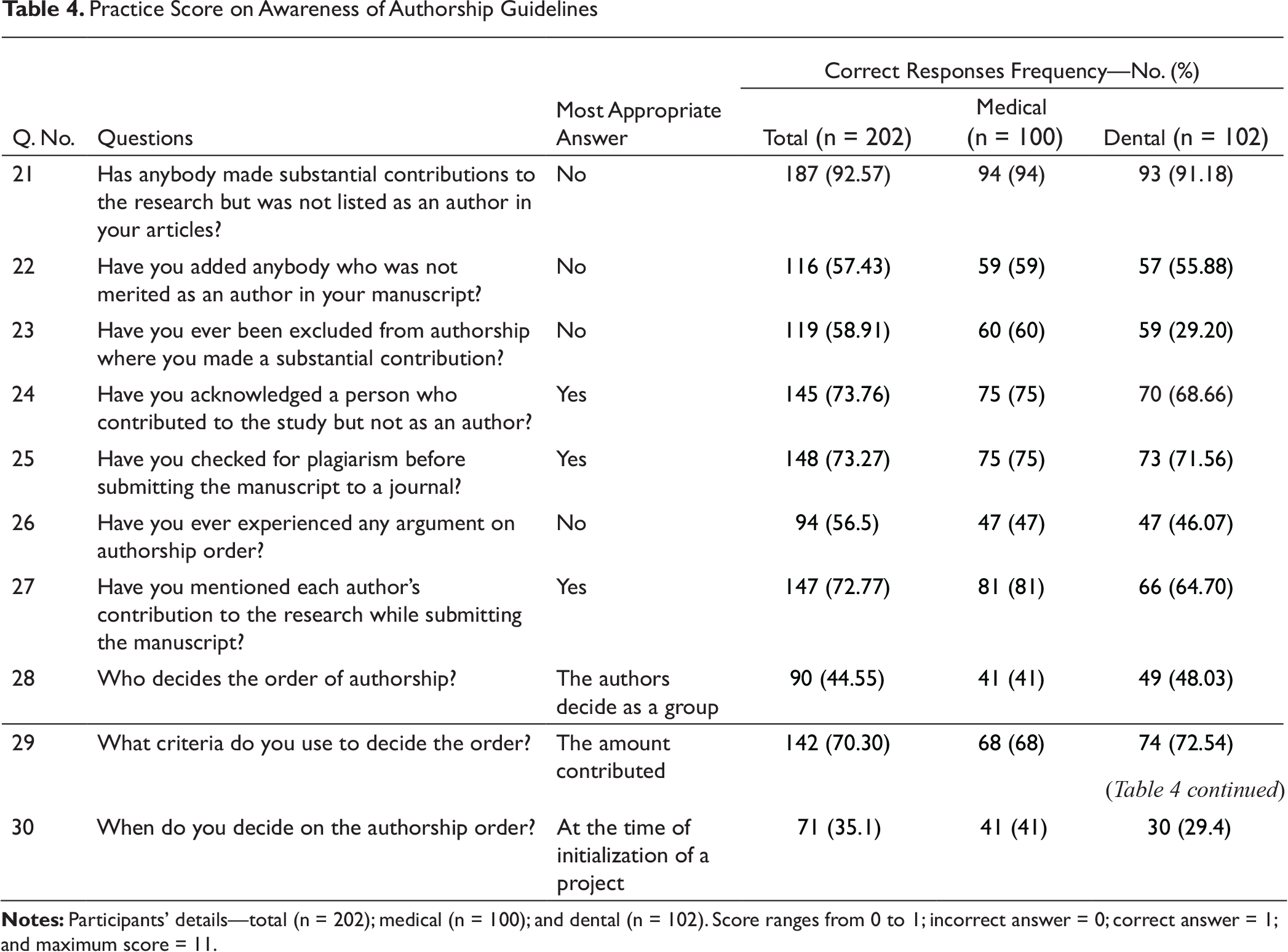
Q1 to Q11 represented participants’ knowledge of authorship (Table 2). Q12 to Q20 represented participants’ attitude towards authorship (Table 3). Q21 to Q30 represented the participants’ practice of authorship (Table 4).
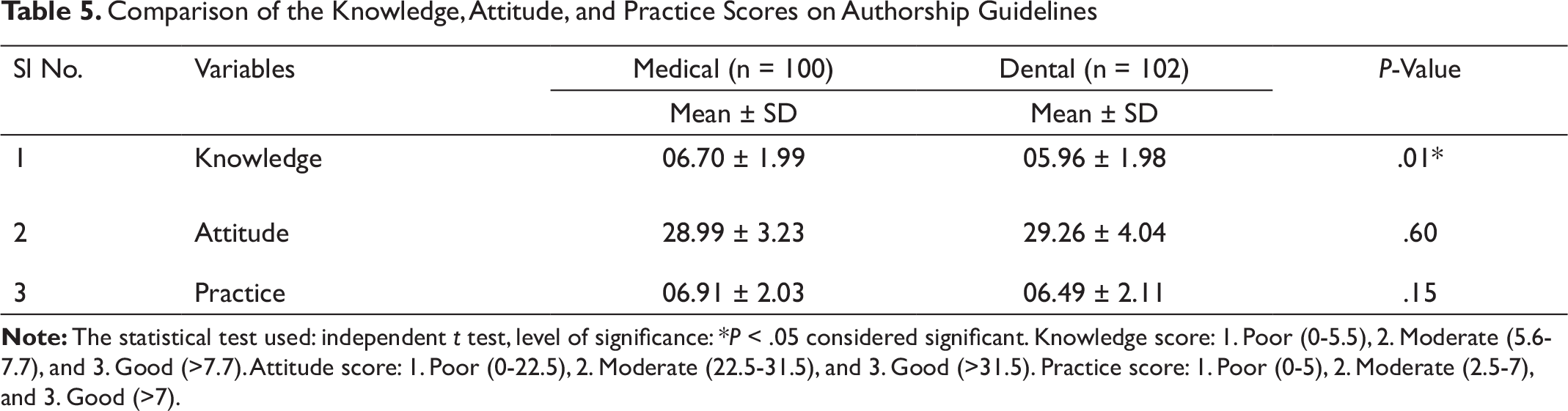
Participants’ mean scores of knowledge of, attitude towards, and practice of authorship guidelines were moderate (Table 5). There was a statistically significant difference in the knowledge scores of medical and dental professionals (P <.05). However, there was no statistically significant difference observed in the attitude and practice scores between the 2 groups (P >.05).
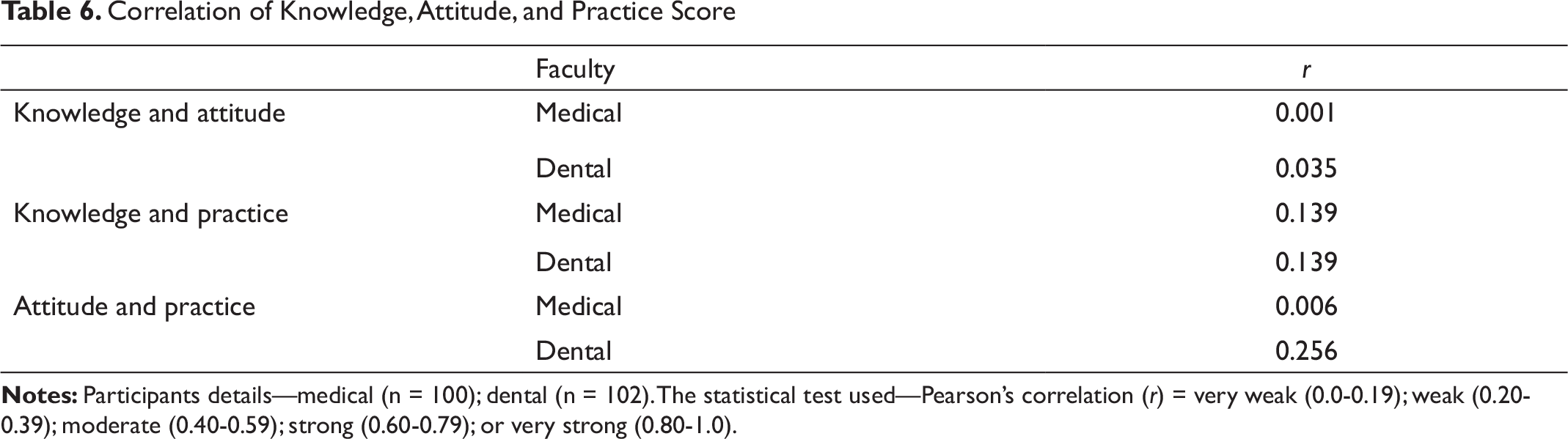
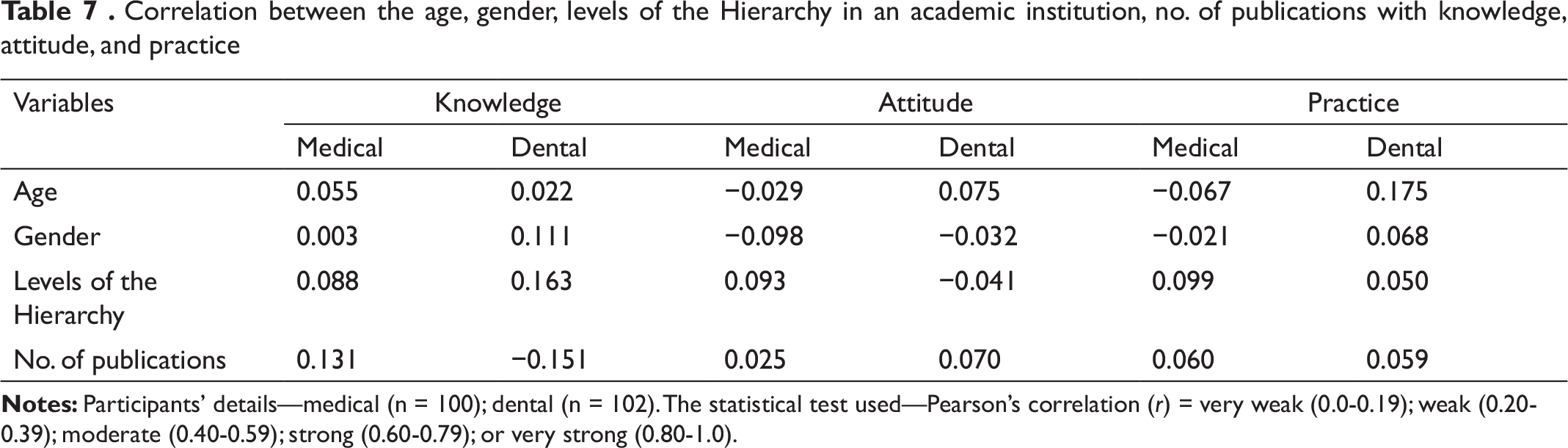
Pearson correlation (r) showed that there is a weak correlation between KAP scores (Table 6). Correlations between the age, gender, number of publications, and different levels of hierarchy and KAP are described in Table 7 and are shown to be weak.
Discussion
Ethical authorship practice is fundamental to the integrity of research. Ethical issues involved with authorship are mainly: (a) inclusion of an author without any substantial contribution; (b) exclusion of an author who had contributed substantially; and (c) inappropriate order of authors in the byline of an article. An author should contribute substantially to the conception of the study, analysis, interpretation of data, drafting of the manuscript, or revising it critically, and finally approval of the version to be published. Participation only in the acquisition of funding or the collection of data or general supervision of the research group is not sufficient for authorship. In this survey, questions were formulated based on authorship guidelines to assess participants’ KAP.
The participants of this study were corresponding authors who are also guarantors, and they had the following demographic details: 90.2% were above 30 years, 39.13% were professors, 75% of the participants had more than 5 publications, and 92% were academicians and researchers. Whereas 85.5% of the respondents in this study claimed to be aware of authorship guidelines (Table 1), Das et al reported that only 22.2% of medical and 39% of pharmacy faculty were aware of authorship guidelines.23 Nylenna et al reported that 97% of the respondents had knowledge of existing authorship criteria.24
Although participants of this study claimed to be aware, it appeared they lacked in knowledge of ICMJE guidelines for authorship criteria. ICMJE authorship criteria are very specific, but sufficient adherence seems to be missing, and the distinction between authorship and acknowledgement criteria is not clear for many (Q2, Q3, Q15, and Q20; Tables 2 and 3).
Authorship in a publication based on a student’s dissertation is a frequent cause of conflict in academic institutions. The traditional practice of adding the names of faculty and head of the department in an article may be either due to the interaction that the student would have had with them during his or her study or due to guidelines issued by the institution. Inadvertently, due to the vulnerability of the student, guest and ghost authorship are practiced. The pressure to publish can also be a major cause. Some institutions make publication mandatory for students, and some require publication for academic progression. However, our participants’ knowledge on the order of authors in a publication based on a student dissertation was good (Q4 and Q5; Table 2). However, very few participants replied correctly to the role of a non-contributing head of department in a student’s project (Q6, Table 2).
Honorary authorship may be practiced due to respect for someone with a reputation in that specified field. Although they might only have taken an opinion from such a person, the authors may feel obliged to include his or her name in the byline. Many times, the inclusion of guest authors is done to increase the chance of acceptance of a paper, although in most reputed journals, the manuscript is blinded during the review process. In order to increase the number of publications, friends and colleagues may add names, with the understanding of gifting authorships mutually. The prevalence of guest authorship in this study was found to be 57.43%, which is relatively more than that found by previous studies (Q22; Table 4).19-29 In this study, the practice score for ghost authorship was low (7.5%) (Q21; Table 4), but many reported that they were excluded from articles in which they had contributed substantially (42%) (Q23, Table 4). The practice of ghost authorship reported in the present study was less than that in other studies.14,25-28
Demographic Description of Total, Medical, and Dental Participants
Participants’ Knowledge on Authorship Guidelines
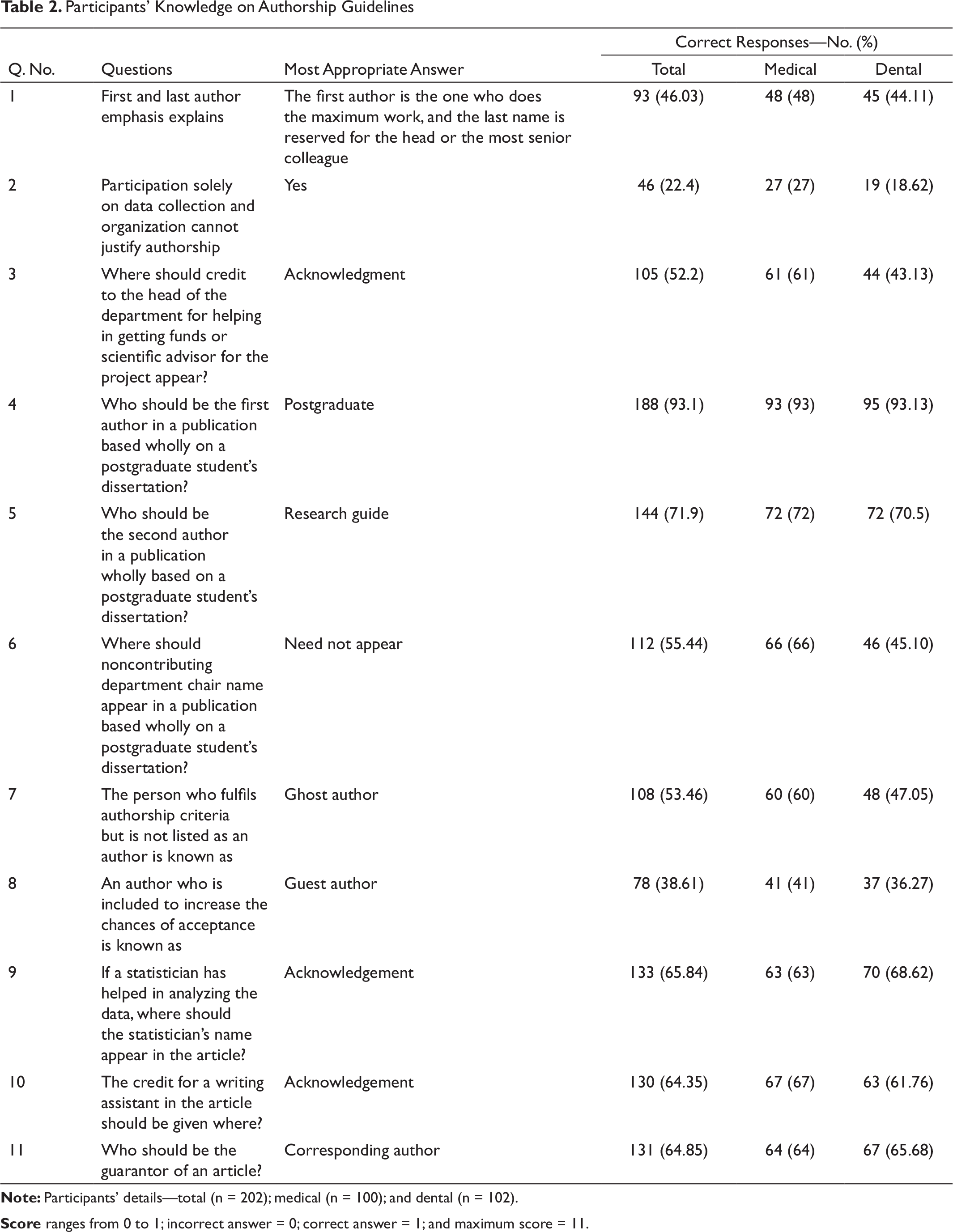
Score ranges from 0 to 1; incorrect answer = 0; correct answer = 1; and maximum score = 11.
Participants’ Attitude Towards Authorship Guidelines
Practice Score on Awareness of Authorship Guidelines
Comparison of the Knowledge, Attitude, and Practice Scores on Authorship Guidelines
Correlation of Knowledge, Attitude, and Practice Score
Correlation between the age, gender, levels of the Hierarchy in an academic institution, no. of publications with knowledge, attitude, and practice
Most guidelines specify that a statistician or a writing assistant involved with a project should only be acknowledged, and in this study, the participants’ knowledge of the role of the statistician or writing assistant was good (Q9 and Q10; Table 2).
The participants of this study had a better understanding of the order of authorship, as compared to those in previous studies.20,23 Most of them followed the order of authorship based on the amount of work contributed (Q29; Table 2), and 51% of them decided the order during conceptualization (Q30; Table 4). Some of them experienced arguments on the order of authorship (Q26; Table 4).
The corresponding author also has the role of a guarantor to oversee that there is no publication misconduct. 65% of participants were aware of the role of the corresponding author, to ensure that the authorship guidelines are followed during manuscript submission. (Q11; Table 2).
Participants were aware of forms of research misconduct such as “plagiarism” and “salami slicing” in scientific writing. Of the participants, 73.27% used a plagiarism-detecting software before the submission of a manuscript to a journal (Q25; Table 4). Salami slicing of a study in order to increase the number of publications is also a form of misconduct, and 17.82% of the participants strongly agreed with our statement that salami slicing swells the literature without providing additional knowledge (Q16; Table 3).
Wolfson and Arora reported that students had a clear understanding of authorship criteria after a discussion-based workshop on authorship education, and that their knowledge on authorship was improved after the workshop.30 The participants of this study also agreed that scientific training on authorship guidelines might empower them to deal with unethical practices (Q17; Table 3).
Limitations of the Study
As this study included only 8 journals, the results of this study cannot be generalized. The data were self-reported by corresponding authors and were not verified with co-authors. Either recall bias, where time interval after the publication was long, or social desirability bias may have resulted in under-reporting. Since this was an anonymized survey, responses from national and international journals could not be compared.
Further Scope
There are very few published studies on the practice of authorship guidelines among dental professionals. More studies are required to bring awareness on guidelines.
Conclusion
The present study concluded that unethical practice still exists, despite authorship guidelines proposed by different associations. Researchers should undergo adequate training on authorship guidelines before the initiation of a project. Participants’ scores in knowledge of, attitude towards, and practice of authorship guidelines were moderate. The knowledge of authorship guidelines among medical professionals was significantly better as compared to dental professionals. There was no difference in the scores for attitude and practice among both medical and dental professionals.
Footnotes
Acknowledgement
This study was carried out as a project for 'Postgraduate Diploma in Bioethics and medical ethics' Center For Ethics, Yenepoya (Deemed to be University).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.