
Abstract
Abstract
VG, 25-year-old male, presented with c/c of forwardly placed lower jaw and history of unsatisfactory previous orthodontic treatment. Extraorally, the patient had asymmetrical face and concave profile, competent lips, positive lip step, and chin deviated toward left side by 2 mm. Intraorally, the patient had Angle’s class III type 3 malocclusion with an overjet of (–1) mm, overbite of 0%, and cross-bite wrt 12, 21. The patient was skeletal class III due to macrognathic and prognathic mandible with hypodivergent growth pattern, and proclined upper and retroclined lower incisors. The patient was managed orthosurgically with bimaxillary surgery (maxillary advancement 3 mm + mandibular setback 7 mm) after presurgical decompensation.
The case report discusses in detail the diagnosis and comprehensive management of the skeletal class III case.
Introduction
The skeletal class III malocclusion may involve both maxillary retrusion or mandibular prognathism. The diagnosis of skeletal class III malocclusion requires evaluation of not only sagittal position of maxillary and mandibular bone but also contribution of transverse and vertical factors. Ellis and McNamara 1 in their study of adult subjects with class III malocclusion found a combination of maxillary retrusion and mandibular protrusion to be the most common skeletal relationship. The role of heredity in the etiology of skeletal class III malocclusion is well established. 2 Litton et al reported a typical finding that one-third of a group of patients with severe class III malocclusion had a parent with the same problem, and one-sixth had an affected sibling. 3 The severity of skeletal class III malocclusion may affect the facial aesthetics to the extent that orthodontics alone may not be the treatment alone. The orthosurgical treatment in such cases is necessary to provide satisfactory results.
Pretreatment Assessment
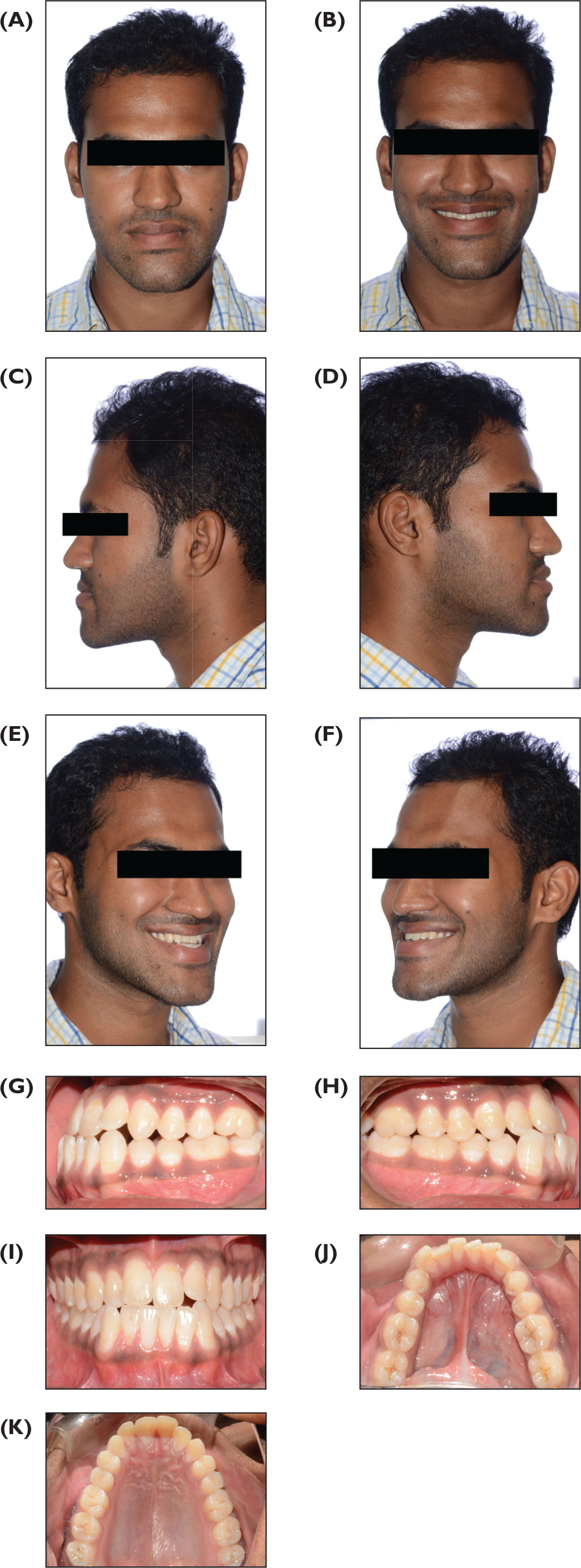
VG, 25-year-old male, reported with chief complaint of forwardly placed lower jaw. The patient had history of orthodontic treatment. On frontal clinical examination, the face was asymmetrical with chin deviation toward left side by 2 mm, leptoprosopic with a concave profile, prominent chin, deficient midface, flat cheekbone contour, and positive lip step (Figure 1A-1F). Intraoral examination showed Angle’s class III Type 3 malocclusion, Overjet of (–1) mm, overbite of 0%, and cross-bite wrt 12, 21. The maxillary and mandibular arches were well aligned with slight crowding in the mandibular arch with all permanent teeth present and good oral hygiene (Figure 1G-1K).
Pretreatment Radiographic Analysis
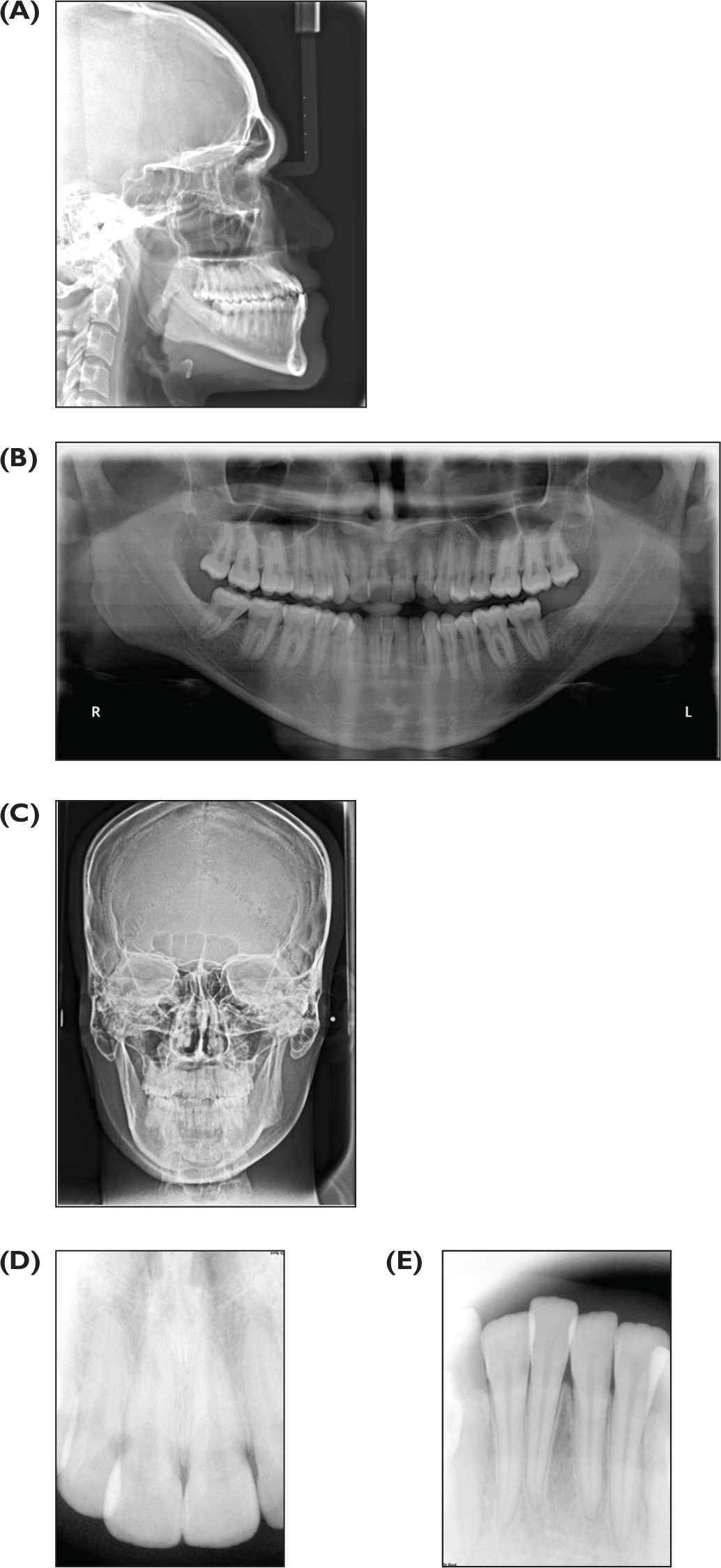
The patient was skeletal class III with macrognathic and prognathic mandible and retropositioned maxilla. The patient had a hypodivergent growth pattern. The maxillary anterior teeth were proclined and mandibular anterior teeth were retroclined (Figure 2A, Table 1). Orthopantomogram (OPG) showed presence of 18, 28, 38, and 48 (Figure 2B). Intraoral periapical radiograph (IOPAR) show no abnormality in morphology of upper and lower anterior teeth (Figure 2C and 2D).
(A-K) Pretreatment Extraoral and Intraoral photographs
(A-E) Pretreatment Lateral Cephalogram, OPG, and IOPAR
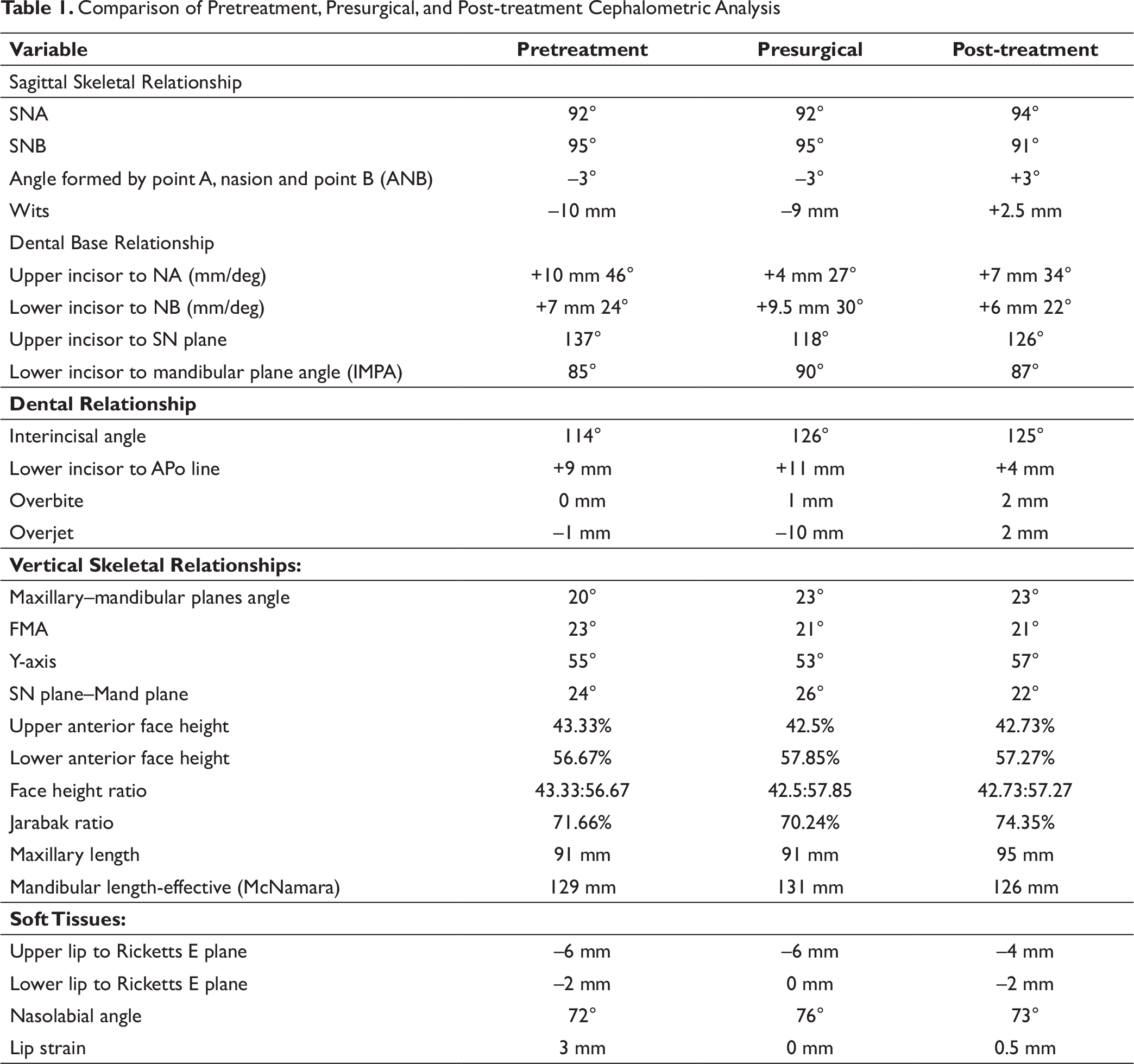
Comparison of Pretreatment, Presurgical, and Post-treatment Cephalometric Analysis
Diagnosis
Skeletal class III bases due to macrognathic and prognathic mandible with hypodivergent growth pattern. Patient showed Angle’s class III molar relation bilaterally and mild mandibular asymmetry.
Dolphin Simulation
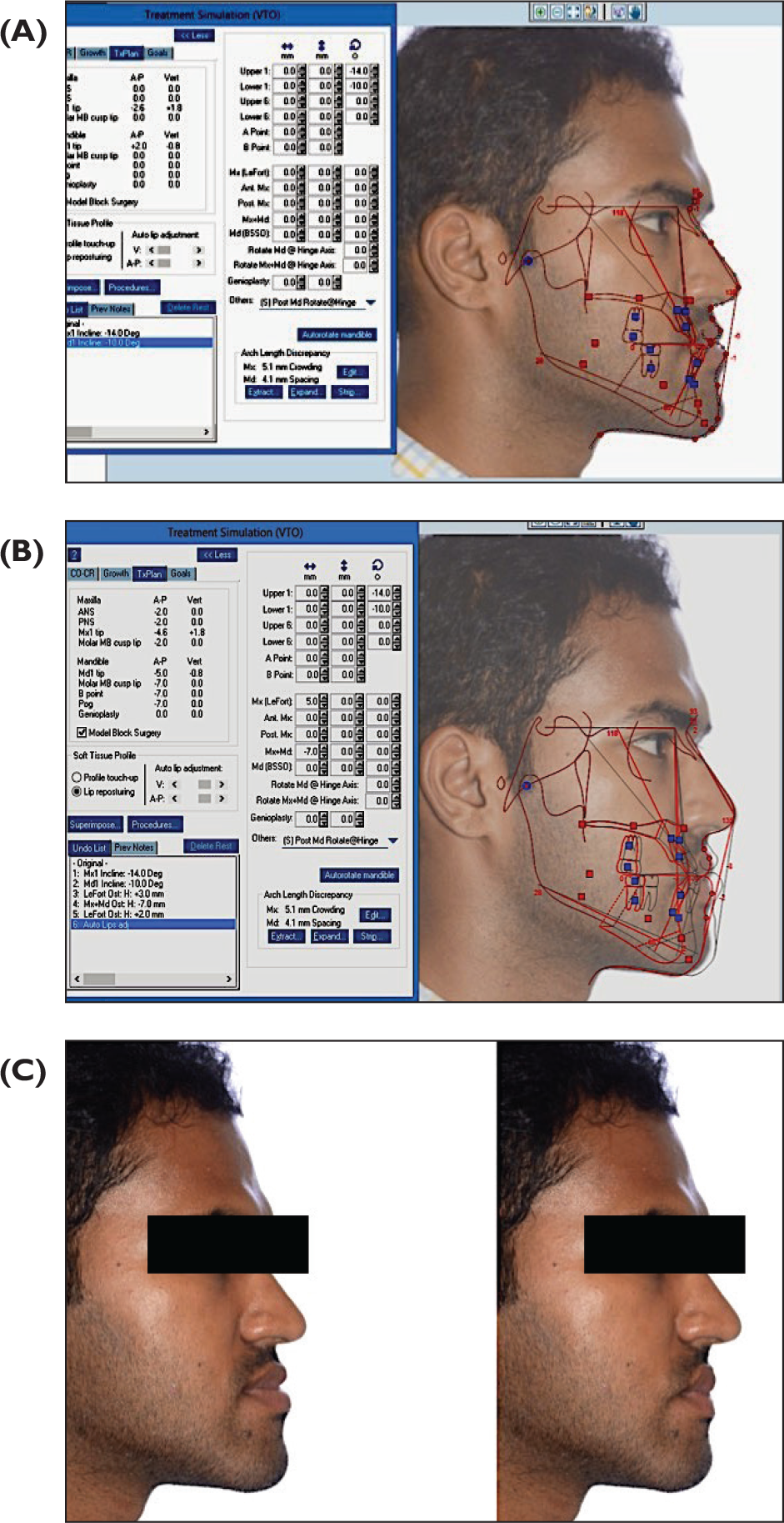
Pretreatment lateral cephalogram was digitized and evaluated on dolphin software. The pre-treatment photograph was superimposed on the lateral cephalogram. The treatment simulation was done with 4 mm anterior sagittal movement of maxilla and 7 mm mandibular setback. After lip repositioning the profile was found to be satisfactory and the plan was finalized (Figure 3A-3C)
Problem List
Concave profile
Skeletal class III malocclusion
Angles class III molar relation bilaterally
Crowding mandibular anterior teeth
Cross-bite wrt 12, 21
Overbite: 0%
Reverse overjet: 1 mm
Discordant midlines
(A-C) Pretreatment Dolphin Simulation
Treatment Planning
The treatment plan was orthosurgical. The decompensation of maxillary and mandibular was planned to gain negative overjet by ext raction of 14 and 24. Bimaxillary surgery (maxillary advancement 3 mm + mandibular setback 7 mm) after presurgical decompensation of the arches.
Treatment Progress
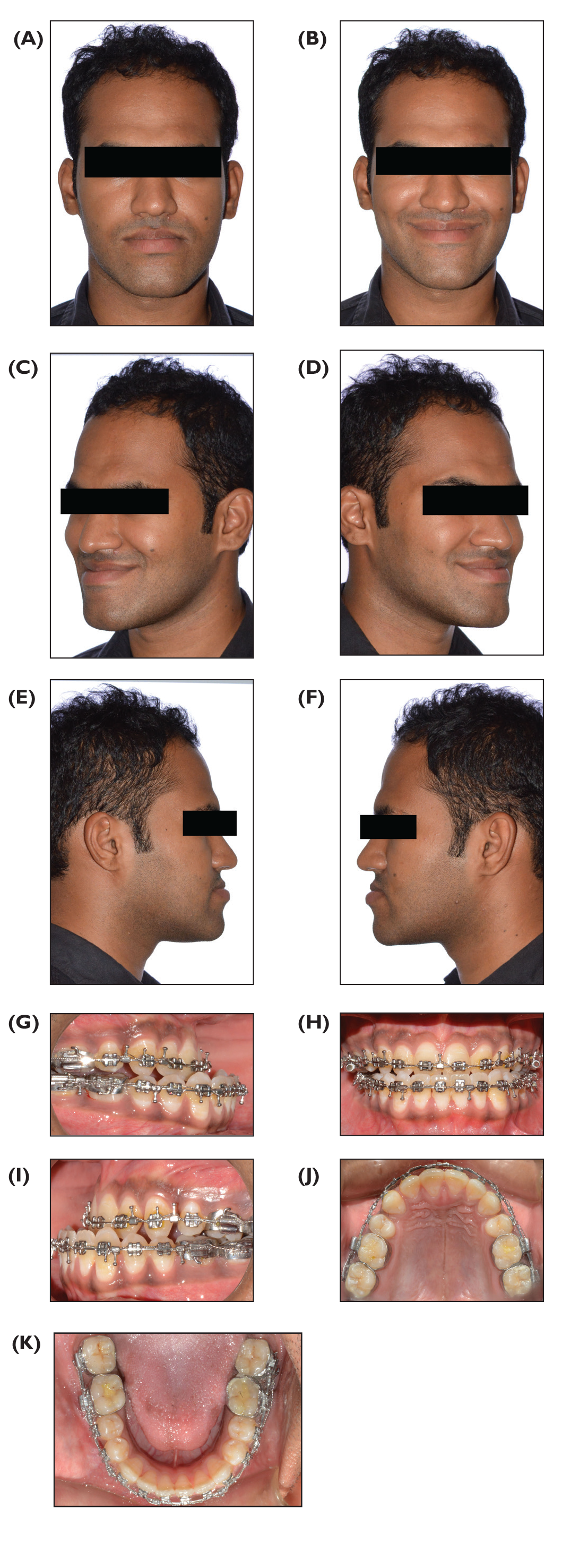
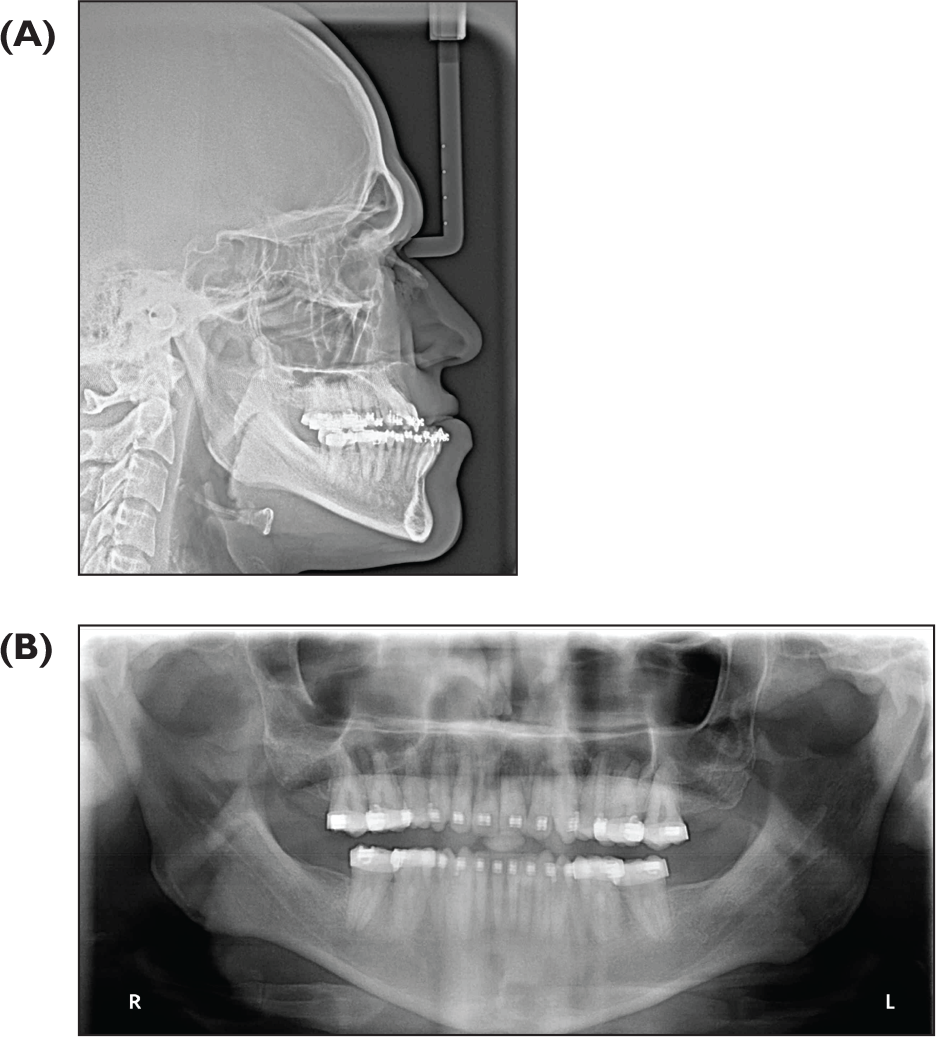
The treatment was started with extraction of 14, 24, 18, 28, and 48 and fixed orthodontic treatment for decompensation. Levelling and alignment were achieved till 0.017 × 0.025 SS in the maxillary arch and 0.016 × 0.022 in mandibular arch. Class II mechanics were used for retraction of maxillary incisors and proclination of mandibular incisors. Decompensation was complete with a negative overjet of 8 mm after 18 months of treatment (Table 1). Figure 4A-4K shows presurgical extraoral and intraoral photographs. Presurgical lateral cephalogram and OPG is shown in Figure 5A and 5B.
(A-K) Presurgical Extraoral and Intraoral photographs
(A, B) Presurgical Lateral Cephalogram, OPG
Presurgical Mock Surgery
Facebow transfer was done to orient the maxilla to the semiadjustable articulator. Wax bite in occlusion was taken to fix the mandibular model. Horizontal lines at a distance of 10 mm were drawn parallel to occlusal plane. Vertical lines were drawn passing through mesio-buccal cusp of first molars and cusp tip of canines. Maxilla was advanced 3 mm with reference to the horizontal and vertical lines. Intermediate acrylic splint was formed at this position. Another pair of models were articulated in the final position after mandibular set back and final splint was prepared.
Postsurgical Management
Bimaxillary surgery (maxillary advancement 3 mm + mandibular setback 7 mm) was done. Patient was kept on class III elastics to prevent any relapse postsurgically for 6 weeks. The surgical wires were removed, repositioning of brackets necessary was done, and vertical settling elastics were given.
Post-treatment Assessment
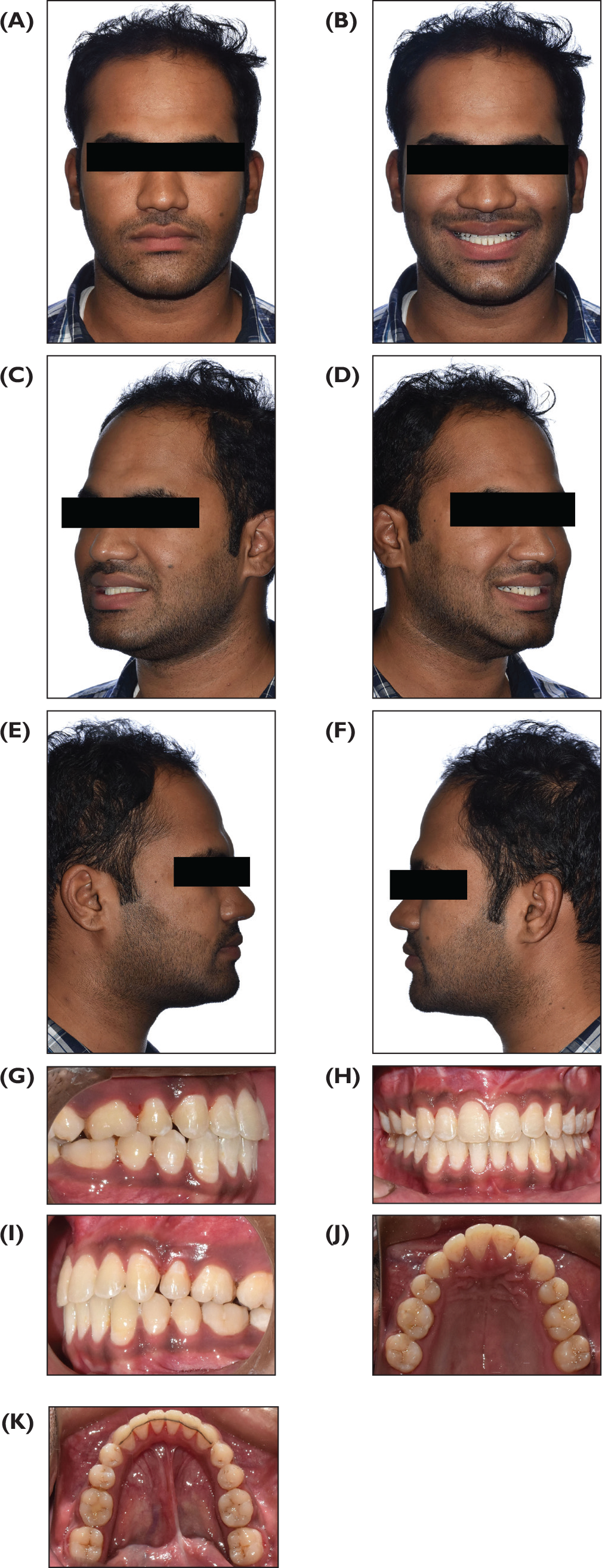
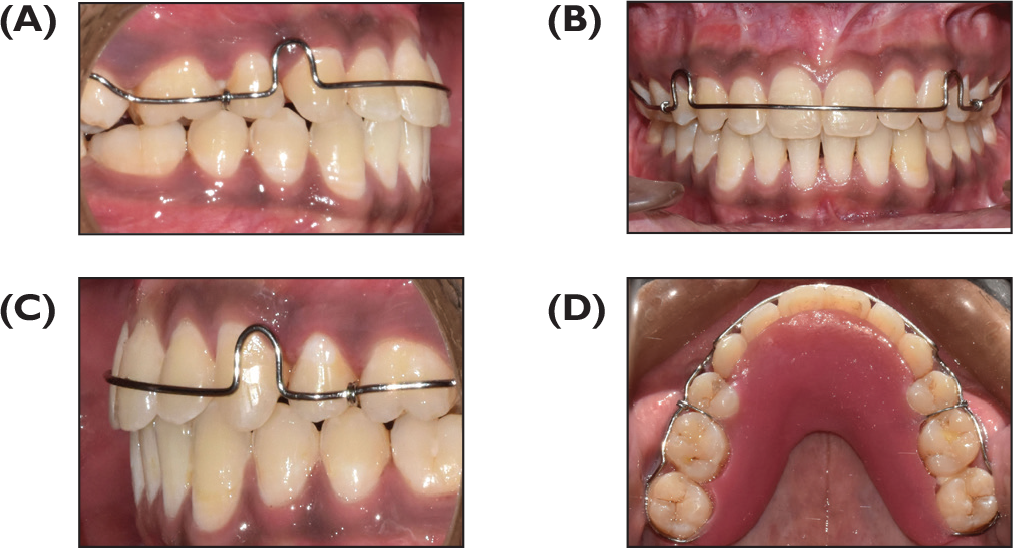
The patient had ideal overjet and overbite of 2 mm and 0% and concordant midlines post-treatment. The case was finished in class II molar relation, class I incisor, class I canine, and premolar relation and canine guided occlusion (Figure 6A-6K). The PAR index showed an improvement of 95.1% posttreatment. Figure 7A-7D shows intraoral photographs with retainers.
(A-K) Post-treatment Extraoral and Intraoral Photographs
(A-D) Maxillary Modified Begg’s and Mandibular Fixed Bonded Retainer
(A-B) Post-treatment Lateral Cephalogram and Orthopantomogram
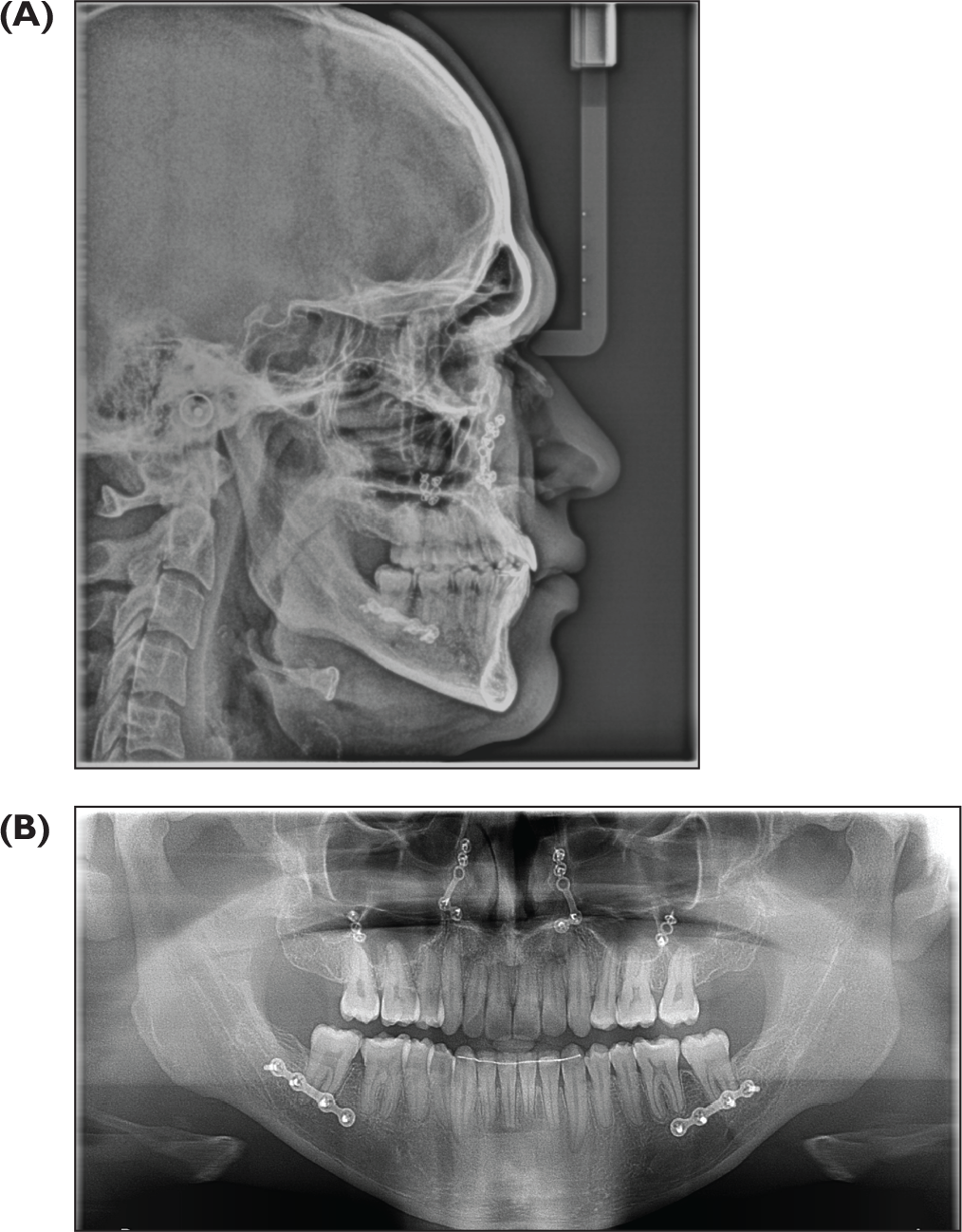
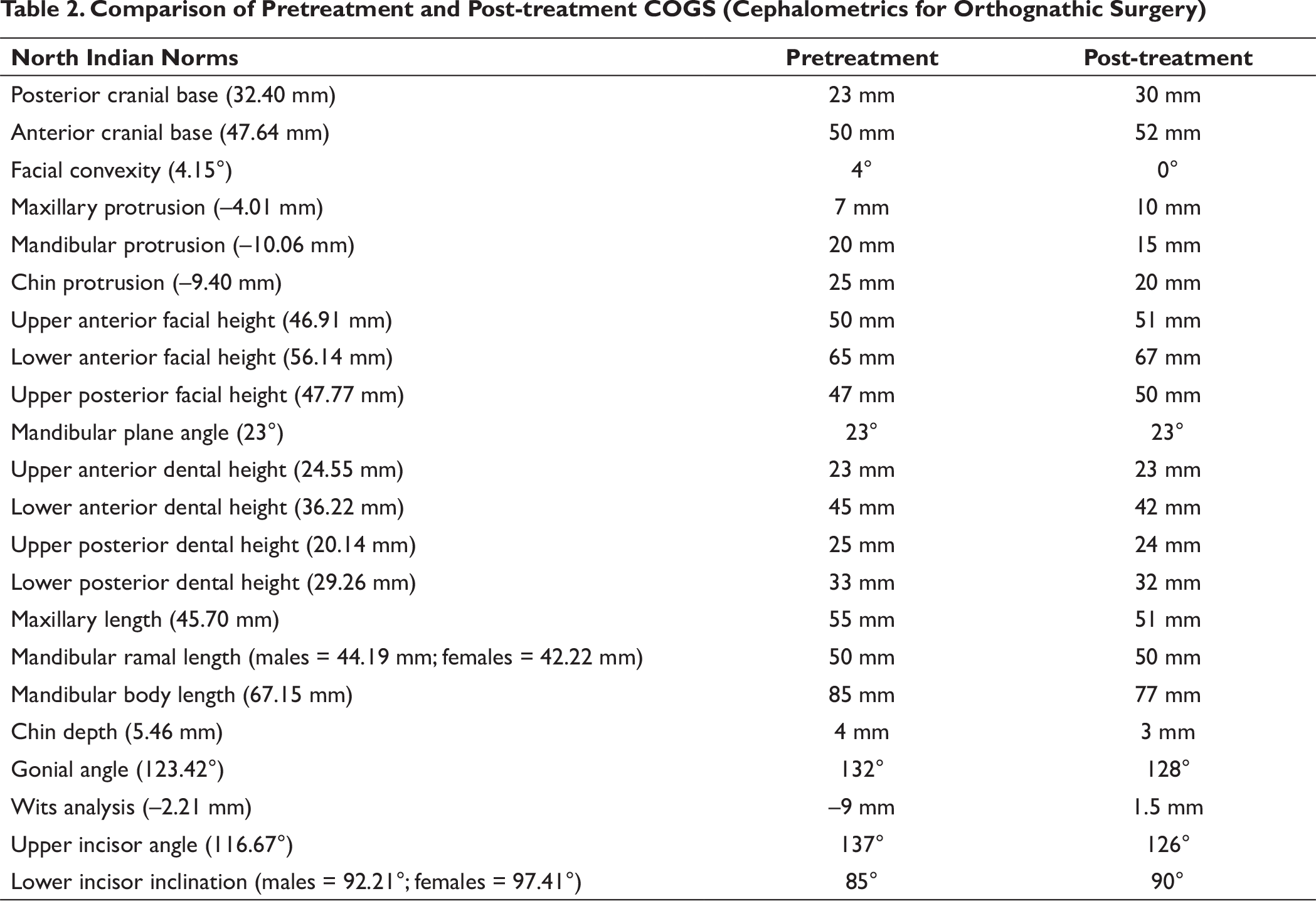
Post-treatment Cephalometric Assessment (Table 2)
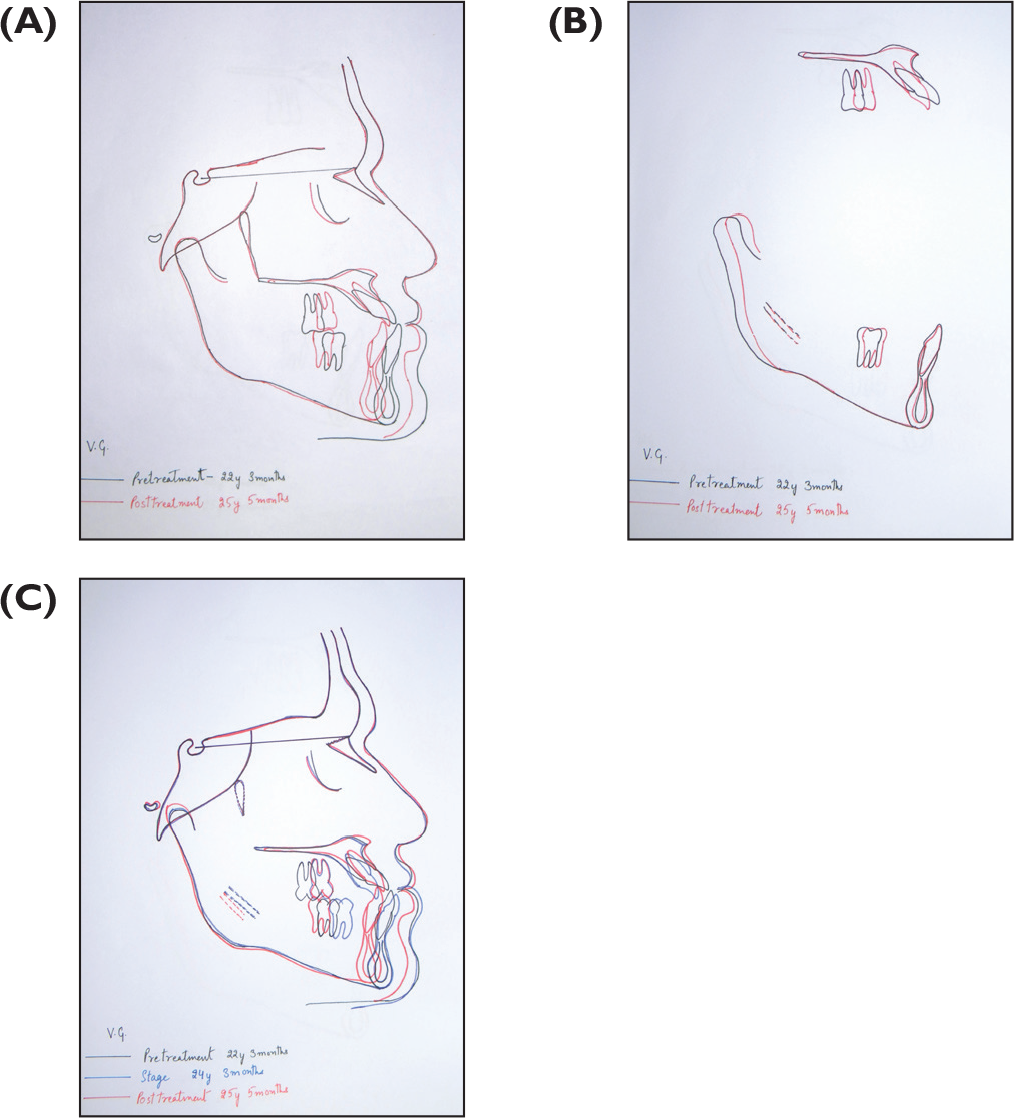
The ANB was improved from –3° to +3° and Wits changed from –10 mm to 2.5 mm, thus showing marked improvement in skeletal class III malocclusion. Maxillary incisor inclination changed from 46° to 34°. There was slight decrease in divergency. Cephalometric superimpositions showed change in position maxilla and mandible before and after surgery (Figure 8). The superimposition of maxilla showed improvement of inclination of maxillary incisors (Figure 9A-9D).
(A-C) Superimposition of Pre- and Post-treatment Lateral Cephalograms
Critical Appraisal
The orthognathic profile was achieved with surgical treatment that addressed the skeletal malocclusion and the concave profile of the patient.
The parallelism of roots was achieved except 46 and 44 that require improvement.
The asymmetry present pretreatment was also addressed.
Microesthetics could have been enhanced by gingival surgery.
IOPAR showed resorption of 11, 12, 21, 22 (Grade 2).
Comparison of Pretreatment and Post-treatment COGS (Cephalometrics for Orthognathic Surgery)
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.