
Abstract
Orthodontics and periodontics have a sophisticated elaborate interdependence as every orthodontic intervention has a periodontal extent. Although orthodontic alignment promotes adequate plaque control, many detrimental effects on the periodontium may be observed during the treatment. Periodontal intervention is required at all stages of orthodontic therapy starting from orthodontist diagnosing a case to mid-treatment analysis of periodontium and also posttreatment investigation of the case. Many a time, successful orthodontic treatment is dependent on the overall maintenance of the health of the periodontium. On the other hand, orthodontic tooth alignment may be used as an adjunctive treatment in periodontally compromised patients. This review will help in better understanding of the orthodontic–periodontal interrelationship for the better framework of the treatment approach to bring out the optimum results in patients.
Introduction
A majority of the population including both adults and children seek orthodontic treatment because of an ever-increasing concern for dentofacial esthetics. Orthodontic treatment is completed by resultant bone turnover so as to move teeth within the alveolus. Since the bony response is facilitated by the periodontal ligament, movement of a tooth is primarily a periodontal ligament phenomenon and requires a healthy periodontium. 1
Orthodontic adjustment of the dentition is advantageous for the maintenance of adequate plaque control, but the process of alignment of teeth through orthodontic therapy may have some detrimental effects on the periodontium through impingement on the gingiva and also by accumulation of plaque and food impaction during the treatment. In addition, an enhanced number of adult patients are becoming esthetically oriented and pursuing orthodontic treatment, making the interdependence between periodontics and orthodontics even more strong and dependable. 2
Periodontal intervention is required at all stages of orthodontic therapy starting from an orthodontist diagnosing a case to mid-treatment analysis of periodontium and also posttreatment investigation of the case. If the orthodontic movement is initiated in cases of gingival inflammation or even if inflammation develops or progresses during treatment, there is an enhanced probability of clinical attachment loss and bone loss. Successful orthodontic treatment usually depends on the maintenance of the health of periodontium before, during, and after orthodontic treatment. 3
This review aims to highlight varied points when periodontal intervention is required before, during, or after orthodontic treatment and also highlight the use of orthodontic treatment as an adjunct to periodontal treatment in periodontally compromised patients.
Malocclusion and Its Effect on Periodontium
Many patients desire orthodontic treatment for esthetic improvement only, but, few malocclusions are likely to traumatize the periodontium, such as impingement of the gingiva in anterior deep bite or recession and mobility of mandibular incisors in anterior crossbite. Orthodontic treatment in such conditions benefits the periodontal health. 3
In misaligned dentition, removal of plaque can be problematic due to the difficulty in reach of brush and floss in such areas leading to increase in inflammation and bleeding (Figure 1). 4 Although there is an increased amount of plaque, inflammation, and bleeding initially with the placement of orthodontic brackets and wires, there is an improvement in the condition during treatment5-7 because of the increased attention to the oral hygiene by the patient and reinforced oral hygiene instructions by the dentist that the patient follows during the course of the orthodontic treatment. 8
There are several potential risk factors leading to clinical attachment loss in orthodontic patients such as greater plaque scores, invasion of the cervical margins of bands subgingivally, deep periodontal pockets, and length of procedure. In patients with reduced but healthy periodontium, orthodontic treatment can be accomplished without irritating the periodontium, but in uncontrolled inflammatory conditions, orthodontic treatment may aggravate inflammation leading to destruction of periodontal tissues even in the patients maintaining adequate oral hygiene. 2
Every orthodontic patient requires an examination by a periodontist, as the tooth and its surrounding structures are continuously being affected by microbial flora and orthodontic treatment might aggravate this condition. Thus, it is imperative that the host tissues are as stable as possible and are free of inflammation during the entire course of orthodontic treatment. Therefore, during patient visit to orthodontic clinic, orthodontists might encounter, during their examination, a non-periodontal patient (children or adult) or a patient with periodontal disease requiring adjunctive treatment.
Orthodontic Treatment in Children/Adolescent Patients
For early recognition of patients with periodontal disease by orthodontists, periodontal examination must be performed before, during, and after orthodontic treatment. 9
Before Orthodontic Treatment
Before any orthodontic treatment, the orthodontist must do a thorough clinical examination that should include assessment of the gingival status, probing depths, mobility, keratinized gingival width, and recession. Examiner must make sure that there is adequate oral hygiene maintenance by the patient and there is no periodontal breakdown. In patients with presence of plaque or gingival inflammation, adequate oral prophylaxis should be done, and the patient should be educated and motivated regarding oral hygiene maintenance throughout the orthodontic treatment. Delay in active orthodontic treatment in patients who are not compliant should be considered until adequate plaque control is attained. 9
There are certain conditions that need careful examination apart from the overall oral hygiene status of the oral cavity. These are as follows:
Gingival Enlargements
Gingival overgrowth (Figure 2) might be present in few patients leading to problematic bonding of brackets and adequate maintenance of plaque, which requires careful diagnosis and planning. 10
Superficial Impacted Teeth
The examiner must be aware that in case of an ideal tooth eruption, the permanent tooth would erupt at the center of the crest of the ridge, conserving both the facial and lingual gingiva. But sometimes teeth fail to erupt into the oral cavity normally and are impacted; this can affect the dental arch form leading to esthetic and functional challenges. Third molars followed by canines are the most commonly impacted teeth.11, 12 Surgical intervention (preventive mucogingival surgery) is often required to expose the impacted canine and it helps in avoiding the periodontal tissue damage. In case of superficially impacted tooth, the tooth could be visualized beneath the gingiva or the mucosa and can be exposed using apically positioned flap before initiation of orthodontic treatment. 13
Gummy Smiles/Excessive Gingival Display
During the initial examination, the clinician may encounter patients with gummy smiles/excessive gingival display. Short clinical crowns in children are frequently related with altered passive eruption. Orthodontic treatment generally precedes periodontal treatment in cases where a combination of altered passive eruption and malocclusion and/or crowding is seen, since leveling of teeth with extrusion or intrusion may effect position of gingival margins. Thereafter, a smile analysis is required so as to assess the nature and extent of gingival display and also to decide whether surgical crown lengthening and/or restorative management of the smile line is needed. 14
During Orthodontic Treatment
Orthodontic appliances usually have a detrimental consequence on oral hygiene condition of patient; thus, reinforced instructions and motivation are required at each visit. In noncompliant patients, orthodontic treatment should be deferred until an evident improvement in periodontal condition is seen. Regular follow-up is advised in all patients throughout active orthodontic treatment, with clinical periodontal evaluation at least every 6 months and radiographic examination at least once a year. In order to improve periodontal condition, orthodontic appliance could be removed and resumed only after the control of the periodontal disease. 9
There are several conditions that need to be addressed during or along with the initiation of the orthodontic treatment. These are discussed in subsequent text.
Deep Intraosseous Impactions
Deep impacted canine might be associated with/without the presence of deciduous canine and there are different surgical approaches for the treatment of the same.
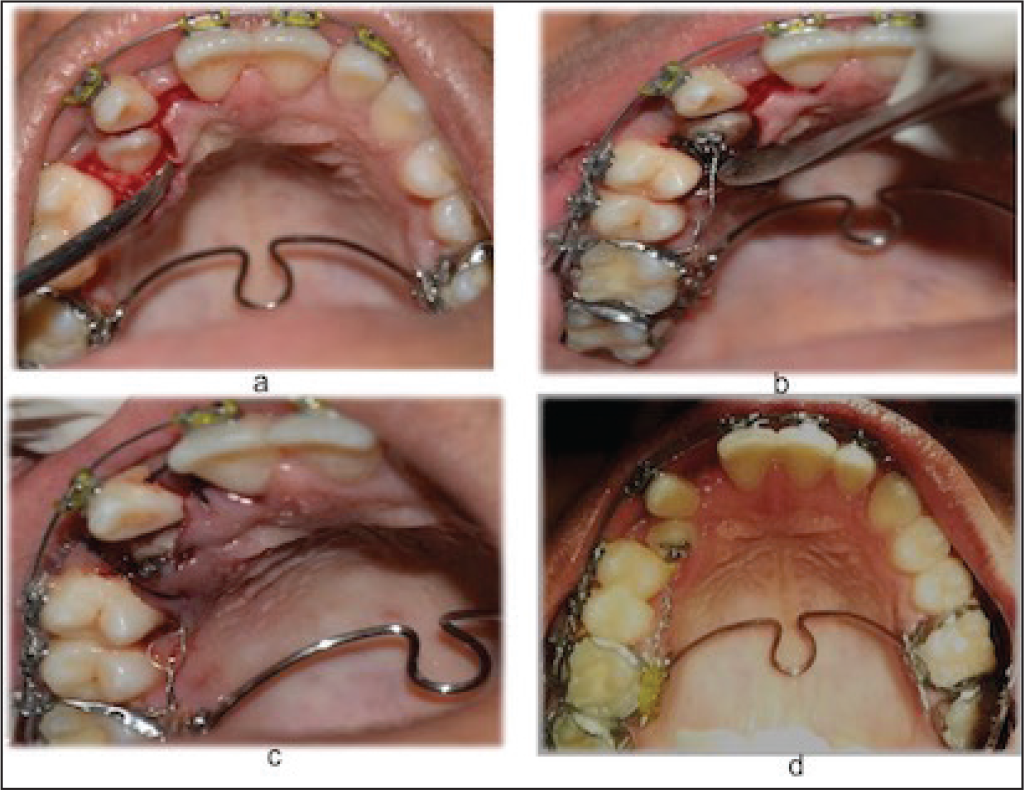
Surgical treatment of labial and palatal impaction not associated with a deciduous canine. Palatally impacted maxillary canine are managed by surgically uncovering the tooth using mucoperiosteal flap and bone removal, followed by placement of bracket leading to autonomous eruption of tooth thereafter before beginning of orthodontic treatment. If properly done, the tooth will erupt autonomously within 6 to 9 months, 13 or it can be pulled slowly through placement of wires along with orthodontic treatment (Figure 3).
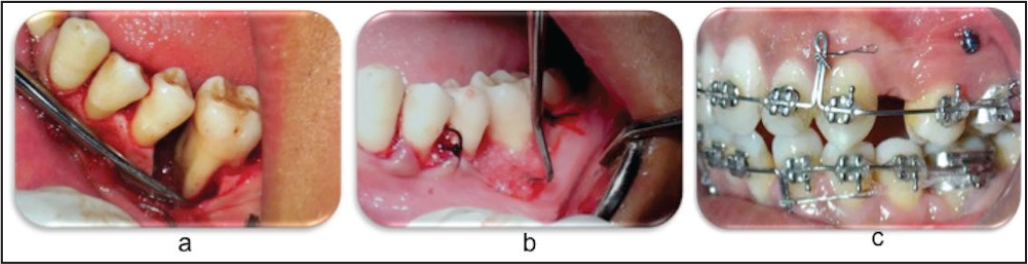
In cases of presence of a labially impacted maxillary canine, surgical procedures are required to expose impacted canine and thereafter its eruption should also provide adequate attached gingiva so as to resist recession and alveolar bone loss. Various techniques are practiced to uncover labially impacted canine such as gingivectomy, apically displaced flap, and closed eruption technique (Figure 4).13, 15-18
Surgical management of impacted tooth associated with a deciduous canine. A technique called “tunnel traction” is performed in such cases where deciduous canine is present in arch and permanent canine is impacted. After the flap elevation and exposure of cusp of permanent impacted canine, extraction of deciduous canine is done. The bone is perforated apically in the socket so as to create a tunnel which connects the socket to the crown of the permanent impacted canine. Through the tunnel, the wire chains connect the socket to the crown of the impacted tooth which serves as an orthodontic traction. Flap is repositioned in its original site. The traction phase begins with the suture removal after 10 days. 13
Ectopically erupting (buccal/lingual) tooth is many a times associated with the inadequate attached gingiva, clinical attachment loss, and bone loss. 19 Buccal eruption may also be associated with thin buccal bone which increases the chances of gingival recession (Figure 5). 20 When deciding for the appropriate treatment simulation of the physiological eruption pattern, ie, eruption of tooth at the center of the alveolar ridge and also pres of adequate and healthy periodontal tissues should be the aim.21, 22
Effect of Malaligned Teeth on Periodontium

Preorthodontic Analysis of Gingival Enlargement

(a) Surgical Exposure and Bone Removal Around Palatally Impacted Canine (b) Placement of Bracket and Traction Wire (c) Suturing (d) Healing After Suture Removal
(A) Surgical Exposure of Labially Impacted Canine and Placement of Bracket and Traction Wire (B) Flap Sutured Back to Its Original Position

Ectopically Erupted Maxillary Canine

(a) Inflammatory Gingival Enlargement in Patient Undergoing Orthodontic Treatment (b) Treated Using Gingivectomy

Aberrant Frenal Attachment

Corticotomy

Development of Recession and Inadequate Width of Attached Gingiva During Orthodontic Treatment

Ectopically Erupting Tooth
In case ectopic tooth eruption has started but not completed, interceptive mucogingival surgery preserves and repositions the keratinized tissue entrapped between the erupting permanent and its deciduous tooth. Different mucogingival surgeries are performed on buccally erupting teeth depending on the position of erupting teeth in relation with the mucogingival junction 13 : double pedicle flap (when the tip of the cusp erupts in the keratinized tissue close to the mucogingival junction), apically positioned flap (when erupting apically to the mucogingival junction), and free gingival graft (when erupting in the alveolar mucosa very apically to the mucogingival junction).
Gingival Hypertrophy/Pseudopockets
Inflammatory gingival enlargements may occur in patients undergoing orthodontic treatment (Figure 6a). Regular follow-ups and oral prophylaxis can improve the condition. If the condition does not improve even after regular scaling, gingivectomy (Figure 6b) is usually considered for restoration of requisite tissue morphology. 10
Aberrant Frenum
Timing and need for frenectomy is a controversy among orthodontists. Many orthodontists favor the concept of waiting till the eruption of all 6 permanent anterior teeth in cases of abnormal frenum. Frenectomy in conjunction with orthodontic treatment is the choice of treatment if diastema remains even after eruption of all 6 permanent anterior teeth,23, 24 and it should be done after the initiation of orthodontic treatment and 6 weeks before the removal of the appliance (Figure 7). This is recommended as it permits healing, tissue maturation, and does not extend orthodontic treatment. 25
Patients to be Treated by Corticotomies
When certain malocclusions cannot be orthodontically camouflaged and but do not require extensive orthognathic surgery, periodontally accelerated osteogenic orthodontics26-28 (Figure 8) and selective alveolar decortication may be viable treatment options in addition to conventional options to hasten orthodontic tooth movement with lesser adverse effects. 29
Mucogingival Deformities
A mucogingival deformity, such as inadequate width of attached gingiva or gingival recession, may develop during (Figure 9) or after orthodontic treatment and necessitate mucogingival reconstructive procedures to repair or reconstruct the destroyed periodontal tissues. 13
For patients who are compliant, have healthy periodontium and adequate plaque maintenance, and require orthodontic tooth movement within the envelope of alveolar bone, mucogingival grafting procedure can be done post orthodontic treatment, even if it is associated with thin periodontal morphotype, aberrant frenal attachment, or inadequate attached gingiva.
On the other hand, in cases of poor oral hygiene or requirement of orthodontic movement outside the envelope of alveolar bone, recession augmentation must be planned prior to the orthodontic treatment. In such patients, if recession develops during movement then it is recommended that active movement be stopped and root coverage procedure should be accomplished first. The orthodontic treatment can be started again after complete healing.30-32
Following Orthodontic Treatment Completion
The plaque-retaining appliances such as orthodontic retainers may cause inflammation and periodontal disease. Post orthodontic treatment completion, regular recall appointments help in timely detection of aggressive periodontitis in young adults and adolescents. As a part of the follow-up, patients are advised for regular periodontal examination along with radiographic evaluation every year. 9
Following an orthodontic treatment, relapse is commonly seen which is due to the presence of gingival and periodontal fibers that are stretched during the treatment and have a tendency to pull the teeth to its native position. 10 Circumferential supracrestal fiberotomy should be carried out in the final stages of orthodontic treatment to severe the attachment of transseptal and supracrestal fibers around the tooth so as to prevent relapse of the rotated tooth after the orthodontic procedure.33, 34
Orthodontics in Adult Patients
Non-periodontal Patients
In adult patients without any periodontal treatment, dentofacial esthetics is the main driving force and the cause of seeking the orthodontic treatment. 35 They are usually younger adults who desired but failed to undergo orthodontic treatment during adolescent period and now because of social pressure are concerned about their esthetics rather than dental health and function. 36 In patients without any periodontal diseases, the orthodontist treatment plan remains same as that of children with only periodontal considerations being the resolution or control of inflammation throughout the orthodontic treatment. Apart from that there are many clinical as well as psychological and biological variations between the orthodontic treatment of adolescents and adults that make adult orthodontics different and challenging requiring special concepts and procedures. Adults have more specific objectives and concerns as far as esthetics is concerned, orthodontic appliances also differ, and treatment time span is also different. There is an increasing demand of invisible appliances, shorter treatment duration, application of lighter forces, and more precise tooth movement leading to the emerging concept of Periodontally accelerated osteogenic orthodontics. The orthodontist must be careful that patients with gingival recession or active periodontal disease are not good contenders for periodontally accelerated osteogenic orthodontics. 37
Periodontal Patient
It is of prime importance to recognize and diagnose patients accurately because with an increase in age of the patient, an increase in susceptibility to periodontal disease has also been observed; and thus it becomes rather more crucial to congruously treat patients with periodontitis who requires orthodontic therapy. 38 Adult patients with periodontal disease are classified into two categories. First category consists of patients who earlier had periodontal disease but are treated now. In such patients, the orthodontic consideration remain the same as mentioned in children as they require comprehensive orthodontic treatment because of their esthetic consciousness. Second category consists of adult patients who require orthodontics as an adjunct therapy. They have other related dental issues and need orthodontics as a part of larger treatment plan involving multiple dental specialties.
The orthodontic-periodontal cases can be managed by the following ways:
Preorthodontic osseous surgical treatment Use of orthodontic treatment as an adjunct to periodontal treatment Post orthodontic treatment of residual periodontal defect
Preorthodontic Osseous Surgical Treatment
Prior to any orthodontic treatment, initial periodontal therapy is suggested for reduction of inflammation. In cases where good plaque control can be obtained and bleeding on probing can be eliminated even in the presence of remaining mild to moderate periodontal pockets, orthodontic treatment along with periodontal maintenance procedures is done first and thereafter phase II (surgical) periodontal therapy is planned. After initial periodontal therapy if pocket depth and bleeding on probing are not eliminated, open-flap debridement is considered first. 38
Regenerative periodontal treatment is recommended prior to orthodontic tooth movement in case of deep intrabony defects (Figure 10) 39 or craters as these defects do not improve with orthodontic treatment. This is because deep periodontal defects cannot be completely cleaned, and unfavorable crown-root ratio and clinical attachment level is attained post osseous resection. Orthodontic treatment may be started when the results of periodontal treatment are stable following 3 to 6 months of periodontal surgery.40, 41
Use of Orthodontic Treatment as an Adjunct to Periodontal Treatment
Hemiseptal defects. In mesially tipped tooth or supraerupted tooth, hemiseptal defects are found. Uprighting these teeth appears to shallow out the angular defects, with new bone forming at the mesial alveolar crest. In cases of supraerupted tooth, osseous defects could be leveled by intruding the tooth and thereafter adjacent cementoenamel junction could be leveled. Stabilization of these teeth should be done for at least 6 months after the completion of the orthodontic treatment and periodontal reassessment should also be done. Usually no further periodontal treatment is required as the pockets either get reduced or are eliminated. 41
Deep Intrabony Defect Treated Before Initiation of Orthodontic Treatment 39
Severe horizontal bone loss. Patients with advanced/severe horizontal bone loss present level of bone which has receeded several millimeters apical to the cementoenamel junction, leading to disproportionate crown-root ratio. If the crowns of these teeth are aligned, an associated increase in tooth mobility or significant bony discrepancies may be observed that would require periodontal surgeries to resolve the created conditions. Therefore, decreasing the clinical crown length of these teeth seems to be the appropriate treatment option. Also, the level of the bone is considered as a guide to position the brackets on the teeth. Usually most of the cases with initial periodontal defects do not require periodontal surgery post orthodontic treatment.40, 41
Furcation Defect. Furcation areas are difficult-to-maintain areas that can deteriorate during orthodontic treatment. Such patients require thorough instrumentation and need to be maintained for a 2 to 3 months follow-up schedule.
In advanced furcations requiring hemisection, orthodontic treatment should be considered first as it simplifies the concentration of tooth movement. After orthodontic treatment, tooth may be hemisectioned.40-42
If such advanced furcation teeth are planned to be used as abutments for a bridge, then orthodontically separating the roots apart leads to desirable restoration. Hemisection, endodontic treatment, and periodontal surgery should be done before beginning the orthodontic treatment. Managing the case in such a manner permits the space created to be cleaned with greater ease and also leads to the elimination of the furcation. 43
Molars with grade III furcation defects may be associated with short or fused roots, severe bone loss, or other factors which hinder both the hemisection and placement of crowns on the remaining roots. Extraction and placement of an implant in such cases would be an appropriate treatment plan which can also facilitate prerestorative orthodontic treatment by becoming an anchor. 41
Root Proximity. The health of the periodontium and accessibility for restoration of posterior teeth is compromised in cases where the interradicular distance is less. Hence, in such cases the roots can be moved apart using orthodontic treatment leading to formation of bone in the adjacent roots by widening embrasure beneath the contact point. It also provides increased bony support and patient’s access to the interproximal region is enhanced. If the roots are to be moved apart using orthodontic treatment, this plan should be made before bracket placement because occlusal contacts may require equilibrium to improve occlusion when the roots are separated.40, 41
Fractured Teeth and Forced Eruption. Fracture extending beneath the gingival margin and terminating at the level of ridge of alveolus does not indicate restoration of the fractured crown as the preparation would extend to the bone level, leading to violation of biologic width with resultant inflammation. For restoration of such teeth, fracture margin should be moved coronally by erupting the fractured root out of the bone. However, when the fracture extends too far apically, extraction and replacement with implant or bridge should be the treatment plan.40, 44, 45
Hopeless Teeth Maintained for Orthodontic Anchorage. Teeth having advanced periodontal disease are considered hopeless and need to be extracted before orthodontic treatment. However, these teeth may be used for orthodontic anchorage if periodontal inflammation can be controlled by non surgical or surgical periodontal therapy
A 6-month stabilization period is required to reevaluate the periodontal status after the orthodontic treatment. Occasionally, in some cases, prognosis of hopeless teeth improves and they are retained but mostly they are extracted after orthodontic treatment.40, 41
Uneven Gingival Margins. Abrasion of the incisal edges or delayed migration of the gingival margins may lead to uneven gingival margins between the adjacent teeth. The solution to such problems could be either repositioning the gingival margins orthodontically or surgically correcting it. The choice must be determined on the basis of following points:
No correction is generally required if gingival margin discrepancy is present between two maxillary central incisors but it is not exposed on smiling. If uneven gingival margins are visible and labial sulcular depth is deep in shorter tooth, excisional gingivectomy is indicated; but if sulcus depth of the short and the long incisors are almost same, gingival surgery is not recommended. If the shortest central incisor is longer than the adjacent lateral incisor, extrusion of the longer central incisor and equilibration of the incisal edge is required. This moves the gingival margin coronally and eliminates the gingival margin discrepancy. In abraded or overerupted teeth, one incisal edge may be thicker than the adjacent tooth. In such cases, the best method of correcting the gingival margin discrepancy is to intrude the short central incisor which moves the gingival margin apically and permits restoration of incisal edges.40, 41, 46-48
Abraded and Overerupted Tooth. Certain destructive habits such as protrusive bruxism lead to abrasion of anteriors with resultant overeruption of teeth. At times, these teeth could not be restored because of inadequate length of the crown being present, leaving the clinician with following two treatment options:
Crown lengthening by gingivectomy/apically repositioned flap Orthodontic tooth intrusion
41
Crown lengthening by gingivectomy/apically repositioned flap: Gingivectomy is indicated in the presence of excess keratinized gingiva and an underlying bone crest at 3 mm or more from the level of gingival resection. Adequate apicocoronal height of keratinized gingival tissues of at least 3 mm should remain after surgery in the presence of subgingival restorations.49, 50 Orthodontic tooth intrusion: Orthodontic intrusion of teeth is done in patients with overeruption of the maxillary anteriors with normal vertical maxillary development. It is necessary to hold these teeth for at least 6 months in the intruded position, so that the principal fibers accommodate to the new intruded position. This procedure is usually a distinct advantageous procedure over crown lengthening unless the patient has extremely long and broad roots or has had an extensive horizontal periodontal bone loss.
41
Missing Papilla. A careful analysis of (a) distance between the contact point and bone crest, (b) papillary height in the interdental area, (c) root divergence, and (d) shape of teeth should be done to determine the correct treatment. Orthodontic treatment can help restore lost interdental papilla, if the root angulation is divergent. By closing open contacts the interproximal gingiva is squeezed and is moved incisally by creating a more esthetic papilla. In cases where the position of the interproximal bone level is apical, eruption of the adjacent teeth is considered. 41
Gummy Smile. Gummy smiles should be evaluated before orthodontic treatment is initiated as it could be because of (a) short upper lip, (b) hypermobility of upper lip, (c) vertical maxillary excess generally associated with excessive lower facial height, (d) anterior dentoalveolar extrusion, and (e) short clinical crown. Therefore these needs to be treated accordingly. 19
Postorthodontic Treatment of Residual Periodontal Disease
Patients should be put on regular follow-ups and maintenance after the orthodontic tooth movement is completed.
Periodontally hopeless teeth that served as an anchorage during orthodontic treatment can be extracted now.
Any residual periodontal pocket or newly formed pockets should be checked and pockets with associated deep intrabony defects can be treated now using regenerative surgical techniques.
Resective osseous surgeries can be planned in residual pockets with horizontal bone loss.
After orthodontic treatment is completed, patients with adequate plaque control, narrow gingival recessions, and those requiring tooth movement within the alveolar bone envelope can be treated now (Figure 11). Lingual movement of the tooth into a more proper position will lead to decrease in recession and dehiscence.13, 30-32, 40
Recession in Teeth 31, 41, 42 can be Treated Postorthodontic Treatment Evaluation

Conclusion
The relationship between periodontal health and orthodontics is intimate and inseparable. On the one hand, orthodontics could help in removal of plaque-retentive areas, and on the other hand, a stable periodontium helps in the overall success of the orthodontic tooth movement. Patients with periodontal disease could be dealt with periodontal-orthodontic comanagement without any detrimental effects. However, there are two important prerequisites: maintenance of meticulous oral hygiene of the patient, and optimal control of inflammation before and throughout the combined treatment. When adult patients are being treated, the periodontist should be aware about the advantages of orthodontic treatment, and it is as important as it is the orthodontist’s knowledge to recognize which patients need to be referred, which require periodontal evaluation, and which require possible periodontal therapy.
Permission/Acknowledgment
We would like to thank Journal of Indian Society of Periodontology to give us permission to use figures (Figure 10).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.