
Abstract
Aim: To evolve a new cephalometric estimation called the MKG angle using three skeletal landmarks—point key ridge (KR), point M, and point G to evaluate the sagittal relationship between the maxilla and mandible.
Materials and methods: A total of 60 pretreatment lateral cephalograms were selected and segregated into classes I, II, and III groups on the basis of ANB angle, Wits appraisal, and W angle. The MKG angle was constructed between the lines drawn from point M to point KR and point KR to point G. The MKG angle was measured to calculate the mean and the standard deviation.
Results: After using the one-way analysis of variance and the Newman–Keuls test and running ROC curves, the results showed that an MKG angle in the range 51º–59º can be considered to have a class I skeletal pattern. The MKG angle more than 59º indicates a class II skeletal pattern and less than 51º indicates class III skeletal pattern.
Conclusion: The MKG angle can be used as a dependable marker to assess sagittal jaw discrepancy.
Introduction
Cephalometric analysis plays a pivotal role in orthodontic diagnosis and treatment planning. An accurate assessment of the antero-posterior (AP) jaw relationship is a requisite step in orthodontic practice as rectifying it alone can do wonders in improving appearance. So far, various angular and linear cephalometric measurements have been proposed to assess the sagittal jaw relation or discrepancy between maxilla and mandible to assist orthodontic clinicians and researchers.
Most popularly used parameter is angle ANB which was introduced by Reidel in 1952. 1 The nasion being unstable with age questions the reliability of the ANB angle as an indicator of apical base discrepancies. 2 Also, the rotation of head while obtaining a lateral cephalogram or jaw rotation occurring as a result of growth or orthodontic treatment has a direct influence on the ANB angle.3–5 To subdue problems related to the ANB angle, Jacobson introduced “The Wits appraisal” relating points A and B to the functional occlusal plane. 6 However, Wits appraisal also has a limited value when consecutive comparisons were performed throughout orthodontic treatment as it describes changes in the occlusal plane instead of pure AP changes of the jaws. 7 Hence, a measurement that is unconstrained of cranial reference planes or the dental occlusion, reflecting the true skeletal AP relationship without being influenced by changes in relation to other parameters, would be expedient in determining the apical base relationship.
Despite the fact that the Beta angle 8 does not use the cranial reference planes, it uses points A and B, which are subjected to change due to regional remodeling,9, 10 and also point C is puzzling to be located on the lateral cephalogram.11, 12
Off lately two more angles, Yen angle 13 and W angle, 14 were introduced to address the drawback of the Beta angle. However, the rotation of jaw either due to growth or orthodontic treatment can be vulnerable to accuracy of the Yen angle. Although the W angle is not affected by the rotation of jaws, it depends on Point S, the midpoint of Sella Turcica which again is an unstable landmark as reported by many studies.15, 16
So, the need for the study was to locate a point which would be free from cranium but constant in relation to its growth. As coined by Atkinson, “key ridge” (KR) that is the lowest point of infrazygomatic crest is a strong buttress of bone which descends and goes forward from the zygoma to the maxillary bone and acts as a support for the maxillary first molar. 17 Bien stated that the KR remains constant in relation to the bones of the cranium throughout life. 18
Despite being proven as an excellent diagnostic marker, 19 the literature shows very few studies that have been done using the KR as a landmark for sagittal discrepancy. Hence, this study aims to introduce a new parameter using the KR to assess true sagittal maxilla-mandibular discrepancy.
The aim of the paper is to develop and test the reliability of a new cephalometric parameter called the MKG angle which consists of three skeletal landmarks—point KR, point M, and point G to assess the sagittal relationship between the maxilla and mandible.
This study was designed to define the mean value and the standard deviation (SD) for the MKG angle in a population with class I skeletal base pattern. It was also conducted to substantiate if any statistically significant difference exists between the mean values of the MKG angle among classes I, II, and III skeletal base population groups.
Methodology
Source of Data
The sample comprised of 60 standardized pretreatment lateral cephalograms of subjects (age 15–25 years) who had reported the Department of Orthodontics and Dentofacial Orthopedics in our institute for orthodontic treatment.
Method
A total of 150 pretreatment lateral cephalograms were traced on an acetate paper using a 0.5 mm lead pencil. Once the lateral cephalograms were traced, the routinely used parameters such as the ANB angle, Wits appraisal, and W angle to determine the sagittal discrepancy were constructed and measured by the same investigator to avoid inter-observer errors. Out of 150 screened lateral cephalograms, 60 lateral cephalograms were selected and subdivided into 3 groups of 20 each, that is, classes I, II, and III skeletal groups, based on the following inclusion and exclusion criteria.
Inclusion Criteria
Class I: ANB angle 1–4, WITS appraisal 0–4 mm, and W angle 51–56.
Class II: ANB angle >4, WITS appraisal >4 mm, and W angle <51.
Class III: ANB angle ≤0, WITS appraisal <0 mm, and W angle >56.
Permanent dentition with no missing teeth.
Patients with age group between 15 and 25 years.
Exclusion Criteria
Patients subjected to prior orthodontic treatment.
Patients with cranial or facial malformation and history of craniofacial trauma.
Poor quality of cephalograms.
The MKG Angle
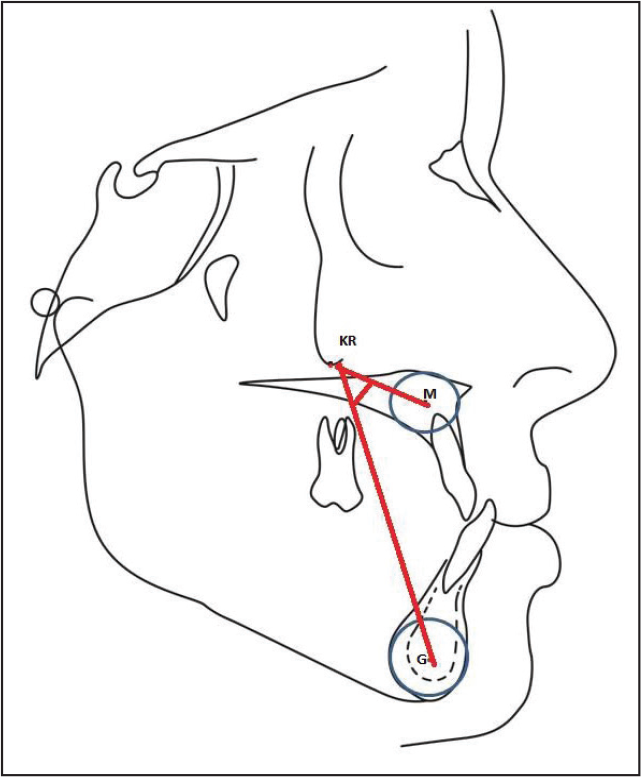
The MKG angle is a new parameter for assessing the sagittal apical base discrepancy. It uses the three skeletal reference points, that is:
The centers of premaxilla and mandibular symphysis were identified by constructing a template with concentric circles whose diameters increased in 0.5-inch increments. The center of the template was marked, and points M and G were identified on the tracings.20, 21
The two lines that would form joining these points are:
Line 1: connecting points M and KR Line 2: connecting points KR and G.
The MKG angle was constructed between lines 1 and 2 drawn from point M to point KR and point KR to point G as shown in Figure 1.
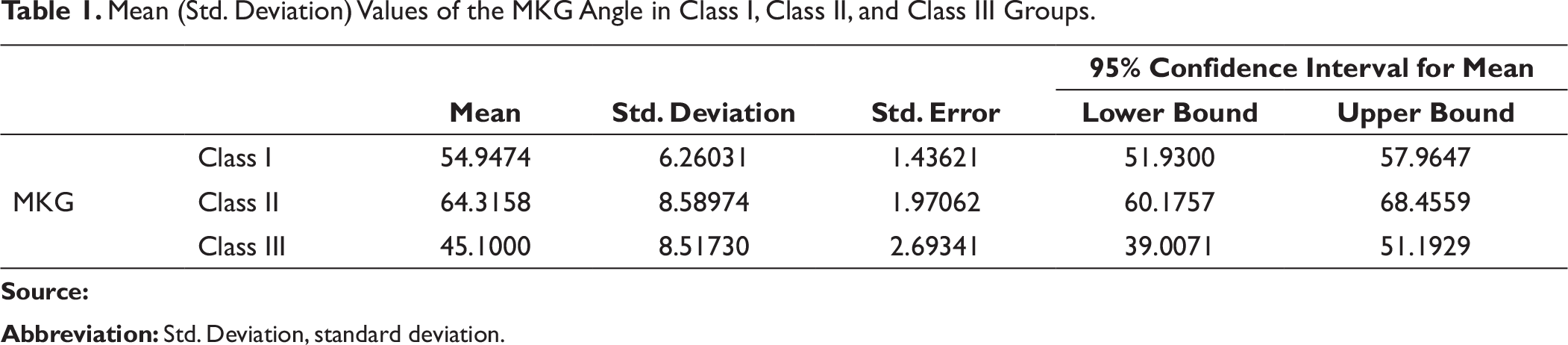
Mean (Std. Deviation) Values of the MKG Angle in Class I, Class II, and Class III Groups.
Statistical Analysis
The data collected were tabulated and summarized as mean ± SD. Groups were compared by factoral analysis (gender and class) of variance (ANOVA) and the significance of mean difference within each group and between the groups was calculated by the Newman–Keuls post hoc test. Groups were also compared by one-factor (Class) ANOVA followed by the Newman–Keuls post hoc test. Receiver-operating characteristics (ROC) curves analysis was performed to examine the sensitivity and specificity of the MKG angle as a test to discriminate between the three different skeletal pattern groups. A P value ≤0.05 was regarded to be statistically significant. SPSS version 14 was used to perform all statistics.
Results
Student–Newman–Keuls Testing for Pairwise Comparisons of Group Means

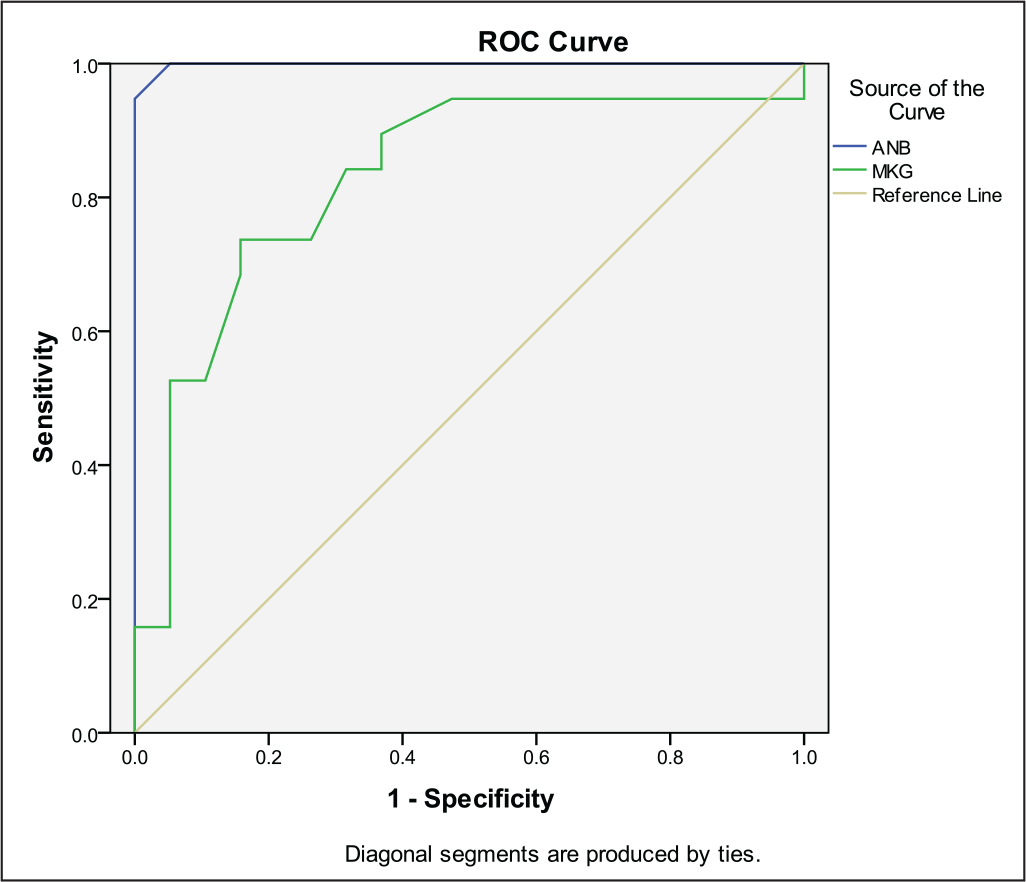
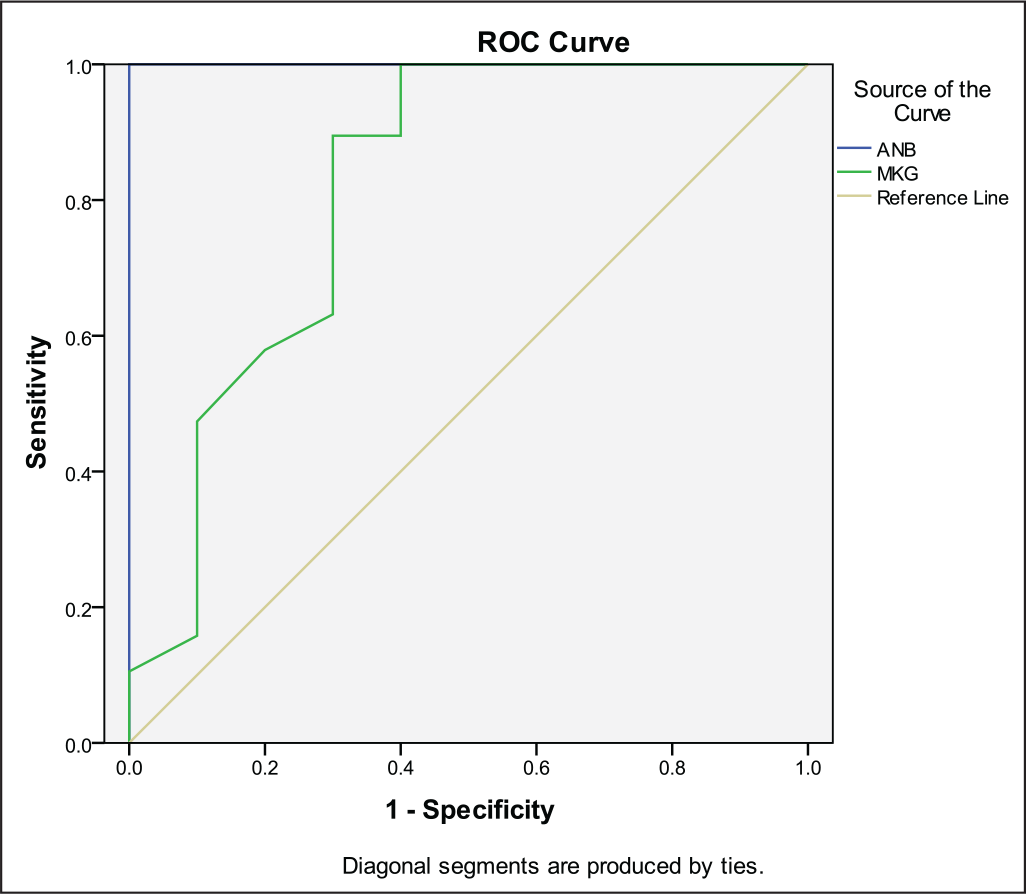
Therefore, the ROC curves show that the cut-off point between the class I and class II groups could be considered an MKG angle of approximately 58.5, and the cut-off point between the class I and class III groups could be considered an MKG angle of approximately 51.2. The results also indicate that a class II skeletal pattern patient has an MKG angle greater than 59 and a class III skeletal pattern patient has an MKG angle less than 51.
Discussion
Predicting the correct AP jaw relationship has a crucial role to play in diagnosis and treatment planning. Numerous authors have tried to assess the sagittal skeletal relationship using various landmarks, right from Riedel (ANB angle), 1 Jacobson (Wits analysis), 6 Baik and Ververidou (β angle), 8 Neela et al. (YEN angle), 13 Bhad (W angle), 14 and so on.
However, the most commonly used measurement to assess the skeletal discrepancy is the ANB angle. The ANB angle in normal occlusions is generally 2. The angles greater than 2 indicate tendencies toward class II jaw disharmonies, whereas a negative angle and less than 0 degree reflect class III jaw discrepancies. Numerous authors have explained that the position of the nasion can affect the relationship of the skeletal bases, affecting also the measurement of ANB due to growth, or due to a lack of accuracy when measuring it. 22 Oktay summarized the factors that could affect the ANB angle as: the age of the patient (ANB decreases with age), the nasion position, the rotation of the sella–nasion (SN) line, the occlusal plane, the maxillae and the facial prognathism. 23
To subdue the limitations of angle ANB, Jacobson suggested the use of the functional occlusal plane rather than the cranial base in his analysis known as the Wits appraisal. 6 On an average, points AO and BO coincided in females and in males BO was located 1 mm ahead of point AO. Point BO would be positioned well behind (positive reading) in the class II skeletal jaw discrepancies, whereas in class III skeletal jaw discrepancies the Wits reading would be negative, that with point BO ahead of point AO. The occlusal plane can be easily affected by tooth eruption and dental development as well as by orthodontic treatment.24–26 This can profoundly prejudice the Wits appraisal. Furthermore, accurate identification of the occlusal plane is not always easy or accurately reproducible. 27
Recently, an alternative angle was suggested by Baik and Ververidou named as the beta angle which uses points free from both the cranial base and the occlusal plane and, hence, not affected by jaw rotations. 8 A beta angle between 27 and 35 is indicative of the class I skeletal pattern, whereas a beta angle less than 27 indicates a class II skeletal pattern and a beta angle greater than 34 indicates a class III skeletal pattern. However, landmarks taken into consideration, that is, points A and B are susceptible to remodeling by orthodontic treatment and growth.24, 25, 27 Furthermore, as shown by various studies, the reproducibility of the location of condylion on mouth-closed lateral head films is limited.28–30 Instead of condylion, the center of condyle could be used, but approximation of the center of condyle is difficult. 8 This could give a non-significant error of approximately 1 degree.
Over the years, Yen angle 13 and W angle 14 were derived to address the shortcomings of the beta angle. The Yen angle is susceptible to changes with the rotation of jaws that could either be due to growth or orthodontic treatment. A Yen angle from 117 to 123 could be considered to have the class I skeletal relationship. The Yen angle less than 117 reflects the class II skeletal pattern, whereas greater than 123 reflects the class III skeletal pattern. Although the W angle is not affected by the rotation of jaws, it depends on point S, the midpoint of sella turcica, which is again an unstable landmark as proved by many studies.15, 16 A W angle between 51 and 56 suggests to have a class I skeletal pattern. An angle smaller than 51 is considered to be indicative of the class II skeletal relationship, whereas an angle greater than 56 is considered to be indicative of the class III skeletal relationship.
All other parameters measuring sagittal dysplasia introduced over the years are affected by at least one of the following factors: poor reproducibility of landmarks, patient’s age, growth changes in reference planes, jaw rotations, and changes due to orthodontic treatment. 31
To overcome some of the limitations of the previously discussed parameters, the MKG angle was developed. This measurement does not depend on unstable landmarks or the functional occlusal plane. It uses three stable points—KR, M, and G.
This angle utilizes the skeletal landmarks G and M points to represent the mandible and maxilla, respectively (Figure 1). These points were originally introduced by Nanda and Merrill and later used by Braun and co-workers. They are marked at the center of the largest circle placed tangent to the anterior, superior (represented by the nasal floor), and palatal surfaces of the premaxilla and the internal anterior, inferior, and posterior surfaces at the mandibular symphysis, respectively.20, 21 These points are not affected by local remodeling secondary to dental movements, unlike points A and B. Also, points M and G can be used to assess the growth vector of maxilla and mandible, respectively, which in itself defines the stability of these points even during active growth periods.
Taking the KR in consideration, the forward part of the zygoma and the malar region of the maxilla remodel in conjunction with the contiguous maxillary complex, and their respective modes of growth are similar. As the maxilla lengthens horizontally by posterior remodeling, the malar region also remodels posteriorly by continued deposition of the new bone on its posterior surface and resorption from its anterior surface. This remodeling process keeps this area’s position in the proper relationship to the lengthening maxillary arch as a whole. The cheekbone thereby proportionately matches the maxilla in (1) the directions and amount of horizontal and vertical remodeling relocation and (2) the directions and amount of primary displacement. 32
Limitations and Scope of the Study
Current study included smaller sample size. Further studies are recommended using the larger sample size.
Rotation of jaws can affect the readings.
Key ridge, being a bilateral landmark, can result in errors in identification and variability. Thus, further studies are recommended using digitized software packages.
Conclusion
This study elucidated that the MKG angle could be a potential marker for assessing jaw discrepancy constructed on stable landmarks. Nevertheless, a clinician must be aware of the importance of other cephalometric measurements in the orthodontic treatment planning. The MKG angle in the range 51–59 can be considered to have a class I skeletal pattern. The MKG angle more than 59 indicates a class II skeletal pattern, whereas less than 51 is class III skeletal pattern.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.