
Abstract
Abstract
Objectives: Various fluoride varnishes have shown promising result in preventing enamel demineralization around orthodontic brackets as they do not depend on patient compliance. The objective of the study was to compare the effect of light-curable fluoride varnish (Clinpro XT) and conventional topical fluoride varnish (Fluoritop SR) in preventing enamel demineralization adjacent to orthodontic brackets.
Methods: 20 patients who required extraction of four first premolars for orthodontic treatment were bonded with orthodontic brackets and each premolar received single application of Clinpro XT and Fluoritop SR fluoride varnish in 2 diagonally opposite quadrants and rest 2 premolars acted as control. The sample teeth were debonded and extracted after 1 month and 2 months of varnish application. The samples were sectioned using hard tissue microtome and evaluated under polarized light microscopy to measure the depth of demineralization.
Results: Kolmogorov Smirnov test showed normal distribution of data. Comparison between the study groups with depth of demineralization scores showed statistically significant variation in one-way analysis of variance test. Turkey’s multiple post hoc procedures showed statistically significant difference in the depth of demineralization between all the 3 groups after 1 month and 2 months. Dependent t test showed statistically significant increment in the depth of demineralization in all the 3 groups between 1 month and 2 months.
Conclusion: This study concluded that single application of both Fluoritop SR and Clinpro XT was effective in reducing significant depth of demineralization compared to control. Clinpro XT showed significantly less demineralization compared to Fluoritop SR after 1 month and 2 months of varnish application.
Introduction
Decalcification or demineralization is the loss of calcified tooth material. Areas of enamel demineralization are clinically visible as white spot lesions that occur due to alterations in the optical properties caused by subsurface mineral loss.1, 2 The dissolution takes place due to the acid produced by bacteria present in dental plaque. These lesions mainly develop due to an imbalance between demineralization and remineralization of the enamel.3, 4 The white spot lesions are supposed to be the early signs of enamel caries.1, 5
Enamel demineralization around fixed orthodontic appliances remains an unwanted negative side effect of fixed orthodontic treatment. 6 Orthodontic appliances facilitate the deposition of plaque as the shape and design of orthodontic appliances create potent sites for plaque accumulation. Plaque accumulation also increases due to the use of multiple arch wires, loops, and various elastics throughout the course of orthodontic treatment. Most common areas for plaque accumulation are cervical areas just gingival to bracket base, around excess adhesive materials and loose bands. 7 Poor oral hygiene of the patients and poor patient compliance are also crucial reasons for increased enamel demineralization. Various literatures showed huge contrasting results, from 2% to 97%, in the prevalence of white spot lesions and enamel demineralization associated with orthodontic treatment.8-16
Prevention of this decalcification that may occur during orthodontic treatment is very important because these lesions are unaesthetic, potentially irreversible, and cariogenic. Often patients blame orthodontists for these unaesthetic white spot lesions as these lesions tend to develop during orthodontic treatment. These white spots can progress into cavities, stay stable for a long time, or recover to a certain extent, depending on the oral environment.17-19
Orthodontists are very much aware of this issue and have attempted to prevent it, but demineralization around orthodontic fixed appliances continues to be a problem. Various methods have been put forward to prevent or decrease enamel demineralization but most of these procedures, however, depend on patient compliance which is unpredictable.5, 14, 20
Various techniques have been created to deliver fluoride adjacent to orthodontic brackets to minimize demineralization, without a need for patient compliance. One of them is the application of topical fluoride varnish around orthodontic attachments. Application of topical fluoride varnish is more effective than other fluoride products because it forms a layer over the enamel surfaces and releases fluoride for longer period. The effect of various topical fluoride varnishes has been demonstrated in multiple in vitro and in vivo studies.21-26 But, there are very few studies done on the effect of light-cure fluoride varnish in the reduction of white spot lesions around orthodontic brackets.27-29
Fluoritop SR (ICPA Healthcare Ltd, Mumbai, India) is a topical fluoride varnish with high fluoride content as each milliliter contains Sodium Fluoride I.P. 50 mg equivalent to 22.6 mg of fluoride (22,600 ppm). On the other hand, Clinpro XT (3M ESPE, St. Paul, MN 55144-1000, USA) is a light-curable RMGIC varnish which forms a protective layer and provides a barrier that remains on the tooth for 6 months according to the manufacturer’s claim. Thus, the aims of the study were as follows:
To assess the outcome of single application of a topical fluoride varnish and light-curable fluoride varnish (LCFV) in preventing enamel demineralization around orthodontic brackets after 1 month and 2 months from the beginning of fixed orthodontic treatment using polarized light microscopy in comparison to control. To compare the effect between a single application of a topical fluoride varnish and LCFV in preventing enamel demineralization around orthodontic brackets after 1 month and 2 months from the beginning of fixed orthodontic treatment.
Methodology
In this split mouth study, 20 patients who consented for all first premolar extraction with no or mild crowding were selected from the Department of Orthodontics and Dentofacial Orthopedics of our institution. These 20 subjects were divided into the following sub groups according to the timing of extractions:
10 patients whose all 4 first premolars were extracted after 1 month of bonding. 10 patients whose all 4 first premolars were extracted after 2 months of bonding.
The inclusion criteria were as follows:
Patients whose all first premolars erupted completely without any damage to the buccal surface. Patients with no visible white spot lesion or fluorosis lesion on the first premolars. Patients whose first premolar extraction could be delayed for 1 month or 2 months without delaying the total treatment duration.
The exclusion criteria were as follows:
Patients with carious or restored first premolars. Patients with demineralization or fluorosis on first premolars. Patients with fractured teeth, erosion, or abrasion on first premolars.
For bonding, the teeth were cleaned using oil-free pumice paste, and buccal surfaces of teeth were etched using 37% orthophosphoric acid and preadjusted edgewise stainless steel orthodontic brackets (3M Unitek Gemini Metal Brackets [3M ESPE, St. Paul, MN 55144-1000, USA]) were bonded at the appropriate position on the buccal surfaces of the teeth using standard light-cure composite resin (Transbond XT Light Cure Adhesive Paste [3M ESPE, St. Paul, MN 55144-1000, USA]). Suitable orthodontic treatment was carried out and arch wire was placed and ligated with elastomeric ligature ties. All subjects were instructed not to eat or clean their teeth for 4 hours after varnish application as per manufacturer’s instruction. Each patient was instructed to maintain proper oral hygiene, and a nonfluoridated dentifrice was prescribed for daily use throughout the period of the study.
Each group of patients received fluoride varnish application by using split mouth design. Single application of fluoride varnishes either Fluoritop SR (Figure 1A) or Clinpro XT (Figure 1B) were applied as per manufacturers recommendation30, 31 in 2 diagonally opposite quadrants and no varnish was applied in the other 2 diagonally opposite quadrants which acted as control. As every patient served as his or her own control, randomization was achieved by split mouth design.
For Fluoritop SR group, buccal surface of the selected first premolar was cleaned with water jet and dried with air syringe. Then recommended quantity of varnish was painted on buccal surface directly with an applicator brush around the orthodontic bracket and allowed to dry. 30 For Clinpro XT group, buccal surface of the selected first premolar was cleaned with water jet and then dried with air syringe. Then, 37% orthophosphoric acid was applied on the tooth surface around the orthodontic bracket. After 15 s, the 37% orthophosphoric acid was rinsed and dried with air syringe. Clinpro XT is a 2-paste system and has to be mixed freshly before application. Both the pastes were mixed for 15 s and then painted on the buccal surface of the tooth around orthodontic bracket using an applicator brush. Then the varnish was light-cured for 20 s. 31
Debonding of the brackets was done very carefully using a debonding plier to prevent any enamel microfracture around the base of the brackets. The sample teeth were extracted after 1 month in 10 subjects and after 2 months in other 10 subjects. The roots of the samples were washed thoroughly and kept in 0.1% thymol solution to avoid any fungal growth throughout the duration of storage.
(A) Topical Flouride Varnish [Fluoritop SR (Sodium Fluoride I.P. 50 mg)]. (B) Light-Curable Flouride Varnish (Clinpro XT)

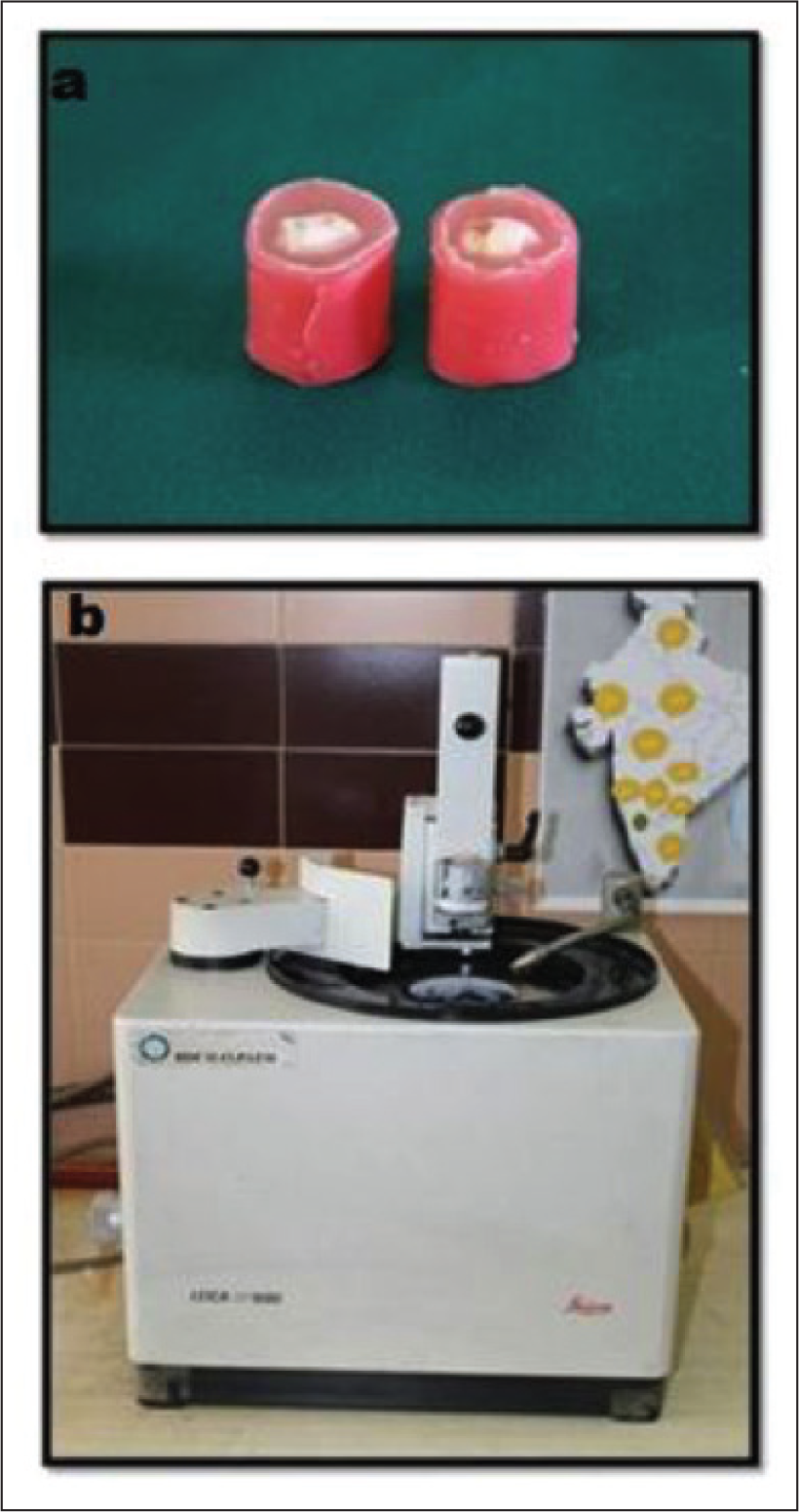
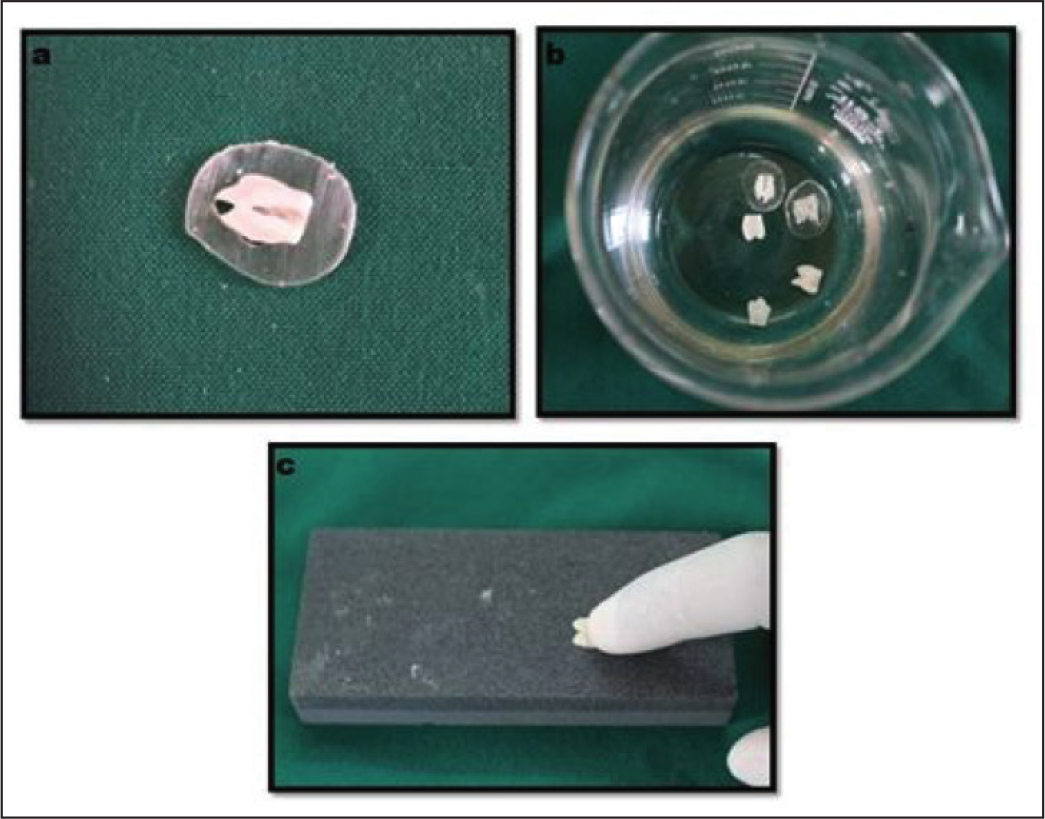
Before sectioning using hard tissue microtome, the roots of all sample teeth were cut 2 mm apical to the cemento-enamel junction. To protect the sample teeth from fracturing during thickness reduction, the samples were placed in a cylindrical-shaped mold made of cold-cured acrylic (Figure 2A). Hard tissue microtome (SP1600 Leica, Germany; Figure 2B) was used for making buccolingual sections of the sample teeth at a thickness of 100 to 150 µm (Figure 3A). Then, buccolingual sections of the samples were kept in acetone solution to dissolve the cold cure acrylic surrounding the section (Figure 3B). Hand grinding was done using silicon carbide combination stone to decrease the thickness of each section to 60-80 µm for better visibility under polarized light microscope (PLM; Figure 3C). After thickness reduction, each section was mounted on glass slides using mountant (Figure 4A) and left overnight for drying. Mounting was done very carefully to avoid the formation of any air bubble around the area of interest.
(A) Samples Embedded in Cold Cure Acrylic (B) Hard Tissue Microtome (SP1600 LEICA, Germany
(A) Bucco-Lingual Sectioning Done Using Hard Tissue Microtome (B) Sections Kept in Acetone to Dissolve Cold Cure Acrylic (C) Thickness of Sections Reduced by Hand Grinding
(A) Mounting Done on Glass Slides Using Mountant (b) Polarized Light Microscope (Leica DMRB, Germany)

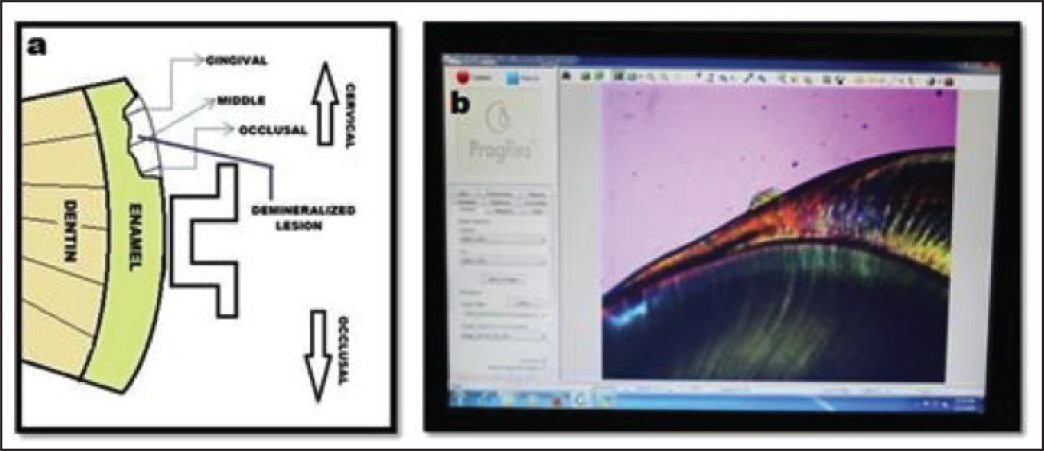
The mounted slides were examined under polarized light microscopy (Leica DMRB, Germany) (Figure 4B) using xylene as imbibed medium by an experienced oral pathologist. Microphotographs of the cervical area of the buccal surface just apical to the bracket base were captured with fixed magnification of 50 times using ProGres SpeedXT core 3 (Jenoptik, Germany) camera. In each section, linear measurements of the deepest part of the gingival, middle, and occlusal zones of the demineralized enamel lesions were taken using ProGres CapturePro 2.8.8 software (Jenoptik, Germany) with the same magnification (Figures 5A, 5B). The depth of demineralization of each section was calculated by averaging those 3 measurements.
(A) Schematic Diagram of the Method Used to Measure Depth of Demineralization (B) Microphotograph Taken and Depth of Enamel Demineralization Measured Using ProGresstm Software
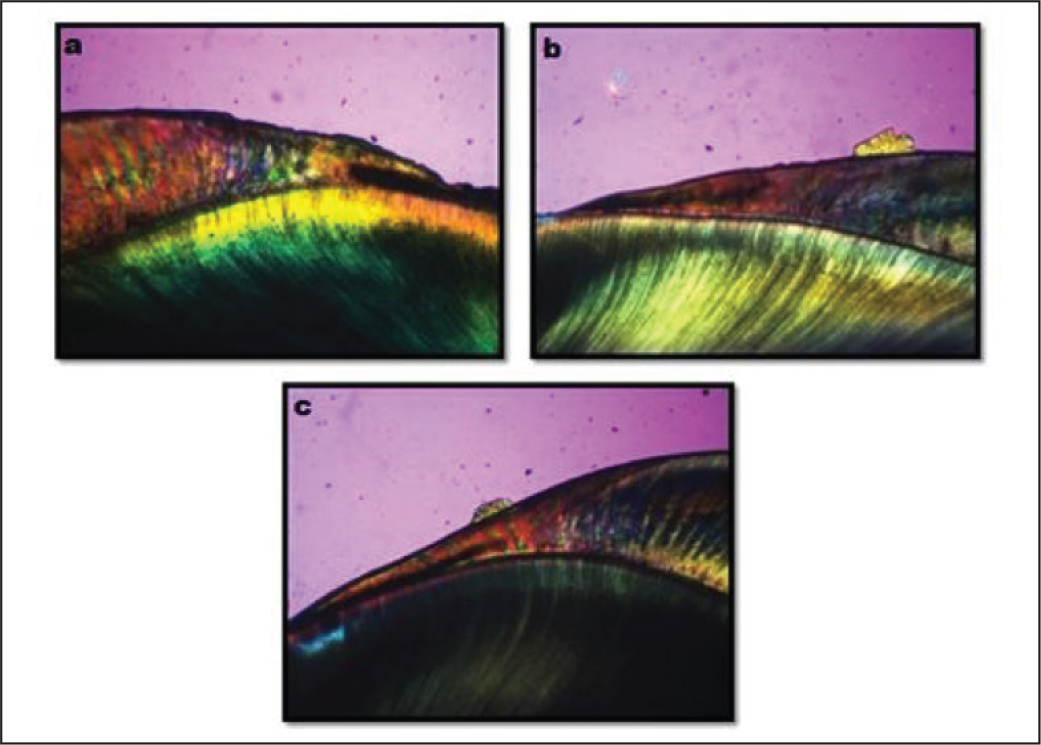
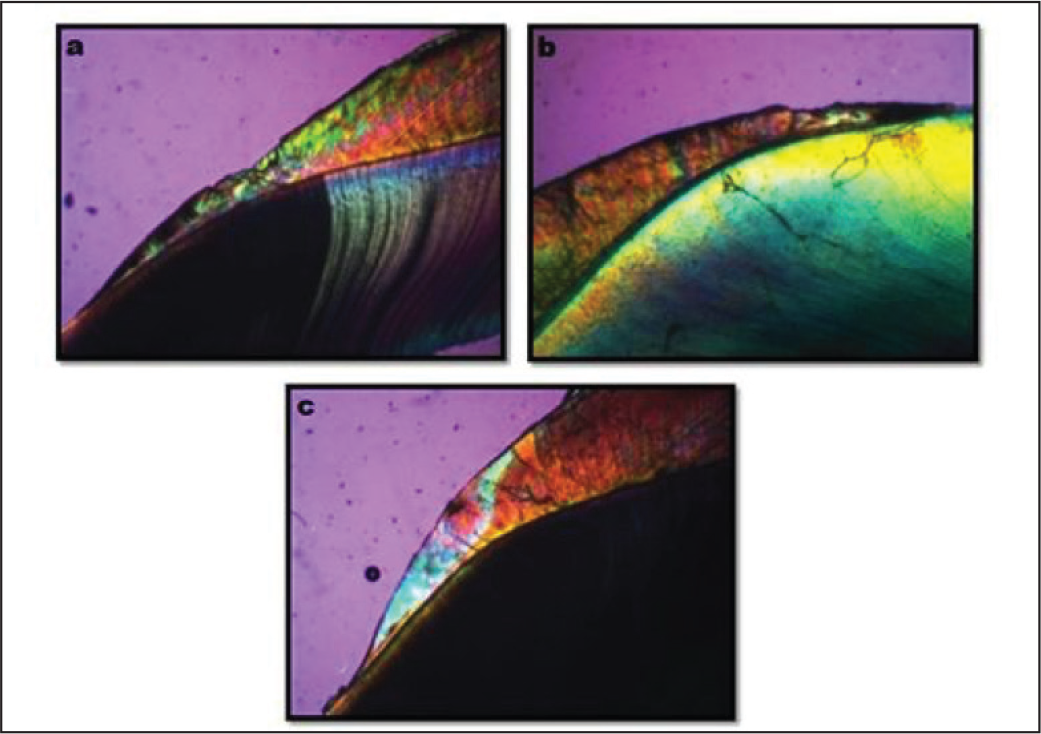
(A) Polarized Light Microscopy Microphotograph Showing a Section of Control Group After 1 Month (B) Polarized Light Microscopy Microphotograph Showing a Section of CTFV Group After 1 Month (C) Polarized Light Microscopy Microphotograph Showing a Section of LCFV Group After 1 Month
(A) Polarized Light Microscopy Microphotograph Showing a Section of Control Group After 2 Month (B) Polarized Light Microscopy Microphotograph Showing a Section of CTFV Group After 2 Month (C) Polarized Light Microscopy Microphotograph Showing a Section of LCFV Group After 2 Month
Sample Size Estimation
Based on changes from 1 month to 2 months, the depth of demineralization scores as follows:
Standard deviation in the Fluoritop SR group S1 = 5.49 Standard deviation in the Clinpro XT group S2 = 4.82 Mean difference between Fluoritop SR and Clinpro XT = 8.43 Effect size = 1.1668 Alpha error (%) = 5 Power (%) = 95 Sided = 2 Number needed (n) = 10 in each group
Where
Z1-α/2 = Z-value for α level = 1.96
Z1-β = Z-value for β level = 1.982
S = Average of S1 and S2
Statistical Analysis
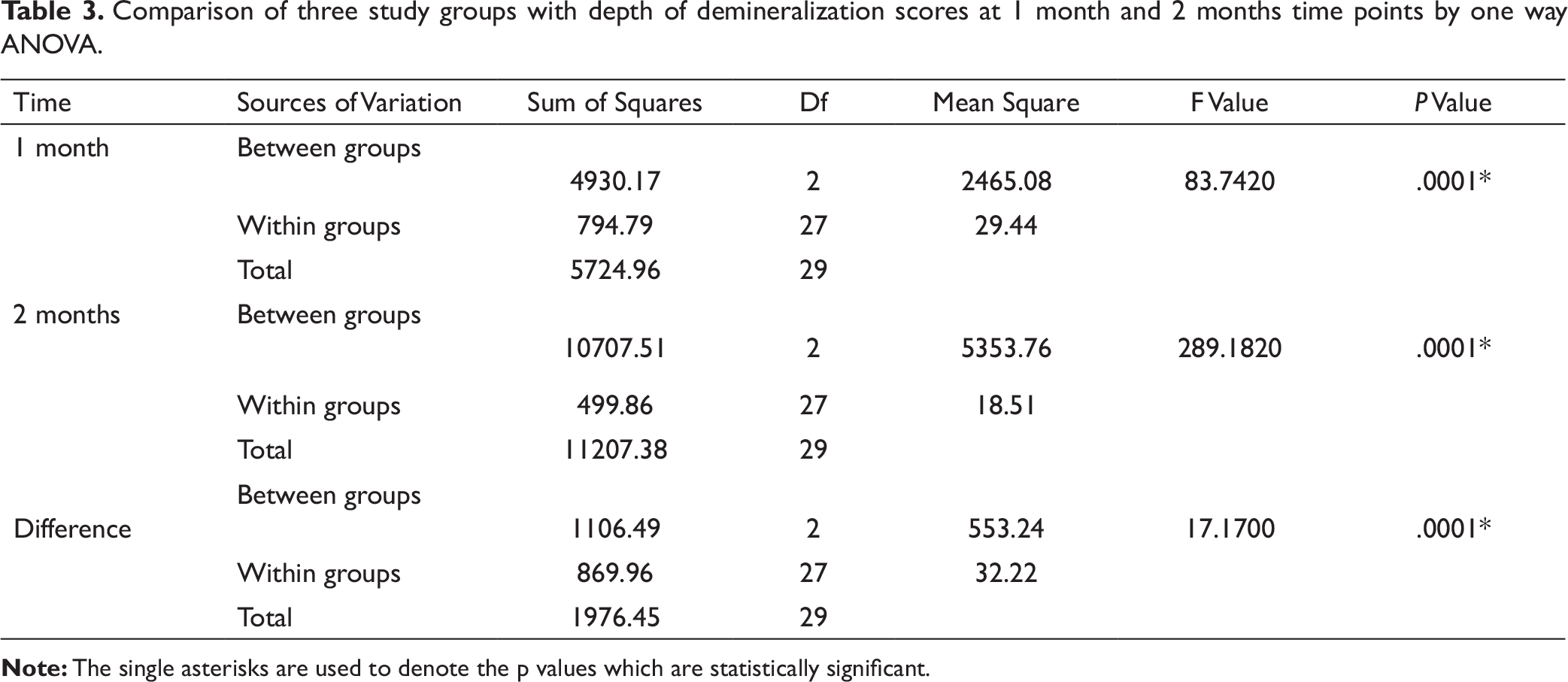
The statistical analysis was done using SPSS (Statistical Package for Social Sciences) version 20.0 (IBM, Armonk, NY). Normality of depth of demineralization in 3 study groups at 1 month and 2 months’ time points was done by Kolmogorov Smirnov test. The mean score for each group and their standard deviation were calculated. Comparison of these 3 study groups with depth of demineralization scores at 1 month and 2 months’ time points was conducted by one-way analysis of variance (ANOVA). Pairwise comparison of the study groups with depth of demineralization scores at 1 month and 2 months’ time points was performed by Tukey’s multiple post hoc procedures. Comparison of 1 month and 2 months with respect to the depth of demineralization scores in these study groups was done by dependent t test.
Results
Normality of depth of demineralization in three study groups at 1 month and 2 months time points by Kolmogorov Smirnov test.

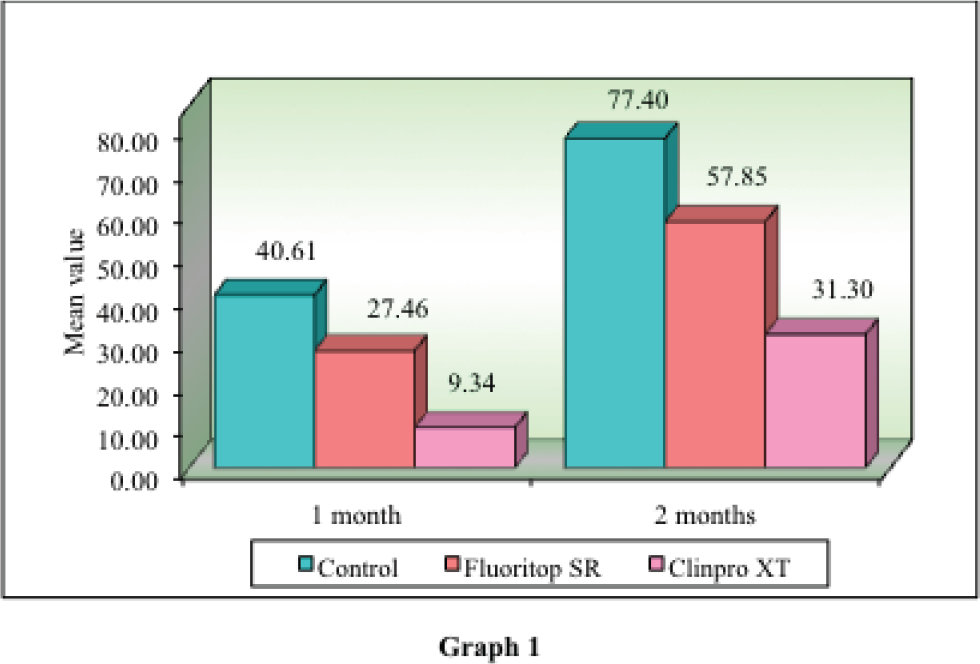
Summary of depth of demineralization in three study groups at 1 month and 2 months time points.
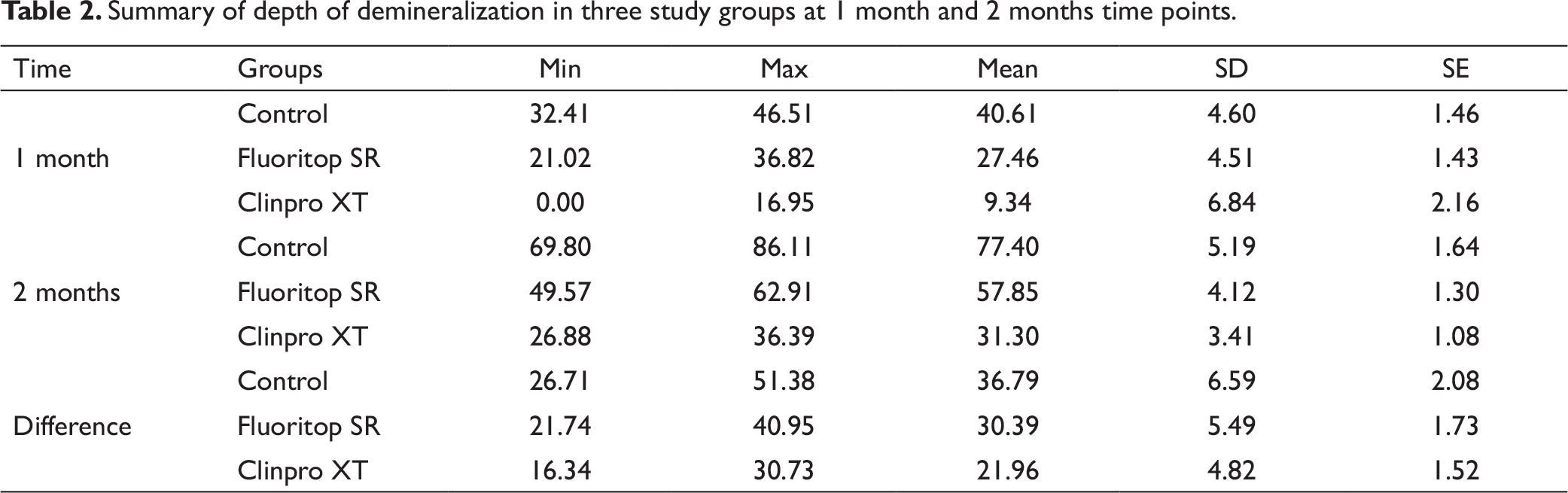
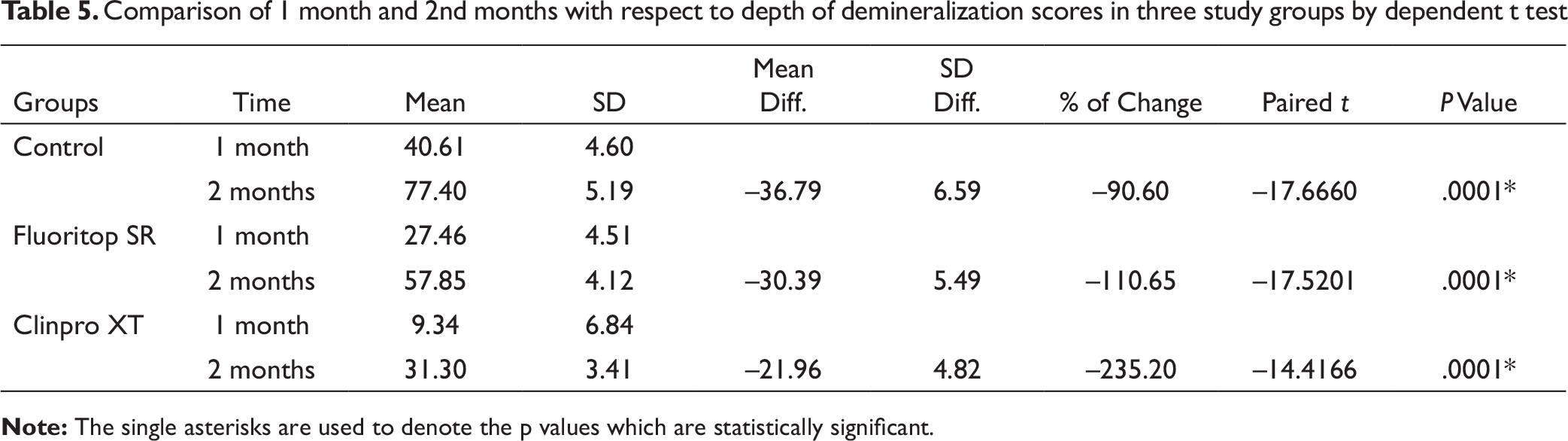
All the samples in control group, conventional topical fluoride varnish (CTFV) group, and LCFV group showed enamel demineralization after 1 month in polarized light microscope microphotograph evaluation, except 3 samples which did not show any demineralized lesion in LCFV group. The mean depth of demineralization was 40.61 ± 4.60 µm, 27.46 ± 4.51 µm, and 9.34 ± 6.84 µm in control group, CTFV group, and LCFV group, respectively, after 1 month of varnish application. All samples in the control group, CTFV group, and LCFV group showed enamel demineralization after 2 months of bonding, and the mean depth of demineralization was 77.40 ± 5.19 µm, 57.85 ± 4.12 µm, and 31.30 ± 3.41 µm in control group, CTFV group, and LCFV group, respectively, after 2 months of varnish application (Table 2).
Comparison of three study groups with depth of demineralization scores at 1 month and 2 months time points by one way ANOVA.
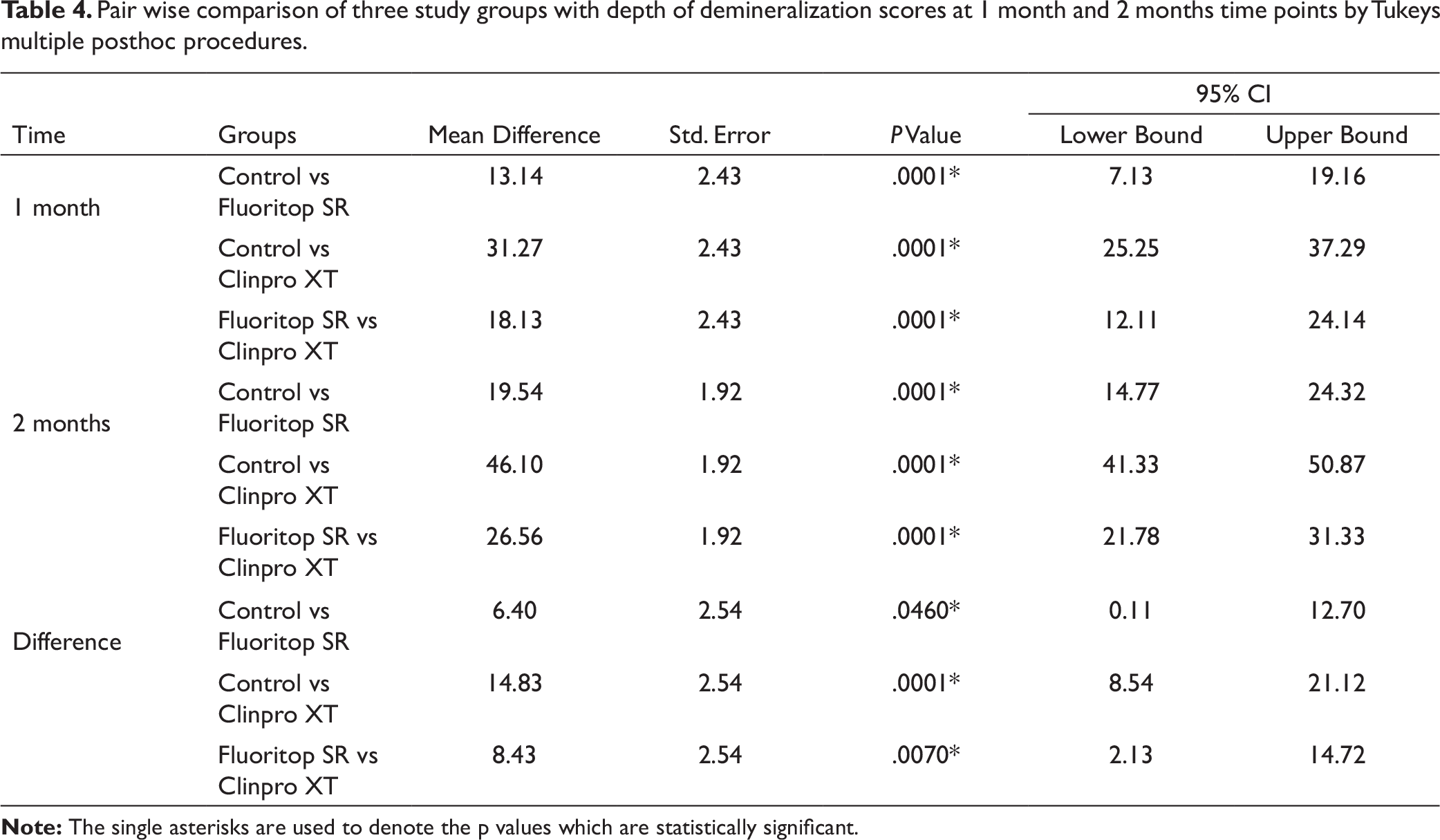
Pair wise comparison of three study groups with depth of demineralization scores at 1 month and 2 months time points by Tukeys multiple posthoc procedures.
Comparison of 1 month and 2nd months with respect to depth of demineralization scores in three study groups by dependent t test
The results of Tukey’s multiple post hoc procedures showed the mean difference in the depth of demineralization between control and CTFV group, between control and LCFV group, and between CTFV group and LCFV group after 1 month were 13.14 µm, 31.27 µm, and 18.13 µm, respectively, and they all were statistically significant (P < .05). The mean difference in the depth of demineralization between control and CTFV group, between control and LCFV group, and between CTFV group and LCFV group after 2 months were 19.54 µm, 46.10 µm, and 26.56 µm, respectively, and they all were also statistically significant (P < .05). The difference between the depths of demineralization between all the groups after 1 month and 2 months were also statistically significant (P < .05; Table 4).
Comparison of 1 month and 2 months with respect to the depth of demineralization scores in the 3 study groups was conducted by dependent t test. The results of dependent t test showed that the depth of enamel demineralization in control group, CTFV group, and LCFV group were increased from 1 month to 2 months by 90.60%, 110.65%, and 235.20%, and they all were statistically significant (P < .05; Table 5).
Discussion
Various studies used different techniques for examining enamel demineralization such as direct visual examination, 13 photographic examination,13, 32, 33 scanning electron microscopy,34, 35 stereomicroscopy, 34 polarized light microscopy,22, 23-25, 36-39 cross-sectional microhardness,40, 41 DIAGNOdent measurements,26, 29 and stylus profilometer 42 to determine enamel demineralization. Among all the techniques, PLM is the most sensitive and reliable method for examining early lesions of enamel demineralization; hence, we chose PLM for our study.
Enamel demineralization was visible as the loss of continuity of the surface enamel in PLM microphotograph evaluation. It has been shown in previous studies that demineralization starts to appear around orthodontic brackets after 1 month of bonding. 6 Our study also found demineralized area on enamel surface after 1 month of bonding. The mean depth of demineralization measured in CTFV group after 1 month of varnish application was 33% less than the control group. 7 out of 10 samples showed enamel demineralization after 1 month of varnish application in LCFV group in PLM microphotograph evaluation. We even found a layer of LCFV on 1 sample in the microphotograph. Mean depth of demineralization after 1 month of varnish application in LCFV group was approximately 77% less than the control group and 66% less than CTFV group.
The mean depth of demineralization in CTFV group after 2 months of varnish application was approximately 25% less than the control group. The mean depth of demineralization in LCFV group after 2 months of varnish application was approximately 60% less than the control group and 46% less than CTFV group.
The results of Tukey’s multiple post hoc procedure indicate that both Fluoritop SR and Clinpro XT showed significantly less depth of demineralization after 1 month and 2 months compared to the control group, and when the depth of demineralization was compared between Fluoritop SR and Clinpro XT group, Clinpro XT showed significantly less demineralization than Fluoritop SR.
The results of dependent t test indicate that LCFV group showed the highest increment in the depth of demineralization between 1 month and 2 months than the control and CTFV groups. This indicates that LCFV tends to lose its preventive action against enamel demineralization more rapidly from 1 month to 2 months. This might be due to increased wearing off of the varnish from the enamel surface.
Our study indicated that LCFV is more effective than CTFV after 1 month and 2 months of varnish application. This observation supports the study done by Shah et al 39 where they compared the effect of Clinpro XT (LCFV) and Duraphat (CTFV) after 45 days, 90 days, and 120 days of bonding around orthodontic brackets. They found that Clinpro XT is more effective in preventing enamel demineralization than Duraphat varnish which is similar to our study.
Mehta et al 28 observed that single application of LCFV (Clinpro XT) effectively reduced enamel demineralization around orthodontic brackets after 15, 30, 45, 90, and 120 days using polarized light microscopy. The average depth of demineralization in control group after 30 days in their study (40.17 ± 2.89 µm) is comparable to our study (40.61 ± 4.60 µm). However, they did not find any demineralization in any of the experimental teeth except for 3 teeth throughout the study period, in our study we found enamel demineralization in 70% teeth after 30 days and 100% teeth after 60 days. The possible reason for the difference in the depth of enamel demineralization might be because they bonded only the first premolars to be extracted in the whole arch and placed T loop to facilitate plaque accumulation, whereas in our study we bonded all the teeth till first molar and carried out suitable orthodontic treatment. So, in our study plaque accumulation was more than their study as the adjacent teeth of the premolars to be extracted also bonded with orthodontic brackets and cleaning of plaque would be difficult as brackets and arch wires make the area difficult to clean. It has been previously established that orthodontic treatment causes significant increase in the population of different bacteria numerically. 43 More plaque accumulation means more microorganisms and hence more depth of demineralization.
Farhadian et al 25 conducted an in vivo split mouth study using topical fluoride varnish (Bifluoride 12) and observed that there is 40% reduction in depth of enamel demineralization in the experimental group compared to control group after 85 to 95 days of varnish application using polarized light microscopy. Our study found approximately 33% and 25% reduction in the depth of demineralization after 1 month and 2 months, respectively, in CTFV group (Fluritop SR). The reason behind the difference in the depth of demineralization in our study in comparison to their study might be because of the high concentration of fluoride present in the varnish (Bifluoride 12, 6% calcium fluoride, and 6% sodium fluoride, 56,300 ppm) in their study compared to topical fluoride varnish (Fluoritop SR, 5% Sodium fluoride, 22,600 ppm) used in our study.
In our study, only first premolars were included; therefore, demineralization of other teeth could not be examined. Sex variations and age factors for demineralization were not taken into consideration for this present study. In our study, only the linear depth of demineralization was measured, but measurement of the area of the demineralized lesions would have been more significant. So, future studies can be done incorporating the above-mentioned factors in the study design. Other commercially available fluoride varnishes also can be compared with these varnishes.
Conclusions
The following conclusions could be made from this study:
Significant enamel demineralization occurred adjacent to orthodontic brackets after 1 month and 2 months of bonding of orthodontic brackets. Single application of both LCFV and CTFV was effective in reducing significant depth of demineralization after 1 month and 2 months of varnish application compared to control; however, none of them could completely eliminate enamel demineralization. LCFV showed significantly less enamel demineralization compared to CTFV after 1 month and 2 months of varnish application around orthodontic brackets.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.