
Abstract
Abstract
Tooth transposition is an unusual form of positional interchange of two adjacent teeth. The maxillary canine is the most frequently involved tooth. This is a case report of a complete left maxillary canine transposition with lateral incisor and impacted right maxillary 2nd premolar. Careful planning of the orthodontic transposition correction was done, and teeth were followed meticulously to their normal positions.
Introduction
Tooth transposition is an unusual form of positional interchange of two adjacent teeth. The maxillary canine is the most frequently involved tooth. 1 The etiology of transposition is unclear; however, various theories have been proposed, such as a genetic interchange in the position of developing tooth buds, failure of canine root resorption, mechanical interferences obstructing normal path of eruption of permanent tooth, premature loss of primary teeth and retained deciduous teeth. Chattopadhyay et. al found that tooth transposition was prevalent in 0.4% of the Indian population, 2 with more common unilateral transpositions compared to bilateral transpositions and the left side being more frequently involved than the right side. Peck and Peck found that most common type is between the canine and maxillary first premolar (Mx.C.P1), while the second most common type is the transposition of maxillary lateral with canine (Mx.C.I2). 3 However, there have been very few case reports documenting the orthodontic positional correction of Mx.C.I2.4–7 Such literature on treated cases of tooth transposition would provide orthodontists with the best understanding of the treatment options.
This is a case report of a complete left maxillary canine transposition with lateral incisor. Careful planning of the orthodontic transposition correction was done, and teeth were followed meticulously to their normal positions.
Case Report
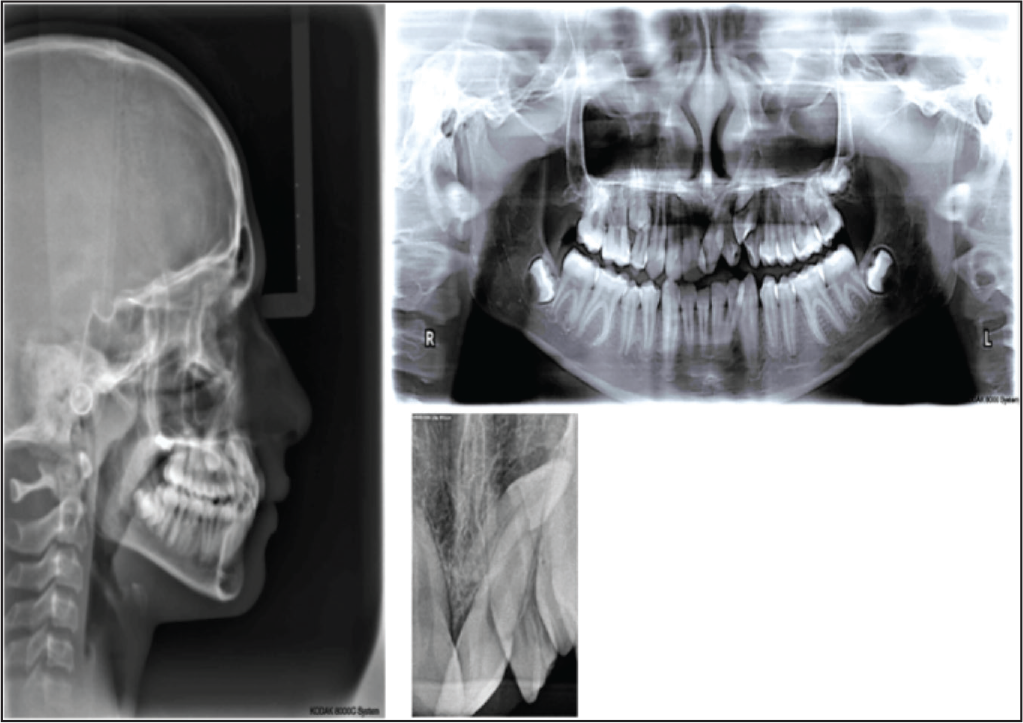
A 12-year-old male was referred to the Department of Orthodontics to rule out the cause and management of transposition of left upper canine to lateral incisor by a general dentist. On extra oral examination, a straight profile, competent lips, and deep mentolabial sulcus was observed. On intraoral examination, the patient was observed to be in the late mixed dentition stage with erupting 23 distal to 21. He had 2 mm of overbite and overjet, mesially tipped 21 with gingival recession. Radiographic examination showed that 15 was impacted beneath 14. All developing permanent teeth up to the second molars were present (Figure 1).
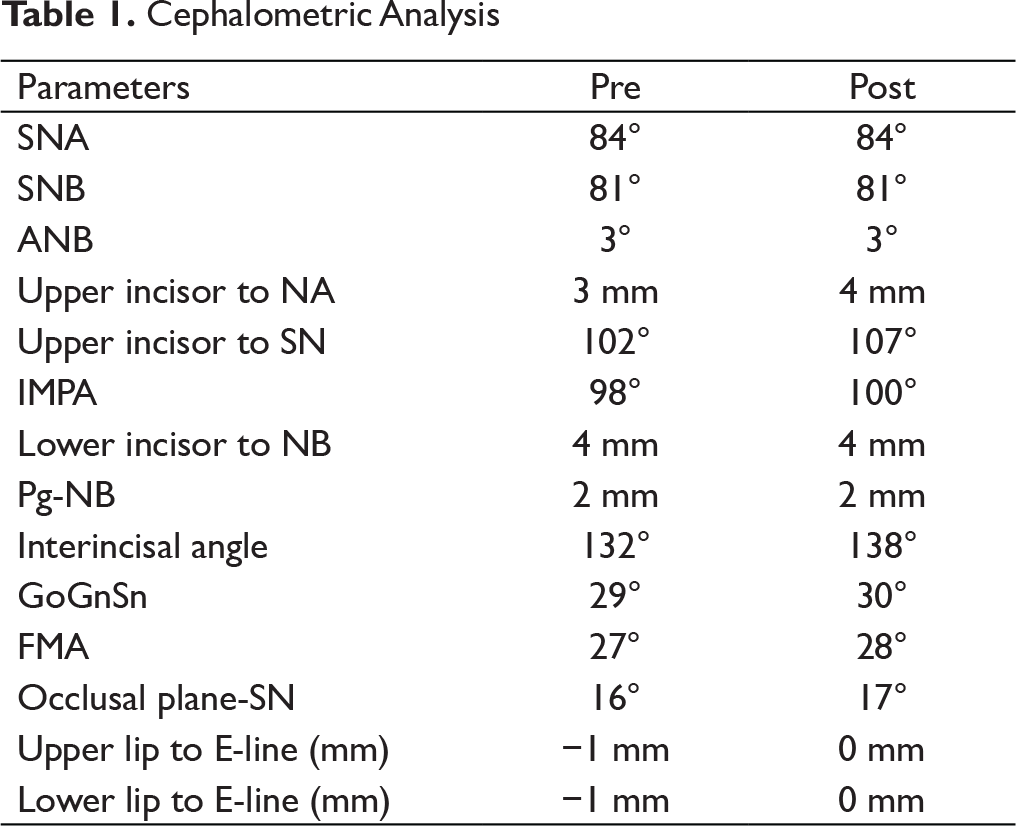
A panoramic radiograph forwarded by the dentist revealed that the 23 was impacted and positioned between the 21 and 22, while 15 was impacted apical to the hypoplastic 14 (Figure 2). A possible etiology for this condition in this patient could be multiple supernumerary teeth in the maxillary left lateral incisor region that had been extracted previously by the general dentist 2 months ago. Cephalometric analysis indicated mild skeletal Class II relation with an average mandibular plane angle (Figure 2).
12-Year-old Male Patient with Mild Skeletal Class II Relationship Before Treatment

Pretreatment Radiographs
Treatment options include:
1. Alignment of teeth in their transposed positions, followed by selective reshaping and/or composite buildups of the transposed teeth. 2. Orthodontic correction of the transposition.
In this case, orthodontic correction of the transposition was done as it was the treatment option preferred by the patient, and the canine inclination was favorable, which would facilitate midline correction.
Treatment Objectives
The treatment objectives were:
Alignment and levelling; Correction of the transposition; Achievement of functional Class I molar and canine relationship; Achievement of ideal overbite and overjet; and Maintain the pleasing facial esthetics.
Orthodontic treatment was initiated by banding the first permanent molars and bonding all the other teeth until the premolars.
Treatment consisted of two stages: Simultaneous molar distalization, intrusive and distal movement of the canine, followed by mesiolabial movement of the maxillary left lateral incisor (Figure 3 and 4).
Treatment Progress at 8th and 15th Month, Respectively

Treatment Progress with Pendulums Appliance

MBT* brackets in the maxillary arch followed by placement of a Pendulum appliance for bilateral molar distalization with 90° preactivation of the titanium molybdenum alloy (TMA) spring, followed by 45° every month. The maxillary arch was aligned using light forces with a 012′′ thermal NiTi archwire for 6 months followed by 0.016 0.022′′ Niti. Since the archwire was not engaged to the lateral incisor, the tooth was free to physiologically move out of the canine root’s path. A button was bonded on palatal surface of 22, and an attachment was given to the helix of the Pendulum appliance with elastomeric chain to initiate palatal movement. A Begg bracket was bonded on distal surface of 23. A cantilever spring was constructed using 0.017 × 0.025′′ TMA wire with two 3-mm-diameter helices attached to molar tube in order to intrude and distalize the canine for a period of 8 months. The force exerted by the cantilever spring for canine intrusion was 20 g as measured with a dontrix gauge. The lateral incisor was then aligned with. 012′′ and. 016′′ thermal nickel titanium archwires.
After 8 months of distalization, 7-mm space was achieved bilaterally (transpalatal arch was given in the maxillary arch for retention). The maxillary right second premolar naturally erupted in this space. Distal movement of the maxillary left premolars was achieved by placing a 150-g super-elastic nickel titanium open-coil spring between the lateral and the first premolar on a 017′′ × 025′′ stainless steel archwire. The total treatment time was 28 months; maxillary and mandibular removable Hawley appliances were given post treatment for retention purposes.
Treatment Results
Cephalometric Analysis
Treatment Progress with Pendulums Appliance

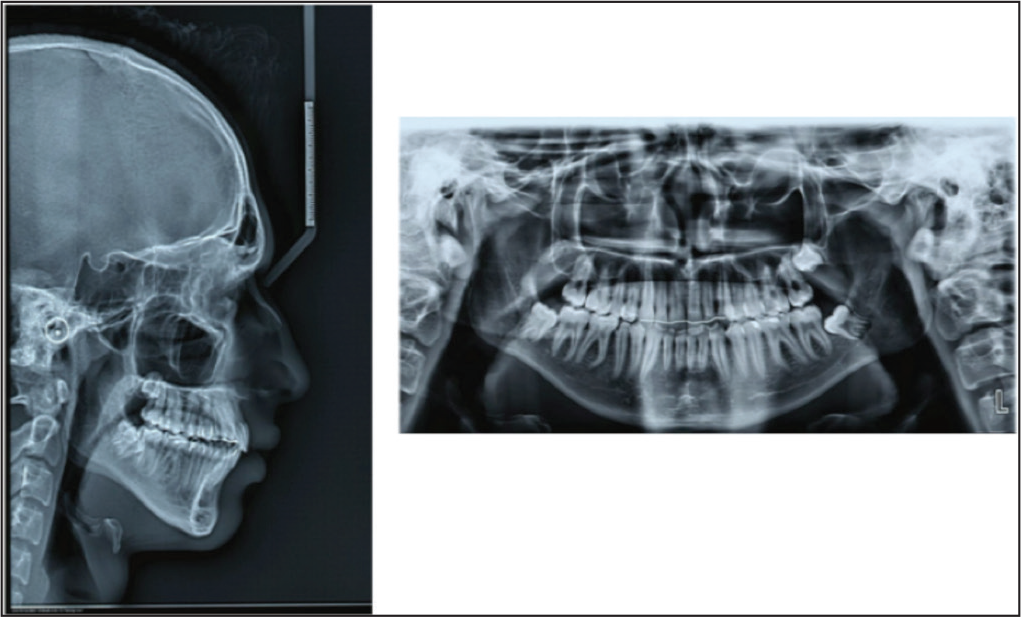
Post Treatment Radiographs at the End of 28 Months
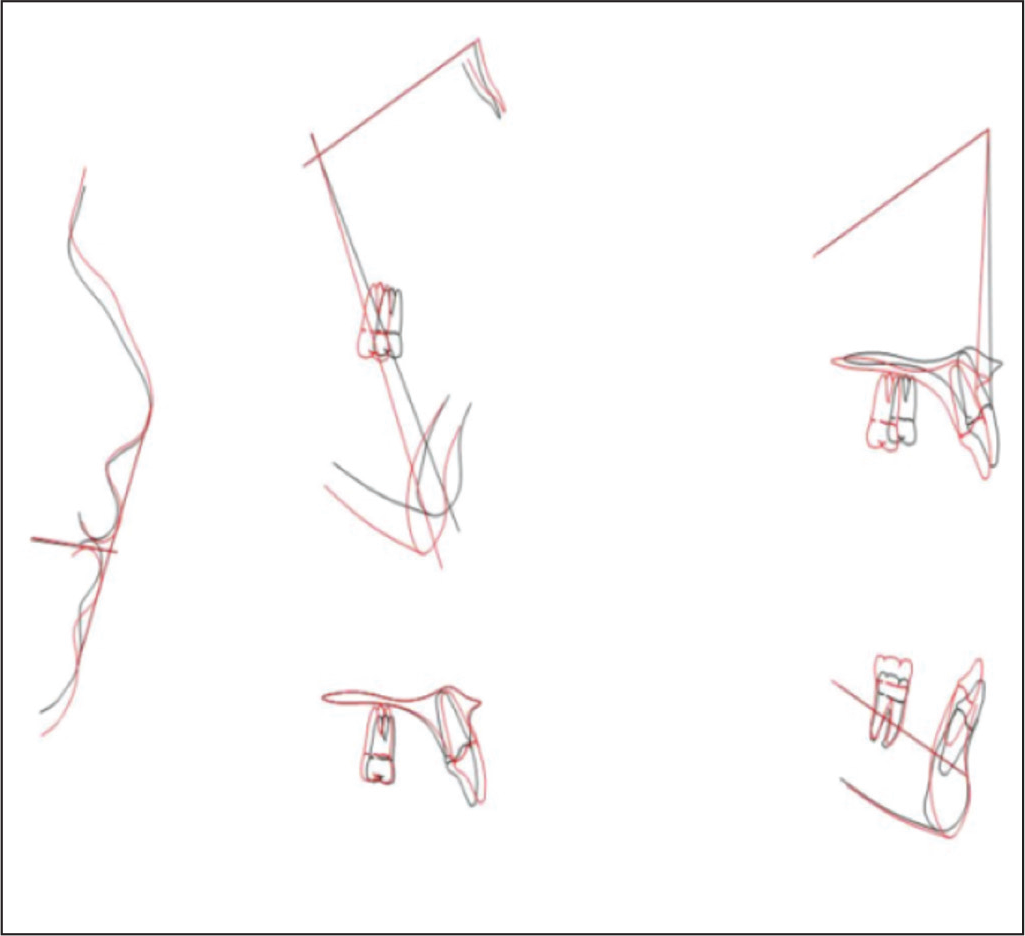
Superimposition of Pre and Posttreatment Cephalometric Tracings
A follow-up after 4 years showed a stable result despite the patient confirming that the upper retainer was never used. There was also no history of secondary caries in relation to the lower right first and second molars, which was treated at the end of orthodontic treatment (Figure 8).
Post Retention 4 year Follow Up

Discussion
Various parameters need to be considered while planning for correction of a transposed tooth, which includes tooth morphology, position of the root apices, periodontal support, width of alveolar bone, facial aesthetics, treatment time, patient cooperation, and appliance design. In this case report, the lateral incisor–canine transposition was detected in developing stage, and timely intervention was carried out to finish the case successfully in Class I functional occlusion. However, if the canine had already erupted between the central and lateral incisors, the treatment would have to be limited to aligning the teeth in their transposed position. Low orthodontic forces facilitated bodily movement and translation of canine to bypass the lateral incisor. Since the alveolar bone width of this patient was adequate and since the left maxillary canine had not fully erupted, moving the canine into its ideal position was possible with fully controlled optimal orthodontic forces. No sign of root resorption or any other damage to the canine or lateral incisor was seen. Left lateral incisor showed clinically acceptable periodontal support with some gingival recession palatally during active treatment phase, which subsided after the finishing stages.
The maxillary canines are cornerstones of the dental arch, for both aesthetics and normal masticatory function. Treatment time required for correction of the transposed tooth must be considered from a cost–benefit point of view. The patient was very well informed about the comparatively longer treatment time.
Biomechanically, cantilevers are able to produce statically determinant force systems, giving the clinician opportunity to deliver qualitatively and quantitatively precise forces.8, 9 A cantilever spring fabricated using titanium–molybdenum alloy was utilized with fixed end inserted into a molar tube and the free end engaged in the Begg’s bracket. Since the molar was being distalized by Pendulum appliance, it provided sufficient anchorage. Appropriate preactivation and subsequent intraoral activation of the TMA springs achieved 7-mm space. 10 The subsequent eruption of impacted second premolar into the space created by using Pendulum appliance is being reported for the first time in literature.
Controlling the tooth movement within the alveolar bone was crucial and different strategies were used during the treatment. The first step was to intrude the canine and move the root of the lateral incisor palatally. The second step was to let the canine bypass the lateral incisor, following which the canine and lateral incisor alignment was initiated to obtain normal inclination. The total treatment time for this case was 28 months, at the end of which satisfactory results were obtained. Cephalometric superimposition (Figure 7) showed significant mandibular growth (both vertically and horizontally) accounting for normal growth. Even after proclination of maxillary incisors, the patient exhibited straight profile, normal size and shape of the nose, and average nasolabial angle.
Conclusion
With careful monitoring of the tooth movement, it is feasible to orthodontically correct tooth transpositions. Impacted premolar can be brought into occlusion by creating space using Pendulum appliance.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.