
Abstract
Abstract
Purpose: Understanding the effects of different corticotomy designs on the velocity of maxillary canine retraction.
Materials and Method: The 3-dimensional model of maxillary dentition was constructed and 3 corticotomy designs were compared with the conventional approach of canine retraction. 4 models were constructed for the present study: 1 with no corticotomy cuts (model 1), 1 with vertical cuts on both buccal and palatal side (model 2), other with cuts only on buccal side (model 3), and 1 with circular holes (model 4). Stress intensity and force distribution were evaluated after applying 150 gm of orthodontic forces on maxillary canine.
Results: Models with corticotomy approaches exhibited approximately twice the displacement when compared with conventional noncorticotomy procedure. The stresses were mainly concentrated on the distal side of the canine in all the models. The rate of canine retraction was the highest in model with buccal and palatal corticotomy compared to other designs.
Conclusions: Corticotomies help orthodontists to alter the biomechanical responses of dentoalveolar structures during maxillary canine retraction and accelerate tooth movement. Clinically, buccal corticotomy is a better choice for the patients as it is less traumatic and more acceptable to patients.
Introduction
Conventional fixed orthodontic tooth movement requires 1 to 2 years; more time is required for extraction cases which is a great concern for patients.1 Thus, to reduce the overall treatment time, many biochemical methods have been introduced to speed up the orthodontic treatment. Currently, corticotomies are the most popular method for acceleration of orthodontic treatment by means of regional acceleratory phenomena, leading to an increase in the rate of bone turnover after being exposed to an insult, thus doubling the velocity of tooth movement as shown in many studies.2
Corticotomy has roots in orthopedics going back to the early 1900s. In 1959, Kole expanded on this philosophy by addressing additional movements, including space closure and cross-bite correction.3 Suya after 32 years modified Kole’s procedure, and his procedure is being widely used till date by some clinicians.4 Although this technique proved to be effective in shortening the treatment time, it fell in disuse because of the high degree of invasiveness, patient discomfort, and postoperative complications. To decrease patient discomfort and diminish surgical intervention, corticotomy with vertical cuts and circular holes only on buccal cortical plate is given priority over the both-sided approach in many studies nowadays.5
These researches have been applied in animal experiment or clinical case reports; however, studies that evaluated the stress distribution in periodontium to help the clinicians to select the most efficient method for clinical adoption are lacking. Therefore, the aim of the present study was to evaluate the effects of different corticotomy designs on the rate of maxillary canine retraction.
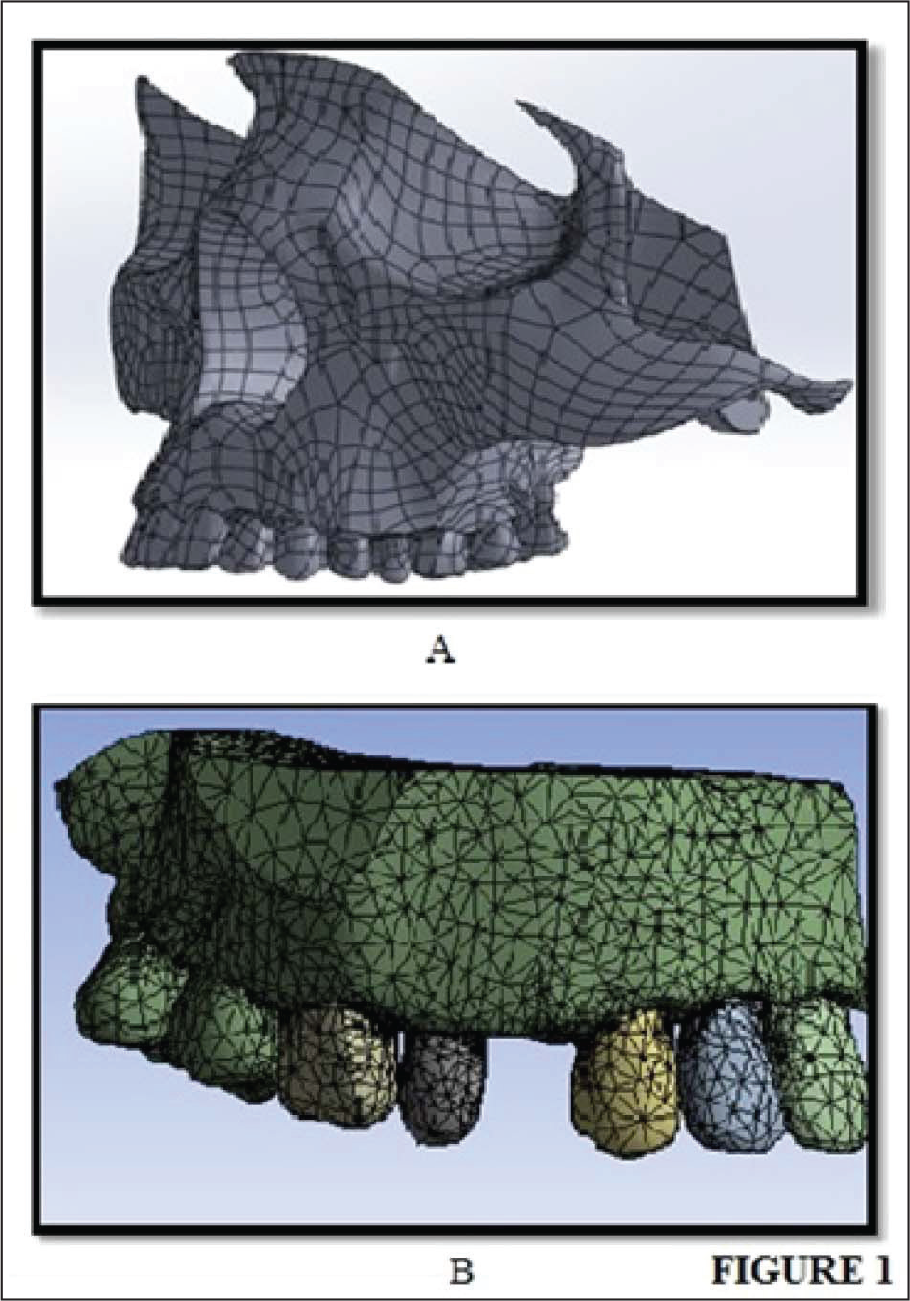
3D FEM (finite element method) Model (A) 3D Laser Scanned Model of Skull (B) Finite Element Geometrical Model with Mesh and Boundary Definition
Materials and Method
3-dimensional (3D) models for the study were constructed by 3D laser scanning using an Optical 3D Scanner (Activity 101, Smart Optics Sensor technik GmbH, Bochum, Germany). The only region of interest (maxilla in this study) was selected (Figure 1).
The 3D geometric models were converted to finite element models using hypermesh version 13.0. The model of maxillary dentition with first premolar extractions was stimulated. Using ANSYS software version 16.1, preadjusted edgewise brackets (MBT 0.022 × 0.028 inch slot) were modeled for the canine and second premolar with molar tubes, along with the stainless steel arch wire of 0.016 × 0.022 inch.
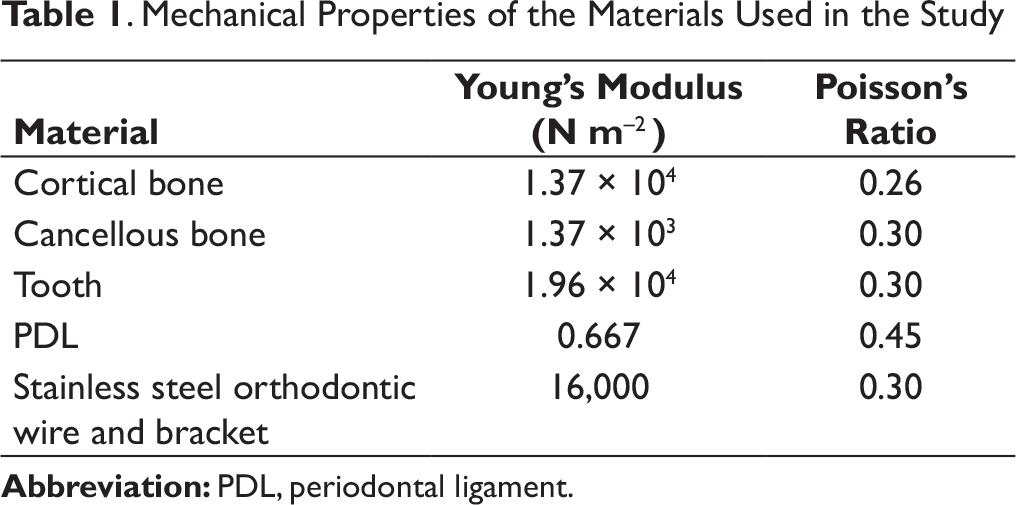
. Mechanical Properties of the Materials Used in the Study
Total Number of Nodes and Elements
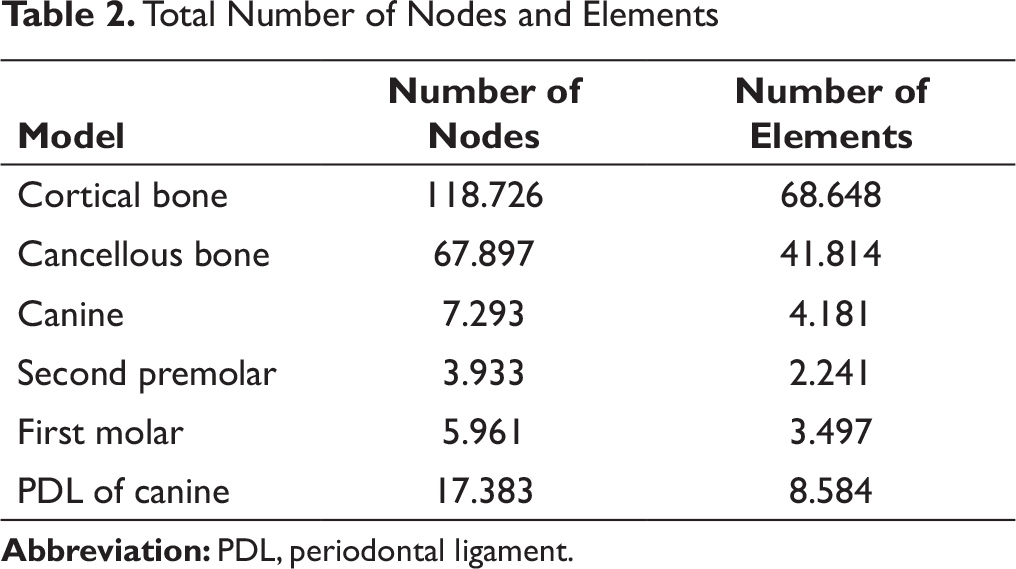
The element shape in the model was 3D tetrahedral. The interface between the teeth and the bracket was connected, to avoid interference of the composite bonding material. At the interfacial nodes between the archwire and the brackets, only sliding without friction was allowed to prevent unnecessary bracket-wire interplay. 4 models were built in this study. These models can be classified as follows:
(The osteotomy cuts were 2 mm deep and 2 mm wide.)
(Vertical cuts similar in nature as in model 2 were placed only on buccal cortical plate.)
Corticotomy was done with a series of 5 circular holes at a distance of 2 mm 90 (determined according to the length of canine root) and a diameter of 1.5 mm along the buccal cortical plate mesially and distally adjacent to canine.
All the analysis was performed using ANSYS version 16.1 (Canonsburg, Pennsylvania, USA) software after the application of 150 gm of retractive force, and the results were interpreted. After completing the model fabrication and running the fem, the distribution of stresses were studied on bone, pdl, canine and molar along x, y, and z axes.
Results
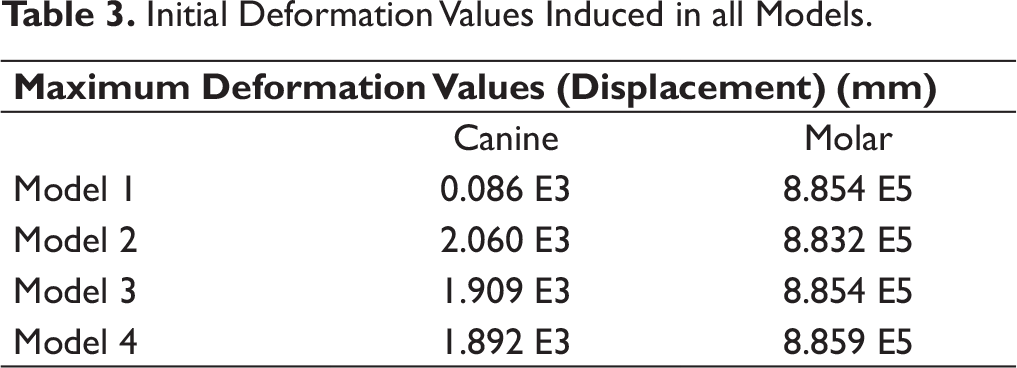
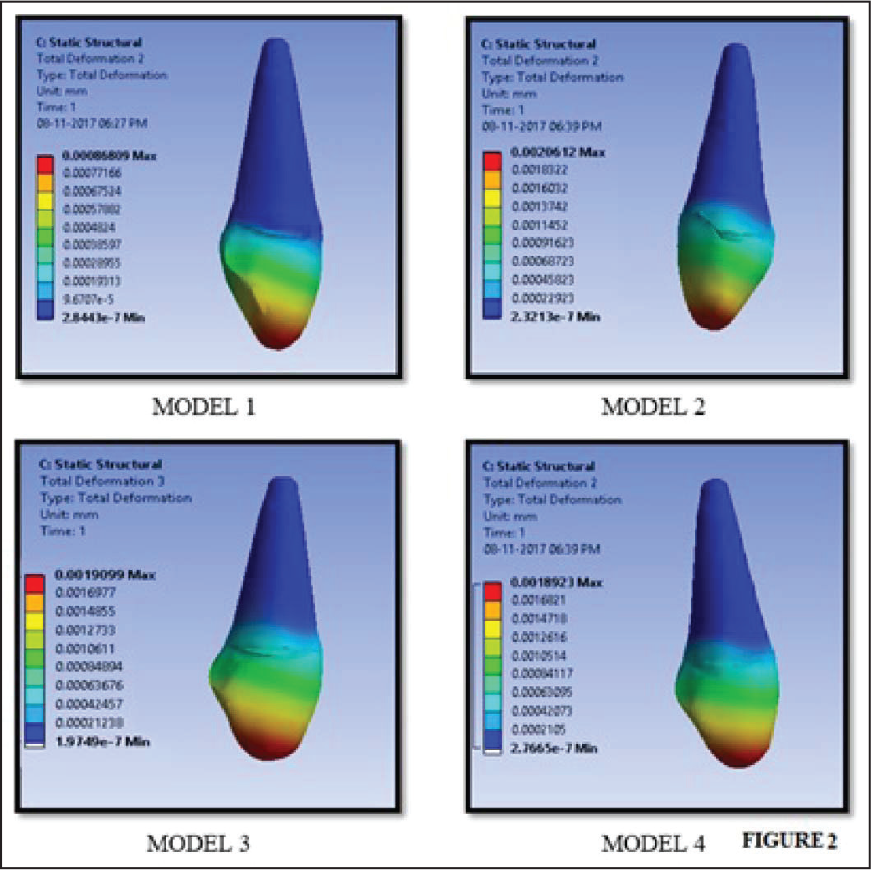
Initial Deformation Values Induced in all Models.
Initial Deformation of Canine in Different Models
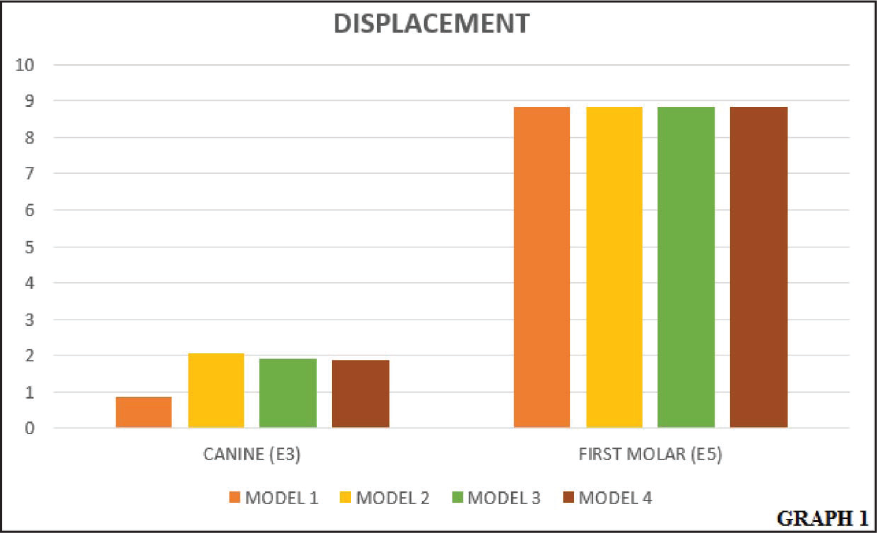
Displacement of Canine and First Molar in Different Models
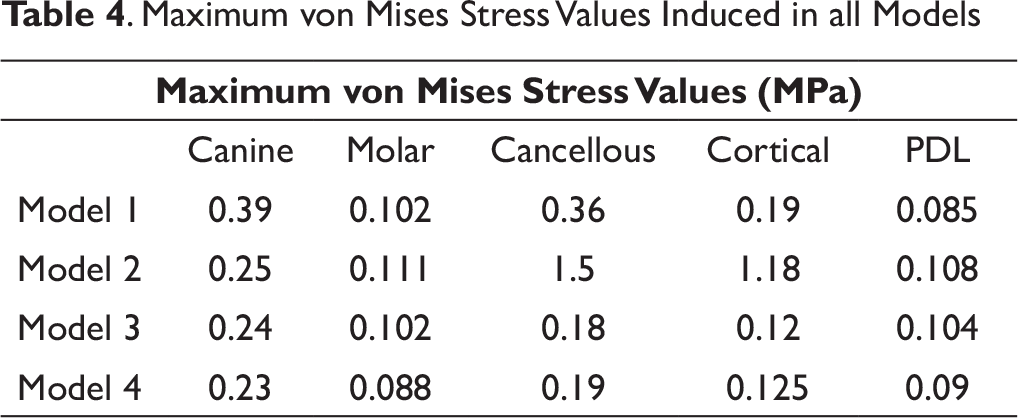
. Maximum von Mises Stress Values Induced in all Models
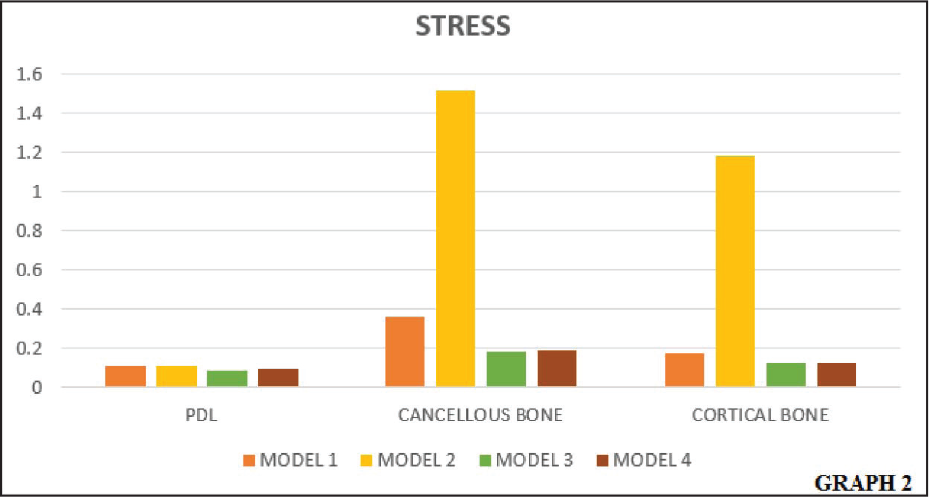
von Mises Stresses on PDL, Cancellous, and Cortical Bone in Different Models
The canine in all the models displayed clockwise rotations under the influence of retractive forces. The high stress distribution was noticed on the middle of distocervical region of the canine (corresponding to the application site of orthodontic force) and mesiocervical region of the first molar in all the models. The greatest stresses were seen in model 1, while the least stresses were noticed in model 4 (Table 4, Figure 4).
The PDL is the first structure to experience the stresses when exposed to orthodontic forces. The maximum stresses on PDL were concentrated on the cervical regions of canine and there were significant differences in the stress values with changes in corticotomy designs (Table 4, Figure 4).
In the alveolar bone, the stresses in the cancellous bone were more compared to the cortical bone and were mainly concentrated on the alveolar crest of the canine in all the models (Table 4, Figure 4).
Discussion
For successful orthodontic treatment, the goals must be set during the planning stage to finish the case within the shortest possible time without compromising the quality and stability of the results and also preserving the periodontium. Optimal tooth movement requires the application of biomechanically sound orthodontic forces and an alveolar bone that offers less resistance to movement.1
It has been shown in many previous studies that alveolar corticotomies (ACS) associated with orthodontic treatment significantly accelerate tooth movement, thereby reducing treatment duration.6,7 It was suggested that due to the surgical injury in the form of cuts and holes, the resistance offered by the cortical bone would be reduced.2
Bone remodeling is a resultant of change in stress or strain induced by the orthodontic appliance, and to understand their nature, 3D finite element method can be efficiently used. It is considered to be a valid and most widely used approach to help orthodontists understand the physiologic responses of the dentition to orthodontic forces.5
In the present study, the effects of different corticotomy designs on the periodontium were observed. Under the influence of retractive forces, the rate of canine displacement in the corticotomy models was approximately double when compared to conventional approach without corticotomy. This finding agreed with those of previous clinical reports,5 where it was seen that the rate of canine retraction with corticotomy was about twice that of the control side in the first 2 months. Lino8 evaluated the active treatment period with corticotomy in case of bimaxillary protrusion and concluded that corticotomy-facilitated orthodontic treatment shortens orthodontic treatment period without any anchorage loss or adverse effects. Similar findings were reported by Kim et al9 in an animal study, where they observed extensive direct resorption of bundle bone with less hyalinization.
The reason for faster tooth movement in corticotomy models was surgical insult to the denser layer of cortical bone that offered the most resistance to the tooth movement.10 Generally, during orthodontic tooth movement, the cortical bone offers maximum resistance to resorption and could also block tooth movement in most of the cases.11
On evaluating the stress pattern on the bone, the stresses were found to be more in the cancellous bone than in the cortical bone. Injury to the cortical bone leads to the slower response compared to rapid modeling of trabecular bone and lamina dura immediately adjacent to the injury. Hence, as an initial response to the orthodontic forces, the rapid remodeling of cancellous bone takes place followed by slower remodeling of cortical bone.12
The effect of accelerated tooth movement and safety of periodontal tissue are prime concerns during corticotomy. In our study, although the maximum amount of stresses in PDL of canine was noticed in model 2, compared to other models, but they were well below the ultimate tensile strength of PDL, so PDL was safe in all the models. Furthermore, on studying the pattern of stress distribution on first molar, it was observed that all the corticotomy models produced least stress compared to a model without corticotomy.
Compared with the conventional method of canine retraction, model 2 with buccal and palatal corticotomy revealed the greatest displacement of canine when equated with all other models. The reason for increased tooth movement in model 2 might be due to increased surgical insult. The finding of this study was in accordance with Yang2 who concluded that continuous circumscribing cut around the root of the canine exhibited the maximum rate of canine displacement. This was further supported by Mcbride et al12 and Cohen et al13 who revealed that the magnitude of the surgical insult affects bone maturity. The bone on the insult side showed greater trabecular numbers, less trabecular thickness, and less trabecular separation than did the bone on the control side, leading to greater tooth movements.14 These changes were made possible by the combination of demineralized bone matrix and immature, uncalcified bone secondary to the increased strain that allows for faster tooth movement.15,16
Displacement of canine in model 3 and model 4 with vertical cuts and circular holes only on buccal cortical plate respectively was less when compared with model 2, which is in accordance with Yang2 in 2015. These findings were further supported by an FEM study conducted by Pacheco et al17 in 2016 who evaluated stresses in the PDL of maxillary canine after retraction by different ACS procedures such as buccal vertical cuts and circular holes. According to them, the corticotomy approaches on only the buccal cortical plate could not mechanically reduce the bone resistance and were insufficient to cause differences in stress distribution.
The present study confirmed that models with different corticotomy designs affected the biomechanical responses of the periodontium. However, FEA (finite element analysis) provides a “Snap-shot” view and does not depict the changes that occur over time.18,19 The simulation in FEM study is based on mechanical laws, and this method may not be sufficient for predicting orthodontic tooth movement in clinical scenarios.
Conclusion
Within the limitations of study methodology, the following conclusions can be drawn.
The rate of canine displacement with corticotomy was twice when compared with conventional orthodontics. Corticotomy on both buccal and palatal cortical plates showed better responses in terms of canine displacement compared with other approaches. Sometimes, giving cuts on both the cortical plates can be traumatic to the patient, then corticotomy cuts only on buccal cortical plates can also be given to accelerate the orthodontic tooth movement.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.