
Abstract
Abstract
Background: The review attempts to provide synthesis of published studies evaluating the influence of an aberrant frenum attached close to the gingival margin or with inadequate width of attached gingiva on the growth of the maxilla.
Methodology: This review was reported using the PRISMA checklist as a template. PubMed, EBSCO and Google scholar were searched for in earlier publications up to January 2019. In addition, reference lists of the included studies were hand searched. The eligibility criteria were listed out based on Population, Intervention, Comparison, Outcome, Study type (PICOS) concept.
Results: A total of 148 articles were found by database search strategies and 27 additional studies by hand search. Finally three cross sectional and one longitudinal study were selected based on the eligibility criteria. A meta-analysis was not justified. Risk of bias was assessed using AXIS tool for cross sectional studies and Newcastle-Ottawa scale for longitudinal study. Common weaknesses of the studies were failure to justify or calculate the sample size and insufficient statistical reporting.
Conclusion: This review reveals that there is a need for methodologically standardized studies that will throw light on to the physiological importance of labial frenum in the growth of the nasomaxillary complex.
Keywords
Introduction
Alterations in volume, shape or position of any part of an organism as a result of growth will have a mechanical effect on adjacent structures.
1
One part of the facial pattern must not be overemphasized at the expense of another to maintain the balance. 2 Henceforth, a radical explanation of the role of muscle function and soft tissues associated with craniofacial growth is emphasized. As growth can alter the balance of these structures, a proper understanding of the magnitude and the direction of growth is essential.
The premaxilla is closely related to the development of face and its abnormal growth may lead to malformations. It serves as a stabilization element3, 4 and is influenced by that part of the cartilaginous nasal septum which is united with a fibrous connective tissue band called septopremaxillary ligament.4, 5
The maxillary labial frenum is a mucous membrane fold which develops as a posteruptive remnant of tectolabial band at around 8 to 10 weeks of intrauterine life that connects the tubercle of upper lip to the palatine papilla. With the growth of the alveolar process, the frenal attachment generally relocates to an apical position. 6 It runs along the midline of the upper lip, across the alveolar process, and inserts into the interincisal suture. 7 Studies report that an aberrant frenum can influence the growth and development of the maxillary anterior region. 8
Delaire stated that any abnormalities in the insertion of the nasolabial muscles at the lower part of the nasal septum plays a decisive role in restricting maxillary development by directly interfering with the peripheral boundary system which is a transmitter of biomechanical stimuli.1, 9 Thus, any structural variations such as a wide frenum, attached close to the gingival margin, even after the eruption of anterior teeth or limitation of the movement of the upper lip due to the frenal pull, could have a detrimental effect on the growth of its associated skeletal structures.8, 10, 11 Hence, the purpose of this review is to expand our knowledge in understanding the role of maxillary labial frenum in maxillary growth through an extensive literature review, summarizing and synthesizing the information thus obtained.
Materials and Methods
This systematic review was reported using the Preferred Reporting Items for Systematic Reviews and Meta-analyses checklist as a template. 12
Protocol and Registration
No review protocol or systematic review registration was considered.
Information Sources
With the assistance of a health science librarian, a systematic electronic search was conducted in databases such as PubMed, EBSCO, and Google Scholar. In addition, a limited gray literature search was also conducted. The references of the selected articles were hand-searched for additional relevant studies that might have been missed out. Only published articles in English/translated to English were selected. The dried skull measurements were excluded, as the review was intended to assess the fragile nonosseous anatomic structures such as nasal septal cartilage and labial frenum which are unpreserved in dry skulls.
Searches
A complex Medline search via PubMed was performed to identify any relevant study, based upon various combinations of key words and specific medical subject headings in all fields (Table 1). The additional searches were modified appropriately. All papers assessed through full-text reading, all identified papers and reviews were subjected to hand-search of their references for relevant papers that might have been missed during the electronic search.
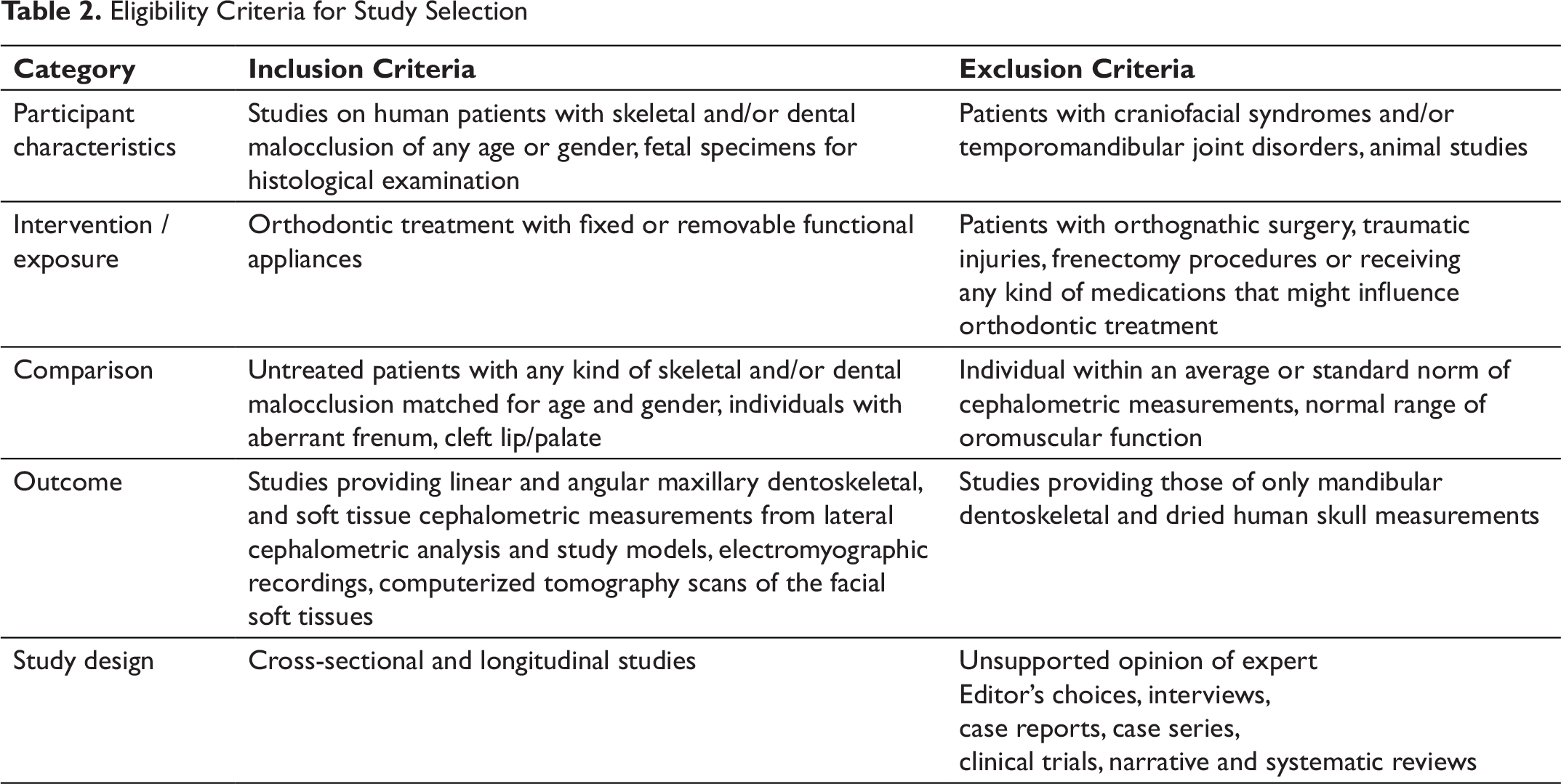
Eligibility Criteria and Study Selection
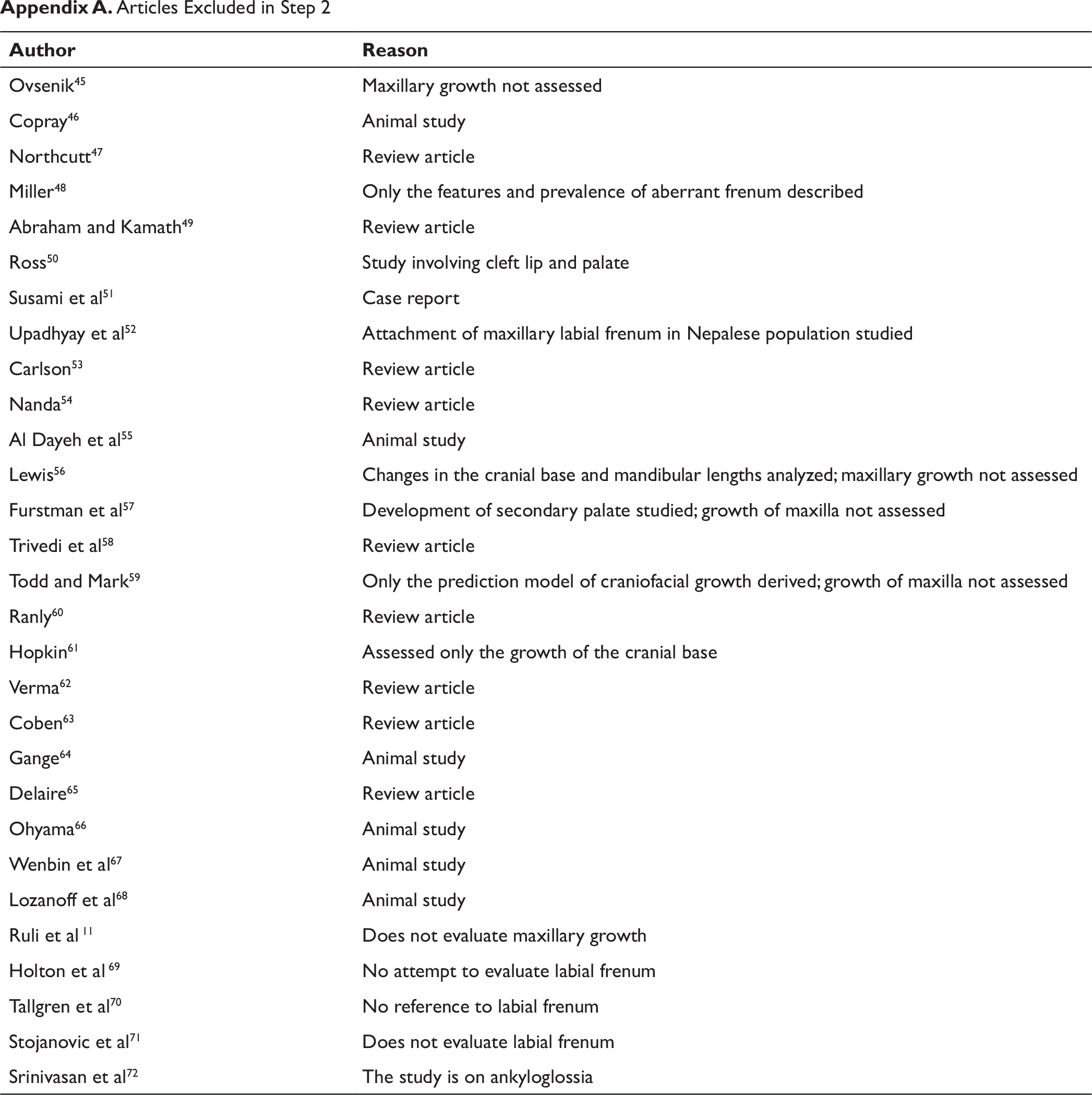
The inclusion and exclusion criteria were listed out based on PICOS (Population, Intervention, Comparison, Outcome, Study type) concept (Table 2). A positive exclusion method was used, whereby only those publications that did not meet one or more of the inclusion criteria were excluded. The selection of articles at each stage is presented in Figure 1. In step 1, only the titles and abstracts collected from the earliest records till January 2019 were considered. In step 2, copies of full articles were reviewed from those selected in step 1; the ones that fell under the exclusion criteria were excluded (Appendix A). In both steps of the review process, 2 reviewers independently reviewed the titles and abstracts and disagreements were resolved through discussion until consensus was achieved. 4 articles which satisfied the selection criteria were included in the present study.
Data Extraction
Data were extracted from selected articles by 2 reviewers independently with respect to study design, population characteristics, methods used to analyze the data, results of the study, and reliability and validity of the reported method.
Risk of Bias Assessment
Search Strategy for EBSCO (1935 up to January 2019)
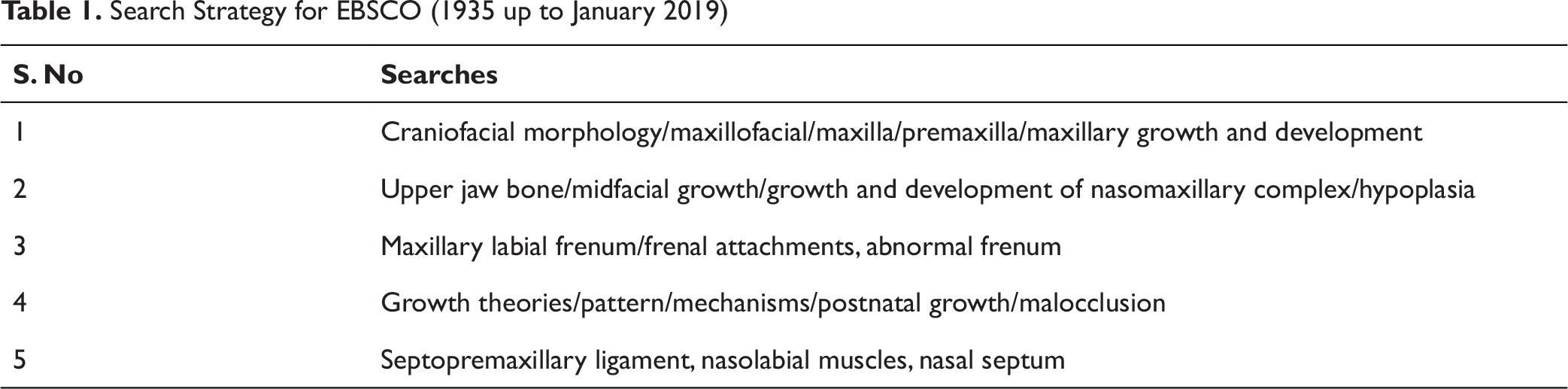
Search Strategy for EBSCO (1935 up to January 2019)
Eligibility Criteria for Study Selection
Flow Diagram of the Study Selection Process (Adapted from Preferred Reporting Items for Systematic Reviews and Meta-analyses 2009 Flow Diagram)
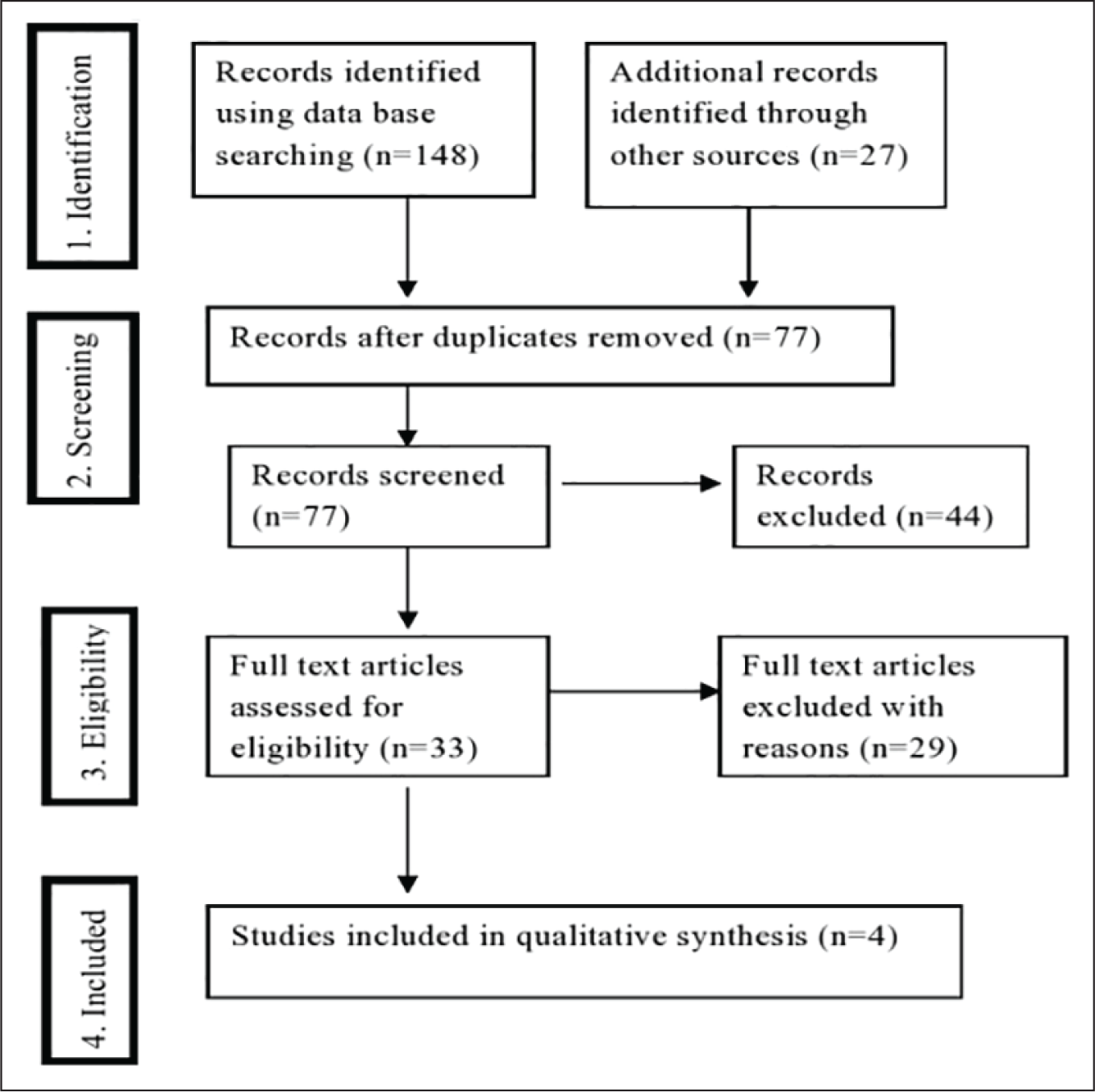
Table 3A. Critical Appraisal Tool for Cross-Sectional Studies (AXIS)
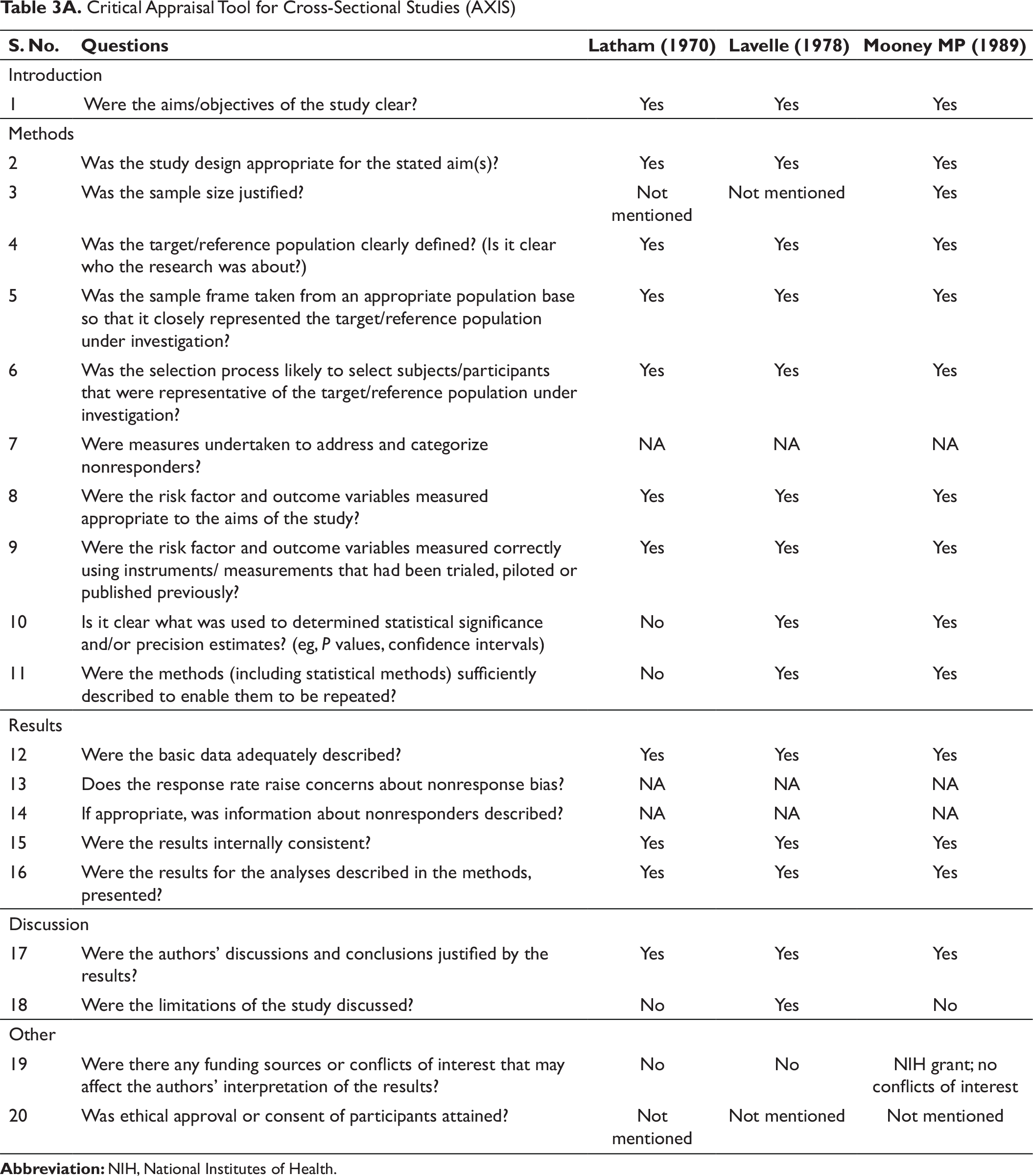
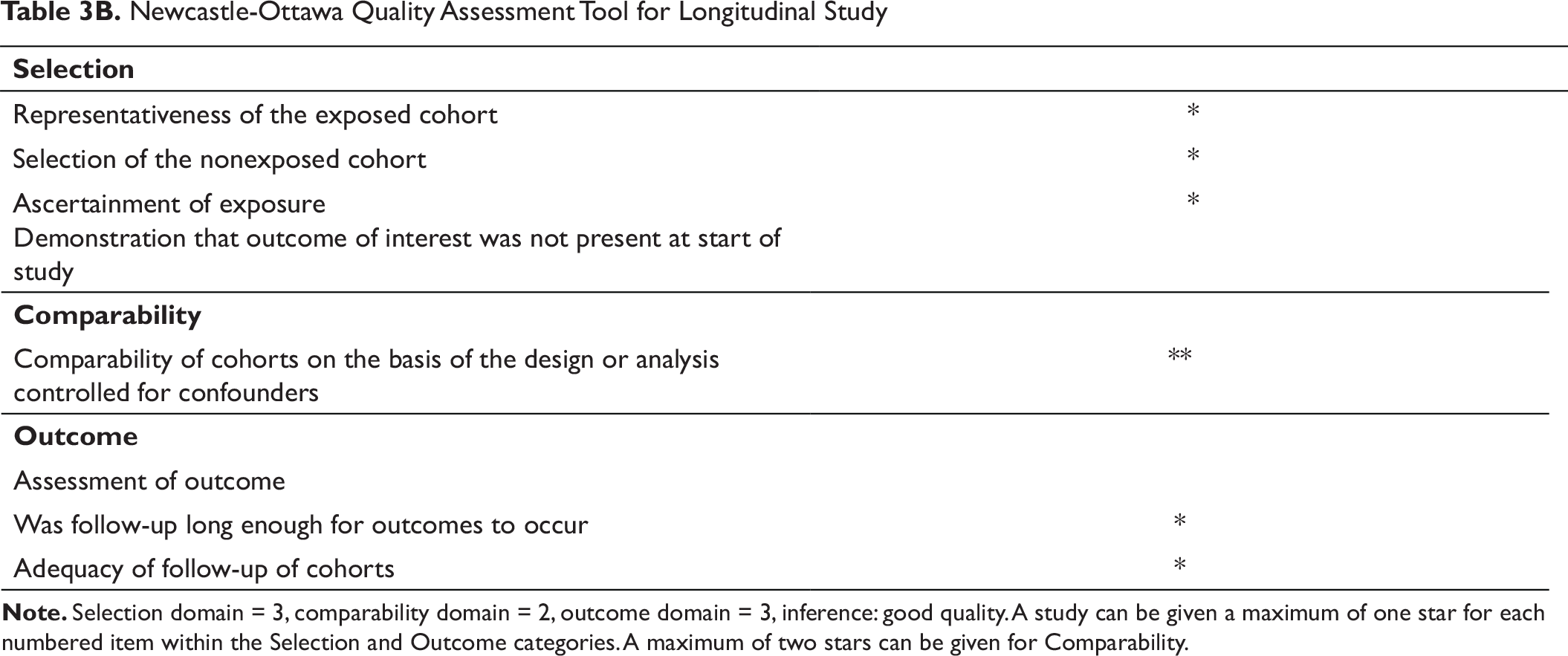
Table 3B. Newcastle-Ottawa Quality Assessment Tool for Longitudinal Study
Results
Literature Flow
The initial electronic search yielded 148 studies and 27 additional studies by hand-search. After reading titles, abstracts, and application of inclusion and exclusion criteria, 77 studies were examined in their full-text forms. From these, 4 studies were deemed eligible for inclusion in the review for qualitative synthesis.
Publication Bias
Statistical analysis of publication bias was not indicated since no quantitative synthesis was undertaken.
Study Characteristics and Critical Appraisal of Included Studies
The summary of the data extracted from the selected articles is shown in Table 4.15-18 There were one longitudinal and three cross-sectional studies. The reliability of measurements was reported only in the study conducted by Mooney et al and is supported by National Institutes of Health grant. 18 The AXIS is a unique tool consisting of 20 components to critically appraise the quality of 3 cross-sectional studies included in this review (Table 3A). The credibility and reliability of the results of the included studies are related to the aims, methods, and analyses of the results. The NOS had been used to assess the quality of the longitudinal study (Table 3B). There are 3 domains in this tool. A study can be given a maximum of 1 star for each numbered item within the selection and outcome categories. A maximum of 2 stars can be given for the comparability domain. The score of the NOS was then interpreted as good, fair, and poor quality. Accordingly, the study conducted by Lavergene and Petrovic is considered as good quality and is supported by the AIP grant awarded by the Institut national de la santé et de la recherche médicale (INSERM) is the French National Institute of Health and Medical Research. 17
The kappa score of 0.81 revealed that there was substantial agreement between the reviewers. Justification of sample size was reported in only 1 study (Mooney et al), 18 and the determination of statistical significance and precision estimates was poor in the study by Latham. 15 Limitations of the study were discussed only by Lavelle. 16 In any of the included studies, either attainment of ethical approval or consent of the participants was not mentioned.
Qualitative Synthesis of Included Studies
A meta-analysis was not feasible because there were no selected studies of similar comparisons, reporting similar outcomes at similar time points to justify the combination of study results. A variety of outcome measures reported in each study does not allow us in most cases for standardized reporting of results.
Results of Individual Studies
An early explanation of the maxillary displacement was the nasal septal theory proposed by Scott, who stated that the nasal septal cartilage is buttressed against the cranial base which pushes the midface downward and forward.19, 20 Later, Latham who has done a pioneer work in growth and development of maxilla, modified Scott’s theory by stating that the septum is firmly attached to the premaxilla by a fibrous perichondral attachment called septopremaxillary ligament.4, 5, 15 He described this ligament as an apparent “key” structure that has a strong developmental relationship between the early maxillae and the nasal septum. Delaire had also described this ligament as the cellulous septum of the upper lip.4, 21 Though animal studies were excluded in the review, experimental studies on animal models also support the fact that the resection of septopremaxillary ligament resulted in deficient growth of the midface.22-25
Summary of Characteristics of Included Articles
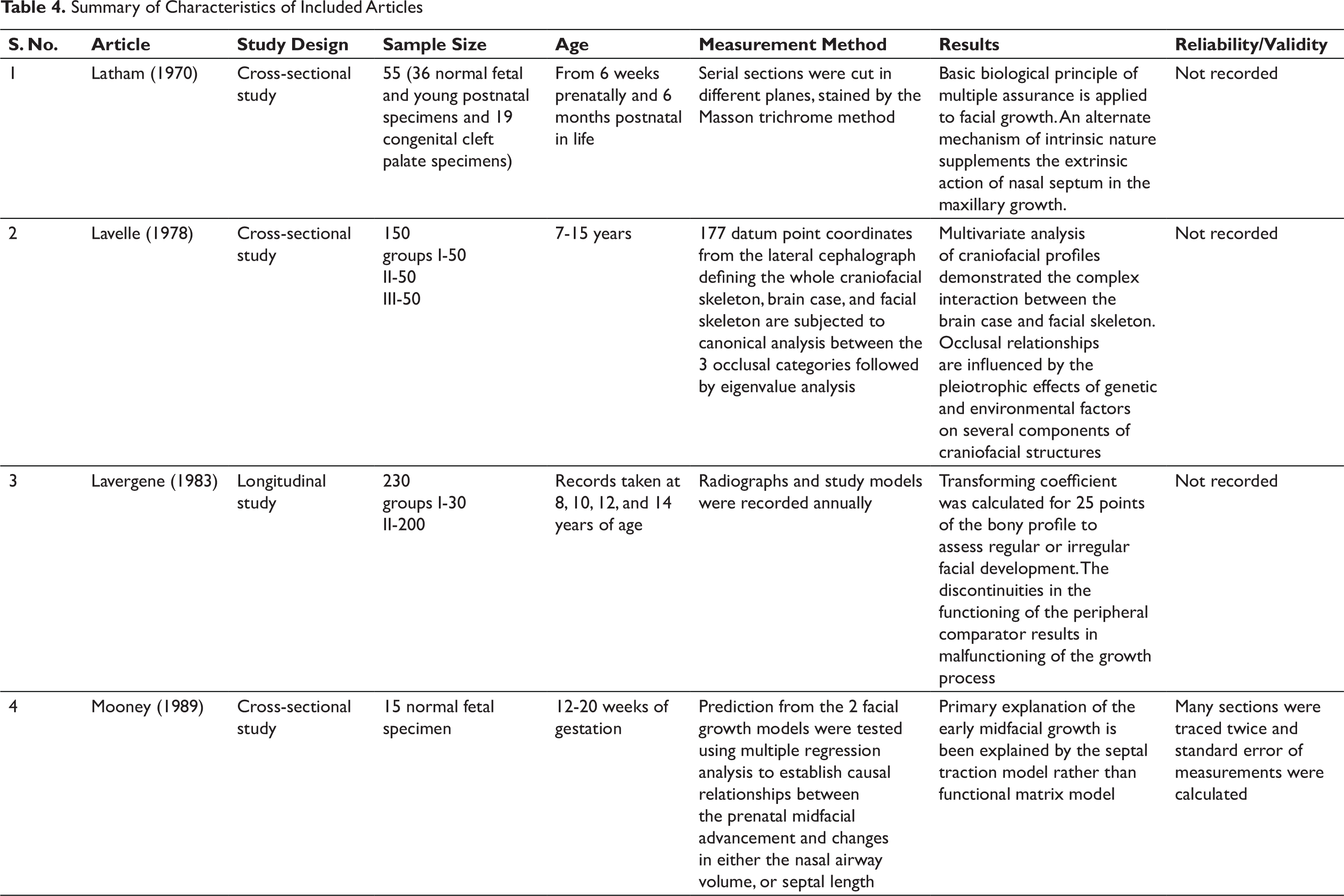
The study conducted by Lavergene and Petrovic tests the reality of the concept of an overall regularity of the biological mechanism that controls growth. At crucial moments of facial development very small fluctuations can result in variations in occlusal relationship. According to the servosystem concept, the pathogenesis of maxillary and mandibular malrelationship is due to malfunctioning of the servosystem. The sequential analysis of upper jaw growth control by somatotropin–Somatomedin by Lavergene and Petrovic emphasized the appositional growth of the anterior premaxillary extremity. It stated that the induction mechanism emanating through the forward traction of maxillary labial frenum and septopremaxillary ligament, biomechanical action of the labionary muscles results in local stimulation of the bone growth. The thrust effect on the premaxillary bone by these structures consists of histologic traction component of collagen fibers connecting the cartilage and bony trabaculae located immediately behind it. 17
Henceforth, the maxillary labial frenum, a dynamic structure with a diverse morphology 26 has a physiological importance by housing the septopremaxillary ligament 7 and the pull of the ligament induces alveolar basal bone development and translative growth of the maxilla. 1 Thus, the labial frenum, apart from providing stability to the upper lip, also contributes to the regulation of the midfacial growth.7, 27-31 In many instances, an aberrant frenum is reported to be associated with syndromic and nonsyndromic conditions with a retarded growth of the maxilla. 32
Discussion
The phenotype of the craniofacial region is determined by the combined effects of the genetic, intrinsic and extrinsic environmental factors. Structural variations can be either due to differences in functions or due to changes in the manner in which the functions are carried out, or both. The soft tissue matrix in which the skeletal elements are embedded tunes the bone morphology and forms the primary determinant of skeletal growth. 33 Most of the craniofacial defects are the result of the formation of abnormal extracellular matrix such as collagen and elastin. 34 Skeletal dysplasia are the outcome of interaction of numerous factors such as shape, the number and arrangement of teeth, relationship of the jaws and their related soft tissues including lips, cheek and tongue.35-37
The multiple assurance theory of Latham states that the processes and mechanisms of growth are always multifactorial. If any one of the determinants of growth process becomes inoperative, other morphological components provide an alternative means to achieve more or less the same developmental and functional end results, although perhaps with some degree of anatomic distortion. 15 Many studies support that the septopremaxillary ligament along with the maxillary labial frenum serves as a means of transmitting the septal growth force to the premaxilla bringing about the downward and forward maxillary growth in the prenatal and early postnatal stages.17, 23, 36 However, few animal studies revealed that the nasal septum provides only a mechanical support in the midfacial development. 20
The facial growth occurs as a response to functional needs. The muscular dysfunction during the early dentition period, if not self-corrected, becomes severe later. The tension of lip and cheek plays an important role in guiding the occlusal development which Moss described as form follows function. The developmental processes are regulated by intracellular signal transduction integrating the epigenetic information through the plasma membrane and cytoplasm to the nucleus. 34 Delaire established that the anatomic and neurophysiologic correlations between the labial frenum, septopremaxillary ligament, and interincisal suture are important determinants of vertical and anteroposterior relationship of mandible and nasomaxillary complex. 9 The fibrous tissue of the maxillary labial frenum traverses anteroposteriorly and merges with the submucosal fibers of the upperlip.26, 38 Hence, it can be assumed that in the case of an aberrant frenum these fibrous fibers are disrupted and remain attached to the interincisal suture that would halt the mechanotransduction process and limit the maxillary growth.
The Servosystem model of Petrovic explains that along with the genetic factors, the adaptability of the cells and tissues comprising the craniofacial skeleton influences the growth. He assumes that the maxillary displacement is by the direct thrust of the septal cartilage. The role of biomechanical forces exerted by the nasolabial muscles and the induction mechanism emanating from the septopremaxillary ligament and maxillary labial frenum results in forward traction of premaxilla.17, 19, 20 Moreover, a labial frenum which is retained in its primitive state even after the completion of the growth of the maxillary anterior alveolar process is indicative of maturational arrest. 39 Further any abnormalities in the integrity of the nasolabial muscles and/or mutilation of the labial frenum could also lead to retarded maxillary growth as stated by Delaire. 9
The Nasomaxillary Complex and Nasolabial Muscles
The nasomaxillary complex is displaced by the translation of the maxilla with the frontal bone, vertical elongation and the anterior rotation. The translative movement is influenced by the active growth of the brain and the cartilaginous nasal septum from birth to 3 to 4 years of age. The anterior thrust of the septal cartilage is transmitted to the anterior nasal spine by the septopremaxillary ligament and the nasolabial muscles. Delaire and Precious extensively studied about the potential role of the nasolabial muscles in regulating the maxillary growth which is enclosed in the maxillary labial frenum.4, 9
The transverse and the anteroposterior premaxillary growth are almost complete by 7 years of age, but the posterior part of the maxilla continues to grow actively during this period. 4 Mooney et al stated that the histological sections of the normal and cleft fetal and perinatal specimens suggest a complex interrelationship between the growth of the cartilaginous nasal septum, nasolabial muscular integrity, and midfacial advancement. 18
Nasolabial muscles are arranged in 3 concentric rings and are inserted onto the anteroinferior part of the nasal septum in the labioseptopremaxillary region. They play a unique role in the morphogenesis of maxilla. The important physiological elements in the superficial aponeurotic system are the transverse nasalis and Orbicularis oris which support the corresponding half of the upper lip and labial commissures. These fibers intermingle with the fibers of levator labii superiois, levator labii superiois alaque nasi, depressor septi, and levator anguli oris. The functions of the upper lip are primarily related to the horizontal and oblique fibers of the labionary muscles which produce pressure against the opposing lip and underlying structures. The upper lip forms the sagital fascia that forms a partition from the inferior border of the nasal septum to the frenum. Thus, the maxillary labial frenum forms the inferior aspect of this fascia, regulating the midfacial growth, and acts as an important determinant of vertical and anteroposterior relationship of both the jaws.17, 27, 40, 41
Maxillary Growth and Maxillary Labial Frenum: A Novel Synthesis
The maxillary labial frenum encloses the connective tissue: elastic fibers originating from the periosteum of the alveolus, septopremaxillary ligament from the anteroinferior part of the nasal septum to the mucosal part of the middle of the upper lip and then to the interincisal suture behind.4, 7 The primary function of the frenum is to keep a balance between the growing bones and the lip musculature. Aberrant frenum may affect the movement of these structures that may have an effect on the position of jaws and arrangement of dentition. 10
This review relates the modern concepts with the genomic and epigenetic mileu. The normal and abnormal skeletal growth mechanism is under the influence of nonskeletal tissues either directly or indirectly. 36 Once the functional occlusion is established, cartilaginous growth centers disappear and the maxillary growth depends on the secondary apposition of bone in the sutures and development of the dentition, predominantly under the functional control. It is a well-established fact that the aberrant labial frenum can result in hypofunctioning of the upper lip, which would indirectly have an impact on the growth of the maxilla.8, 27, 28
Functioning of the upper lip especially the movements of projection demonstrates the muscular anchorage at the anteroinferior part of the septum and anterior nasal spine which is transmitted to the interincisal suture, thus contributing to the facial growth regulation.27, 28, 36 A lack of stimulation of nasolabial muscles and lateral expansion of septopremaxillary ligament could result in deficient anterior maxillary growth. Changes in form or function of the bone are followed by structural changes in their internal architecture and external conformation. Thus, in case of an aberrant frenum, there is restricted lip movement altering the functional activity of septopremaxillary ligament and of the muscles in the labioseptopremaxillary region. This can be demonstrated with the myofunctional appliance where the orofacial muscles are activated to correct the abnormal muscle function.1, 42
The labial frenum is an important constituent of septopremaxillary traction system. 7 The importance of the frenum in regulating the facial growth could be emphasized by the symmetric reconstruction of the nasolabial muscles and preserving the integrity of the frenum during the cleft lip repair. 7 Altered muscle activity is the source of tension for the bones of attachment and causes bony changes. Todd stated that one area of disharmonic growth leads to subsequent disharmonies in the associated structures. 33 The independent growth of one part might influence the growth of the adjacent parts which in turn was growing independently. This is supported by Graber who emphasized the 3-dimensional effect of the muscles by his “3 M’s”. 43 Thus, in case of an aberrant frenum, bone formation takes place in presence of distorted muscular forces. 4
An analogy is helpful. A hypoplastic maxilla and deformed dental arch are the common sequelae after the cleft lip treatment. The scar tissue formed after the cleft lip repair can be either due to the tension of the tissues or on the tightness of the suturing or inherent reaction to surgical trauma. 44 Similarly, an aberrant labial frenum is considered to be in a state of maturational arrest 39 and the connective tissue and the muscle fibers in such cases might be entrapped into the periosteum of the interincisal suture. So, it is assumed that the muscle pull and the tension of the tissues in the aberrant frenum could act as scar tissue retarding the maxillary growth.
Limitations
There was only one longitudinal study included in this review. For assessing growth, longitudinal studies are the best choice that would obtain data at consistent intervals. The selected studies varied greatly with respect to the age, developmental stage, data collection techniques and analysis.
Conclusion
Extensive research in craniofacial biology is a necessity in understanding the myriad complexity of factors regulating the growth and development. An adequate knowledge of the developmental events and mechanisms of mechanical response of maxillary frenum on the maxillary growth is essential for planning an appropriate orthodontic therapy and intercepting the progression of the developing malocclusion.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.