
Abstract
Abstract
Objective: To investigate the effects of leukocyte-platelet-rich plasma (L-PRP) on the alveolar bone changes at the compression and tension sides during orthodontic tooth movement.
Materials and Methods: Around 20 New Zealand white rabbits were used in a split-mouth design. The maxillary first premolar was moved mesially with a nickel-titanium closed-coil spring. One side of the maxilla was randomly injected with L-PRP, while the contralateral side served as the control which received normal saline. The alveolar bone adjacent to the maxillary first premolar was scanned using microcomputed tomography at days 0, 7, 14, and 28. Microstructural parameters including bone volume fraction, trabecular thickness, and trabecular separation of alveolar bone were assessed on the compression and tension sides of the maxillary first premolar.
Results: Compared between the groups, the L-PPR group showed a significantly decreased bone volume fraction on the compression side on days 7 and 14 but significantly increased bone volume fraction on the tension side on day 14. However, there were no statistically significant differences in the parameters of trabecular thickness and trabecular separation.
Conclusion: Local administration of L-PRP may promote bone resorption on the compression side and bone formation on the tension side at the initial stage of orthodontic tooth movement.
Introduction
Orthodontic tooth movement is a process of bone remodeling with the consequence of an inflammatory process. Several pro-inflammatory cytokines and growth factors are released in response to mechanical forces and induce an inflammatory response in the early stage of tooth movement. Additionally, these molecules trigger a cellular response to promote bone resorption at the compression side and bone formation at the tension side. Therefore, the increased production of cytokines and growth factors may increase bone-remodeling activity. Consequently, the rate of tooth movement is accelerated.1, 2
Platelet-rich plasma (PRP) has been advocated as high concentration growth factors and cytokines that are secreted by activated platelets. 3 These bioactive molecules play an important role in stimulating cellular proliferation, migration, differentiation, and angiogenesis that are involved in the process of bone remodeling. 4 Although several studies suggested that the efficacy of PRP on bone healing resulted from the positive effect of the PRP contents, it is still controversial in the published results.5, 6 The reason for the difference of opinions may be the variations of the cellular constituents in PRP, particularly the presence of leukocytes in PRP. 7
Leukocyte-platelet-rich plasma (L-PRP) has high concentrations of leukocytes in PRP. Numerous studies provided evidence to support the application of L-PRP for therapeutic efficacy on tissue regeneration. 8 Furthermore, L-PRP was shown to contribute to enhanced cellular proliferation, chemotaxis, angiogenesis, and osteogenesis.9, 10 Moreover, previous studies reported that concentrations of leukocytes in L-PRP were related to increased levels of pro-inflammatory cytokines including interleukin (IL)-1, IL-6, and tumor necrosis factor-α (TNF-α) which are involved in the upregulation of the inflammatory process. 11 Additionally, the leukocytes in PRP may possibly stimulate the nuclear factor kB pathway through IL-1 and TNF-α to induce bone resorptive activity leading to decreased bone density. 12 For this reason, the inclusion of leukocytes in PRP may be desirable for bone remodeling during orthodontic tooth movement.
The increased demand for shorter durations of orthodontic treatment has been advocated to develop new methods to accelerate tooth movement. PRP was introduced to enhance the rate of tooth movement through increased osteoclastic activity which resulted in decreased bone density.13, 14 Moreover, a previous study demonstrated that the clinical effect of L-PRF facilitated orthodontic tooth movement into the recent extraction sockets. 15 Although research studies have been conducted to determine the benefits of PRP application on accelerated orthodontic tooth movement, the effects of the presence of high concentrations of leukocytes in L-PRP on bone remodeling remain unclear.
Recently, microcomputed tomography (micro-CT) has been suggested as the gold standard to evaluate bone morphology and microstructure. This technique can provide high-resolution three-dimensional (3D) images to obtain excellent reproducibility and accuracy of data for quantitative assessments. Additionally, micro-CT can be used to directly measure the 3D morphology of the trabecular bone including trabecular thickness and separation. 16 Therefore, the purpose of this study was to investigate the effects of L-PRP on the alveolar bone microstructure at the compression and tension sides during orthodontic tooth movement using micro-CT.
Materials and Methods
Study Design
This study was approved by the Animal Ethics Committee, Prince of Songkla University (MOE 0521.11/074). A total of 20 male New Zealand white rabbits, 3-to-4 months old and 2.5 to 3 kg in weight, were used in this study. Around 5 rabbits were randomly selected for the baseline group at day 0 (no intervention). The maxillary right and left sides of 15 rabbits were randomly divided into two groups, the L-PRP and the control groups, using a split-mouth design. In each animal, one side of the maxilla was randomly assigned to receive a single injection of L-PRP, while the contralateral side, which served as the control, received an injection of normal saline. All injections were submucosally administered in volumetrically equivalent at the buccal and lingual areas of the first maxillary premolar. The rabbits were analyzed for the bone volume fraction (BV/TV), trabecular thickness (Tb.Th), and trabecular separation (Tb.Sp) on the pressure and tension sides of each group on days 0, 7, 14, and 28.
All procedures were completed under general anesthesia by intramuscular injection. The rabbits were weighed to calculate an accurate dose of ketamine hydrochloride (25 mg/kg) in combination with xylazine hydrochloride (5 mg/kg).
L-PRP Preparation and Application
An amount of 10 mL of autologous blood was drawn from the central auricular artery of each rabbit into ethylenediaminetetraacetic acid anticoagulant. The L-PRR was prepared using the two-step centrifugation method as reported in a previous protocol. 17 In brief, the blood was centrifuged at 250g for 10 min for separation into three fractions: platelet-containing plasma at the top, buffy coat in the middle, and red blood cells at the bottom. The top two fractions were collected into a new tube and centrifuged again at 1,000g for 10 min. After discarding the supernatant platelet-poor plasma, the precipitated platelets and leukocytes in the residual plasma were homogenized to obtain 1 mL of L-PRP. A sample of 0.5 mL of the L-PRP was set apart to determine the concentration of platelets and leukocytes using a hematology analyzer. The remaining 0.5 mL of the L-PRP was submucosally injected with a 27 gauge dental needle into the buccal and lingual areas of the first maxillary premolar.
Orthodontic Procedures
A nickel-titanium closed-coil spring (13 mm in length and 1.5 mm in diameter) was ligated between the maxillary first premolar and incisor on each side. A force gauge (Correx, Haagstreit, Bern, Switzerland) was used to measure 100g of force to move the maxillary first premolar mesially. Retention of the appliance was checked at each time point to ensure they were unimpaired.
Microcomputed Tomography Analysis
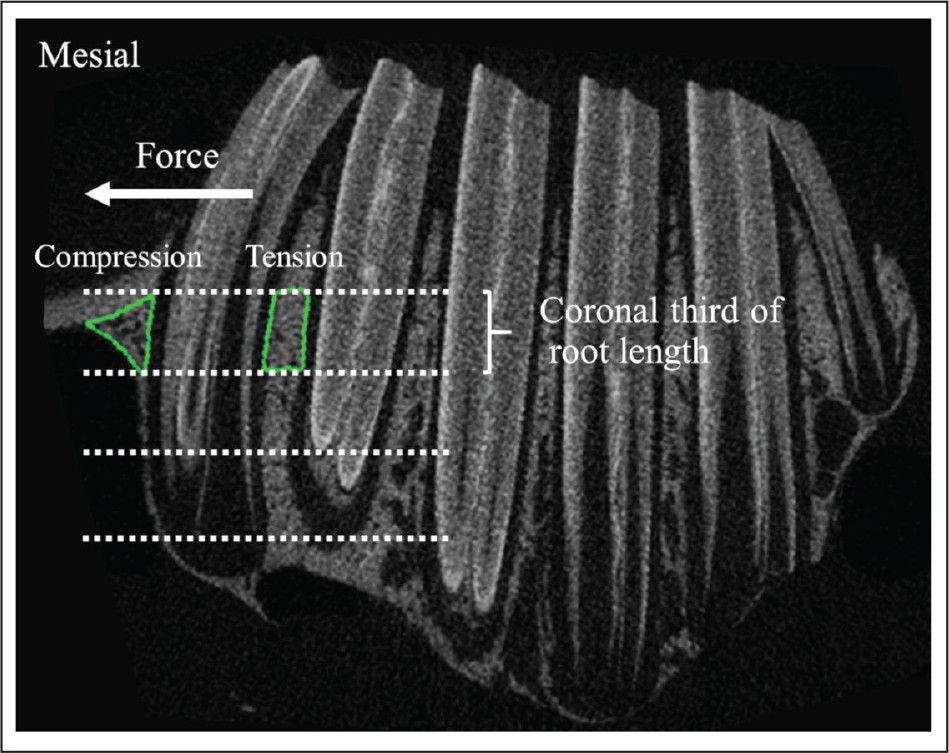
The rabbits were euthanized with an overdose of anesthetic drug at each time point (0, 7, 14, and 28 days). Then the maxillae were harvested and fixed in 10% neutral buffered formalin within 48 hours. The dissected maxilla was scanned using a Scanco µCT 35 system (Scanco Medical, Bassersdorf, Switzerland) with a voxel size of 18.5 µm at the condition of 70 kVp and 114 µA. After scanning, the image reconstruction was performed with the manufacturer’s software. To analyze the images, the region of interest was defined as the areas of alveolar bone at the mesial and distal sides near the coronal thirds of the root of the maxillary first premolar as representatives of alveolar bone properties at the compression and tension sides, respectively (Figure 1). Measurements of the microstructural parameters of alveolar trabecular bone including the BV/TV, Tb.Th, and Tb.Sp were determined using image analysis software (µCT 35 Version 4.1, Scanco Medical, Bassersdorf, Switzerland).
Regions of interest of alveolar bone at the mesial and distal sides of the coronal thirds of the root of maxillary first premolar.
Statistical Analysis
The data are presented as means and standard deviations of each group. The Shapiro-Wilk test was used to assess the normal distribution for all parameters which showed normal distributions. A comparison of the results between the groups was carried out by independent-sample t-test. The intragroup comparisons were analyzed using repeated measure one-way analysis of variance (ANOVA) followed by the Bonferroni post-hoc comparisons when a significant overall main effect was found (P < 0.05). Intraclass correlation coefficients were used to assess intraoperator reliability. All subjects were randomly selected and repeatedly evaluated at two weeks after the first measurement. A P value less than 0.05 was considered to indicate a statistically significant difference. The statistical analyses were performed using SPSS version 17 (SPSS, Chicago, IL, USA).
Results
Components of Whole Blood and L-PRP
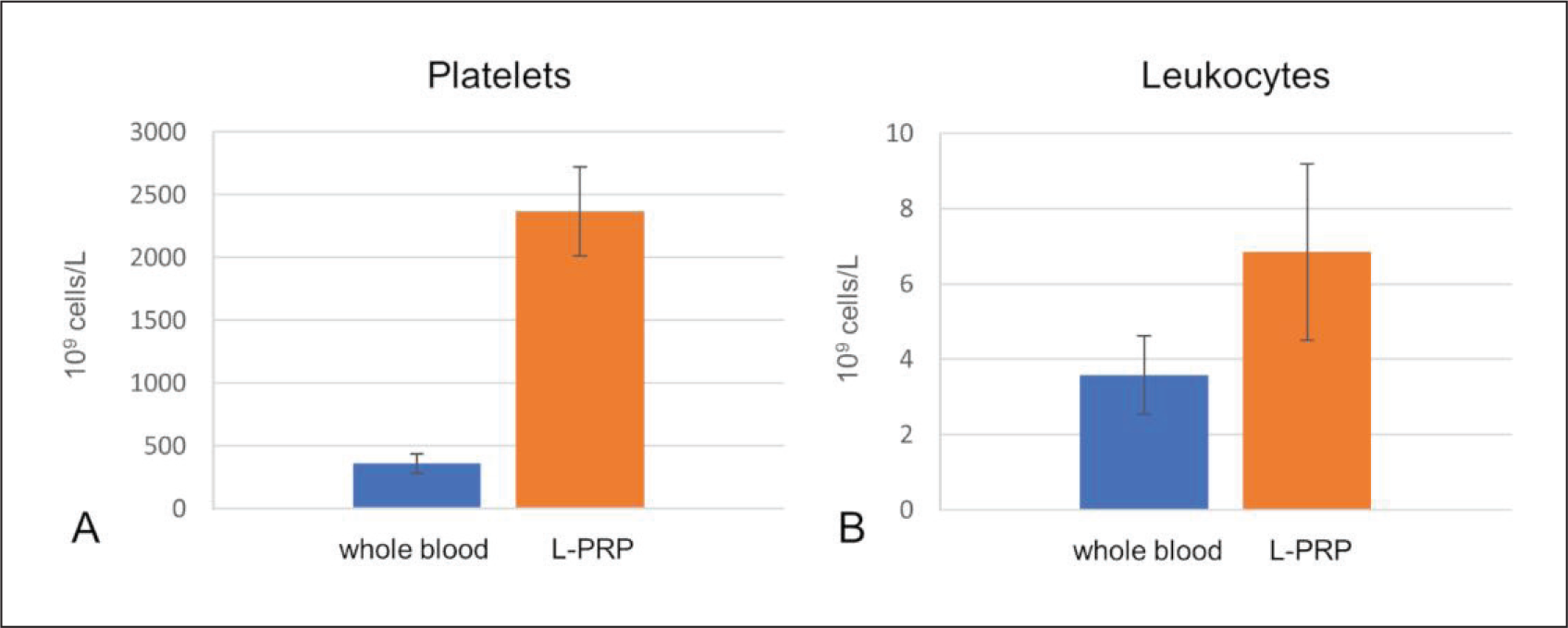
The mean platelet concentrations of whole blood and L-PRP were 360.90 ± 77.92 × 10 9 cells/L and 2,366.81 ± 353.81 × 10 9 cells/L, respectively (Figure 2A). The mean leukocyte concentrations of whole blood and L-PRP were 3.58 ± 1.05 × 10 9 cells/L and 6.85 ± 2.34 × 10 9 cells/L, respectively (Figure 2B).
Microstructural Parameters of the Alveolar Trabecular Bone
The intraclass correlation used for the intraoperator reliability evaluation was 0.81 for the micro-CT analysis. Thus, the measurement technique was considered to have acceptable reliability.
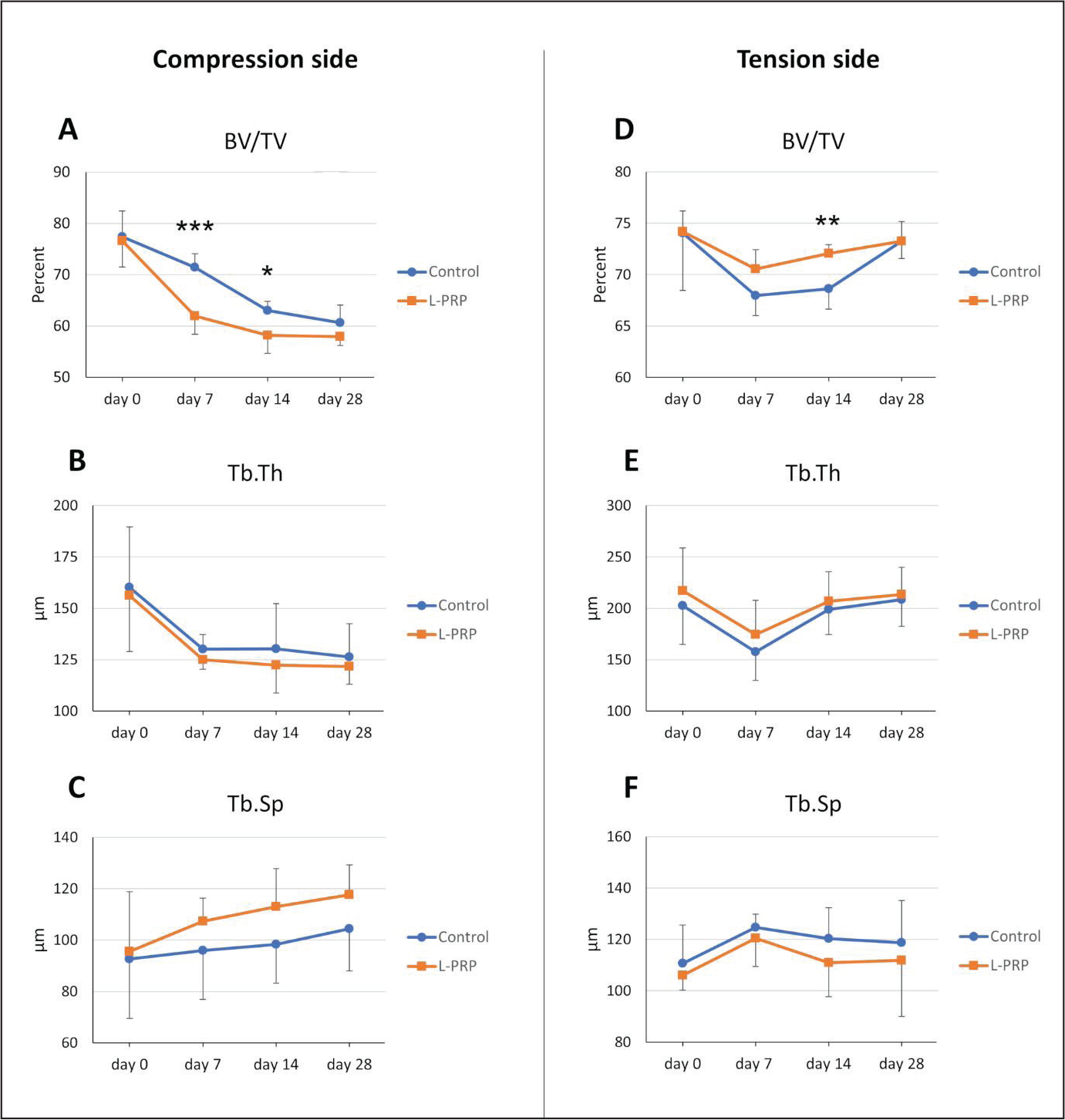
Microstructural parameters for the trabecular bone on the compression (mesial) side of the root of the maxillary first premolar are summarized in Table 1. The results demonstrated that the significant decreases of BV/TV were found in the L-PRP group from day 0 to day 7 (P < .05) and the control group from day 7 to day 14 (P < .05). In a comparison of the two groups, the L-PRP group showed significantly lower BV/TV values than the control group at day 7 (P = .001) and day 14 (P < .05; Figure 3A). However, the changes in Tb.Th and Tb.Sp were not significant (Figure 3B and 3C).
Concentrations of (A) Platelets and (B) Leukocytes in Whole Blood and L-PRP
. Microstructural Parameters of Trabecular Bone on the Compression Side of the Maxillary First Premolar at Different Time Points
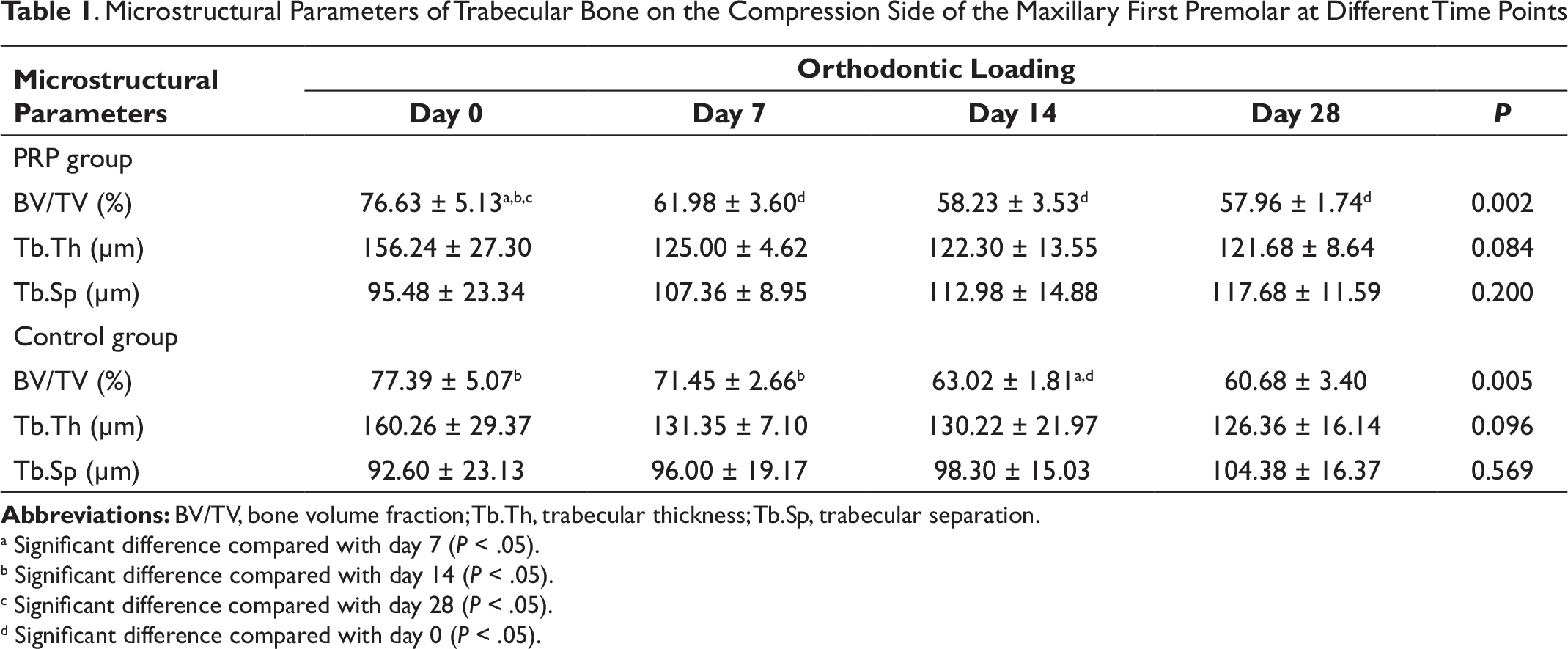
Abbreviations: BV/TV, bone volume fraction; Tb.Th, trabecular thickness; Tb.Sp, trabecular separation.
a Significant difference compared with day 7 (P < .05).
b Significant difference compared with day 14 (P < .05).
c Significant difference compared with day 28 (P < .05).
d Significant difference compared with day 0 (P < .05).
. Microstructural Parameters of Trabecular Bone on the Tension Side of the Maxillary First Premolar at Different Time Points
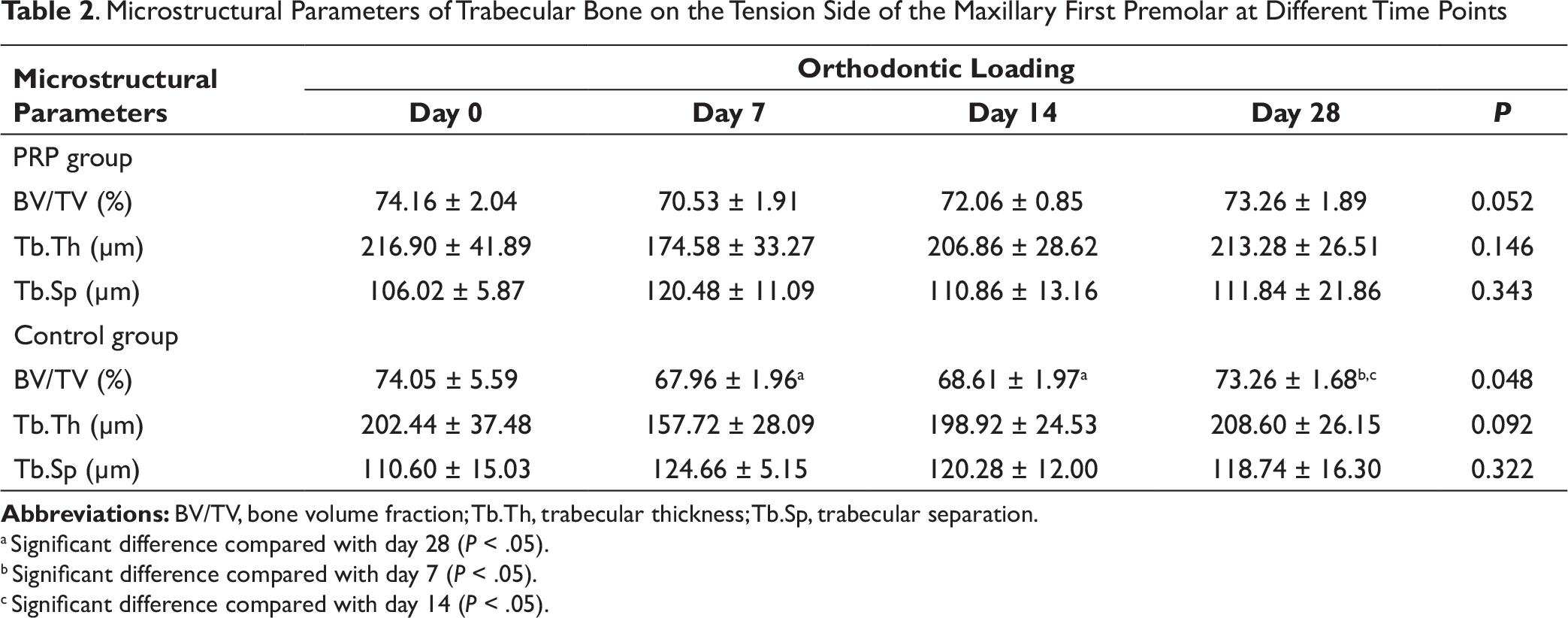
Abbreviations: BV/TV, bone volume fraction; Tb.Th, trabecular thickness; Tb.Sp, trabecular separation.
a Significant difference compared with day 28 (P < .05).
b Significant difference compared with day 7 (P < .05).
c Significant difference compared with day 14 (P < .05).
The microstructural parameters for trabecular bone on the tension (distal) side are summarized in Table 2. A comparison between the two groups showed that the L-PRP group had a significantly greater BV/TV value than the control group at day 14 (P < .01; Figure 3D). However, the Tb.Th and Tb.Sp did not have any significant differences at any of the time points (Figures 3E and 3F).
Discussion
This study investigated the effect of L-PRP on the microstructural bone changes under orthodontically-induced tooth movement. Our results showed that an injection of L-PRP had the positive effect of inducing bone remodeling which decreased bone density on the compression side but increased bone density on the tension side. A previous study by Akbulut et al 18 reported that an injection of PRP without leukocytes did not have a beneficial effect on either bone formation or bone resorption. This possibly resulted from the different cellular constituents of PRP, particularly the leukocytes which have an influence on the levels of growth factors and cytokine concentrations. The presence of leukocytes in PRP could contribute to higher levels of growth factors compared to leukocyte-poor PRP. 19 Another reason for different results is the different methods of evaluation. For example, a histologic analysis can provide more information on the cellularity in bone remodeling. However, the limitation is the 2-dimensional (2D) stereological analysis of a few random 2D planar sections which can only infer the trabecular morphology, such as trabecular thickness and separation. On the other hand, direct 3D measurements can provide these parameters with a larger volume of interest. The high-resolution 3D images using micro-CT in this study could directly measure the bone microstructure without model-based stereology. 16
On the compression side, alveolar bone change of the maxillary first premolar demonstrated that the BV/TV in the L-PRP group was significantly less than the control group on days 7 and 14 after force application, which corresponded to greater decreases of Tb.Th in the results. It indicated that a greater bone density reduction possibly resulted from osteoclast induced bone resorption on the surface of the trabecular bone. Similarly, an increase of Tb.Sp due to bone resorption on the trabecular surface leading to more space between trabeculae was observed in the L-PRP group. This may have occurred because of the increased proinflammatory cytokines derived from the leukocytes in the PRP including IL-1, IL-6, and TNF-α. 11 The roles of these cytokines are involved in the process of bone resorption initiated by cytokine-induced inflammation during orthodontic tooth movement. 2 Therefore, the presence of leukocytes in the L-PRP may augment the inflammatory and catabolic cytokine availability leading to the initiation of inflammation and bone resorption on the compression side, which resulted in a greater reduction of trabecular bone density and thickness as well as a greater increase in the trabecular space.
Interestingly, our results found that the BV/TV on the compression side in the L-PRP group had significantly decreased during the first week, while the control group showed a sharp decrease of BV/TV in the second week. This finding agreed with a previous study that reported decreased alveolar bone density that began on day 3 and was more significant on day 7 in PRP injected rats. 13 Meanwhile, the results in the control group demonstrated that the reduction of alveolar bone density remained steady from day 3 to 7 and then dropped considerably after the first week. In accordance with the phases of orthodontic tooth movement, the initial phase is a rapid tooth movement that occurs in a few days after force application. Then, the lag phase, known as a time of limited tooth movement, which is because of the elimination of hyalinized tissues until day 7. Finally, it is the post-lag phase in which the undermining bone resorption occurs thereafter. 20 Therefore, our findings could imply that the significantly-decreased BV/TV in the first week in the L-PRP group may possibly indicate a decreased time period of the lag phase after the initial phase of orthodontic tooth movement, which resulted in accelerated tooth movement. In agreement with a clinical study, 15 the positive effect of leukocyte-platelet-rich fibrin was facilitating tooth movement into the socket of extracted premolars.
On the tension side, the L-PRP group showed a significantly greater BV/TV than in the control group on day 14. This result agreed with the finding of a previous study 21 that found significant bone neoformation in the irradiated tibiae of rats at day 14 after PRP application. This might be explained by the growth factors derived from the platelets in the PRP including transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), vascular endothelial growth factor (VEGF), and insulin-like growth factor (IGF), which are involved in bone repair and regeneration. Hu et al 22 demonstrated that the expressions of VEGF and PDGF in PRP are important mediators to enhance angiogenesis by recruiting the endothelial cells and osteogenesis by directly regulating the differentiation of osteoblasts. They also suggested that the influence of these factors was able to increase alkaline phosphatase activity and the expression of type I collagen which indicated osteoinductive ability. Thus, anabolic growth factors released from the platelets in L-PRP may have beneficial effects on bone formation at the tension side.
According to the biphasic theory of orthodontic tooth movement, orthodontic forces induce the biological responses of cells resulting in two sequential phases of alveolar bone remodeling in which the catabolic phase occurs followed by the anabolic phase. 23 Similarly, our results showed that the BV/TV on the tension side had a slight decrease in the first week followed by a continuous increase until day 28 when the BV/TV was nearly the same as day 0. Like a previous study on a rat model, 24 the gene expressions relevant to bone resorption were observed at day 3 after orthodontic force application, while the gene expressions relevant to bone formation were observed after 7 days. Additionally, a micro-CT study to analyze alveolar bone on the tension side during orthodontic tooth movement illustrated that bone formation occurred with thicker trabecular bone in the second week. 25
During orthodontic tooth movement, the compression force induces cellular responses to release inflammatory mediators which activate osteoclast-mediated bone resorption. Osteoclasts are crucially important in the activation of osteoblasts through direct cell-cell interaction or paracrine signaling that directly recruits and activates osteoblasts. Additionally, growth factors including TGF and IGF-1 are released from the matrix of resorbed bone to induce osteoblast migration and differentiation for new bone formation. 26 A previous study suggested that the compartment in orthodontic tooth movement could not be divided into two different areas that react independently to a force applied. 27 Therefore, accelerated tooth movement should focus on promoting both osteoclastogenesis and osteoblastogenesis. As a result, the administration of L-PRP may be a feasible method to facilitate orthodontically-induced tooth movement due to a combination of catabolic and anabolic biological factors released from L-PRP to provide a favorable environment for the balance of bone resorption and bone formation during bone remodeling.
Numerous studies suggested that isolated chemical agents used to stimulate an artificial pathway were able to increase the rate of tooth movement.28, 29 However, tooth movement is a biological process of bone remodeling induced by mechanical loading that triggers many cytokines to participate in the inflammatory process. Thus, injection of one cytokine or growth factor may not imitate a balance between pro- and anti-inflammatory mediators in the normal inflammatory response. 30 In contrast, L-PRP contains various growth factors and cytokines with a natural balance of anabolic and catabolic functions, 31 which are supposed to be more effective than the actions of a single growth factor. Additionally, these biological molecules have a longer sustained release due to fibrin clots of the PPR that are delivered slowly into the injection site. However, our results showed that the clinical efficacy of L-PRP on bone remodeling may have a positive influence at the 2-week interval of orthodontic tooth movement. This result was consistent with the findings of Schar et al 9 : the growth factors and catabolic cytokines of L-PRP were almost degraded after 2 weeks of application.
A limitation of this study was the limited sample size which may have contributed to the lack of statistical significance in Tb.Th and Tb.Sp. Furthermore, the measurements of the release of growth factors and cytokines in the L-PPR injections were not performed. The characteristics of the biological properties may be needed to clarify the biological responses of L-PRP on tooth movement. In addition, a micro-CT analysis does not provide a detailed characterization of the cellular events. Thus, further studies are needed to perform histological examinations, and the duration of the L-PRP injection needs to be determined for optimal effectiveness to promote bone remodeling in orthodontic tooth movement.
From these results, a single submucosal injection of L-PRP may have a positive effect on bone remodeling at the initial stage of orthodontic tooth movement to promote both bone resorption on the compression side and bone formation on the tension side in terms of changes in BV/TV of alveolar bone.
Conclusion
On the compression side, the BV/TV significantly decreased at days 7 and 14 in the group that received L-PRP.
On the tension side, the BV/TV significantly increased at day 14 in the group that received L-PRP.
The injection of L-PRP appears to have influenced the decrease in bone density on the compression side at the initial stage at the first week, while normal tooth movement was observed in the control group in the second week.
Footnotes
Acknowledgments
This study was supported by Graduate School and Faculty of Dentistry, Prince of Songkla University, Songkhla, Thailand.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.