
Abstract
Abstract
Introduction: A change in occlusion during orthodontic treatment can affect muscles and joints surrounding the jaw, resulting in temporomandibular disorders (TMD). The aim of this study was to determine the effect of orthodontic treatment with straight-wire appliance on the incidence of TMD in young adults.
Materials and Methods: A cohort study was carried out involving 177 adult patients (91 in the treatment group and 86 in the control group). Fonseca’s questionnaire was used for TMD evaluation for all patients at the time of obtaining orthodontic pretreatment records (T0). TMD assessment was repeated after an average of 3 years of initial assessment for both the treatment and control groups (T1).
Results: The number of patients with TMD changed significantly (P < .001) from T0 to T1 in both groups. The prevalence of TMD increased from 36.3% to 41.8% in the treatment group and decreased from 46.5% to 38.4% in the control group after 3 years. The relative risk of developing TMD after orthodontic treatment was 1.16, whereas the odds of TMD resolution after orthodontic treatment was 0.73, both of which were statistically nonsignificant (P > .05).
Conclusion: Orthodontic treatment with noncustomized straight-wire appliance has nonsignificant effects on the incidence of TMD in young adults.
Keywords
Introduction
Temporomandibular disorders (TMD) affect the lives of about 56% to 87.7% of the world population.1, 2 The most common symptoms associated with temporomandibular joint (TMJ) are joint sounds, pain in TMJ, pain in adjacent muscles, restriction of mouth opening, and jaw deviation to 1 or both sides during mouth opening. 3 TMJ noises are best heard by the patient himself, but palpation and auscultation are valid procedures that can help in the diagnosis of joint sounds. 4 The importance of possible etiological factors for the development of TMD has been evaluated in many studies.5, 6 Factors predisposing to the development of TMD can be systemic, psychological (personality and behavior), and structural (malocclusion and other types of occlusal discrepancies, joint laxity, and others).5, 6 According to some studies, the occlusal factors are of minor etiological importance for pain and functional disorders in the masticatory system, but the role of occlusion in the etiology of TMD is still controversial.7, 8
Malocclusion and TMJ disorders are 2 separate entities, but both are quite prevalent in different groups of population. As the function of TMJ is directly related to the mandibular movements as guided by occlusion, 9 researchers from every part of the world have been trying to find the association between malocclusion and TMJ disorders. Some investigators have stated that joint sounds are related to orthodontic malocclusions, but a final conclusion has not been reached.10-13
Any type of orthodontic treatment that directly affects the bite plane of the patient also affects the muscles and joints surrounding the jaw. 14 Hundred percent control over bite plane cannot be expected from any type of orthodontic treatment that uses appliances with noncustomized appliance prescription. 15 The cosmetic correction usually brought about by straight-wire appliance, comprising of brackets, bands, archwires, and accessories, can strain TMJ in an attempt to accommodate for changes. This reorganization of joint structures may help in the resolution of TMD or, contrarily, may interfere with the normal functioning of the joint. 16 It is yet unclear whether orthodontic treatment is actually helping the patient in terms of TMJ functioning or not.
A TMD secondary to malocclusion should ideally respond to fixed orthodontic treatment, and interestingly, some investigations have actually shown that both the signs and symptoms of TMD decrease during the active phase of orthodontic treatment. 17 But the long-term follow up after orthodontic treatment does not show any promising results. The reason might be that the orthodontically moved teeth are more sensitive to contact, resulting in a decrease of oral parafunctions and altered activity of the jaw muscles. This might provide temporary relief in TMD. 18
With a few exceptions, 12 treatments of malocclusions with fixed orthodontic appliances do not have a great preventive influence on the development of signs and symptoms of TMD.13, 19 But the incidence of TMD as a complication of orthodontic treatment is not fully investigated. So, it may be practical to say that the role of orthodontics in TMD development is not fully known and therefore deserves further investigation. In this context, we planned this study to determine the effect of fixed orthodontic treatment on the incidence of TMD.
Materials and Methods
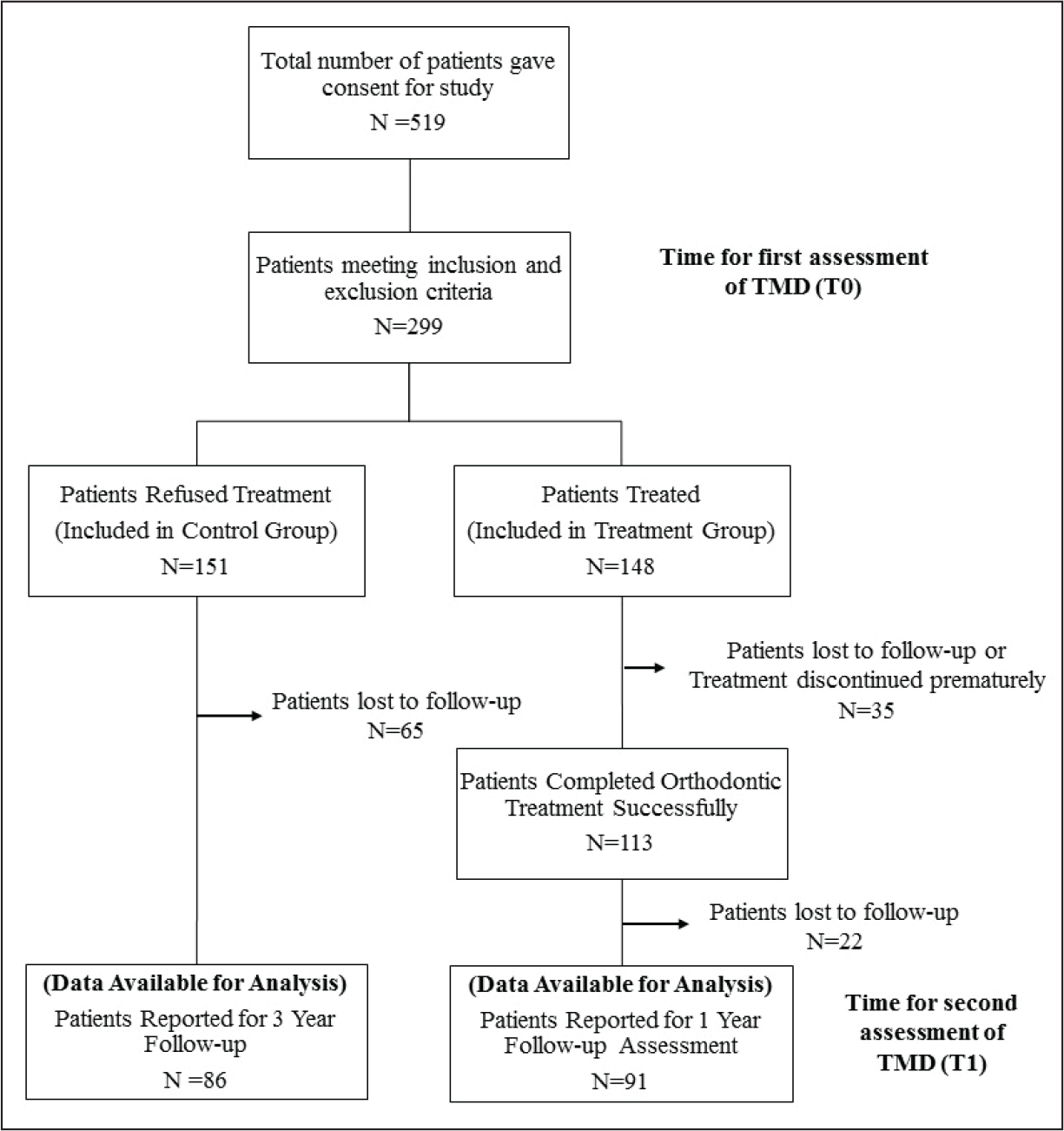
This was a multicenter cohort study involving patients with grade 2 to 4 dental malocclusion according to the Index of Orthodontic Treatment Needs (IOTN) dental health component. Ethical approval was obtained from an institutional ethical review committee prior to data collection (ethical committee approval no. DAS-12-07). Sample size for the treatment and control groups was calculated by taking α = .05 and keeping a power of study of 80%. Findings of Pullinger et al 20 were used for sample size calculation, showing that at least 76 patients were required in each group. However, to improve the power of the study, maximum number of available patients were included in the study. A nonprobability consecutive sampling technique was used. In total, 91 patients requiring only fixed orthodontic treatment were included in the treatment group and 86 patients also requiring only fixed orthodontic treatment but opted not to receive any type of orthodontic treatment were included in the control group. Informed consent was obtained prior to data collection. Strengthening the Reporting of Observational Studies in Epidemiology guidelines for reporting cohort studies were followed. The process of reaching the final number of participants in each group is elaborated in Figure 1.
Flow Chart Representing the Process of Reaching the Final Number of Participants
The following inclusion criteria were used:
patients having no missing (excluding third molars) or heavily restored tooth patients with good quality pretreatment orthodontic study models patients more than 17 years and less than 31 years of age
Patients in the treatment group underwent comprehensive orthodontic treatment with fixed orthodontic appliance at 3 different teaching institutes of Pakistan under the supervision of consultant orthodontists.
The following exclusion criteria were included:
patients who had incomplete orthodontic treatment patients with a history of any syndrome patients with a positive history of trauma to the craniofacial region or any other condition that could affect the function of TMJ
Data Collection
A complete history was taken from each patient, and relevant information was recorded on separate pro forma for the treatment and control groups. Clinical examination and evaluation of dental casts were carried out to determine the IOTN category of each patient.
The assessment of TMD was carried out using a questionnaire proposed by Fonseca.
21
This tool can be used for classification of patients according to severity of TMD and has been proven to be highly efficient in obtaining epidemiological data.
22
Fonseca’s questionnaire, composed of 10 questions, follows the characteristics of a multidimensional evaluation.
21
These questions were as follows:
Is it hard for you to open your mouth? Is it hard for you to move your mandible from side to side? Do you get tired/muscular pain while chewing? Do you have frequent headaches? Do you have pain on the nape or stiff neck? Do you have ear aches or pain in craniomandibular joints? Have you noticed any TMJ clicking while chewing or when you open your mouth? Do you clench or grind your teeth? Do you feel your teeth do not articulate well? Do you consider yourself a tense (nervous) person?
The study participants were informed that these questions should be answered with a “yes,” “no,” or “sometimes” and that only 1 answer should be marked for each question. The patients in the control group were called after 3 years, and the same data collection protocol was repeated to record a second assessment. As the average duration of orthodontic treatment was around 2 years, the second assessment for patients in the treatment group was carried out 1 year after treatment, making it a 3-year period in total from the time of the first assessment. The time of this second assessment for TMD was regarded as T1.
Information regarding the nature and duration of orthodontic treatment, time passed since completion of orthodontic treatment, and whether any tooth was extracted for orthodontic purposes was also collected for the treatment group. Lastly, patients in the treatment group were asked whether orthodontic treatment had any effect, either positive or negative, on their masticatory abilities.
Data Analysis
Fonseca’s questionnaire contains a reference index that was used to classify participants as having mild TMD, moderate TMD, severe TMD, or no TMD. For the analysis, the answers “yes,” “sometimes,” and “no” from each questionnaire were attributed a value of 10, 5, and 0, respectively. The final value was compared with the clinical index, and the patients were classified according to the clinical index classification of Fonseca’s questionnaire:
Total score between 0 and 15 points No TMD Total score between 20 and 40 points Mild TMD Total score between 45 and 65 points Moderate TMD Total score between 70 and 100 points Severe TMD
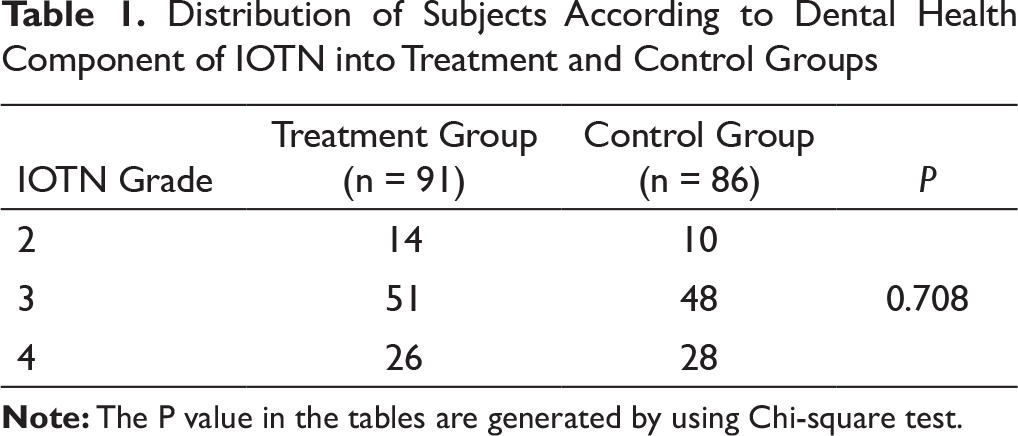
Distribution of Subjects According to Dental Health Component of IOTN into Treatment and Control Groups
Results
The control group had 86 participants (57 female and 29 male), while the treatment group had 91 participants (63 female and 28 male). Participants in the control and experimental groups had comparable severity of dental malocclusion according to IOTN (P = .708) (Table 1).
The mean ages of patients in the treatment group and control group were 21.44 + 3.16 and 21.36 + 2.55 years, respectively. This age difference was statistically nonsignificant (P = .856). Similarly, both groups had comparable gender distribution (P = .748). The orthodontic treatment of 41 patients involved extraction of 1 or more permanent tooth for orthodontic reasons. The mean treatment duration was 24.14 + 2.95 months (21.67 + 2.39 and 26.43 + 3.34 months for nonextraction and extraction cases, respectively).
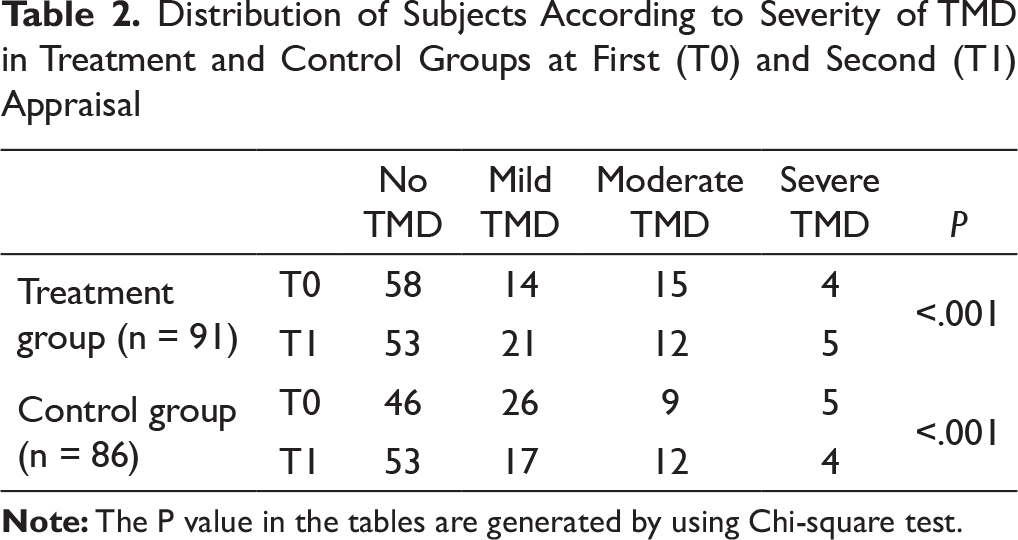
Highly significant differences (P < .001) were found in the prevalence of TMD at T0 and T1 in both groups. More than half the participants (63.7% in the treatment group and 53.5% in the control group) were categorized under no TMD group at the T0 according to Fonseca clinical index. More participants moved from the no TMD group to different TMD groups after orthodontic treatment, while the number of participants free from any TMD increased at T1 in the control group. The prevalence of TMD increased from 36.3% at T0 to 41.8% at T1 in the treatment group and decreased from 46.5% at T0 to 38.4% at T1 in the control group (Table 2).
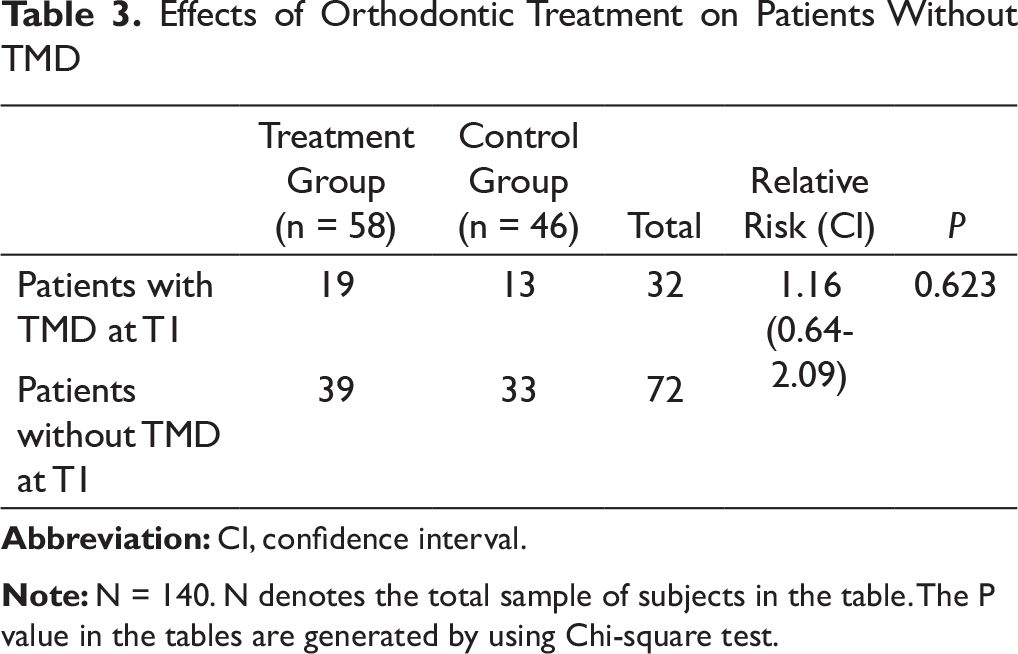
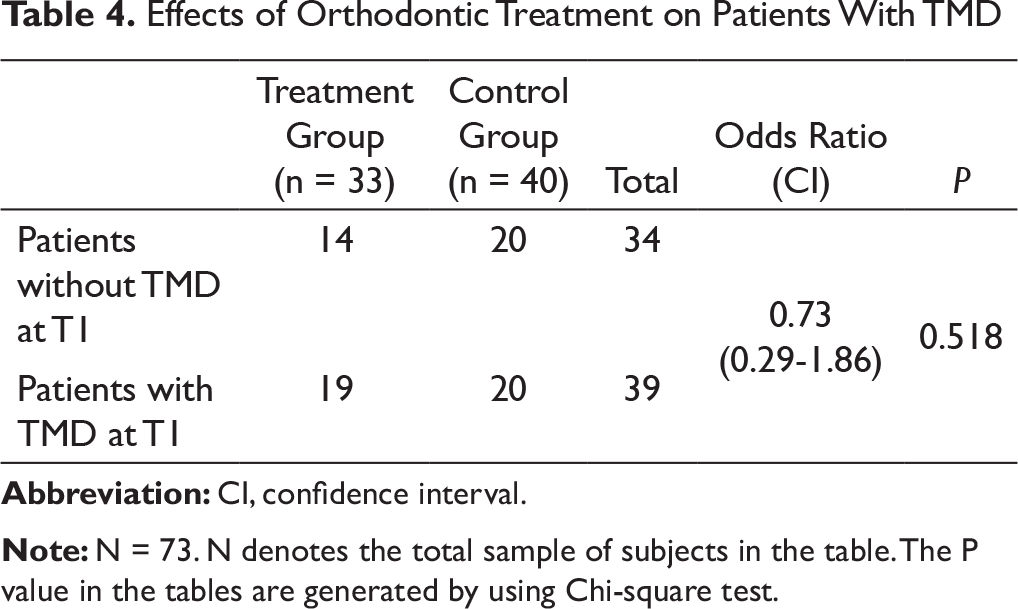
Jaw deviation was present in 4 participants out of which 3 recovered after orthodontic treatment. One patient developed jerky movements of the joint on wide mouth opening after orthodontic treatment, while maximum mouth opening was reduced in 1 patient. The relative risk of developing TMD after orthodontic treatment was found to be 1.16 (Table 3), while the odds of TMD resolution after orthodontic treatment was 0.73, both of which were statistically nonsignificant (P > .05) (Table 4).
Distribution of Subjects According to Severity of TMD in Treatment and Control Groups at First (T0) and Second (T1) Appraisal
Effects of Orthodontic Treatment on Patients Without TMD
Effects of Orthodontic Treatment on Patients With TMD
Discussion
Fonseca’s questionnaire is a reliable tool for collecting a large volume of information in a relatively short period of time. It is easy to use, has good patient acceptability, and is almost devoid of any examiner influence. 22
The dental occlusion achieved at the end of orthodontic treatment does not stay the same. A minor degree of relapse is inevitable in most of the cases. Relapse is most common in the first year after orthodontic treatment and may result in occlusal interferenes. 23 Hence, a second assessment was carried out after 1-year retention period in the treatment group.
The relationship between the so-called occlusal interference and the development of TMD is still controversial, but several reviews declare it very weak or nonexisting. 24 The correlation of different signs and symptoms of TMD with orthodontic treatment has been extensively discussed in previous studies.25-27 Magnusson et al 28 followed teenaged individuals over 5 years and showed that joint sounds come and go and often are unrelated to the major masticatory symptoms. In the present study, a significant change in the severity of TMD was noticed among adult patients who did not have any kind of orthodontic treatment, thus corroborating the findings of previous studies.28-30 Moreover, the current study failed to denote a significant increase in the risk of developing TMD after fixed orthodontic treatment. Researchers know that it is difficult to establish a cause and effect relationship between orthodontic treatment and TMD because of a large number of confounders affecting the TMJ function.5, 6
Studies that evaluated the effects of orthodontic treatment on TMD gave heterogeneous results with some studies finding small positive effects in treated patients and others finding no differences or negative effects between groups. 31 Our study showed that orthodontic treatment is likely to affect the functioning of TMJ, but the frequency of clinical changes brought about by such treatment is not significant when compared with the control group. Though majority of the participants in our study identified improvement in their masticatory efficacy after orthodontic treatment, pain in TMJ and associated muscles is still the leading symptom after fixed orthodontic therapy. Similar complications of orthodontic treatment with fixed appliances have already been reported by Mohlin et al. 32
Although this study directly addressed the clinical aspects of TMD, the use of diagnostic imaging techniques and a psychiatric evaluation could be of greater benefit in terms of correct diagnosis of underlying pathology. The current study investigated young adults only as with increasing age the signs of wear and tear of dentition and confounders like missing teeth or dental prosthesis get common. However, the effects of orthodontic treatment in other age groups should also be investigated as there is evidence that the adaptability of TMJ decreases with age. 30 Literature provides us with enough evidence that severe skeletal and dental malocclusions are frequently associated with TMD.33, 34 In this study, an attempt was made to exclude all such cases by including patients with IOTN grade 2 to 4 malocclusion. IOTN is among the most reliable indices used for the assessment of orthodontic treatment need and was chosen as a tool to assess the treatment need of study participants in the present study.35, 36 Lastly, the study included both patients who had extraction and nonextraction orthodontic treatment. There has been a debate regarding the effect of extraction versus nonextraction orthodontic treatment on the development of TMD.37, 38 More recently, Okeson reported in his centennial special article 39 that the effect of extraction versus nonextraction orthodontic treatment on TMD is equivocal. Therefore, we combined the sample of both extraction and nonextraction groups to increase the power of the study.
This multicenter study gives an insight into how frequently a simple treatment of mild to moderate malocclusion with contemporary fixed appliance can affect the TMJ functioning and the masticatory efficiency of a patient, which is probably a neglected aspect of orthodontist treatment.
Conclusion
There was no significant risk of developing TMD with fixed orthodontic treatment with straight-wire appliance in adults with orthodontic problems of mild to moderate malocclusion. However, a majority of the orthodontically treated patients noticed a significant improvement in their masticatory function, but the odds of TMD resolution were nonsignificant.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.