
Abstract
Abstract
Loss of the mandibular molar can lead to extrusion of maxillary molar, which may result in occlusal interference and inadequate space to restore the mandibular edentulous space with prosthesis. This molar extrusion also leads to functional disturbance. Thus, the present article will showcase the fabrication of simplified spring to intrude the maxillary first molar within 9 weeks.
Introduction
Tooth intrusion is one of the most difficult movements in orthodontic mechanics, and it becomes more difficult when molar is extruded due to the absence of its antagonist tooth 1 (Figure 1A). Molar extrusion can result in many problems such as occlusal interferences and functional disturbances, 2 and thus, it is very necessary to intrude it so that prosthetic rehabilitation can be achieved in the antagonist tooth region.
There are several intra and extraoral mechanics for the intrusion of molar's, 3 but nowadays the most commonly used one is a temporary anchorage device (TAD). As placing TAD is an invasive procedure, majority of the patients hesitate to place it in them and thus ask for other alternatives. In some cases, an inadequate space was observed for the placement of TADs between the posterior teeth roots for molar intrusion. Thus, this article showcases an easy way out to intrude the maxillary first molar by using simple spring mechanics without using TADs.
Showing (A) extruded maxillary first molar, (B) Intraoral buccal view of intrusion spring, (C) Palatal anchorage unit on working cast, (D) Intraoral palatal view of intrusion spring.

Materials Required
Pre-fabricated molar bands and stainless steel band strips, 19 gauge stainless steel wire, 0.16 × 0.22″ stainless steel wire, solder, flux, and weldable premolar brackets.
Methodology
Anchorage Unit
The pre- fabricated bands were placed on maxillary first molars bilaterally including the extruded first molar (Figure 1A) and fabricated on both first premolars. The premolar brackets were welded on the first premolar band of the first quadrant and at the center of the extruded first molar band both palatally and buccally. Next, maxillary impression was made, and these bands were transferred for working models.
On the working model, the one end of 19" SS wire was soldered palatally to the bands of both first premolars bilaterally and to the first molar band on counter side (second quadrant) in order to gain anchorage from them. An anchorage was further enhanced by fabricating an acrylic plate on Palate incorporating the free ends of 19" SS wire (Figure 1C).
Fabrication of Spring
The springs were fabricated with 0.16 x 0.22" SS wire and were placed both buccally and palatally for the intrusion. Both springs consisted of 2 arms i.e. active arm and retentive arm along with helix for activation. The active arm was kept longer as compared to the retentive arm for more flexibility.
Placement of Spring and Activation
On buccal aspect, the retentive arm of fabricated spring was ligated in first premolar bracket for anchorage purpose and active arm in maxillary first molar bracket for its intrusion. (Figure 1B) On palatal aspect, the retentive arm of spring was embedded in acrylic plate for palatal anchorage, whereas active arm was ligated in extruded maxillary first molar bracket (Figure 1C and D). A 60° gingival bend was given in active arm both buccally and lingually for the true intrusion forces.
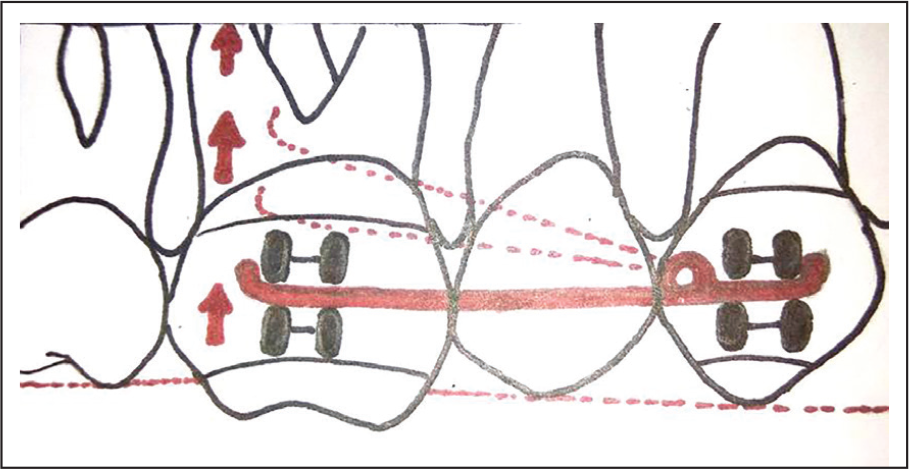
Schematic diagram shows simplified intrusion spring and how spring activated for true intrusion of maxillary first molar.

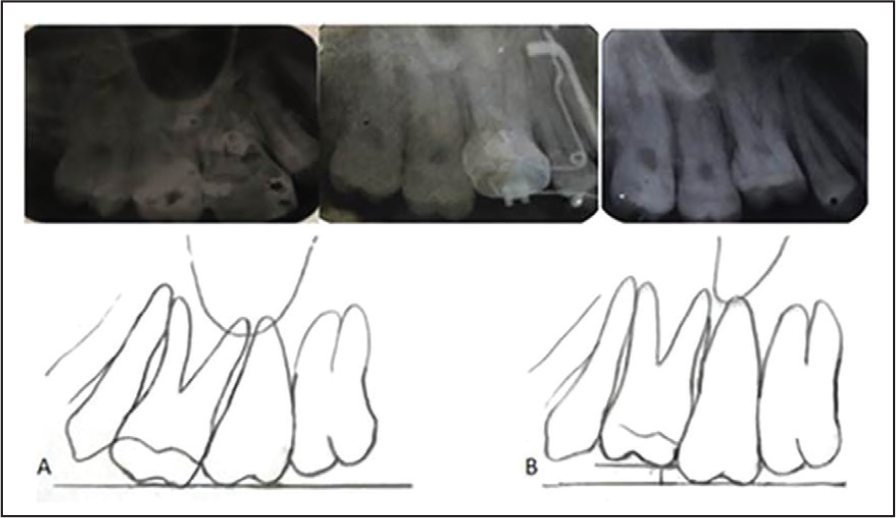
An IOPAR shows an Intra-oral periapical radiograph of maxillary first molar: pre-Intrusion, mid-Intrusion, post-Intrusion and schematic diagram shows comparison of: (A) Pre-Intrusion and (B) Post-Intrusion IOPAR tracings.
For true intrusion, after every 3 weeks, these springs were activated by closing the helix or by bending the active arm gingivally both buccally and lingually by 60° (Figure 2). The anchorage from palate and other teeth avoided the reactionary extrusive forces of other teeth and resulted in true intrusion instead of buccal tipping of molar.
In the patient, after continuous active therapy for 9 weeks, a significant true intrusion of molar was observed without showing any sign of palatal cusp hanging, that is, buccal tipping (Figure 3). An over intrusion was done to overcome the relapse. An IOPAR shows an Intra-oral periapical radiographic view of the well appreciated true intrusion of Maxillary first molar (Figure 4).
Advantages
It can be used in cases where TADs cannot be used due to inadequate space for its placement.
Noninvasive procedure, simple design, and easy fabrication.
This is a segmental approach and can be used on either side for molar intrusion.
It can be used in patients undergoing molar intrusion who do not want complete orthodontic treatment.
Summary
Thus, it can be concluded from this article that these simple springs can be used for true intrusion of molar as they are very easy to fabricate, easy to activate, non-invasive, can be used segmentally, and there is no need to bond rest of the teeth.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.