
Abstract
The clinical relevance of pancreatic histologic changes in cats is unclear. Determination of clinical relevance is complicated by the focal to multifocal nature of these lesions, variable clinical presentation of affected cats, and common comorbidities. Examining the histologic changes on serial pancreatic sections from a cohort of young adult shelter cats without externally observable clinical disease could inform what should be considered normal in cats. Pancreata were obtained from 48 cats euthanized for population control. While hypoalbuminemia was common, liver enzyme activity and gastrointestinal panel results were largely unremarkable. The pancreas was sectioned every 1 cm, routinely processed, and evaluated by a board-certified veterinary pathologist. Pancreatic histologic changes were uncommon in this cohort of cats. Hematoxylin and eosin-stained sections that showed lymphocytic infiltrates were recut for CD3 and CD20 immunohistochemistry. The distribution of CD3 and CD20 positive cells and their percentages were recorded. Of 48 cats, 13 cats (27%) had localized lymphocytic infiltrates with a median percentage of affected sections of 14% (range: 7%–92%). There were no differences in observed percentages or distribution of T- or B-cells. Scattered CD3+ T-cells were incidentally identified in intralobular parenchyma. As mild lymphocytic infiltration was uncommon in this group of cats, it may not indicate a physiological response, as the anticipated response to antigenic stimulation would be expected to occur more diffusely and more commonly. Thus, the role of these infiltrates may reflect bystander inflammation or a primary pathological process (pancreatitis) and likely varies depending on the specific disease context.
The pancreas is a critical organ for digestion and metabolism because of its exocrine and endocrine functions. Pancreatitis, an inflammatory condition of the pancreas, is among the most common exocrine pancreatic disorders in cats, as evidenced by histologic studies. 15 Histologically, the chronic form, often characterized by lymphoplasmacytic infiltration and fibrosis, is the most common.7,21,32 The histologic prevalence is more accurately estimated when serial sectioning of the pancreas is performed, as this approach increases detection of focal to multifocal lesions that are characteristic of the disease in cats and reduces the likelihood of false-negative results.
A previous necropsy study documented that chronic pancreatitis (CP) was present in 67% of 115 cats presented for necropsy and in 45% of 41 apparently healthy cats. 7 Another study documented lymphocytic inflammation of the pancreas in 56/60 (93%) cats that presented for necropsy and mild lymphoplasmacytic infiltration (affecting <10% of the section) in 51/60 (85%) cats. 32 The authors of that study deemed this to be consistent with erratic small nests of lymphocytes (which is considered normal),24,32 rather than inflammatory infiltrates, which is a debated interpretation. 16 A review has hypothesized that a high prevalence of lymphocytic inflammation may reflect a physiological response to antigenic stimulation. 3 These varying interpretations highlight the challenge of determining the clinical relevance of mild lymphocytic infiltrates as well as other histologic lesions of pancreatitis in cats. It is therefore important to determine whether lymphocytic infiltrates are normal (physiological), an epiphenomenon of other primary pathological changes in the pancreas (bystander inflammation), or pancreatitis.
Determination of the clinical relevance of histological lesions of the feline pancreas is limited by typically small tissue samples and a focal to multifocal distribution of feline pancreatic lesions. Pancreatic biopsies without lesions need to be interpreted cautiously, 33 whereas pancreata collected for the purpose of research studies, allow for much more extensive serial sectioning and hence a more comprehensive assessment for multifocal lesions.7,32 However, similar intense histologic assessment from a healthy feline population is lacking, but could contribute significantly in interpreting the relevance of cellular infiltrates.
We had the opportunity to work with an animal control facility that had to euthanize animals for population control. It was deemed that evaluation of pancreatic tissue from this group could act as an apparently healthy study group. In addition, the types and distribution of cells, particularly lymphocytes, could be determined so that the clinical relevance might be interpreted in affected cats. Scattered lymphocytes, especially around ducts, vessels, and in peri-islet locations, have generally been considered physiologic in humans. 4 Until now, no research studies have characterized the phenotypes and spatial distribution of the immune cell infiltrates in the feline pancreas.
Accordingly, the aims of this study were (1) to determine the prevalence and characteristics of exocrine pancreatic histopathologic changes and (2) to immunohistochemically characterize the various patterns of lymphocytic infiltrates identified in our study population. We hypothesized that if certain histological changes should be considered physiologic, they would occur consistently across serial sections of the pancreas from individual cats, and in multiple cats in the study population.
Materials and Methods
Cats that were scheduled to be euthanatized due to over-population were enrolled in our study from 2019 to 2021. Pancreata from 48 cats were isolated from the duodenum and collected within approximately 1.5 hours of death. Serial sections that were perpendicular to the longitudinal axis of the pancreas were made every 1 cm, and subsequently stained with hematoxylin and eosin (H&E) for grading by a board-certified veterinary pathologist using a published semiquantitative scoring system for pancreatitis, 15 which was established based on a past study. 7 The scoring was based on an ordinal point system for 2 histologic variables of acute pancreatitis (AP; neutrophilic inflammation and edema/fat necrosis) and 3 histologic variables of CP (lymphocytic inflammation, fibrosis, cystic degeneration). The ordinal point system allows translating subjective impressions of the percentage of affected parenchyma (or number of cysts for cystic degeneration) to a score from 0 through 3, with 3 being most severely affected. Score 0 for most histologic variables indicates its absence in the evaluated section, except for lymphocytic inflammation (eg, fibrosis scores: 0, 0%; 1, <15%; 2, 15%–30%; 3, >30% of the parenchyma affected; cystic degeneration scores: 0, 0 cysts; 1, ≤3 cysts; 2, 4–5 cysts; 3, ≥6 cysts.). Scores of 1, 2, and 3 for lymphocytic inflammation correspond to <25%, 25%–50%, and >50% of the parenchyma affected, respectively. Score 0 for lymphocytic inflammation was defined as no or isolated lymphocytes or erratic small nests of lymphocytes; specific maximal number of lymphocytes or percentage of affected parenchyma that qualified as “small nests of lymphocytes” was not defined in the scoring system. Distribution of the lymphocytic infiltrates that were not parenchymal (ie, interstitial, periductal) was not defined in the scoring system and hence was not specifically assessed when determining the score for lymphocytic inflammation. Similarly, distribution of fibrosis (eg, perilobular, interlobular, intralobular, periductal) was not part of the scoring system, and hence distribution of fibrosis was not considered when determining the score for fibrosis.
A classification of different types of pancreatic cystic lesions was not specifically defined in the establishment of the scoring system,7,15 but cystic (acinar) degeneration was reported to be gradually increased as other lesions of CP were more prominent in cats in the study. 7 Accordingly, cystic degeneration was defined as cysts that developed centrilobularly, lined by acinar cells, initially without much evidence of fibrosis or inflammation.
Mean cumulative scores (MCSs) for each histologic variable were calculated by dividing the sum of the scores from each section by the number of sections evaluated, as described in previous studies.31,32 The mean cumulative score for CP (MCS-CP) was a sum of the MCSs for lymphocytic inflammation (MCS-LI), fibrosis (MCS-fibrosis), and cystic degeneration. Due to the lack of number of cats with lesions consistent with AP and without a species-specific scoring scheme for nodular hyperplasia, MCS-based analyses were not performed for AP or nodular hyperplasia in this study.
Blood was collected either antemortem or immediately postmortem for serum biochemistry and a gastrointestinal (GI) panel, including feline pancreatic lipase immunoreactivity (fPLI) concentration, and feline trypsin-like immunoreactivity concentration. Serum biochemistry profiles were analyzed using an automated analyzer (AU 480 chemistry analyzer, Beckman Coulter, Indianapolis, Indiana); serum cobalamin (reference interval, 290–1500 ng/L) and folate concentrations (reference interval, 9.7–21.6 μg/L) were measured by automated competitive binding chemiluminescence immunoassays (IMMULITE 2000 XPi, Siemens Healthineers, Erlangen, Germany). Serum fPLI concentrations (reference interval, ≤ 4.4 μg/L) were measured using a commercially available enzyme-linked immunosorbent assay kit (Spec fPL, IDEXX Laboratories, Westbrook, Maine). 45 Serum trypsin-like immunoreactivity concentrations were measured by a previously validated inhouse radioimmunoassay36,37 at the Gastrointestinal Laboratory, Texas A&M University.
CD3 and CD20 Immunohistochemistry Assay
To evaluate the immunohistochemical characteristics of sections containing lymphocytic infiltrates on the H&E-stained slides, CD3 and CD20 immunohistochemical assays (Table 1) were performed on unstained slides from each of the blocks. Immunohistochemistry (IHC) was performed using the Leica BOND RX Fully Automated Advanced Staining System (Leica Microsystems, Buffalo Grove, Illinois). Lymph nodes were used for positive control tissue for each tray (batch control), and pancreatic parenchyma (areas without lymphocytic infiltrates) was used as a negative tissue control.
Immunohistochemistry assay protocol and reagents.

Abbreviation: NA, not applicable.
CD3 and CD20 Immunohistochemical Characteristics
Distributions of T- or B-lymphocytes were recorded (parenchymal, interstitial, or periductal) for each stained section. Parenchymal localization was defined as within the pancreatic parenchyma (intralobular). Interstitial was defined as areas that are outside of the pancreatic parenchyma (such as interlobular, within connective tissues) and not close to a pancreatic duct; periductal was defined as located in the immediate vicinity of a pancreatic duct as determined by histologic assessment, including the connective tissue that surrounds the pancreatic duct, and within or around the pancreatic ductal epithelium.
When at least one cluster (defined as a group of at least 5 lymphocytes easily identifiable at low power at 4×) of lymphocytes was present, the percentage of T- and B-lymphocytes was estimated.
Statistical Analyses
Demographics, number of cats with histologic pancreatitis, and its severity were described by descriptive statistics. Normality was assessed with a Shapiro-Wilk test and quantile-quantile plot. Serum biochemistry and GI panel results were compared between cats with or without pancreatic lymphocytic infiltrates using a t-test or a Mann-Whitney U test as appropriate. Adjusted P values were calculated using the Bonferroni method to control type I error inflation due to multiple comparisons. Spearman’s correlations were evaluated between MCS-LI and serum fPLI concentration, MCS-CP and serum fPLI concentration, and between MCS-LI and MCS-fibrosis. All statistical analyses were performed using R Statistical Software (v4.5.1; R Core Team 2022) or GraphPad Prism software (v9.0.0; GraphPad, San Diego, California). Statistical significance was set as a P value < .05.
Ethical Approval
The study was reviewed and approved by the Clinical Research Review Committee at Texas A&M University (IACUC 2017-0190 CA and IACUC 2020-0121 CA). Informed owner consent forms were obtained from the animal control facility for each enrolled cat.
The data analyzed in this study are available via reasonable request to the author.
Results
Demographics
Most cats (40/48, 83%) were domestic short hair cats, followed by domestic medium hair cats (5/48, 10%), and one cat each for domestic long hair, Maine Coon, and Siamese. Cats were estimated to be young based on dentition and available records (median age: 2 years, range: 0.5–6 years). There was approximately equal distribution between intact males (26/48 cats, 54%) and intact females (22/48 cats, 46%). In general, cats were mildly underconditioned, with a median body condition score of 3.5 (range: 2–5) of 9. Of 48 cats, only 1 (2%) showed histologic lesions consistent with AP (ie, edema and fat necrosis, without concurrent neutrophilic infiltration), and 15 (31%) showed lesions consistent with CP (ie, lymphocytic infiltrates, fibrosis, cystic degeneration) in at least one pancreatic section (Table 2).
Number of cats with histologic pancreatitis and the associated severity per published score. 15

Abbreviations: AP, acute pancreatitis; CP, chronic pancreatitis.
Scoring of Histologic Variable and Percentage of Affected Pancreatic Section
The median number of pancreatic sections evaluated per cat was 13 (range: 9–17) sections. In this cohort, cats with either histologic lesions consistent with AP or CP were only mildly affected, with all identified lesions being scored as 1 (Table 3).
Number of cats affected with each histologic variable and the associated scoring.

Lymphocytic infiltrates were the most common finding (13/48 cats, 27%), followed by fibrosis (8/48 cats, 17%), and cystic degeneration (2/48 cats, 4%) (Fig. 1). The median percentage (min.–max.) of sections affected by these lesions per cat was 14% (7%–92%) for lymphocytic infiltrates, 9% (7%–58%) for fibrosis, and 20% (13%–27%) for cystic degeneration (Supplemental Fig. S1). The median MCS (min.–max.) of histologic lesions per cat was 0 (0–0.92) for lymphocytic/mononuclear infiltrates, 0 (0–0.58) for fibrosis, 0 (0–0.27) for cystic degeneration, and 0 (0–1.5) for total CP score (Supplemental Fig. S2).

Features of mild chronic pancreatitis in cats. Pancreas, cat. Hematoxylin and eosin. (a) Small cluster of lymphocytes within (intralobular) and surrounding (interlobular) pancreatic lobules. Case 18. (b) Large cluster of intralobular lymphocytes. Case 33. (c) Mild interlobular fibrosis with mild mononuclear infiltrates. Case 35. (d) Cystic degeneration. Large cyst lined by acinar cells and surrounded by a fibrous band and lymphocytic infiltrates. The lining cells have normal zymogen granules. Inset: high magnification of lining acinar cells with zymogen granules and fibrosis. Case 41.
None of the cats had neutrophilic inflammation in any of the sections, but one cat had histologic lesions consistent with AP, which was determined based on edema and fat necrosis in a single section (MCS = 0.06).
Of 48 cats, 12 cats had nodular hyperplasia identified on H&E-stained slides; 4/12 cats (n = 17/36 sections) had nodular hyperplasia and lymphocytic inflammation concurrently present in at least one of the H&E-stained sections. Of these 17 sections, 14 sections from 3/4 cats had observable lymphocytic infiltrates surrounding or within the nodular hyperplastic focus.
Serum Biochemistry and GI Panel Results
Serum biochemistry and GI panel results are summarized in Supplemental Table S1. Hypoalbuminemia was the most common biochemistry alteration (34/48 cats, 71%), followed by hyperglycemia (33/48 cats, 69%), and elevated aspartate aminotransferase activities (23/48 cats, 48%). Otherwise, liver values (eg, alanine transaminase, alkaline phosphatase, total bilirubin, gamma-glutamyl transferase) and GI panel results were largely unremarkable for the study cohort of cats (Supplemental Table S1). The few cats with abnormalities in these parameters included the following: for cats with pancreatic lymphocytic infiltrates (13/48 cats, 27%), hypoalbuminemia was common (9/13 cats, 69%). Three of these 13 cats had elevated alanine transaminase activities, 4/13 cats had hypocobalaminemia, and 1/13 cats had a serum fPLI concentration in the equivocal range (5.8 µg/L, case 8). There were no statistical differences in serum biochemistry and GI panel results between cats with or without pancreatic lymphocytic infiltrate in this cohort, as all adjusted P values were 1 (Table 4).
Biochemistry and gastrointestinal panel results of cats with or without pancreatic lymphocytic infiltrates.

Abbreviations: ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BUN, blood urea nitrogen; fPLI, feline pancreatic lipase immunoreactivity; fTLI, feline trypsin-like immunoreactivity; GGT, gamma-glutamyl transferase.
Correlation Between Selected MCS of Histologic Variables and Serum fPLI Concentration
Serum fPLI concentrations were not statistically significantly correlated with MCS-LI (rs = 0.16, P = .29) (Supplemental Fig. S3a). The cat (case 8) with the most extensive lymphocytic infiltrates throughout the pancreas (11 affected sections of the total 12 sections) had the highest serum fPLI concentration (5.8 µg/L). Supplemental Fig. S3b shows the scatter plot of serum fPLI concentrations and MCS-CP, which did not show a statistically significant correlation (rs = 0.25, P = .09); 15 cats had an MCS-CP that corresponded to mild CP (Table 2). MCS-LI and MCS-fibrosis were statistically significantly correlated (Fig. 2; rs = 0.57, P < .0001).

Scatter plot for the correlation between mean cumulative scores for lymphocytic inflammation (MCS-LI) and mean cumulative scores for fibrosis (MCS-fibrosis) of pancreata sections from 48 cats euthanized for population control. Spearman’s correlation coefficient = 0.57 (95% confidence interval: 0.34–0.74), P value < .0001. The positive correlation indicates that cats that were more affected by lymphocytic infiltrates had more extensive fibrosis, suggesting that lymphocytic infiltrates might be involved in the pathogenesis even in this cohort of cats with mild lesions.
CD3 and CD20 IHC
Among the 13 cats with pancreatic lymphocytic infiltration, there were a total of 39 affected sections. Unstained sections were recut from these 39 tissue blocks to perform CD3 and CD20 IHC. Of the 39 recut sections, 19/39 (49%) sections from 7 cats had T- and/or B-cells present on the recuts. Nineteen of 39 (49%) recut sections revealed cluster(s) of T-cells, and 17/39 (44%) sections revealed cluster(s) of B-cells, while 16/39 (41%) had both. Of the clusters of lymphocytes, the median percentage of T-cells was 50% (range: 25%–50%), and the median percentage of B-cells was 50% (range: 20%–75%). However, the percentages of T- and B-cells could be quite different between clusters (Fig. 3).

Composition of CD3+ and CD20+ lymphocytes in pancreatic lymphocytic infiltrates in cats. Pancreas, cat. CD3 and CD20 immunohistochemistry (a) CD3+ T-cells and (b) CD20+ B-cells comprising approximately 50% each of a lymphocyte cluster. Case 18. (c) CD3+ T-cells comprising approximately 75% of the cluster while (d) CD20+ B-cells occupy around 25% of the cluster, showing vague follicular organization. Case 10.
For the distribution of the lymphocytes, T-cells are present in similar proportions in the parenchyma, interstitium, and around the pancreatic ducts, in terms of both the percentage of affected sections and the number of affected cats. B-cells seemed to be mostly located periductally, followed by interstitial and parenchymal locations in terms of percentage of affected sections; however, slightly more cats had B-cells identified in the interstitium (Fig. 4, Table 5).

Examples of the distribution of CD3+ T-cells in cat pancreas. Pancreas, cat. CD3 immunohistochemistry. Examples of immunolabeling for CD3+ T-cell clusters that are present (a) in the parenchyma (case 39), (b) around the pancreatic duct (case 8), and (c, d) in the interstitium (cases 35 and 41).
Distribution of T- and B-cells and percentages of affected sections and cats. a
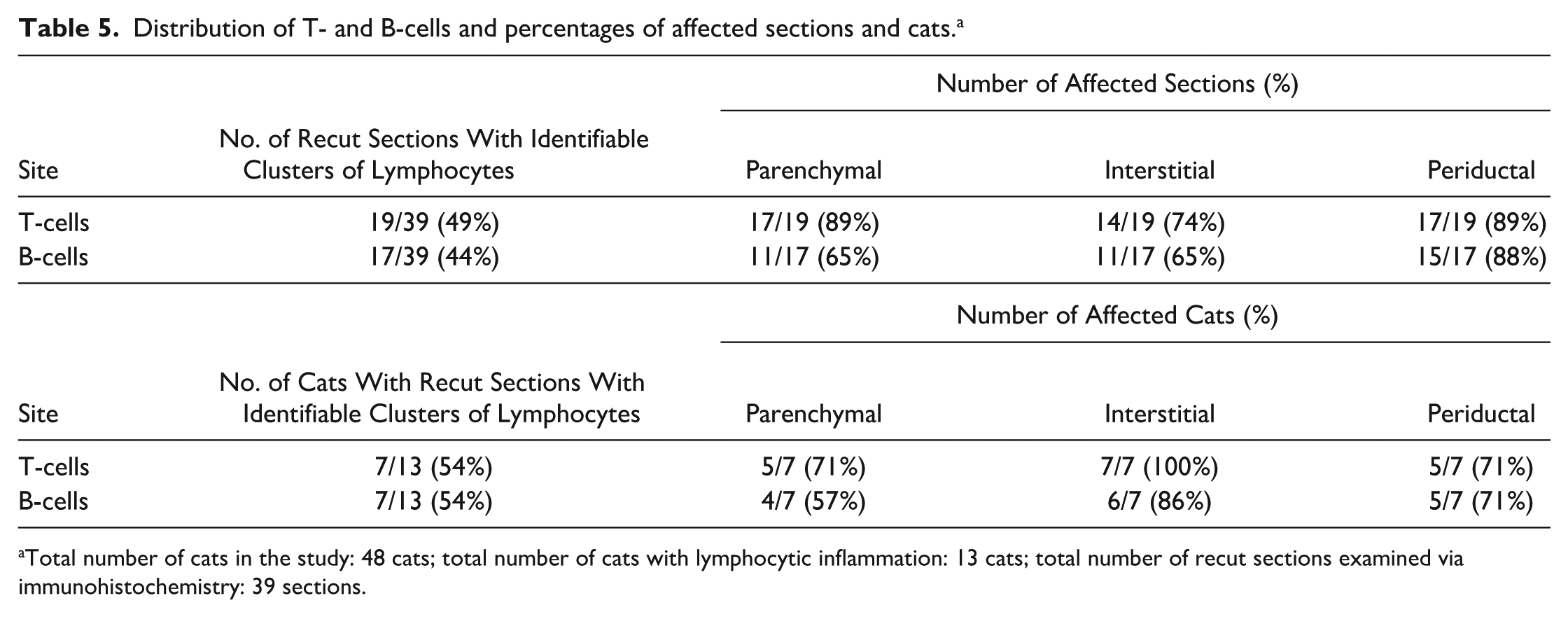
Total number of cats in the study: 48 cats; total number of cats with lymphocytic inflammation: 13 cats; total number of recut sections examined via immunohistochemistry: 39 sections.
Surprisingly, because they were not apparent on H&E-stained sections, scattered, intralobular CD3+ T-cells were commonly identified throughout the parenchyma in 33/39 (85%) sections and were distinctly different from lymphocytic clusters (Fig. 5a, b). These scattered CD3+ T-cells were more spread out in the parenchyma, with variable densities (Fig. 5a–c) and were not necessarily immediately adjacent to the clusters of lymphocytes (lymphocytic infiltrates) that were more readily identifiable on the H&E-stained slides. Scattered CD3+ T-cells were not found to be accompanied by CD20+ B-cells (Fig. 5d). CD20+ B-cells were mostly found in cluster(s) mixed with CD3+ T-cells.

Immunohistochemical features of scattered, intralobular parenchymal lymphocytes in cat pancreas. Pancreas, cat. (a) Lymphocytic clusters and scattered, intralobular, parenchymal CD3+ T-cells spreading throughout the parenchyma of the pancreas. Scattered CD3+ T-cells are present in areas that were not in close proximity to lymphocytic clusters. CD3 immunohistochemistry (IHC). Case 8. (b) Section with smaller lymphocytic clusters. Scattered CD3+ T-cells can be seen in areas without lymphocytic clusters. CD3 IHC. Case 8. (c) Scattered CD3+ T-cells spread throughout the parenchyma without close lymphocytic clusters. CD3 IHC. Case 8. (d) CD20 IHC of the same section as (c) demonstrating that scattered CD3+ T-cells were not commonly accompanied by CD20+ B-cells. CD20 IHC. Case 8.
Discussion
Our study examined serial pancreatic sections of cats euthanized for population control and aimed to characterize the changes in pancreata from said population. Importantly, this population was determined to be relatively healthy, based on ancillary testing, and thus represents a different population compared with those described in all prior studies. Those studies examined pancreatic sections from cats presented for necropsy.7,13,32 The cohort of cats evaluated in this study comprised relatively young adult cats, with a slightly low to ideal body condition, and with an even sex distribution.
Pancreatic lesions were uncommonly identified in young adult cats euthanized for population control. Lymphocytic inflammation was the most frequently identified lesion in this cohort of cats (13/48 cats, 27%), with a score of 1 on all of their respective affected sections. The median percentage of affected serial pancreatic sections was 14%, and approximately 50% of recut sections had identifiable lymphocytic clusters that were available for CD3 or CD20 IHC assessment, suggesting multifocal localized lesions. Given the lack of consistency across sections and between cats, these findings suggest that mild parenchymal lymphocytic clusters might not represent a normal response to antigenic stimulation as hypothesized by some previous studies.3,32 It remains to be determined whether these infiltrates represent bystander inflammation, or a primary pathological change associated with pancreatitis. If it is associated with pancreatitis, it would also be important to determine whether lymphocytic infiltrates reflect de novo CP when there is no histologic evidence of concurrent AP.
The score 0 for lymphocytic inflammation was defined as either none, isolated lymphocytes, or erratic small nests of lymphocytes.13,15 A prior study defined lymphocytic inflammation affecting <10% of a section to be normal as part of the analyses,24,32 while others suggested that such values should be given more credence. 16 A clearer definition of the expected number of lymphocytes, and what represents “small nests” is needed to reduce ambiguity in interpretation of future studies.
Frequently seen biochemistry abnormalities in this cohort of cats such as elevated aspartate aminotransferase activities, hyperphosphatemia, and hyperkalemia were thought to be a result of hemolysis that occurred during blood draw, from autolysis if postmortem blood was used, or from delayed sample separation. Hypoalbuminemia was the most common altered blood parameter; malnutrition was thought be the predominant cause, as liver values, kidney values, and GI panel results were relatively normal. Nonetheless, liver disease, kidney disease, and GI disease could not be ruled out due to lack of histologic examination of these organs. No differences in biochemistry or GI panel results were seen between cats with or without pancreatic lymphocytic infiltrates. These results may suggest that mild pancreatic lymphocytic infiltrates were a primary pathological process in this cohort, as there are no specific biochemical changes specific to pancreatitis, 15 and there is no strong evidence of other primary diseases such as concurrent biliary or GI tract disease as a possible cause. 26 Alternatively, because of the extent and distribution, localized pancreatic lymphocytic infiltrates may require finer serial sectioning to be uncovered in some of the cats, or the analysis was underpowered due to sample size. Further studies with larger sample sizes and various degrees of pancreatic lymphocytic infiltrates might be better suited to evaluate a potential association.
Despite differences between study populations, lesions considered consistent with CP were identified in this cohort, similar to past studies.7,32 The severity scores were mild for individual histological variables and also for the MCSs for each of our cats (Table 3, Supplemental Fig. S2). To explore the clinical relevance of mild pancreatic lymphocytic infiltrates, we evaluated the relationship between MCS-LI and serum fPLI concentrations. The MCS-LI was not correlated with serum fPLI concentrations (Supplemental Fig. S3a); however, the range of MCS-LI and serum fPLI concentrations were both limited by low values in this study cohort. Therefore, extrapolation of this relationship outside of the observed range needs to be interpreted cautiously. Notably, when cats had an MCS-LI of 0 or minimally above, the corresponding serum fPLI concentrations were within the reference interval. The cat with the highest MCS-LI in this study (case 8) had the highest serum fPLI concentration (5.8 μg/L, which falls within the equivocal range). A similar trend was observed with MCS-CP (Supplemental Fig. S3b): the cat (case 8) with the highest MCS-CP in this cohort had a score of 1.5, corresponding to mild CP (Table 2), and had the highest serum fPLI concentration (5.8 μg/L, which falls within the equivocal range). This finding could be in concordance with a previous study that showed serum fPLI concentration (measured with a different assay, ie, a radioimmunoassay) is a sensitive parameter in cats with moderate to severe pancreatitis, but not in cats with a mild form of the disease. 13 Future studies in cats with wider ranges of MCS-LI, MCS-CP, and serum fPLI concentrations might be better suited to evaluate any association between these parameters. Comparing MCSs of different histological variables between cats with or without pancreatitis, similarly to a past study performed in dogs, 29 could further determine whether any level of MCS-LI might have clinical significance.
In one review, it was discussed that the clinical relevance of mild lymphocytic inflammation in the absence of significant concurrent fibrosis is undetermined. 3 It is unclear if lack of concurrent fibrosis is a good way to determine the clinical relevance of mild lymphocytic inflammation/infiltrates as that review suggested. CP is a chronic fibro-inflammatory process, and lymphocytic infiltrates can drive and mediate the development of fibrosis,28,40 which could explain our findings of a positive correlation between the MCS-LI and MCS-fibrosis (Fig. 2). Fibrosis does not typically develop without a preceding inflammatory process.1,2,19 Hence, mild lymphocytic inflammation without concurrent fibrosis could represent an early, resolving, or mild form of pancreatitis. On the other hand, pancreatic fibrosis that is not associated with concurrent inflammatory infiltrates might indicate resolved previous inflammation, be a result from long standing edema, be caused by other disease processes, or even be associated with aging. 8
Most research regarding the pathophysiology of pancreatitis has been performed in experimental animal models.27,43 The etiology and pathogenesis of CP in cats is not entirely understood. While pancreatitis has been sporadically reported in cats with trauma, various infections, hypotension, and a history of some medications, >95% of pancreatitis cases in cats are considered to be idiopathic. 15 Hence, inciting trigger(s) are poorly understood. However, a pathophysiologic framework has been extrapolated and hypothesized for cats26,35,41: CP can be a result of recurrent AP or develops as a de novo process. In cats, the pancreatic duct joins the bile duct before entering the duodenum at the major duodenal papilla, 46 which is similar to humans.5,38 This anatomy may predispose cats to multiorgan inflammation, involving the pancreas, liver, and intestines, collectively termed “triadititis,”26,34,35 and hypothesized to have either a bacterial- or an immune-mediated pathogenesis. 26 Although hepatic and intestinal comorbidities can occur in humans with CP, 6 a multiorgan fibro-inflammatory disorder is more common for a distinct etiology/subtype of CP, type 1 autoimmune pancreatitis. 25
In humans, the pathological importance of pancreatic lymphocytic infiltrates has been questioned in the past and then overturned by multiple studies supporting the involvement of immune cells in the pathogenesis of pancreatitis.9,10,17,39 It has been previously reported that major histocompatibility complex class II-deficient mice spontaneously developed exocrine pancreatic damage comparable to that seen in humans with CP. 39 The IHC results demonstrated a predominant intrapancreatic infiltration with CD8+ T-cells. Transfer of these T-cell subsets into nude mice resulted in the same changes, indicating that CD8+ T-lymphocyte subsets were responsible for the induction of the pathological process in this animal model of CP. 39 These findings shifted the paradigm; cellular infiltrates were regarded as merely an epiphenomenon of other primary pathological changes in the pancreas to having primary pathophysiological importance in human patients. 17 Recent findings confirm that immunologic processes are of primary pathophysiological importance in several pancreatic diseases in humans, including autoimmune pancreatitis and pancreatic cancer; the nature and role of these infiltrates, however, vary significantly depending on the specific disease context. 47 Similar studies have not yet been performed in cats with pancreatitis. The results of a clinical trial in cats with presumed CP demonstrated a reduction in serum fPLI concentration following cyclosporine treatment, 44 indicating that T-cells could play a role in mediating pancreatic inflammation in cats. However, the specific cell types and their role require further elucidation.
Of 12 cats with nodular hyperplasia, 4 cats (33%) had lymphocytic infiltrates, concurrently identified on the same slide; 3 of which had observable lymphocytic infiltrates surrounding or within the nodular hyperplastic focus. Although nodular hyperplasia is more commonly identified in older cats and regarded as a benign, noncancerous condition, 22 it was also identified in this cohort. It was unexpectedly associated with lymphocytic infiltrates, thus requiring consideration of a potential role in the pathophysiology in this cohort. Nodular hyperplasia is also a common lesion in dogs and shows a positive correlation with age, regardless of the presence or absence of pancreatic inflammation, necrosis, or fibrosis. 30 A similar study in cats may inform whether nodular hyperplasia indicates antecedent inflammation or regenerative nodular tissue response, and whether there is a correlation with age.
Histopathology is regarded as the gold standard to diagnose CP in cats. 15 Necropsy samples more easily allow for this. However, a clinical diagnosis of CP is not straightforward in all cats; a consensus has not been reached for the clinical diagnosis of CP in cats. Often there is a discrepancy between research studies and clinical diagnoses due to disparate diagnostic criteria.14,44 Similar challenges exist in diagnosing CP in humans where histopathology is not regarded as the gold standard, and it is recommended that pathologists consider clinical history and radiological features in making the diagnosis of CP. 11 Imaging modalities, such as computed tomography or magnetic resonance imaging, are recommended as first-line diagnostics in human patients, and histological examination is recommended when the clinical and functional evidence of CP is strong, but imaging modalities are inconclusive. 18 Risk factors are not well understood for pancreatitis in cats and clinical presentations are often variable, 15 but similar diagnostic algorithms as are used for humans might be useful in cats. Many believe that pancreatic histology should be reserved as the last resort, given the invasive nature of sample collection and difficulty interpreting a normal pancreatic biopsy result. 33 An establishment of clinical diagnostic criteria and when and how to integrate histopathology findings is thus warranted. 15
IHC has not yet been incorporated into the routine histological examination of the feline pancreas, 15 but has the potential to inform pathophysiology as a research tool. About 50% of the recut sections in our study had infiltrates of either T- or B-lymphocytes, suggesting that these lesions were highly localized. As an attempt to characterize the immunophenotype, we performed CD3 and CD20 IHC. There were no obvious differences in percentages of T- or B-cells comprising the lymphocytic clusters across sections. Most cats had evenly mixed clusters (Fig. 3a, b), while one cat had a follicle-like structure (Fig. 3c, d). Whether these follicle-like structures represent lymphoid neogenesis, 23 or are similar to follicular pancreatitis in humans, 20 requires further investigation.
In addition, we evaluated the presence or absence of lymphocytic infiltrates in the parenchyma, interstitium, and/or around the pancreatic ducts, in an attempt to infer possible physiological or pathological roles of the identified lymphocytic infiltrates in this cohort. There were no obvious specific spatial distributions for either T- or B-cells, nor were there obvious differences between the 2 cell types in our cohort of cats. Both T- and B-cells were commonly present at all these locations. Of note, in this study, we only recorded the presence or absence of the lymphocytes at a given tissue location. The quantity/density of lymphocytes and perhaps further subtyping (CD4/CD8) of lymphocytes, as has been reported in some human studies, will need to be further evaluated to provide more comprehensive insights during future studies. Ultimately, a combination of quantitative, qualitative, and spatial analyses would provide a more comprehensive understanding of lymphocytic infiltrates and their role in the development of pancreatitis in cats.
Scattered variably dense CD3+ T-cells were unexpected by the pathologist but were commonly identified throughout the parenchyma in 33/39 (85%) sections. The scattered CD3+ T-cells were distinct from clusters of lymphocytes and were likely missed historically on H&E-stained slides, as they would appear as a small nucleus only. This pattern was not a feature for CD20+ B-cells, even for cats with multiple sections affected by lymphocytic infiltration. The scattered CD3+ T-cells need to be further characterized phenotypically, functionally, and transcriptionally to understand their role, if any, in pancreatic pathophysiology. It is unknown whether these cells represent recirculating or tissue-resident lymphocytes. 12 Bedossa et al 4 analyzed normal and CP tissue from humans using IHC. They found that normal human pancreatic tissue contained very few lymphocytes, but when present, were almost exclusively T-cells. These were found in the epithelium and in the connective tissue surrounding the pancreatic duct. The presence of scattered, intralobular, parenchymal CD3+ T-cells was not described in that study. 4 Another study identified T-cells that were largely restricted to the periductal and acinar areas of the exocrine pancreas in nondiseased pancreata from organ donors. 42 The role of scattered CD3+ T-cells in the pancreas of cats in our study requires further elucidation.
Pancreatic lesions are often multifocal in cats, which makes pancreatic biopsies less informative, unless gross lesions can direct sampling or there is diffuse disease. As a result, several research studies have adopted serial pancreatic sectioning for evaluation.7,32 However, scoring systems for pancreatic histopathology are designed for a single section, such as the one developed in the consensus statement that was used as a basis for this study. 15 The use of MCS helps to summarize both the severity and extent of the lesions when whole pancreatic tissue is evaluated. Disease activity index31,32 and disease chronicity index 31 derived from MCS have been used in past research studies to represent disease process and severity. Evaluation of association between disease activity/chronicity index, serum fPLI concentration, and clinical activity index 44 may provide further insight into clinical relevance of histologic changes of the pancreas in cats.
This study had several additional limitations. We aimed to include cases that could represent a young adult healthy population, but limited medical records were available, as the cats enrolled were all shelter animals with an unknown history. In addition, physical examination and complete blood counts were not readily available in the shelter setting, nor were full necropsies performed. Some of the histological findings might reflect undiagnosed conditions rather than physiological changes. In addition, cats in this study were mostly young adults, so results might not be relevant to older populations. Blood samples were taken either under sedation or immediately postmortem; the effect of this sampling timing is unknown but is expected to be minimal. For CD3/CD20 IHC, an isotype antibody control was not used, but the specificity of the CD3/CD20 assays was ensured by evaluation of areas of pancreatic parenchyma without lymphocytic infiltration (negative tissue control). Percentages of the T- or B-cells within clusters were estimated and were not based on manual count or automated methods. In this cohort, lymphocytic clusters were small and could have been missed, even with consecutive slides made from each block. Distribution of the lymphocytic infiltrates were recorded on CD3 and CD20 IHC slides in a qualitative manner (presence/absence basis). Compartment-specific counts would be needed to make further inferences.
This study demonstrated that lymphocytic infiltration was uncommon in H&E-stained slides of pancreatic tissue from young adult cats euthanized for population control. When present, only a small percentage of serial pancreatic sections were affected by mild lymphocytic infiltrates that trended with serum fPLI concentration and fibrosis. This may indicate that mild lymphocytic infiltration is not a physiological response, but whether mild lymphocytic infiltrates are indicative of silent bystander injury, or a primary response associated with pancreatitis, still needs to be further evaluated. This may rely on integration of other clinical information, such as clinical signs, clinical pathology, imaging evidence, and other histologic parameters of pancreatitis. Future longitudinal studies and case-control studies are needed to elucidate the role of lymphocytes in the pathogenesis of feline pancreatitis.
Supplemental Material
sj-pdf-1-vet-10.1177_03009858261451483 – Supplemental material for Serial examination of the pancreas from shelter cats euthanized for population control for the prevalence of histologic and immunohistochemical changes
Supplemental material, sj-pdf-1-vet-10.1177_03009858261451483 for Serial examination of the pancreas from shelter cats euthanized for population control for the prevalence of histologic and immunohistochemical changes by Yu-An Wu, Shelley J. Newman, Jonathan A. Lidbury and Joerg M. Steiner in Veterinary Pathology
Footnotes
Acknowledgements
We greatly thank staff members of the Animal Control Facility, which, however, would like to stay anonymous; Ms Kelly Mallett for her help with histopathology logistics; and Dr Adrian Tinoco Najera for his help with sample collection. Part of the results were presented at the 2022 American College of Veterinary Internal Medicine (ACVIM) Forum in Austin, TX and the 2023 ACVIM Forum in Philadelphia, Pennsylvania.
Supplemental material for this article is available online.
Author Contributions
YW performed the necropsy, sample collection, and histologic preparation; SJN performed histologic evaluations; and the manuscript was written by YW with contribution from all other authors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Drs Wu, Newman, Lidbury, and Steiner are affiliated with the Gastrointestinal Laboratory at Texas A&M University, which offers laboratory testing on a fee-for-service basis. Dr Newman is the owner of Newman Specialty VetPath and provides various services, including histopathology diagnostics on a fee-for-service basis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.