
Abstract
Ankole-Watusi cattle, Bos taurus ankole, have a unique wide-based horn structure with a large communication to the frontal sinus compared to other cattle breeds. A total of 6 cases of cornual sinusitis presented at the Toronto Zoo and Disney’s Animal Kingdom Lodge® and Disney’s Animal Kingdom® Theme Park with a head tilt. Clinically, 4 of the 6 cases had concurrent otitis at the time of initial clinical observation. Medical management was the standard across all cases with limited surgical success in 2 cases. Due to intractable and progressive clinical signs despite treatment attempts, euthanasia and postmortem examinations were performed. All animals had gross and histologic evidence of cornual sinusitis with massive mucoid exudate in either 1 or both horns. Fluid accumulation and sinusitis within the cornual sinus should be considered a differential diagnosis in Ankole-Watusi cattle with a head tilt.
From Africa, Ankole-Watusi (AW) cattle, Bos taurus ankole, are common in zoological institutions.8,9 Like other Ankole cattle, they feature unique, massive wide-based horns. 5 The expanded cornual process and diverticulum are extensions of the frontal bone and sinus and occupy nearly all of the outer horn. 10 This creates a dramatically larger communication with the main frontal sinus compared to domestic cattle (Supplemental Fig. S1a). Like other sinuses in the skull, the cornual process contains a delicate meshwork of bony trabeculae covered in vascular mucosa with large intervening spaces (Supplemental Fig. S1b). Histologically, the sinuses are lined by ciliated, pseudostratified epithelium with abundant goblet cells (respiratory-type epithelium). In this article the term cornual sinus describes the analogous structure of the cornual diverticulum of domestic cattle in AW cattle.
Sinusitis commonly affects the frontal and less often the maxillary sinus in domestic cattle. 11 Calves are most affected as dehorning and respiratory tract infections are common and pathogens can access the frontal sinus via the cornual diverticulum or nasal cavity, respectively.11,13 Frontal sinusitis has also been reported in aged bucking bulls from horn tipping. 12 Nonspecific clinical signs commonly include tachypnea, lethargy, nasal discharge, and head tilt/abnormal head position, which could also reflect other conditions such as otitis or encephalitis.11-13 Radiographs and horn percussion are practical and useful methods to confirm sinusitis.11,12 The prognosis is generally guarded to poor, even with medical and surgical treatments.11-13 Herein, cornual sinusitis and mucoid exudate associated with a head tilt is described in 6 AW cattle from 2 zoological institutions.
This case series utilized medical records and postmortem reports of AW cattle that underwent postmortem examinations from 2004-2020 in 2 zoological institutions accredited by the Association of Zoos and Aquariums: the Toronto Zoo (institution 1; Toronto, Ontario, Canada) and Disney’s Animal Kingdom Lodge® and Disney’s Animal Kingdom® Theme Park (institution 2; Walt Disney World® Resort, Bay Lake, Florida, USA). Inclusion required a clinical history of head tilt (Supplemental Fig. S2). Case management was not standardized and was performed at the discretion of the attending veterinarians. Institution 1 had one case and institution 2 had 5 cases present with a head tilt, which were subsequently diagnosed with cornual sinusitis with mucoid exudate (Table 1). Postmortem examinations were performed by or under the supervision of a board-certified veterinary pathologist, and ancillary testing was performed at their discretion. Variable tissues were collected for histology in all cases, including the cornual sinus mucosa and/or trabecular bone in 3/6 cases.
Signalment, clinical outcome, gross and histologic findings, and ancillary test results of Ankole-Watusi cattle with cornual sinusitis with mucoid fluid accumulation.
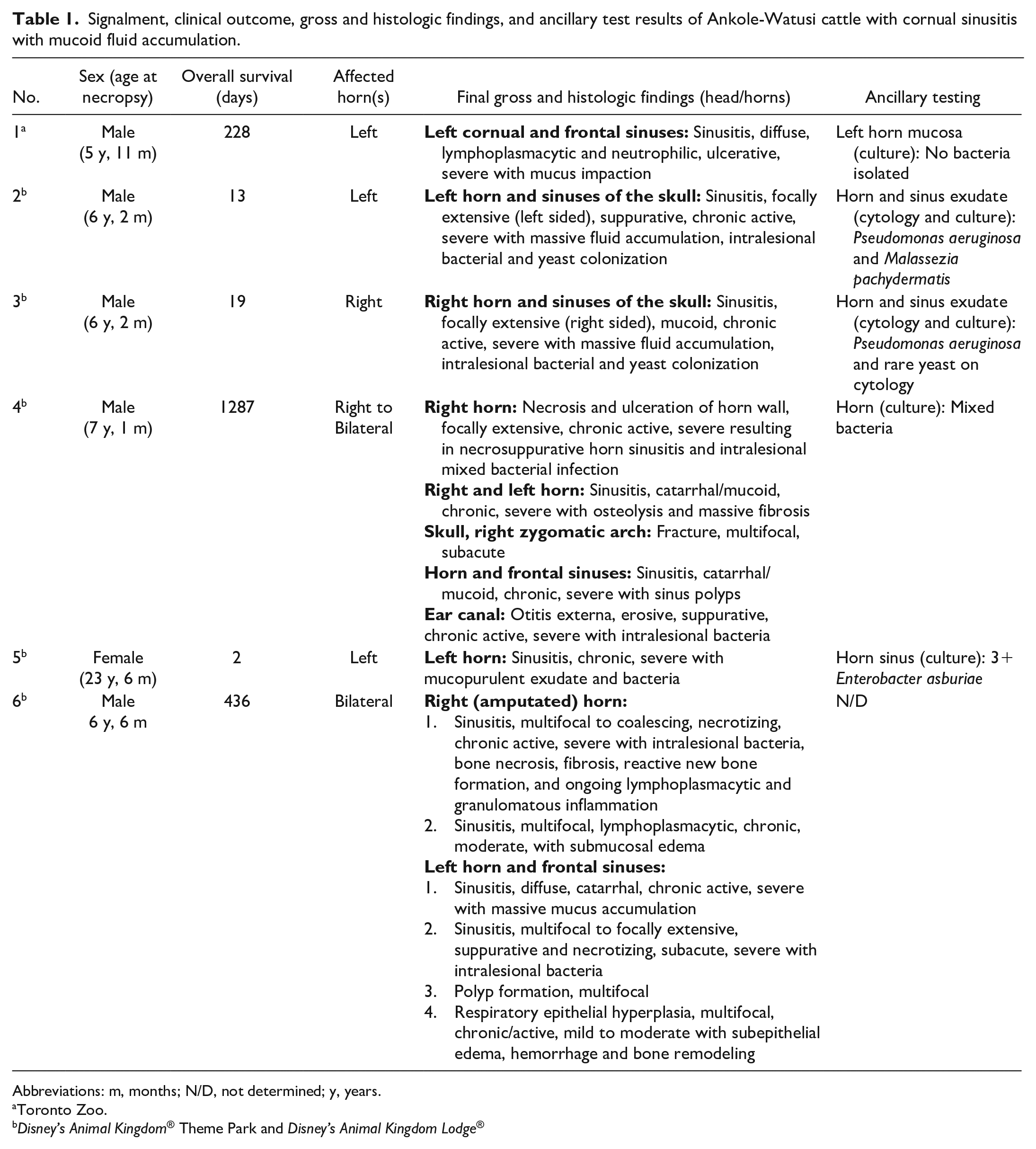
Abbreviations: m, months; N/D, not determined; y, years.
Toronto Zoo.
Disney’s Animal Kingdom® Theme Park and Disney’s Animal Kingdom Lodge®
Most cases were male (5/6) between 3 and 7 years of age and had a median time of head tilt of 123.5 days (Table 1). The head tilt was unilateral in 5/6 cases (3/5 left and 2/5 right), while it shifted from right to left following horn amputation in the remaining case (Supplemental Table S1). In most cases (5/6), the severity of the head tilt varied but was persistent and progressive. The sole female (case 5) had an acute and severe head tilt immediately after anesthesia for an unrelated condition and prior to euthanasia within 48 hours. Initial observations, physical examination findings, and ancillary test results are available in Supplemental Table S1. Confirmed or suspected otitis was the most common condition diagnosed with the first observation of a head tilt. Otitis was diagnosed concurrently with a head tilt for cases 1, 4, and 6, and preceded the head tilt in case 5. On otoscopic examination, cases 4 and 5 had no tympanic membrane on the ipsilateral side of the head tilt. Evidence suggestive of current horn trauma or a history of previous horn trauma was noted in 4/6 cases (3/4 ipsilateral and 1/4 contralateral). Cornual radiographs (anterior-posterior view) in case 1 demonstrated replacement of the air spaces by soft tissue/fluid opacity. Infrared thermography showed an increased heat signature (red) of the affected horns in 2 cases (right in case 4 and both in case 6) compared to the unaffected horn or other unaffected animals (Supplemental Fig. S3).
All chronic cases received medical management with antibiotics and analgesics representing the most common treatments (Supplemental Table S2). A mucolytic and/or corticosteroid treatment were used in 4/6 cases. Case 5 was only on a long-term custom immunotherapeutic for chronic allergic skin disease. Surgical management was attempted in cases 4 and 6. Approximately 2 years prior to euthanasia, case 4 underwent total ear canal ablation with exploration of the frontal sinus. Case 6, 1 month before euthanasia, had a custom horn drainage system implanted through the cornual and frontal sinuses. There was some degree of successful drainage, but improvement was short-lasting. Due to progressive trauma, the right horn was amputated. This resulted in the remaining horn touching the ground within 48 hours, leading to euthanasia. Clinical signs prior to euthanasia are reported in Supplemental Table S2 with the most common being progressive head tilt with a lack of response to therapy (5/6).
On postmortem examination, cornual sinusitis was reported in all cases and was ipsilateral to the head tilt in 4/6 cases (3/4 left and 1/4 right) and bilateral in 2/6 cases (Table 1). Massive, predominantly mucoid exudate within the sinus was observed with sinusitis (hyperemia and loss of bony trabeculae) (Fig. 1a, b). These lesions extended to the frontal sinus (Fig. 1c). Final postmortem and antemortem diagnoses and ancillary test results are in Table 1. Both horns were weighed in 4/6 cases, wherein the affected horn was 1.7- to 3.0-fold heavier than the unaffected horn. At necropsy, both horns from case 4 were affected with the right side weighing 3-fold more and this was the side of the clinically apparent head tilt. This case also had 2 fractures of the zygomatic arch alongside marked proliferation of spongy bone and fibrous tissue filling 80% of the cornual sinus. Case 6 was also bilaterally affected at necropsy, however only the left horn was weighed at this time as the right horn had been previously removed and the weight not recorded. In 2/5 cases, various bacteria were cultured at postmortem (Table 1). Histology of the cornual sinus (3/6 cases) revealed mucosal inflammation (sinusitis) ranging from necrosuppurative to lymphoplasmacytic and neutrophilic (Fig. 2). Submucosal edema, variable hemorrhage, osteolysis, and bone remodeling were also seen (Fig. 2). Intralesional bacterial colonies were described either by cytology (cases 2 and 3) or histology (case 4). In case 4, the lumen of the external ear canal contained neutrophils, debris, and mixed bacteria with erosion and hyperplasia of the epithelium.
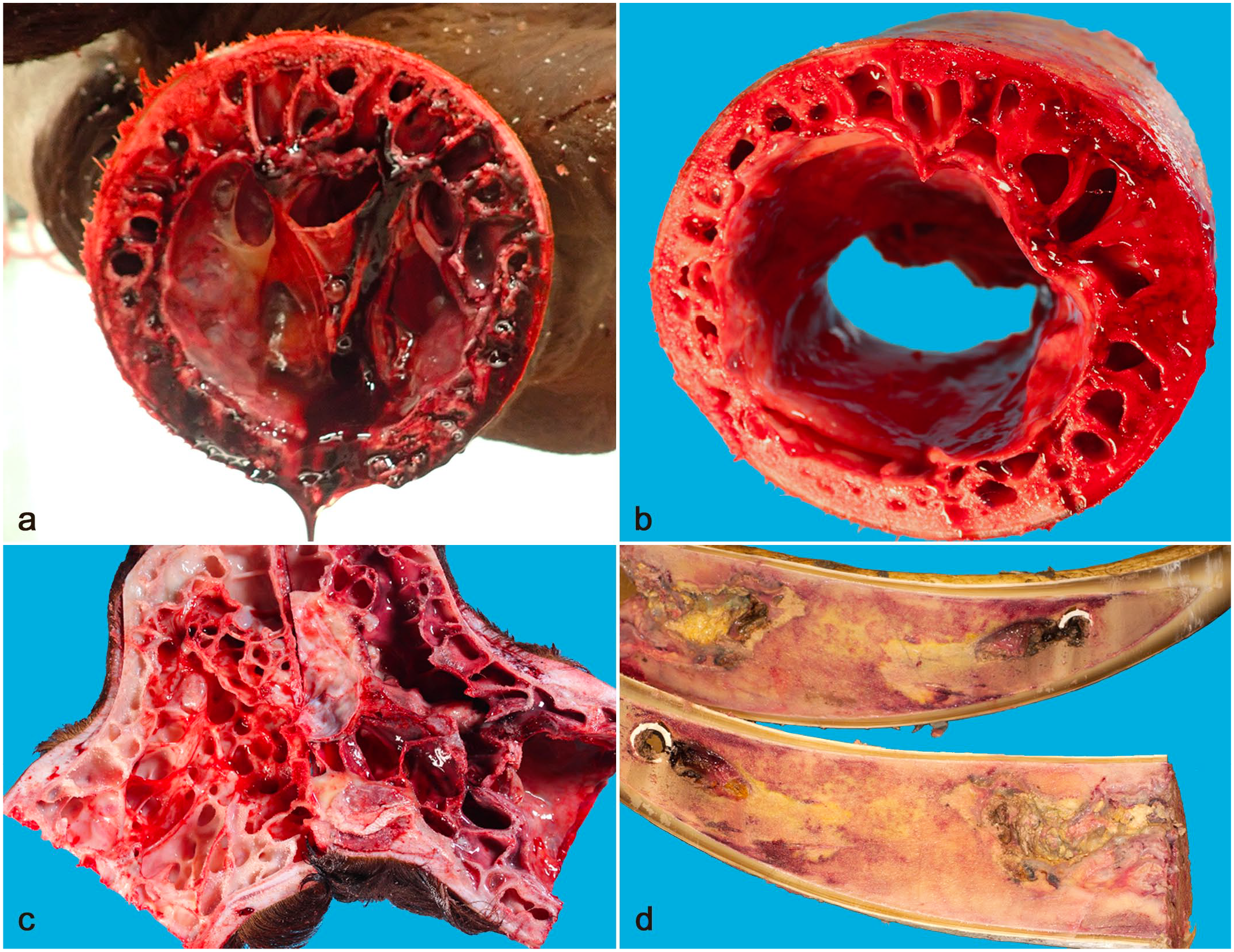
Macroscopic features of cornual and frontal sinusitis, Ankole-Watusi cattle. (a) Abundant mucoid discharge from the cornual sinus with hyperemia of the mucosa. Case 1. (b) Loss of central bony trabeculae of the cornual sinus with hyperemia of the mucosa. Case 1. (c) Loss of bony trabeculae and hyperemia of the mucosa of the affected frontal sinus (right) compared to the contralateral unaffected sinus (left). Case 1. (d) Proliferation of spongy bone and fibrous tissue with purulent material in the distal cornual sinus of the amputated right horn. A portion of the surgically-placed draining apparatus is present distally in both sections of the right horn. Case 6.
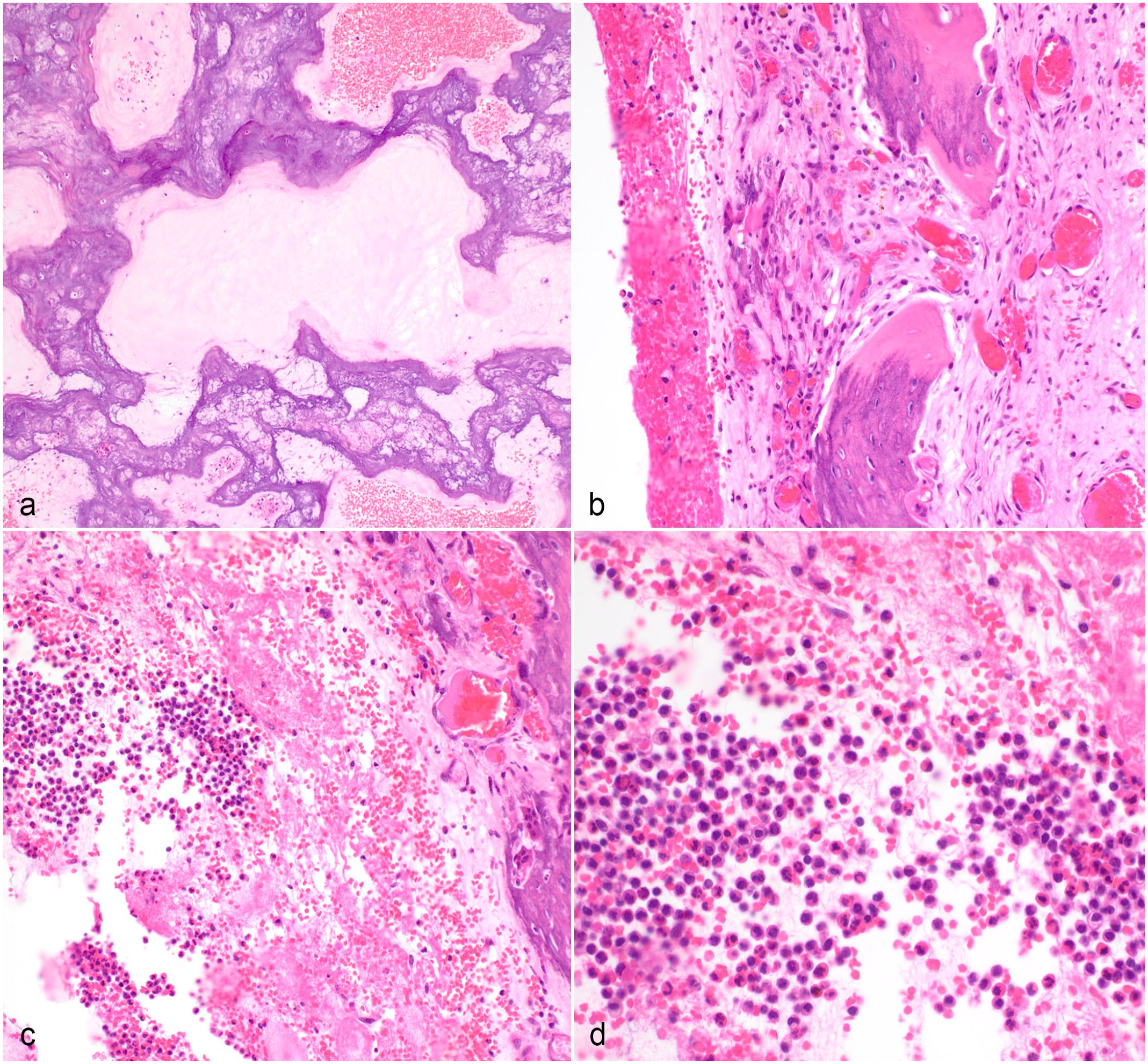
Histologic features of cornual sinusitis, Ankole-Watusi cattle. Hematoxylin and eosin. Case 1. (a) Inspissated mucus present within the cornual sinus with hemorrhage. (b) Cornual sinus mucosa with hemorrhage, congestion, ulceration, lymphocytic and plasmacytic inflammation, and bony lysis. (c) Ulcerated cornual mucosa with hemorrhage, fibrin, and neutrophils on the surface and within the sinus cavity. (d) Increased magnification of (c) within the neutrophilic exudate.
Although AW cattle are popular in zoological collections, published reports of disease are limited.2,14 Despite the frequency with which head tilt was observed in the 2 institutions, the susceptibility of this breed to cornual sinusitis is yet undocumented. Differential diagnoses for head tilt in domestic cattle are numerous. Due to nonspecific clinical signs, various antemortem diagnostics and postmortem examination were required to diagnose the cause. In 2 cases, infrared thermography was highly suggestive of inflammation in the affected horn due to an increased heat signature (Supplemental Fig. S3). This finding suggests an increased vascular flow, commonly identified with inflammation. 7 In humans, thermography may be more sensitive at diagnosing inflammation of the sinuses than radiographs. 4 Further investigation is warranted to evaluate this tool in detection of cornual sinusitis in cattle. In the current report, the mucoid exudate within the cornual sinuses resulting in unbalanced weight was suspected to be a significant contributor in the persistent head tilt, but whether it represented the main determining factor could not be established.
A head tilt can also result from otitis media/interna and neuritis of the vestibulocochlear nerve.1,10,15 Otitis externa was present in 4/6 cases, and cases 4 and 5 had no tympanic membrane on the ipsilateral side of the head tilt, suggesting a likely involvement of the middle ear, as commonly described in dogs. 15 On the other hand, otitis media can also result from ascension or hematogenous spread as in calves with Mycoplasma bovis pneumonia.1,6 Alternatively, otitis may have initiated the head tilt and subsequent postural change could have impaired the clearance of the cornual sinus exacerbating the process. The middle/inner ears were not examined histologically, so we cannot determine whether otitis media played a causative role in our cases, but it remains a possibility. No consistent cause of otitis externa was noted in these cases and suspected causes included yeasts, ear mites, and allergic dermatitis. Although dehorning and horn tipping are common causes of sinusitis in domestic cattle, only 2/6 cases had lesions suggestive, but nonconfirmatory, of trauma.11-13 Hence, trauma can be an initiating event for sinusitis but it is not consistent in AW cattle.
African subpopulations of AW cattle exhibit genetic and morphologic diversity.3,9 A variation in the angle to which the horns sit in relation to their skull varies among these subpopulations.5,9 Traditionally, a selection was made for large and upwardly curved horns, which is reflected in the morphometric measurements of the horns and skull.5,9 In the current report, the authors hypothesize that a horizontal horn conformation (Supplemental Fig. S2) could predispose to poor drainage of the cornual sinus, resulting in fluid accumulation. Additionally, all chronic cases were male, which could reflect differing horn conformations and/or behavior between sexes. Further investigation is required to determine whether North American selection standards differ from those in Africa and whether both populations experience the same incidence of mucoid exudate and cornual sinusitis.
Case 5 was unique as the cow had a chronic history of allergic skin disease, otitis, and rhinitis with an acute (<48 hour) presentation of the head tilt. We cannot determine whether otitis and an initial head tilt with poor drainage or a respiratory infection initiated the sinusitis. The unique presentation of this case along with the hypotheses discussed above further support the likely multifactorial nature of this clinical manifestation.
Herein, we described 6 cases of AW cattle with cornual sinusitis and massive mucoid exudate presenting as a head tilt. All cases eventually resulted in euthanasia due to progressive and intractable disease. Based on the clinical evidence, this condition is hypothesized to be multifactorial and further investigation is required. No treatment has proven superior in the management of these cases, although surgical amputation of the affected horn is not recommended due to the weight of the remaining horn. A case-control study would be beneficial in further understanding the pathogenesis and developing care options.
Supplemental Material
sj-pdf-1-vet-10.1177_03009858241295396 – Supplemental material for Head tilt in 6 Ankole-Watusi cattle (Bos taurus ankole) with chronic exudative cornual sinusitis
Supplemental material, sj-pdf-1-vet-10.1177_03009858241295396 for Head tilt in 6 Ankole-Watusi cattle (Bos taurus ankole) with chronic exudative cornual sinusitis by Latasha Ludwig, Emily Rätsep, Deidre Fontenot, Kenneth J. Conley, Carlos E. Rodriguez and Cédric B. Larouche in Veterinary Pathology
Footnotes
Acknowledgements
The authors acknowledge Geoffrey A. Wood and Brandon N. Lillie at the University of Guelph for their support in this collaboration, as well as all the Toronto Zoo and Disney’s Animal Kingdom® Theme Park and Disney’s Animal Kingdom Lodge® staff involved in the care of these cases, including pathology, technical, keeping, and veterinary personnel. Additional acknowledgements provided to Sarah Donato for assistance in accessing the Ontario Veterinary College’s Anatomical Reference Collection.
Author Contributions
All authors contributed in either clinical management and/or pathologic (gross and histologic) evaluation of cases for their respective institutions; LL, ER, CBL, and DF contributed to the experimental design and collection of records; LL performed retrospective review of the records and statistical analysis; the manuscript was written by LL, ER, and CBL with contributions from the other authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.