
Abstract

The Veterinary Cancer Guidelines and Protocols (VCGP) group is composed of individuals from different disciplines involved in cancer research from around the world. Their mission is to improve the care of animals with cancer through standardization of tumor evaluation. To achieve this goal, they have created resources, including guidelines and protocols (available at vcgp.org), that will facilitate uniformity in cancer studies and enable accruement of large data sets, which can be compared across laboratories and permit assessment of larger patient cohorts for more robust analysis.
The VCGP group recently created a document that provides guidelines for developing, reporting, and validating histologic tumor grading systems 2 on primary tumors, and we want to bring this to the attention of those interested in veterinary oncology. The document covers a wide spectrum of related issues and was co-authored by 20 individuals with various areas of expertise, including anatomic and clinical pathology, oncology, surgery, epidemiology, and statistics. The following is an overview of the major points, which are simplified and depicted in Fig. 1, and readers are encouraged to consult the full document for details and additional concepts. 2 A similar document covering guidelines for cytologic grading systems is planned, and colleagues interested in contributing are encouraged to contact any of the VCGP board members.
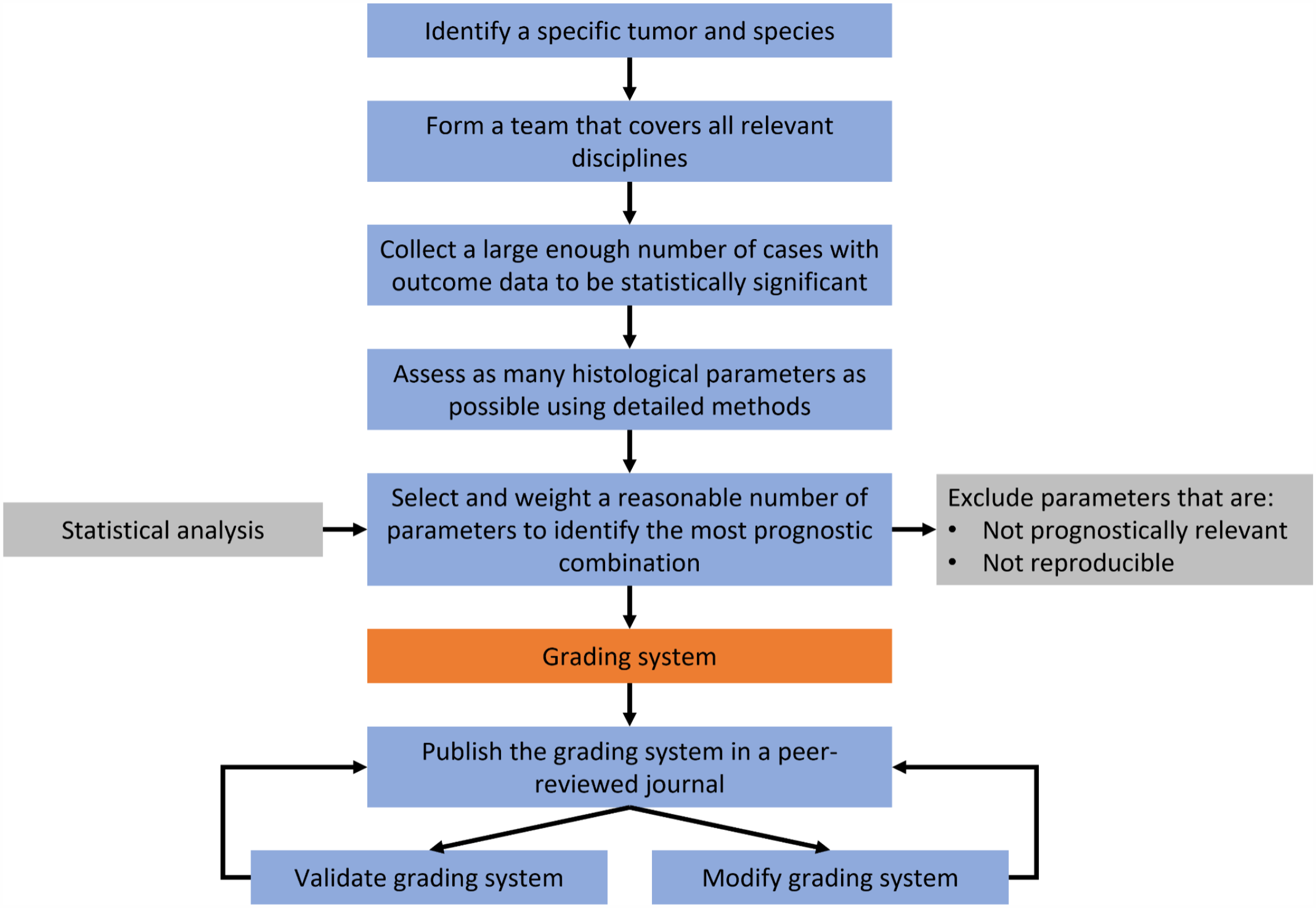
Workflow algorithm for developing a histologic grading system.
A histologic tumor grading system is a system that provides probabilities for clinical outcomes, such as recurrence, metastases, and survival metrics, based on defined microscopic features. 1 The purpose of a grading system is to subdivide a potentially aggressive type of cancer into categories that correlate with clinical outcomes. Tumor grade can be a critical factor, when integrated with other factors, in helping the clinician/oncologist/surgeon assess the prognosis and direct patient treatment.
Grading systems should be established for and applied to 1 tumor type in 1 species and should not be applied broadly across different species. They should be simple to apply, reproducible, unambiguous and accurately segregate tumors with different behaviors.
Desirable characteristics of any grading system include 3 Rs:
Reproducibility within and across observers and laboratories;
Relevance to prognosis (predicting 1 or more clinical outcomes); and
Realism in terms of applicability in a routine diagnostic setting.
The development of new grading systems requires participation of primary care veterinarians, oncologists, radiologists, pathologists, surgeons, epidemiologists, and statisticians. For grading systems to be clinically useful, it is imperative to apply appropriate statistical assessment to study results, which are based on standardized tumor parameters correlated with standardized outcomes. Standardized clinical outcomes, including histologically confirmed recurrence and metastasis, disease-free intervals, and survival metrics (separated as to euthanasia induced, tumor related, and/or non-tumor related), should be collected. If possible, these data should be collected in a prospective and well-planned manner on as many cases as possible, in which the patients have the same tumor type. Histologic grading systems should use standardized parameters that can be identified during initial histologic evaluation. Studies should assess as many histologic parameters as possible to identify those that predict specific outcomes with the most accuracy. Then, the minimum number of those parameters that, individually or in combination, provide maximal prognostic accuracy should be used in the histologic grading system.
Criteria to determine tumor grades must be sufficiently detailed to ensure others can reproducibly categorize tumors into the grades indicated in the published system. Criteria that are poorly reproducible or are not predictive should not be included in the grading system but should be reported in the peer-reviewed publication so colleagues are aware of those findings. Ideally, the criteria for grading should be unambiguous and easy to recognize and assess.
The new VCGP grading document is limited to histologic features that do not require extensive infrastructure or expertise. Comparison of histologic grade with results from other assays, such as immunohistochemical procedures, in situ hybridization, imaging, cytology, molecular tests, genetic profiles, and flow cytometry, and the standardization of these tests is strongly encouraged. They may prove beneficial to future prognostic or predictive algorithms. Understanding the prognostic value of individual or combinations of tests, and their ability to inform treatment decisions, can be helpful in completing the cost-benefit analysis of the diagnostic work-up. Some owners may not elect testing beyond routine histology and others may choose ancillary tests. This is a reality of veterinary care, and therefore, histologic grading systems that can be performed on routine biopsy submissions fit well with the present philosophy of “spectrum of care.”
All proposed grading systems should be published in a peer-reviewed journal and include details regarding study design, methods, data, and outcomes. The published information must be sufficient to permit other investigators to replicate and validate the findings in new investigations. The publication should include comparison of standardized clinical outcomes, such as disease-free interval, survival or mortality, metastasis, and/or recurrence, between the proposed grading system and existing grading systems. All relevant statistics should be reported. Grading systems or prognostic markers should be evaluated using measures of diagnostic accuracy, such as sensitivity, specificity, survival rate, and receiver operating characteristic (ROC) curves, to determine their diagnostic validity and clinical utility. P-values and statistical significance, which deal with population averages but do not offer insights about the clinical relevance for the individual, are not appropriate.3,4
Study populations may be biased in terms of case selection, including factors such as primary versus secondary versus tertiary care centers, initial therapies, “rescue” therapies, outcome data, retrospective design, and influence of euthanasia. There may also be assessment variation between pathologists. Therefore, the reported prognostic value of the resultant grading system may not be applicable in a different population of pets or for different pathologists. Validation studies should be conducted before implementation of the system on clinical cases. The grading system can be validated by different pathologists in the same demographic population and/or in new populations by precisely following the materials and methods reported by the initial investigators to determine if association between the defined parameter scores and grades and clinical outcomes can be reproduced. The original investigators can provide the complete data sets to an independent group of investigators that repeats the study using the same materials and methods. This approach is a new paradigm in veterinary oncology, and although not as robust as new studies, it should be easier and faster to complete.
The authors and VCGP group welcome feedback on the histologic grading document; please contact any of the authors or a member of the VCGP board (https://vcgp.org/contributors) to provide input.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.