
Abstract

Pulmonary hypertension (PH) in both humans and animals remains an enigmatic problem. PH in all species can occur idiopathically or can be associated with a wide variety of disease conditions. As such, PH has been grouped into various classes and most recently into 5 distinct categories at the 2013 World Congress on Pulmonary Hypertension in Nice. 16 All forms of chronic PH involve pulmonary vascular remodeling that can be characterized by a predominance of pulmonary arterial remodeling, vein remodeling, or a variable contribution of both. 18 In idiopathic pulmonary arterial hypertension (iPAH), the pulmonary vascular remodeling affects largely the precapillary arteries; on the other hand, in venous PH, including pulmonary veno-occlusive disease (PVOD) and PH due to left heart dysfunction, venous remodeling predominates but is often accompanied by pulmonary arterial changes. In fact, these can be pronounced, to an extent exceeding that seen in precapillary PH. Importantly, it is increasingly appreciated that most forms of PH, including those caused by hypoxia, interstitial lung disease, thromboembolism, and connective tissue diseases, may involve both arterial and venous remodeling. 13,14,17,18 Unfortunately, in humans and animals, precise descriptions and documentation of pulmonary vein remodeling are still lacking in most of these conditions, and in animals, there have been no reports of PVOD causing severe PH and death.
In this issue of the journal, Williams et al 19 provide what appears to be the first description of a condition in adult dogs that shares many of the pathologic and clinical features of PVOD that are observed in humans. There were significant consistencies in these dogs with the human condition with regard to clinical presentation, radiologic findings, and lung pathology. 13,14 Similar to humans with PVOD, almost all of the affected dogs presented with dyspnea, exercise limitation, fatigue, and syncope. The dogs reported in these studies all exhibited respiratory distress in the context of what was ultimately shown to be severe pulmonary arterial hypertension (PAH). Also, similar to humans, progressive worsening of clinical signs was observed. PVOD can manifest acutely, and presentation with sudden death has been described as is the case with dogs. 8 Again, similar to humans, it is difficult to distinguish PVOD from PAH on clinical grounds alone since the clinical signs, as in humans, can be similar if not identical. Therefore, other studies need to be done to confirm the diagnosis. Echocardiography, which is always performed in human patients presenting with these findings, demonstrated evidence for increased pulmonary artery pressure as estimated by the velocity of the resurgent jet of flow through the tricuspid valve. 13 It should of course be mentioned that in humans, false positives using this approach are common, and a formal diagnosis of PH requires confirmation by right heart catheterization, although this is probably not possible to perform routinely in animals. 4 Radiologic studies are also helpful in establishing the diagnosis of PVOD. In humans, PVOD is suspected based on radiologic findings showing a combination of pulmonary artery enlargement, features of postcapillary congestion, and a normal-size left atrium. 14 Septal Kerley B-lines in a subplural distribution, interstitial edema, and plural effusions are the principal plain chest radiographic clues to a postcapillary location of vascular obstruction. A diffuse alveolar pulmonary edema pattern is an additional important finding. These findings again seem to be largely recapitulated in dogs presenting with PVOD and PH.
PVOD is a fibrotic disease process that predominately involves venules, small veins, and the veins in interlobular septa (ie, invaginations of pleural connective tissue demarcating up to 20 primary lobules of alveolar tissue), usually with relative sparing of the large veins of the hilum. 13,17 The walls of affected small pulmonary veins show variable occlusive intima lesions and media thickening as a result of a disorganized smooth muscle hypertrophy and collagen matrix deposition (Fig. 1). These changes result in luminal narrowing, with eventual complete occlusion due to recent, or most frequently, intraluminal-organized thrombosis. The partial or complete occlusion of the intima, once diagnosed with an elastic stain (which highlights the intima basal lamina), is diagnostic of veno-occlusive disease. The lung may be involved in a patchy or diffuse pattern. The fibrotic intimal proliferative changes and postcapillary obstruction in PVOD can lead to capillary angioectasia and even to capillary angioproliferation, lesions that are typically seen in classic pulmonary capillary hemangiomatosis (PCH). 14 In fact, it has been reported that PCH-like angioproliferative lesions are found in most patients with PVOD, and conversely arterial and venular lesions are also common in PCH. 8 It is again important to note that the clinical and radiologic features are similar in both conditions. These observations have led to the speculation that PVOD and PCH may in fact represent 2 variances of the same disease. 10 The extensive pathologic studies in the dogs described in this study are very consistent with the human PVOD/PCH spectrum of disease (Fig. 1). It is also important to note, as was found in the dogs, that although the predominant lesions in PVOD are found in the pulmonary veins and venules, both the arterial and capillary components of the pulmonary vasculature are often concomitantly involved. Pulmonary arteries in patients with PVOD often show medial hypertrophy and eccentric intimal fibrosis, key histologic characteristics that are shared with PAH. Interestingly, no plexiform lesions, which are often abundant in the lungs of patients with PAH, are seen in those with PVOD. Again, this is true in dogs.
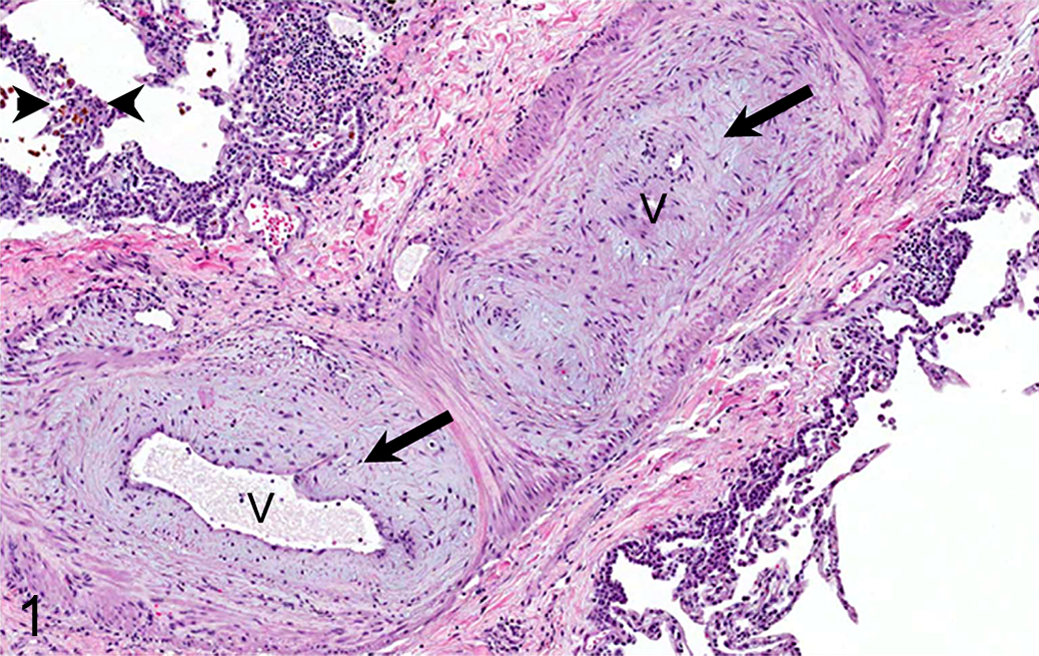
Pulmonary veno-occlusive disease (PVOD), lung, human. Known causes of PVOD include mutations in EIF2AK4, reduced pulmonary vascular EGR/apelin signaling, and chemotherapy agents. However, most human cases are idiopathic. Shown is a classic example of human PVOD with luminal ingrowth of connective tissue (arrows) in a pulmonary vein (V); arrowhead shows an organized thrombus.
Unfortunately, study of pulmonary veins in the setting of lung or cardiac disease has been significantly limited by the difficulty of their reliable identification through histological, anatomic, or molecular means. Recently, the ephrin B4 receptor (EphB4), a developmental venous marker, has been shown to identify pulmonary veins in adult mice. 2 However, this finding is probably not relevant to other species as careful embryologic studies in humans have demonstrated overlap of EphB4 expression between pulmonary veins and arteries, and furthermore, EphB4 does not appear to be present in the pulmonary veins of the rat, suggesting that EphB4 may not be a marker applicable to humans or animal species other than the mouse. 5,6 To address these challenges, a study was recently undertaken to search for unique molecular markers in pulmonary veins. Using a technique termed venous backfilling, veins were identified and then, using laser capture microdissection, isolated venous RNA was obtained for identification of vein markers 6 (Fig. 2). The investigators detected urokinase plasminogen activator receptor (uPAR) expression preferentially in normal pulmonary veins of mice, rats, and human lungs. 6 In control mice, rats, and human lung tissues, uPAR expression could be detected by immunofluorescence, primarily in the media and less so in the intima, and was specific to pulmonary veins (Fig. 2d). To follow up on these observations, the investigators used an aortic banding (AOB) model in rats to mimic PH associated with left heart dysfunction and also evaluated tissues from patients with PH due to left heart disease (PH-LHD). In both the rats and humans, the investigators found that uPAR expression was elevated in pulmonary veins and was significantly associated with cell proliferation. PhosphoERK1/2 was also elevated in the pulmonary arteries and veins of AOB and PH-LHD patients, suggesting its role as a link between uPAR expression and vascular remodeling, which is consistent with the described roles of uPAR signal transduction. 9 These findings are useful to human and animal investigations as they provide an immunohistochemical marker to confirm the identity of pulmonary veins that could be of value in the diagnosis of PVOD (Fig. 2a–e). Hopefully, future studies will identify further markers specific for pulmonary veins and also other molecular signaling pathways that are specific to pulmonary veins and that may be pathophysiologically involved in the disease process.

Given the difficulty in recognizing pulmonary veins (ve) in histological sections, we have developed a technique through which they can be better identified using a backfilling approach (please refer to Hunt et al 6 for details) (a). Fluorescent-tagged solutions are perfused retrogradely via the left atrium, allowing visualization independent of location and overall structural characteristics of the pulmonary venous system. (b) The fluorescent marker (delivered via the left atrium) is colocalized with ephrin B4 receptor in mice, which is detected by immunohistochemistry for ephrin B4 (brown, arrows). (c) Rat pulmonary vein (ve) highlighted by backfilling with agarose and 1-μm fluorescent beads (blue: DAPI nuclear fluorescence). (d) Urokinase plasminogen activator (uPAR) is normally expressed in the intima and media of pulmonary veins, as highlighted in green fluorescence for smooth muscle cell actin in sham (control animals) (SMA, arrows). However, in rats with pulmonary venous hypertension due to aortic banding (AOB), uPAR is also expressed in remodeled pulmonary arteries. Immunofluorescence for SMA (green) and uPAR (red); costaining shows as yellow/orange. (e) uPAR expression is greater in normal pulmonary veins than in normal pulmonary arteries of rat lung, with increased pulmonary arterial expression after aortic banding. The asterisks represent significant difference. Reprinted with permission from the American Journal of Physiology.
The observations of significant venous changes in humans and now dogs raise questions as to the mechanisms involved in generating pulmonary venous abnormalities. Recently, a heritable form of PVOD was discovered to be due to mutations in the gene eukaryotic translation initiation factor 2 alpha kinase 4 (EIF2AK4). 3 Heritable PVOD due to EIF2AK4 mutations is transmitted in an autosomal recessive manner as opposed to the autosomal dominant manner that has been described for the heritable form of BMPR2-related PAH. Interestingly, biallelic EIF2AK4 mutations were present in perhaps approximately 20% of patients with PVOD with sporadic disease, suggesting that even patients without a family history might have a familial form of the disease. 3 However, at present, it remains unclear as to the mechanisms by which EIF2AK4 mutations induce pulmonary vascular remodeling.
Multiple case reports have reported a link between chemotherapeutic agents and radiation therapy with PVOD. 10,15 A recent detailed study of chemotherapy-induced PH from the French PH network was reviewed. 15 This study found that alkylating and alkylating-like agents represent a significant risk factor for the development of PVOD. In addition, the investigators showed that cyclophosphamide (CP), the most frequently used alkylating agent identified in their human study, was capable of inducing PH in 3 different animal models: mouse, rat, and rabbit. 15 Interestingly, in rats, the severity of PH and vascular remodeling was sex dependent, with females being more susceptible than males, as well as time and dose dependent. These studies represent the first evidence that an animal model can be created to induce and thus study mechanisms involved in PVOD. Other natural animal systems exhibit pathologic changes consistent with PVOD. In calves spontaneously developing right heart failure at an altitude (brisket disease), recent reports suggest that there is also a high incidence of pulmonary venous lesions consistent with PVOD in the context of PH and associated arterial changes. 7 Initial reports suggest that these lesions are similar to those observed in the lungs of patients with scleroderma who have PAH. Thus, various spontaneous and induced conditions of animals exhibit PVOD in the context of PH and may provide useful models to study mechanisms pertinent to human disease.
What can be done to treat or at least ameliorate the clinical signs found in animals and humans with PVOD? In humans, little is known. Most prospective studies evaluating novel targeted PAH therapies have generally excluded patients with PVOD. This is principally due to a number of published observations of severe and occasionally fatal adverse outcomes with these treatments. 11 It is speculated that treatment with PAH-specific vasodilator therapies may cause an augmentation of pulmonary arterial blood flow against the fixed resistance of occluded pulmonary venules and veins. This increased hydrostatic pressure gradient may cause vascular leak, which can progress to severe pulmonary edema. However, it should be noted that small case series have shown some success in treating carefully selected individuals with prostacyclin, bosantin, and/or sildenafil. 1,12 Therefore, at present, limited therapeutic options are available. General recommendations include limiting physical activity and avoidance of concomitant medications that can potentially aggravate PH, such as β-adrenergic receptor blockers. Warfarin anticoagulation, which is routinely used in idiopathic PAH, should be considered with caution in PVOD given the association with occult alveolar hemorrhage. Diuretics may offer some symptomatic benefit in those with right ventricular volume overload that is not controlled by dietary measures alone.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.