
Abstract
Diabetic patients are predisposed to periodontal disease as well as dental caries; however, there are contradictory reports about the possible association between dental caries and diabetes. Thus, the authors set out to determine whether diabetes affects onset of dental caries and periodontal disease and to clarify whether dental caries and periodontal disease are associated with each other in diabetic db/db mice. Oral tissue was examined from 68 male mice (diabetic db/db and nondiabetic db/+; aged 20, 30, 40, and 50 weeks) and 20 female mice (db/db and db/+; aged 50 weeks). Macroscopically, caries were seen developing in the diabetic mice by 20 weeks of age. The number of teeth with dental lesions increased with age in the db/db mice at a significantly higher incidence than that of db/+ mice. Histologically, dental caries were detected in 30 of 120 molars in 17 of 20 db/db mice at 50 weeks of age and in 4 of 108 molars in 4 of 18 db/+ mice of the same age. The severity of dental caries in db/db mice was significantly higher than it was in db/+ mice. Dental caries were a primary change that led to bacterial gingivitis and pulpitis. These lesions spread to the dental root and periodontal connective tissue through the apical foramen. Apical periodontitis was more frequent and severe when occurring in close association with dental caries. In conclusion, there is a strong relationship between diabetes and dental caries, but in this model, it is highly probable that the onset of periodontal disease was a secondary change resulting from dental caries.
Several recent studies based on clinical observations have suggested that the teeth of diabetic patients are predisposed to dental caries. 26,39,42 Other researchers, however, have detected no significant difference in caries susceptibility between diabetic and nondiabetic patients. 4,7,14,16 In experimental diabetic rodent animals, there are also contradictory reports; 2 studies reported that diabetes enhanced the incidence of dental caries, 2,12 whereas another did not. 30
Periodontal disease in humans, including gingivitis and periodontitis, is clearly associated with diabetes. Epidemiological studies have suggested that diabetes induces periodontal disease and that its progression may be affected by the systemic conditions of diabetic patients. 22 Human patients with type 2 diabetes have shown a significant increase in risk and severity of periodontal disease. 3,8,9,38,41 The effects of diabetes on periodontal disease induced by ligation and/or bacterial inoculation have been well researched in induced and spontaneous diabetic rodent models. 13,15,19,21,31
The db/db (BKS.Cg-m+/+Leprdb /J) mouse is a well-known strain favored as a model of type 2 diabetes and characterized by obese and diabetic phenotypes owing to disruption of the leptin receptor. 5 In this strain, hyperinsulinemia is apparent by 10 days of age, and blood glucose levels are slightly elevated at 1 month, with diabetes developing by 10 weeks of age, relatively earlier than other diabetic mouse strains. 20,43 Although diabetic complications have been recently investigated in db/db mice, 34,37 few reports have analyzed dental caries or periodontal disease in this strain.
The objective of this study was to determine whether diabetic conditions affect the onset of dental caries and to ascertain whether diabetes induces periodontal disease, focusing on the long duration of hyperglycemia in this strain. In addition, we tried to clarify the morphogenesis and association of the 2 types of dental lesions in this diabetic model—that is, dental caries and periodontal disease.
Materials and Methods
This study used db/db and db/+ mice, as purchased from Charles River Laboratories (Yokohama, Japan). All mice were fed a standard laboratory pelletized diet (Charles River Formula 1, Oriental Yeast, Tokyo, Osaka, Japan) and provided with tap water ad libitum. The animals were handled according to the principles outlined in the Guide for the Care and Use of Laboratory Animals prepared by our institution (Setsunan University, Osaka, Japan) for all experimental procedures.
Macroscopic Examination and Dental Lesion Grading
For the macroscopic examination, we used male diabetic db/db and nondiabetic db/+ mice in groups of 8 or 9 animals aged 20, 30, 40, and 50 weeks, as well as 11 diabetic db/db female mice and 9 nondiabetic db/+ female mice aged 50 weeks. We meticulously observed all teeth under a binocular stereoscope and categorized all macroscopic lesions on the teeth according to severity: ○, intact; ▲, hole in a crown or partial molar defect; and •, complete molar defect (see Table 1 ).
Incidence and scoring of dental lesions in mice.
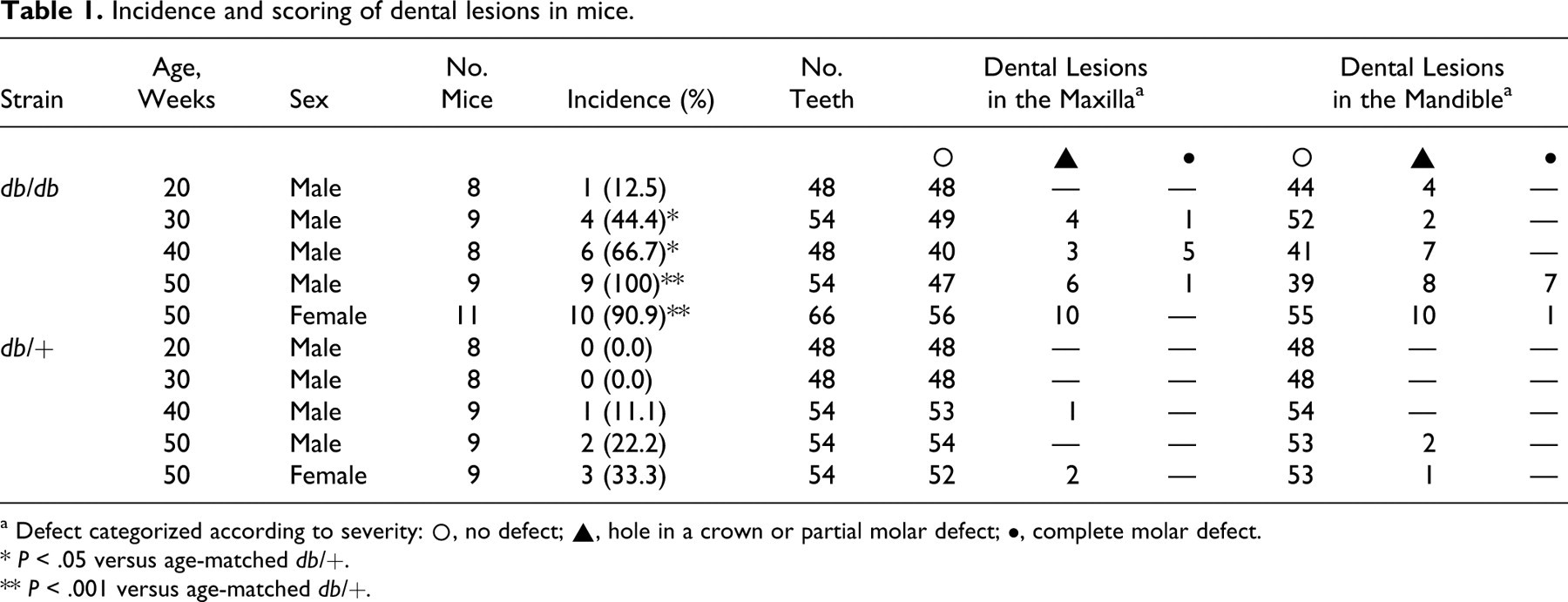
a Defect categorized according to severity
○, no defect
▲, hole in a crown or partial molar defect
•, complete molar defect.
* P < .05 versus age-matched db/+.
** P < .001 versus age-matched db/+.
Histopathological Examination for Dental Caries and Periodontitis
For histopathological examination, we used 9 males and 11 females of diabetic db/db mice aged 50 weeks, along with 9 age-matched males and 9 nondiabetic db/+ females. The mandibles and maxilla were fixed in 10% neutral buffered formalin, decalcified in a 5% solution of EDTA 4 Na for 2 weeks at 4°C, and embedded in paraffin. Four-micrometer sections representing mesial and distal surfaces were made from all molars and stained with hematoxylin and eosin. Severity of dental caries was graded as follows: 0, not observed; 1, dentin caries; 2, dentin caries and pulpitis or pulp necrosis; and 3, decay of corona dentis. Inflammatory changes were evaluated in gingivitis and apical periodontitis, which are the 2 main components of periodontal disease in this study. Gingivitis grade was based on the score of inflammatory cell infiltration: –, no inflammatory cells; +, a few inflammatory cells infiltrating the junctional epithelium; and ++, inflammatory cells scattered throughout the gingival connective tissue. Apical periodontitis evaluation was based on the score of inflammatory cell infiltration: –, no inflammatory cells; +, inflammatory cells infiltrating the apical area; and ++, abscess of the apical area.
For some db/db mice, mandibular molars with dental abnormalities were fixed with 10% neutral buffered formalin and embedded in methylmethacrylate (Wako Pure Chemical Industries, Japan), the blocks of which were sliced with a belt-type cutting device (EXAKT BS-300CL, Norderstedt, Germany), as followed by hand grinding (EXAKT MG-4000, Norderstedt, Germany). Sections approximately 30 μm in thickness were evaluated and graded in the same way as the paraffin-embedded tissues.
Statistical Analysis
Wilcoxon rank-sum test was employed for the analysis of caries scores in each molar, in addition to the chi-square test to determine the ratio of mice or molars developing dental caries. The Mann–Whitney U test was used to compare the frequency of periodontal disease. Pearson correlations were used to examine the relationships between molar caries and apical periodontitis or gingivitis.
Results
General Condition, Urine Glucose, and Blood glucose
No clinical abnormalities were observed in any of the nondiabetic db/+ mice throughout the experimental period. One female diabetic db/db mouse was emaciated at 50 weeks of age. In diabetic db/db mice, the mean body weight apparently increased in comparison with that in nondiabetic db/+ mice at 20 weeks of age but gradually decreased during the experimental period. The average body weight of male and female diabetic db/db mice at 50 weeks of age was 32.9 ± 5.6 g and 36.0 ± 1.0 g, respectively, compared with 31.1 ± 4.0 g and 31.8 ± 2.2 g in male and female nondiabetic db/+ mice, respectively. In all diabetic db/db mice, severe hyperglycemia (> 400 mg/dl) and glucosuria (> 500 mg/dl) continued from approximately 10 weeks after birth to the time of scheduled necropsy. In contrast, all nondiabetic db/+ mice showed normal values (blood glucose < 150 mg/dl, urine glucose < 100 mg/dl) during the experimental period.
Macroscopic Observation
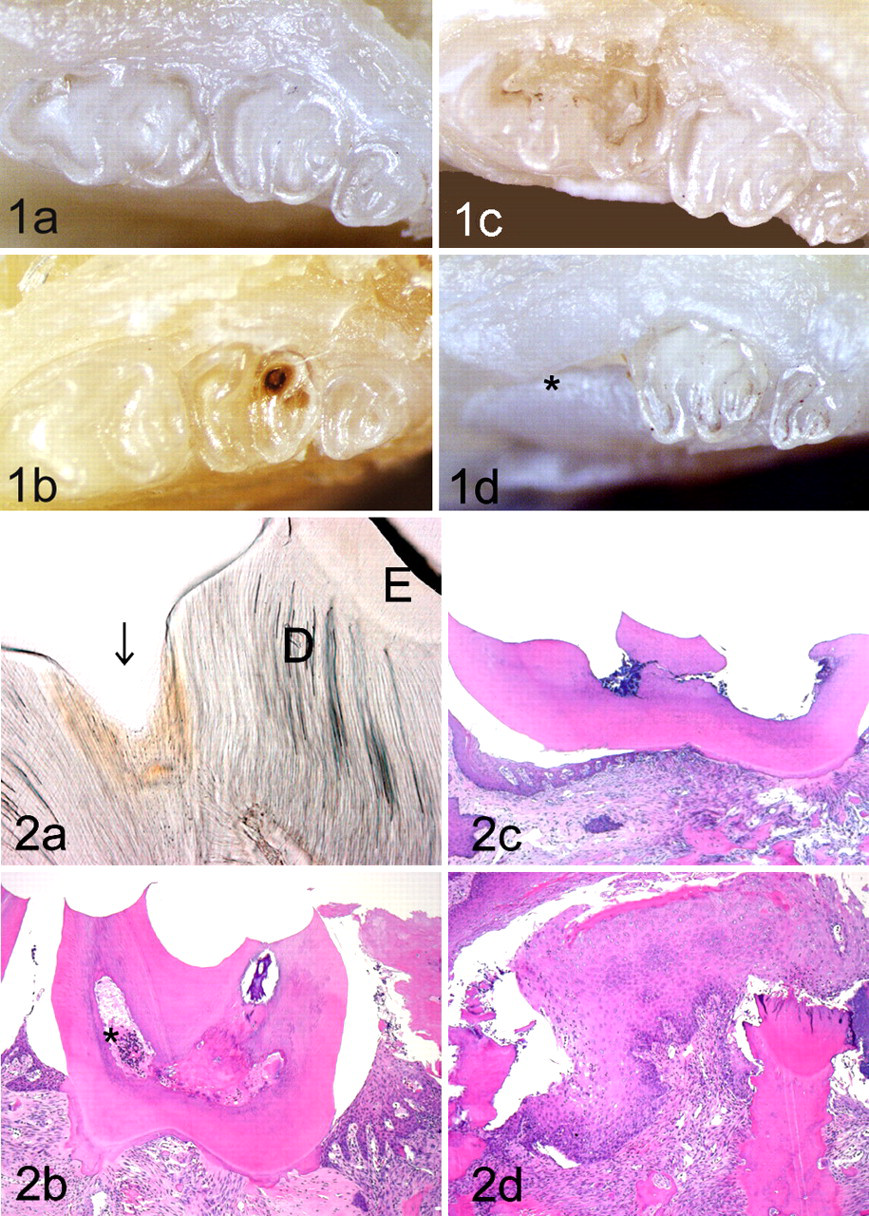
Figure 1 presents typical macroscopic features of carious molars of the mandible and maxilla in diabetic db/db mice. The earliest dental abnormality was a small brown spot on an occlusal fissure of the molar (Fig. 1B). The subsequent lesion was a partial coronal defect with a larger-size dental abnormality (Fig. 1C), whereas the most severe lesions involved loss of the crown of the molar (Fig. 1D).
Some gross dental lesions were detected in mice at 20 weeks of age, with the greater number and severity of lesions in diabetic db/db mice than in nondiabetic db/+ mice. Nondiabetic db/+ mice never had severe molar lesions, such as partial coronal defects and completely destroyed crowns, as observed in the maxillary and mandibular molars of diabetic db/db mice (Table 1).
Histopathological Examination
Histologically, dental caries originated in the crown, with the following 3 lesion severities in the mandibular and maxillary molars of both sexes in almost all diabetic db/db mice. In the ground sections, dentin caries (score 1) initially appeared as a pit in the fossa, an area not covered by enamel. Areas surrounding these pits had brown discoloration and disarray of dentin (Fig. 2A). Next in severity was the deeper dentin caries that developed into pulpitis or pulp necrosis (score 2). These were characterized by necrotic dentin, destroyed dentinal tubules, beading and coalescence of dental tubules at the crown surface, and neutrophil infiltration of the pulp (with and without pulp necrosis) and bacterial colonization (Fig. 2B). In the most severe carious lesions (score 3), the cleft expanded, affecting almost the entire crown, resulting in abscess, pulp necrosis, and decay of the crown (Fig. 2C, 2D). The incidence and severity of histologically assessed dental lesions were significantly higher in diabetic db/db mice than in nondiabetic db/+ mice, in which grade 2 carious molars were detected in only a few cases (Table 2 ).
Incidence and scoring of the caries of molars in db/db and db/+ mice.
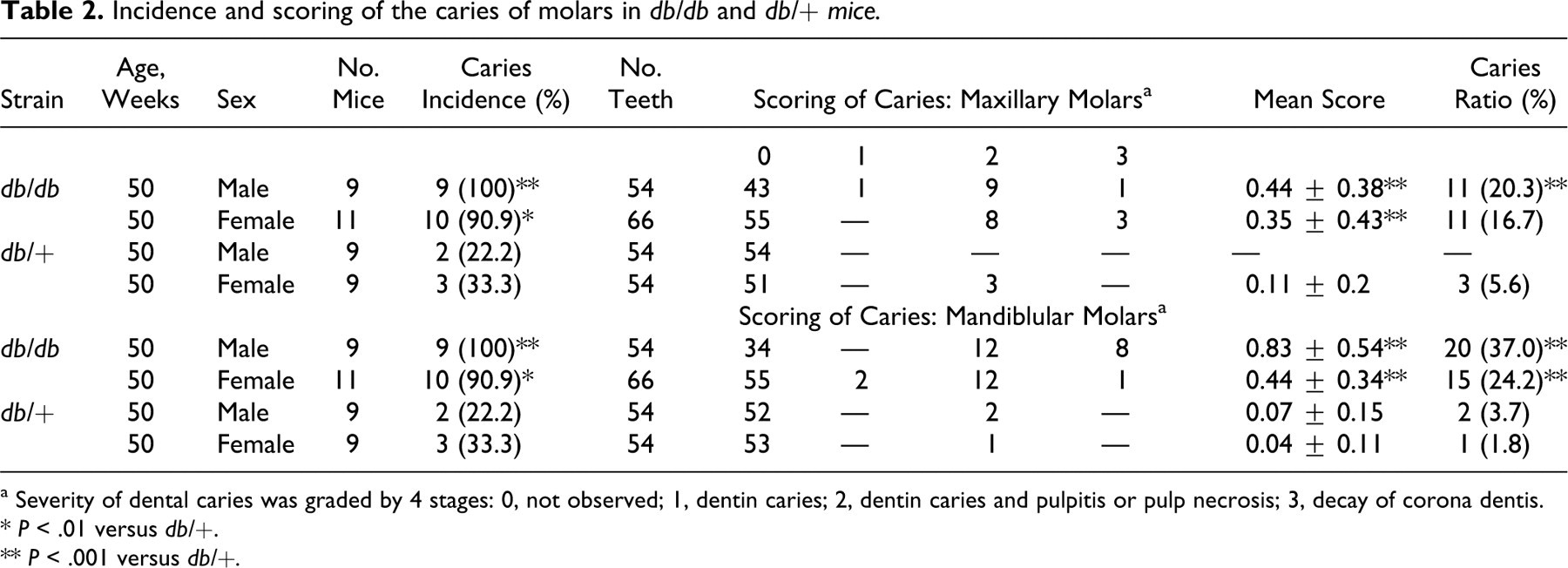
a Severity of dental caries was graded by 4 stages: 0, not observed; 1, dentin caries; 2, dentin caries and pulpitis or pulp necrosis; 3, decay of corona dentis.
* P < .01 versus db/+.
** P < .001 versus db/+.
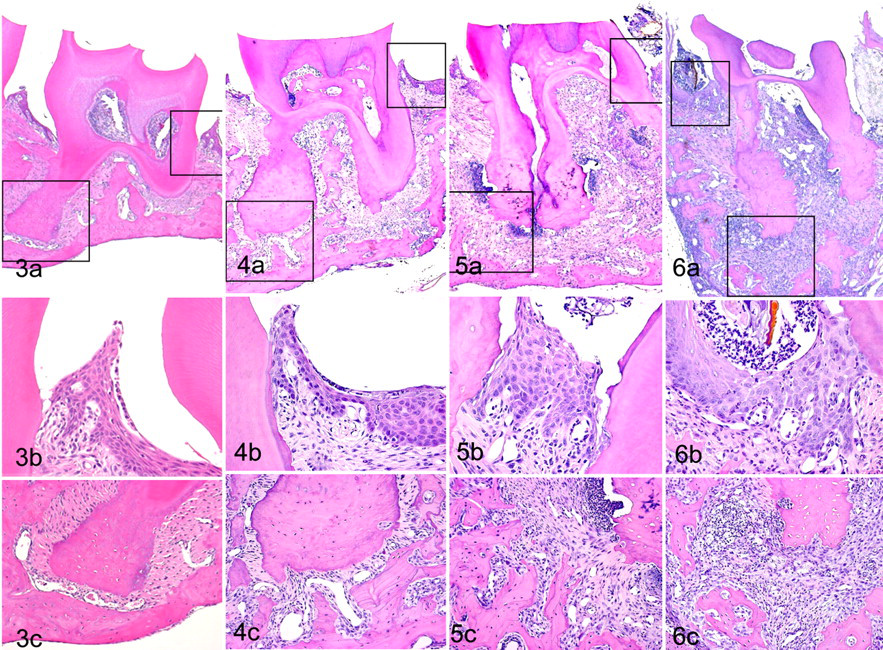
Apical periodontitis involved characteristic changes in the mandibles and maxillas of both sexes in diabetic db/db mice. In the mild lesions, small numbers of neutrophils emigrated to the perivascular area near the apex of the root, coincident with the pulpitis and focal pulp necrosis associated with dental caries (Fig. 4A, 4B, 4C). Severe lesions formed abscesses near the root apex, along with widened apical periodontal connective tissue and neutrophils infiltration (chronic apical suppurative periodontitis; Fig. 5A, 5B, 5C). More severe apical periodontitis was frequently accompanied by widespread dental caries, and the entire pulp cavity and periodontal tissue became filled with necrotic debris and neutrophil (Fig. 6A, 6B, 6C). Apical periodontitis resulted in edematous loosening of connective tissue and extended into adjacent alveolar bone, often with concomitant bone resorption (Fig. 6A, 6C). The incidence and severity of the lesions were significantly higher in diabetic db/db mice than in nondiabetic db/+ mice, which rarely had apical periodontitis (Table 3 ).
Frequency of lesions in periodontal tissue: n (%) a
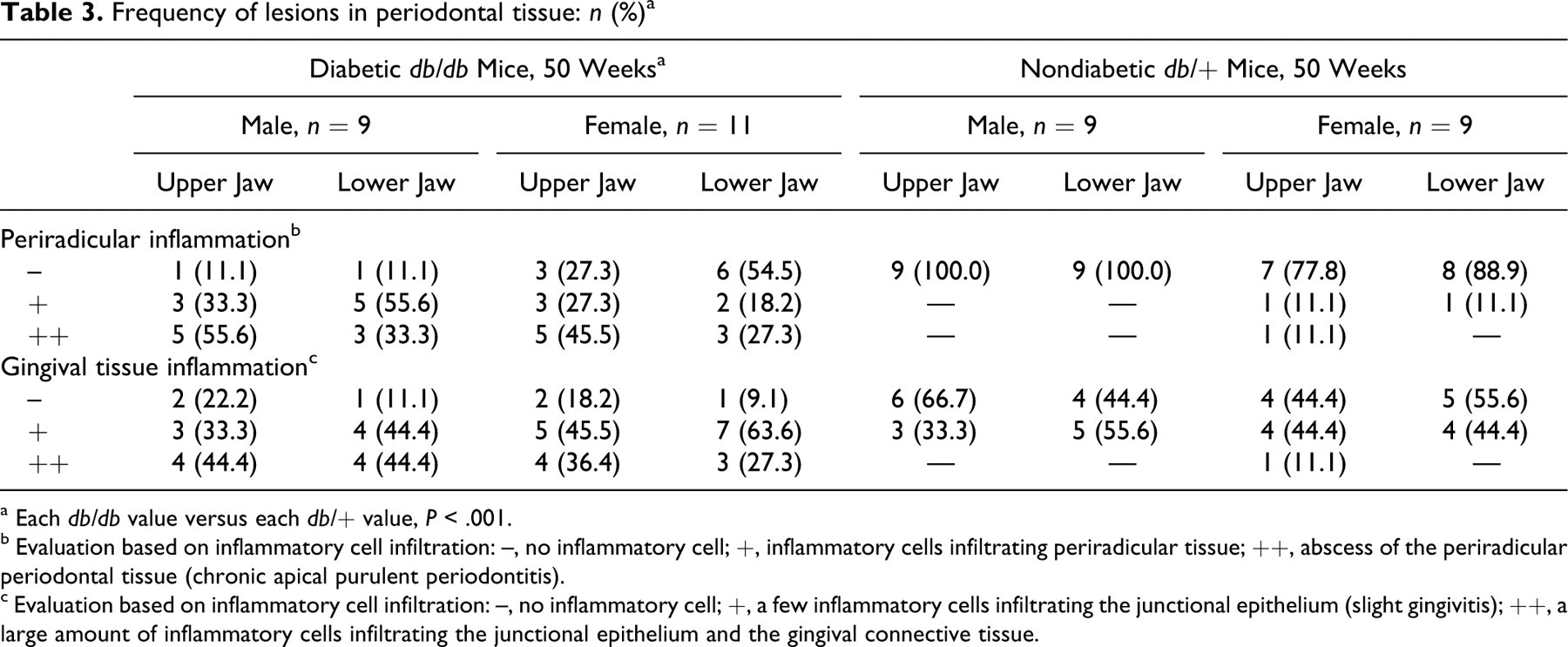
a Each db/db value versus each db/+ value, P < .001.
b Evaluation based on inflammatory cell infiltration: –, no inflammatory cell; +, inflammatory cells infiltrating periradicular tissue; ++, abscess of the periradicular periodontal tissue (chronic apical purulent periodontitis).
c Evaluation based on inflammatory cell infiltration: –, no inflammatory cell; +, a few inflammatory cells infiltrating the junctional epithelium (slight gingivitis); ++, a large amount of inflammatory cells infiltrating the junctional epithelium and the gingival connective tissue.
Small numbers of neutrophils equally emigrated into the mucosal surface of diabetic db/db and nondiabetic db/+ mice, regardless of the presence or absence of dental caries (Figs. 3B, 4B, 5B). However, inflammatory progression occurred in almost half the diabetic db/db mice (Table 3), resulting in severe apical periodontitis with mucosal hyperplasia (Figs. 5B, 6B) and abscess (Fig. 6A, 6B). In such severe cases, gingival pockets were filled with plant and hair shaft debris. In more severe cases, the surface of the teeth affected with severe dental caries was often covered by hyperplastic mucosa with neutrophil infiltration (Fig. 5B). The incidence and severity of gingivitis were significantly higher in diabetic db/db mice than in nondiabetic db/+ mice (Table 3).
There was a significant correlation between severity of caries and severity of apical periodontitis. Periradicular inflammation was observed in diabetic db/db and nondiabetic db/+ mice with dental caries. In many affected teeth, the inflammatory changes frequently extended from the pulp through the dental roots to the periradicular tissue. Severity of apical periodontitis was positively correlated with severity of molar caries: male maxilla, r = .86, P < .001; male mandible, r = .87, P < .001; female maxilla, r = .92, P < .001; female mandible, r = .79, P < .001. In addition, severity of gingivitis was positively correlated with the severity of molar caries: male maxilla, r = .53, P < .001; male mandible, r = .63, P < .001; female maxilla, r = .42, P < .001; female mandible, r = .63, P < .001.
Discussion
When considering the pathogenesis of dental caries, one need note that the lesions have a multifactorial etiology involving 4 main factors: sucrose and other sugars in food, acid-producing pathogenic bacteria, predisposing host factors (the anatomical, physiological, and behavioral characteristics of the host that affect susceptibility to dental caries), and time. 18,32 Researchers have induced caries in experimental animals with a cariogenic diet containing large amounts of sugar and/or an inoculation of infectious cariogenic bacteria into the oral cavity. 29 In earlier studies, a diet high in sucrose or other carbohydrates (cariogenic diet) was used, even in diabetic animals. 2,12,30 In this study, we used Charles River Formula 1, a standard laboratory diet that provided a far lower level of sugar than that in established cariogenic diets, 10 and we confirmed that nondiabetic db/+ mice had a low incidence of dental caries. Therefore, the high incidence of caries in our diabetic db/db mice without experimental manipulations showed that diabetes can be associated with dental caries.
Type 2 diabetes significantly increases the risk and severity of periodontal disease in humans. 3,9,38,41 Likewise, many investigations have shown that diabetes directly increases risk and severity of periodontitis in diabetic animal models. Non-insulin-dependent diabetic animals (Zucker diabetic fatty rats and Goto-Kakizaki rats) have had enhanced ligature-induced periodontal disease. 21,31 Long-standing alloxan-induced insulin-dependent diabetes mellitus can cause advanced periodontal disease. 6,33 In accordance with these observations, most diabetic db/db mice in the present study had gingivitis and apical periodontitis, whereas corresponding lesions were infrequent and mild in nondiabetic db/+ mice. Morphological characteristics of gingival lesions were similar to those described in other studies. 6,33 Our results suggest that dental and apical periodontitis are continuous changes and that the lesions develop from dental caries. Despite considerable recent research into periodontal disease in diabetic animal models, insufficient morphological analyses of dental caries have been carried out in those animals. Yet a recent study reported that severe apical periodontitis was induced in diabetic Goto-Kakizaki rats by high-sucrose solution exposure of the pulp. 17 Thus, the previous and present data support the hypothesis that diabetes enhances the development of apical periodontitis. In addition, severe gingivitis occurred adjacent to teeth with severe apical lesions, and progression of gingivitis correlated well with severity of molar caries. Thus, severe gingivitis might have occurred as a result of severe apical periodontitis owing to dental caries.
The precise pathogenesis of dental caries in diabetic db/db mice has not been determined; however, increased prevalence of caries has been attributed to reduced salivary flow rates in diabetic patients. 27,35 Reduction of salivary flow also plays an important role in reduced wound healing and plaque formation. 25,28 Altered components of salivary secretions may affect profiles of oral microflora in rats and humans. 1,23,24,35 In addition, it is well known that increased susceptibility to infection associated with diabetes is due to impaired function of polymorphonuclear leukocytes. 11,36 Finally, diabetic animals typically have higher food intake than that of nondiabetic animals. 20,40 All of these factors may thus contribute to onset of dental caries and severity of caries-related periodontitis in diabetic db/db mice.
In conclusion, our results indicate that diabetic conditions enhance dental caries and suggest that periodontitis arises secondary from dental caries in db/db mice.
Footnotes
Acknowledgements
We are most grateful to Maiko Mori, Yumi Yamamoto, Akihiro Kanagawa, and Nana Shako of our laboratory for their technical assistance. We also wish to thank our many colleagues for their generous assistance during this study.
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
The authors received no financial support for the research and/or authorship of this article.